Back to Journals » Research and Reports in Urology » Volume 10
Artificial urinary sphincters for treating postprostatectomy incontinence: A contemporary experience from the UK
Authors Serag H ![]() , Bang S, Almallah YZ
, Bang S, Almallah YZ
Received 25 April 2018
Accepted for publication 26 June 2018
Published 4 September 2018 Volume 2018:10 Pages 63—68
DOI https://doi.org/10.2147/RRU.S172252
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jan Colli
Video abstract presented by Y Zaki Almallah.
Views: 2870
Hosam Serag, Shirley Bang, Y Zaki Almallah
Department of Urology, Queen Elizabeth Hospital Birmingham-University Hospital Birmingham, Birmingham, UK
Objectives: To report a real-time contemporary practice and outcome of artificial urinary sphincter (AUS) in patients with postradical prostatectomy urinary incontinence (PPI) in the UK.
Methods: A retrospective observational study of patients who underwent AUS implantation (AMS 800) from 2007 to 2013. Data were collected on patients’ demographics, infection and erosion rate, mechanical failure, reoperation, and continence rates. The study strictly included patients with postradical PPI only. Minimum follow-up was 15 months.
Results: Eighty-four AUSs were implanted over a period of 6 years. Patients’ age ranged between 51 and 78 (median 69, mean 69.25) years. Median follow-up was 37 months, mean 39 months, and range 15–92 months. Among the 83 follow-up patients, 38.5% (32/83) reported that they were completely dry with no pads; 42.2% (35/83) of patients were socially continent (using 1 pad/day) and 19.3% (16/83) using ≥2 pads /day. One patient was lost to follow-up. Reoperation rate was 13.25% (11/83), including nine mechanical failures (10.8%). Two implant infections (2.4%) required explantation, out of which one had erosion (1.2%). Bladder overactivity developed in 6% of patients. Of the 83, 15 (18%) had pelvic radiotherapy.
Conclusion: The implantation of AUS in patients with post-PPI has lower complications and reoperation rates than historical impression painted in the literature. This can be beneficial in counseling as well as during the education process of patients going through the decision process for prostate cancer treatment. Furthermore, these figures can add to our quest to increase the awareness of the success of anti-incontinence surgery among patients.
Keywords: Post-prostatectomy urinary incontinence, artificial urinary sphincter, male incontinence, radical prostatectomy complications, outcomes of artificial urinary sphincter, incontinence surgery counseling
Introduction and objectives
Postradical prostatectomy urinary incontinence (PPI) represents a critical functional complication following prostate cancer surgery and has a significant impact on patient’s quality of life. The artificial urinary sphincter (AUS) is the standard surgical treatment for PPI. Implantation of AUS in patients with PPI is believed to have a better outcome than in those with neurogenic incontinence.1,2 However, PPI patients’ expectation may be higher. Historically, there are high complications and reoperation rates reported following the implantation of AUS and not many studies differentiated between the two groups. Our aim was to report a real-time contemporary practice and outcome of PPI-only patients treated with AUS in a high-volume tertiary center.3,4
Methods
A retrospective study of patients underwent AUS implantation (AMS 800™) for treating PPI from 2007 to 2013. Data were collected from our electronic clinical portal using an Excel sheet, recording patient demographics, date of operation, duration of follow-up, continence, and postoperative complications including infections, erosion rate, mechanical failure, and reoperation. Patients were classified as completely dry (0 pad), socially continent (1 pad/day or no pads but minimal leakage on straining), or incontinent (≥2 pads/day). The completely dry and socially continent groups were considered a satisfactory result. All patients were strictly postradical prostatectomy; no neurogenic or post-transurethral resection of prostate patients were included. Mechanical failure was defined as recurrence of incontinence due to device malfunction within 10 years of implantation. Urethral atrophy was defined as recurrence of the stress incontinence with a functioning device, mainly proven after removal of device.
Recurrence of stress incontinence is defined as deterioration from baseline post AUS implantation. This is identified by increased leakage above baseline and increase in pad usage after a period of improvement.
The preoperative degree of incontinence evaluation included a voiding diary, pad weight, urodynamic studies, and flexible cystoscopy. After thorough investigations, the modality of treatment is discussed with the patients.
Statistical analysis
The statistical analyses were carried out using LIFETEST procedure and two-sample t-test. The Kaplan–Meier method was used to calculate survival-free estimates of mechanical failure or revision. Minimum follow-up period was 15 months.
Results
Eighty-four AUSs were implanted over a 6-year period. Patients’ age ranged between 51 and 78 years, with median 69 years and mean 69.25 years. The median follow-up was 37 months, mean 39 months, and range 15–92 months. One patient was lost to follow-up. Of 83 patients, 15 (18%) had radiotherapy. A summary of results is shown in Table 1 and 2 shows our results compared with similar series published.
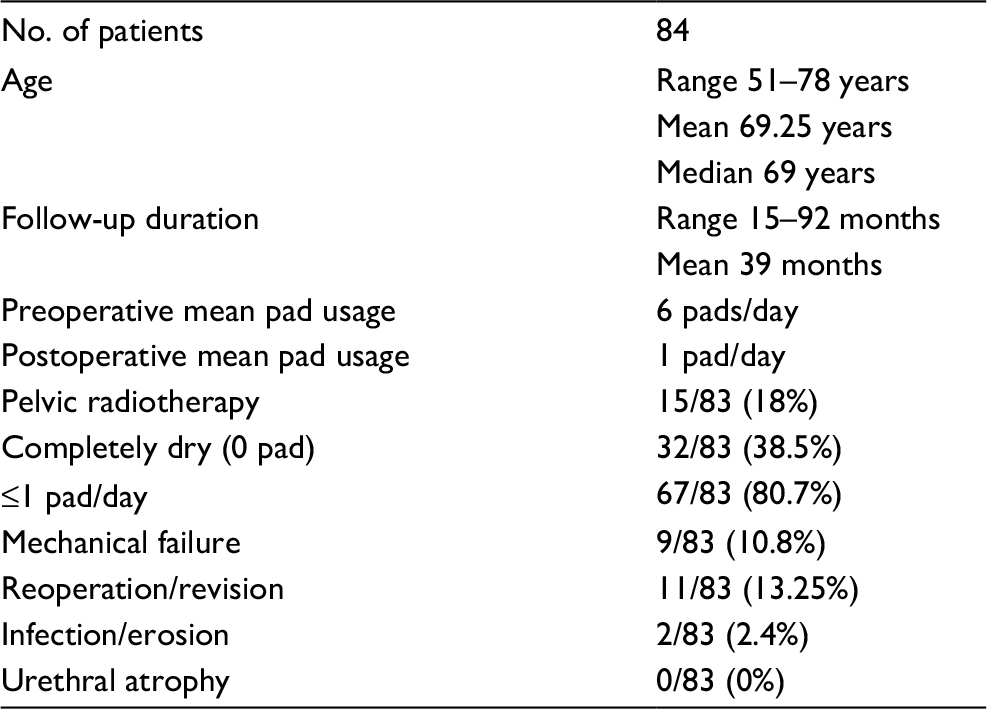 | Table 1 Summary of patient demographics and outcomes |
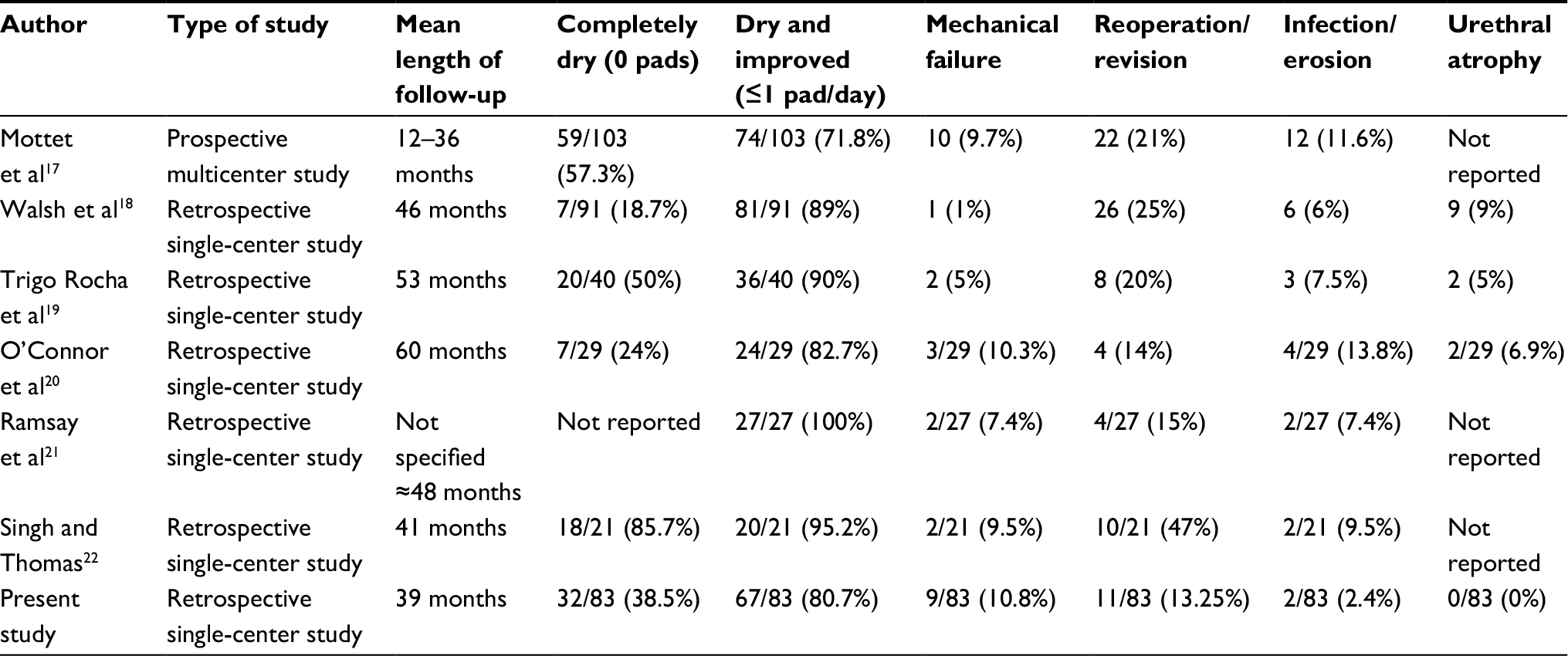 | Table 2 Summary of outcomes in comparison with similar series |
Continence
Among the 83 follow-up patients, 38.5% (32/83) of patients reported that they were completely dry and not using any pads; 42.2% (35/83) were socially continent (using 1 pad/day) and 19.3% (16/83) using ≥2 pads/day. Patients who achieved social continence or better were considered as a satisfactory outcome (ie, using one pad or no pad). There was reduction in average pad usage of 6 pads/day preoperatively to 1 pad/day postoperatively for the whole series. An overall satisfactory result was achieved in 80.7% of cases (67/83).
Revision/Reoperations
Revision surgery was needed in cases that developed a mechanical failure of the AUS or device removal due to infection or erosion. Overall, 13.25% (11/83) had to undergo a revision or a reoperation in relation to the AUS implantation; this includes nine mechanical failures (10.8%) due to malfunctioning device and two device explantations due to infections.
Mechanical failure occurred between 2 and 84 months post AUS insertion, median 18 months and mean 24 months. Every device removed was examined and tested in theater immediately after removal and then sent to the manufacturer for confirmation of mechanical failure.
Figure 1 shows the estimated mechanical failure-free survival, which is 89.9% at 5 years but at 10 years the mechanical failure rates increases which is in keeping with the life expectancy of the device. Figure 2 shows the revision-free estimated survival, 86.75% at 5 years but at 10 years the revision rate will increase as expected due to device failure.
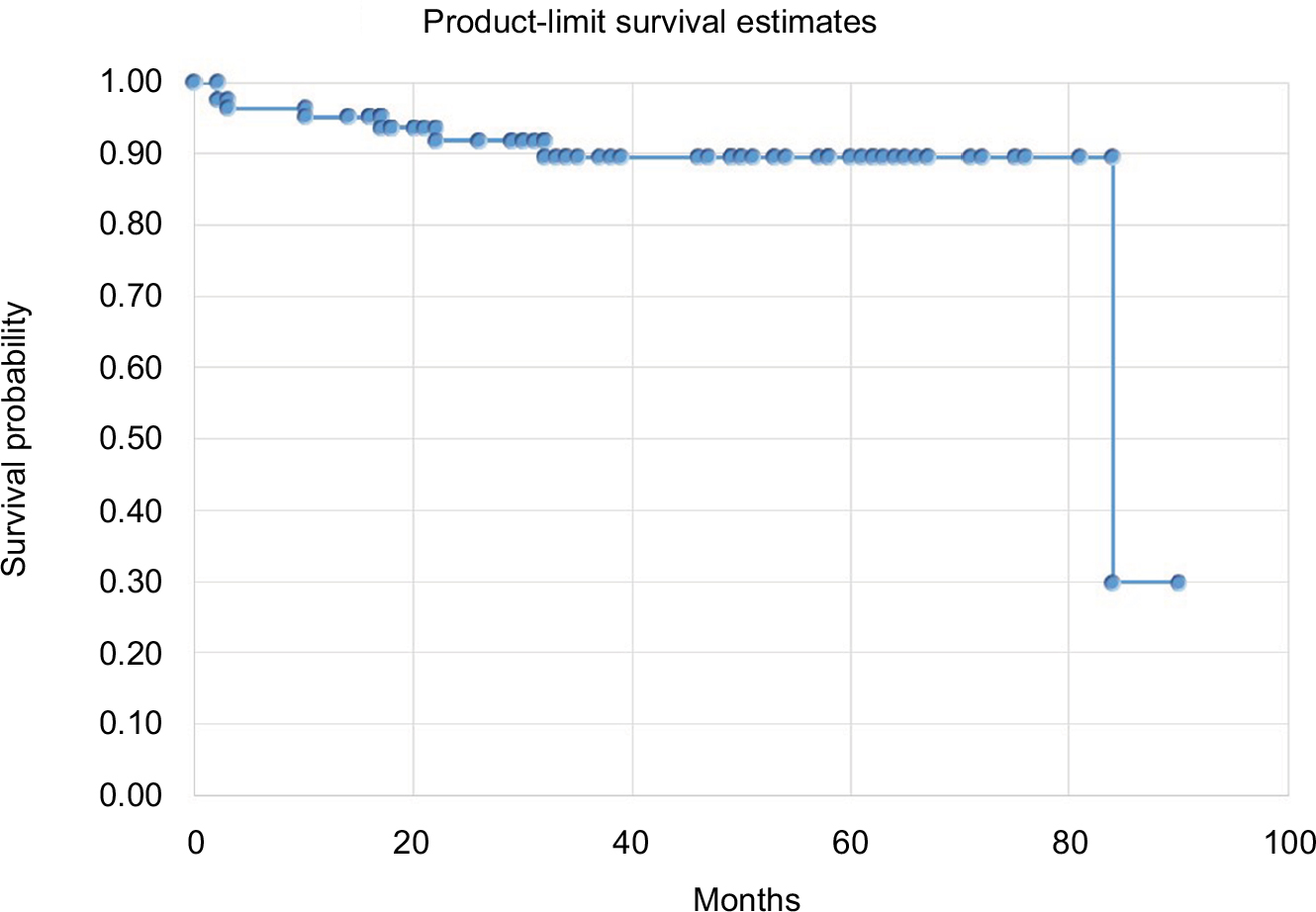 | Figure 1 Estimated mechanical failure-free survival (Y-axis represents survival probability, X-axis represents time in months). Note: Kaplan–Meier curve for time to mechanical failure. |
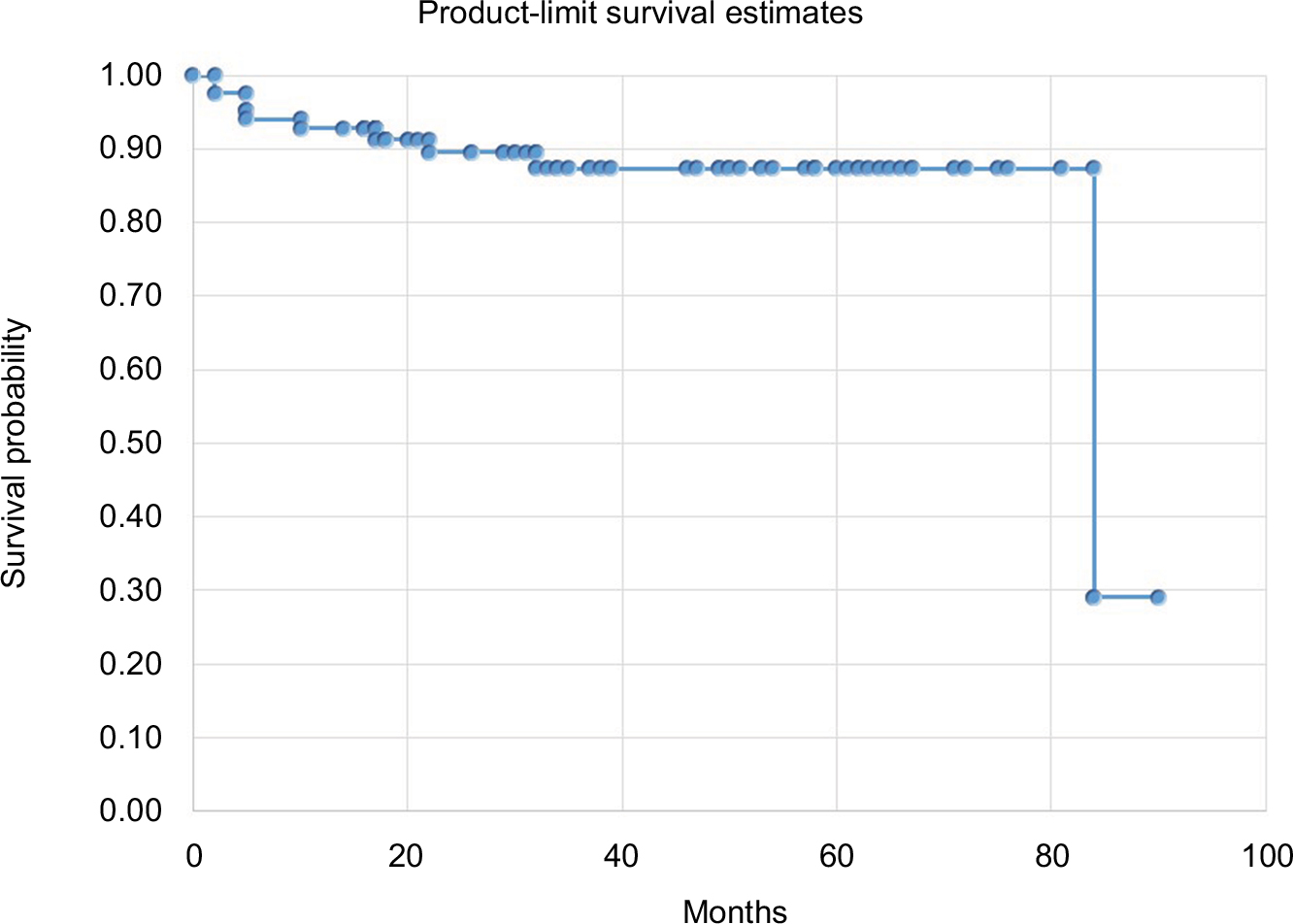 | Figure 2 Estimated revision-free survival. Note: Kaplan–Meier curve for time to revision surgery. |
Infections and erosions
Implant infection requiring removal of device occurred in 2/83 (2.4%) patients. One incidence involved a patient who failed to deactivate the device causing subsequent retention followed by multiple catheterization attempts in emergency department without deactivating the AUS, who subsequently required a suprapubic catheter, then developed abdominal wound infections requiring hospital admission and intravenous antibiotics; this case was the only urethral erosion in the series. The other case presented 6 months post AUS implantation with a scrotal sinus and infection, this was managed initially with antibiotics to stabilize the patient and then the device was removed subsequently. There were two other minor abdominal wound infections and three perineal wound infections, which required treatment with oral antibiotics. Two patients developed urinary tract infections following removal of the catheter and required a short course of oral antibiotics without hospital admission.
Age
Age of the patient at the time of the initial procedure did not seem to be a risk factor for mechanical failure or revision surgery; the results of two-sample t-test to compare age in the nonmechanical failure group (mean age 68 years) vs mechanical failure group (mean age 69 years) show no statistically significant relation with age (P-value=0.6611) and a similar result for revision surgery, the nonrevision group (mean age 67.9 years) vs revision group (mean age 68.36 years) (P-value=0.8436).
Bladder overactivity
De novo bladder overactivity developed in 6% (5/84) of patients, all were managed with anticholinergics and did not require further treatment.
Bladder neck stenosis
Of the 83 patients, 20 (24.1%) had bladder neck stenosis prior to AUS implantation, all underwent treatment and had a flexible cystoscopy prior to establishing a stable open bladder neck. Of the 20 patients, 3 (15%) with previous bladder neck stenosis had revision surgery, one due to erosion and infection following traumatic catheterization and the other two patients had revision surgery due to mechanical failure. One out of these two had recurrence of his bladder neck stenosis after AUS implantation. In the group of patients who did not have prior bladder neck stenosis, 8/63 (12.7%) had revision surgery. There was no real difference between the two groups. Overall, 85% of patients who had previous bladder neck stenosis did not require revision surgery compared with 87% in the group who did not have previous bladder neck stenosis; this implies that the presence of previous bladder neck stenosis does not affect the outcome.
Discussion
The AUS is the gold standard treatment for moderate/severe postprostatectomy incontinence.4–7 Because the device was introduced in 1974, the device has been modified a few times through the years until it reached the current design in 1987.7 The therapies for PPI include pelvic floor muscle exercises, pharmacotherapy, urethral bulking agents, male slings, and AUS.6,8,9 Initial conservative measures are attempted prior to considering more invasive treatments. The choice of surgical treatment depends on the degree and severity of incontinence. Slings are used in mild/moderate degree of incontinence, while AUS is reserved for more severe cases. Currently, the MASTER trial (https://www.mastertrial.co.uk) is recruiting to compare the efficacy of slings vs AUS and provide the evidence to show which of the two modalities is best for which degree of incontinence.
Historically, literature reported AUS outcomes for the treatment of both neuropathic and non-neuropathic incontinence with high complications and reoperation rates.1 Few studies have reported on using AUS in non-neurogenic patients. Reoperation or reintervention is needed either to replace a nonfunctioning device (due to mechanical failure or urethral atrophy) or to explant an infected device.
The efficacy of AUS and continence postinsertion is the most relevant factor from patients’ perspective, and this is reflected in patient satisfaction score. However, the lack of standardization in assessing continence can make it difficult to compare results with other studies.10 A systematic review of 12 studies by Van der Aa et al including data of 623 patients showed that continence was achieved in 61%–100% of cases, complete dryness (0 pads) in 43.5%, and social continence (≤1 pad/day) in 79%. Dry rates (0 pad) were only available in seven studies and varied from 4% to 86%.4 In our series, 38.5% (32/83) of patients reported that they were completely dry with no pads; 42.2% (35/83) were socially continent (using 1 pad/day). Overall satisfactory result was achieved in 80.7% (67/83), with 19.3% (16/83) using ≥2 pads/day; however, this still represented an improvement compared with their presphincter surgery condition.
As any device, AUS is liable for mechanical failure and it could occur in any of the components of the device; the cuff, tubing, pump, or reservoir. In a study by Lai and Boone in 2013, the device failure rate was estimated to be 50% at 10 years.11 In a systematic review by Van der Aa et al, several studies reported mechanical failure rates varying between 2.0% and 13.8%. Failures occured from 11–68 months post insertion, with an average reoperation rate of 26.0% (range: 14.8%–44.8%).4 In another large study on 554 men by Raj et al with a mean follow-up of 68 months, there was a 0.46% infection rate in 435 patients who underwent primary AUS implantation. The cause of failure in 119 patients who underwent secondary AUS implantation was mechanical failure in 31 patients (25.2%) and nonmechanical in 88 patients (73.9%).12
In our series of 84 patients with an average follow-up of 39 months, the overall revision rate is 13.25% (11/83), this includes nine mechanical failures (10.8%), one infected device, and one infected device associated with erosion (2.4%). Early erosion in the first few weeks usually occurs when the urethra is injured during mobilization especially at the dorsal aspect. Late erosion occurs secondary to traumatic catheterization without deactivation of the sphincter.13
Urethral atrophy is a complication of AUS and it is difficult to diagnose. It usually presents with a gradual recurrence of incontinence with an increase in pad usage. This is a diagnosis of exclusion when other causes of incontinence have been ruled out. At the time of revision, the AUS device will be still functioning. We believe the absence of urethral atrophy in our series is related to technique and the choice of cuff. We routinely leave the bulbospongiosus muscle intact in most cases; this provides an extra layer of support to the urethra. The urethral circumference is measured and cuff size is chosen; if there is any doubt about using a 4- or 4.5-cm cuff, we will always use the larger size to make sure it is never too tight. A 4.5-cm cuff was our most frequently used size. We have never used a 3.5-cm cuff and rarely a 4-cm cuff.
In a study by Kim et al, where the longest follow-up was 10 years, the vast majority of complications occur in the first 48 months following insertion of AUS.14 In our study, the average follow-up is 39 months, which implies that most of the complications have already occurred and the figures presented in this study are a true reflection of outcomes on the long-term.
The lower reoperation and complication rate reported encourages a modified counseling of the patients undergoing or recently undergone radical prostatectomy regarding their continence outcome and using more current data, as the complication rates in our series of PPI patients may not be as high as historically reported.
Certainly, the surgeons’ experience is another important factor. Sandhu et al demonstrated a slow but steady decrease in reoperation rates with increasing surgeon experience (P=0.020), showing a plateau in learning curve after 200 procedures; this finding supports centralization of this procedure in tertiary centers with large patient volumes.11,15,16
Conclusion
The implantation of AUS in patients with post-PPI has lower complications and reoperation rate than historical impression painted in the literature. This can be beneficial in counseling as well as during the education process of patients going through the decision process for prostate cancer treatment. Furthermore, these figures can add to our quest to increase the awareness of the success of anti-incontinence surgery among patients.
Ethics approval
Health research authority decision tool was used; this has shown that NHS REC ethics approval was not required. Institutional review board approval was not required as we used anonymized clinical data that have already been collected as part of normal care. University Hospital Birmingham NHS Foundation Trust audit department as well as Research and Development Department were involved in data collection as part of quality reassurance and improvement of care.
Acknowledgments
We thank Dr Wen Wan, PhD (Medical Statistician at Chicago University, USA) for her help with the statistical analysis of this study. Preliminary results of this series have been presented at Society Internationale d’Urologie 2014 and abstract published in Gold Urology Journal, Volume 84, Issue 4, Supplement, October 2014, Pages S1–S146. This publication reflects longer follow-up results.
Disclosure
YZA is an advisor for the National Institute for Health and Clinical Excellence (NICE) and the National Institute for Health Research (NIHR) – Health Technology Assessment (HTA) Program and user/trainer of various male anti-incontinence devices manufactured by American Medical Systems. The authors report no other conflicts of interest in this work.
References
Gonzalez R, Merino GP, Vaughn M. Long-term results of the artificial sphincter in male patients with neurogenic bladder. J Urol. 1995;154:769–70. | ||
Stanford JL, Feng Z, Hamilton AS et al. Urinary and sexual function after radical prostatectomy for clinically localized prostate cancer: the prostate cancer outcomes study. Journal of the American Medical Association. 2000;283(3):354–360. | ||
Sanda MG, Dunn RL, Michalski J et al. Quality of life and satisfaction with outcome among prostate-cancer survivors. New England Journal of Medicine. 2008;358(12):1250–1261. | ||
Van der Aa F, Drake MJ, Kasyan GR, Petrolekas A, Cornu J-N, Young Academic Urologists Functional Urology Group. The artificial urinary sphincter after a quarter of a century: a critical systematic review of its use in male non-neurogenic incontinence. Eur Urol. 2013;63:681–689. | ||
Ravier E, Fassi-Fehri H, Crouzet S, Gelet A, Abid N, Martin X. Complications after artificial urinary sphincter implantation in patients with or without prior radiotherapy. BJU Int. 2015;115:300–307. | ||
Abedin A, Almallah Z. Cuffs, slings, pills and electric shocks: an update on male urinary incontinence. Journal of Clinical Urology. 2014;2:80–89. | ||
Montague DK. Artificial Urinary Sphincter: Long-Term Results and Patient Satisfaction. Advances in Urology. 2012;2012, Article ID 835290. | ||
Sandhu J. Treatment Options for Post-Prostatectomy Incontinence. Urology Practice. 2014;1(4):194–197. | ||
Trost L, Elliott D. Male Stress Urinary Incontinence: A Review of Surgical Treatment Options and Outcomes. Advances in Urology. 2012;2012, Article ID 287489. | ||
Walsh IK, Williams SG, Mahendra V, Nambirajan T, Stone AR. Artificial urinary sphincter implantation in the irradiated patient: safety, efficacy and satisfaction. BJU Int. 2002;89:364–368. | ||
Lai HH, Boone TB. The Surgical Learning Curve of Artificial Urinary Sphincter Implantation: Implications for Prosthetic Training and Referral. J Urol. 2013;189:1437–1443. | ||
Raj GV, Peterson AC, Toh KL, Webster GD. Outcomes following revisions and secondary implantation of the artificial urinary sphincter. J Urol. 2005;173:1242–1245. | ||
McGeady JB, McAninch JW, Truesdale MD, Blaschko SD, Kenfield S, Breyer BN. Artificial Urinary Sphincter Placement in Compromised Urethras and Survival: A Comparison of Virgin, Radiated and Reoperative Cases. J Urol. 2014:192;1756–1761. | ||
Kim SP, Sarmast Z, Daignault S, Faerber GJ, McGuire EJ, Latini JM. Long-term durability and functional outcomes among patients with artificial urinary sphincters: a 10-year retrospective review from the University of Michigan. J Urol. 2008;179:1912–1916. | ||
Sandhu JS, Maschino AC, Vickers AJ. The surgical learning curve for artificial urinary sphincter procedures compared to typical surgeon experience. Eur Urol. 2011;60:1285–1290. | ||
Doherty R, Almallah Z. Urinary incontinence after treatment for prostate cancer. Long term morbidity can be minimized by early referral to specialist centres. BMJ. 2011;343:d6298 | ||
Mottet N, Boyer C, Chartier-Kastler E, Naoum KB, Richard F, Costa P. Artificial urinary sphincter AMS 800 for urinary incontinence after radical prostatectomy: the French experience. Urol Int. 1998;60 (Suppl 2):25–29. | ||
Walsh IK, Williams SG, Mahendra V, Nambirajan T, Stone AR. Artificial urinary sphincter implantation in the irradiated patient: safety, efficacy and satisfaction. BJU Int. 2002;89:364–368. | ||
Trigo Rocha F, Gomes CM, Mitre AI, Arap S, Srougi M. A prospective study evaluating the efficacy of the artificial sphincter AMS 800 for the treatment of post radical prostatectomy urinary incontinence and the correlation between preoperative urodynamic and surgical outcomes. Urology. 2008;71:85–89. | ||
O’Connor RC, Nanigian DK, Patel BN, Guralnick ML, Ellision LM, Stone AR. Artificial urinary sphincter placement in elderly men. Urology. 2007;69:126–128. | ||
Ramsay AK, Granitsiotis P, Conn IG. The use of the artificial urinary sphincter in the west of Scotland: a single centre 10-year experience. Scott Med J. 2007; 52:14–17. | ||
Singh G, Thomas DG. Artificial urinary sphincter for post prostatectomy incontinence. Br J Urol. 1996;77:248–251. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.