Back to Journals » Clinical Interventions in Aging » Volume 20
Applying the Knowledge-to-Action Framework to Implement and Evaluate an Evidence-Based Functional Exercise Program for Elderly Patients After Total Knee Arthroplasty: A Mixed-Methods Study
Authors Qin Z, Ye X ![]() , Liu H, Shen Y, Zou X, Qiu S, Wu Y, Zhan C
, Liu H, Shen Y, Zou X, Qiu S, Wu Y, Zhan C
Received 1 July 2025
Accepted for publication 25 November 2025
Published 11 December 2025 Volume 2025:20 Pages 2515—2534
DOI https://doi.org/10.2147/CIA.S550742
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Zhi-Ying Wu
Zhuzhu Qin,1,2,* Xinxin Ye,3,* Huanju Liu,4 Yan Shen,1 Xiaoling Zou,5 Shi Qiu,6 Yuxuan Wu,1 Chenju Zhan7
1Department of Orthopedics, People’s Hospital of Deyang City, Deyang, Sichuan, People’s Republic of China; 2School of Nursing, Fujian University of Traditional Chinese Medicine, Fuzhou, Fujian, People’s Republic of China; 3Department of Sports Science, Zhejiang University, Hangzhou, Zhejiang, People’s Republic of China; 4Department of Medical Genetics, Naval Medical University, Shanghai, People’s Republic of China; 5Operating Room, People’s Hospital of Zhongjiang, Deyang, Sichuan, People’s Republic of China; 6Department of Sports Medicine, University of Malaya, Kuala Lumpur, Malaysia; 7Department of Nursing, Mindong Hospital Affiliated to Fujian Medical University, Ningde, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chenju Zhan, Department of Nursing, Mindong Hospital of Fujian Medical University, 89 Heshan Road, Fuan, 355099, People’s Republic of China, Tel +86 13809562183, Email [email protected] Xinxin Ye, Department of Sports Science, Zhejiang University, 866 Yuhangtang Road, Hangzhou, 310058, People’s Republic of China, Tel +86-19157731127, Email [email protected]
Purpose: This study aimed to develop a systematic, evidence-based rehabilitation intervention tailored for elderly patients undergoing TKA, informed by stakeholders, and evaluate its impact on patient outcomes.
Patients and Methods: Guided by the Knowledge-to-Action (KTA) Framework, this study comprised two sequential phases. In the knowledge creation phase, we systematically synthesized evidence through comprehensive retrieval, critical appraisal, and integration of high-quality rehabilitation programs for elderly patients undergoing TKA from domestic and international literature. During the action cycle phase, expert panel discussions and stakeholder interviews were conducted to identify barriers and facilitators of implementation, culminating in the co-development of a finalized intervention program. A quasi-experimental study was subsequently implemented to assess its preliminary efficacy in this target population.
Results: Fourteen high-quality sources were synthesized to form 17 evidence-based recommendations across six dimensions. Through expert panels and stakeholder interviews, a structured rehabilitation program was developed, addressing key barriers and implementation strategies. In the subsequent quasi-experimental study (n = 60), patients in the intervention group showed significantly better postoperative pain control, range of motion, and knee function compared to controls (all P < 0.05), with no baseline differences between groups.
Conclusion: The evidence-based rehabilitation program significantly enhanced functional recovery parameters, and pain control efficacy compared to standard care. Implementation of this structured intervention framework demonstrates clinically meaningful improvements in early postoperative outcomes following TKA.
Keywords: elderly patients, total knee arthroplasty, functional exercise, rehabilitation, evidence-based practice, knowledge to action process framework
Introduction
Knee Osteoarthritis (KOA) is a prevalent degenerative joint disease characterized by articular cartilage degradation and periarticular fibrous tissue proliferation.1 Primarily affecting individuals aged 60 years and older, particularly women, its incidence escalates with advancing age. Clinical manifestations include pain, swelling, and restricted range of motion, with severe cases potentially progressing to joint dysfunction or disability.2 According to epidemiological data, KOA affects nearly 365 million people globally, with its prevalence reaching as high as 50% among those over 60, and an estimated 8.1% prevalence for symptomatic KOA in China.3 Chronic joint deterioration in KOA patients may lead to severe functional impairment, with 23% of advanced cases developing disability, thereby imposing substantial economic and psychological burdens on both patients and their families.4
Total Knee Arthroplasty (TKA), also termed total knee replacement, is widely recognized as the most effective intervention for end-stage KOA. This procedure involves replacing damaged joint surfaces with prosthetic components to restore normal joint function and enhance mobility.5,6 Although the success rate of TKA has been widely confirmed, its ultimate outcomes depend not solely on the surgical procedure itself but critically on postoperative rehabilitation exercises.7 Timely and effective functional exercises following surgery are crucial for ensuring surgical efficacy and reducing complication risks. The stress stimulation induced during rehabilitation plays a vital role in accelerating postoperative callus formation, calcium salt deposition in cancellous bone, and facilitating joint reconstruction. Furthermore, functional exercises positively influence the circulatory system by enhancing lymphatic drainage and blood circulation, thereby reducing postoperative edema and hematoma, promoting wound healing, and preventing deep vein thrombosis.8 The flexion-extension movements during exercise improve postoperative range of motion (ROM), increase lower limb muscle strength, and enhance joint stability.9 Restoration of joint function after TKA constitutes a prolonged and progressive process. To optimize muscle strength retention and maintain joint functionality, patients require sustained rehabilitation training over an extended period. Consequently, consistent adherence to scientifically-guided exercise regimens is paramount for achieving optimal postoperative recovery outcomes.
However, current studies indicate suboptimal rehabilitation exercise adherence among post-TKA elderly patients. Research has revealed10,11 that a substantial proportion of patients report persistent pain, unsatisfactory functional recovery, and dissatisfaction with surgical outcomes during extended postoperative periods. Patient-specific factors including individual physical status, exercise-related knowledge deficits, self-efficacy limitations, and postoperative pain management challenges12,13 have been identified as key determinants of rehabilitation efficacy. Under the guidance of evidence-based principles, many existing programs are developed from the top down, mainly through evidence synthesis and expert consultation, without systematically addressing the complex background barriers existing at the care point. These barriers include organizational limitations such as heavy workloads for staff and the unique social and cultural needs of patients. And there is a lack of active participation from all stakeholders (including doctors, nurses and patients themselves) during the implementation process. Therefore, many well-designed protocols have failed to achieve the expected results in actual clinical Settings, indicating that there is still a gap between evidence and practice.
Evidence-based nursing practice revolutionizes conventional care models by integrating best available evidence, clinical expertise, and patient values to drive informed clinical decision-making.14 The complex process of evidence translation necessitates structured theoretical frameworks, with the Knowledge-to-Action (KTA) Process Framework15 developed by Canadian researchers providing a robust implementation roadmap. Domestic and foreign researchers have applied this framework to various studies such as enteral nutrition for critically ill patients16,17 and transformation of clinical nutrition evidence.18 The results show that through multidisciplinary cooperation and combined intervention strategies of multiple approaches, patients can achieve relatively optimistic clinical outcomes.
Therefore, building upon the successful application of the KTA model in other fields, this study employs it to address the evidence-to-practice gap in post-TKA rehabilitation. The novelty of our research, however, extends beyond simply constructing a program. We aim to develop a contextually-tailored functional exercise plan through a rigorous, stakeholder-driven process. Specifically, our study will: (1) integrate multiple evidence dimensions, combining clinical evidence with qualitative data on local barriers, and (2) utilize a co-design approach with active stakeholder engagement to ensure the program’s real-world feasibility. Ultimately, this research seeks to not only construct a comprehensive functional exercise program for elderly patients after TKA but also to preliminarily validate a model for its sustainable implementation in practice.
Materials and Methods
Planned Process: Knowledge to Action Framework
Our study was guided by the Knowledge to Action (KTA) framework and conducted in two phases: knowledge creation and the action cycle, as illustrated in Figure 1.15 During the knowledge creation phase, a systematic literature review, quality appraisal, and evidence synthesis were performed to produce comprehensive, clear, and reader-friendly recommendations. In this phase, the process involves synthesizing multiple types of evidence, including clinical decision support systems, clinical guidelines, and expert consensus statements.19,20 When necessary, we retrieve original research studies to ultimately generate the best available evidence relevant to our research topic. The registration number of this stage of research at the Evidence-Based Nursing Center of Fudan University is: ES20220732. In the action cycle phase, the KTA model guided the entire process, encompassing the identification of problems, selection of appropriate knowledge resources, adaptation of knowledge to specific contexts, evaluation of potential barriers, monitoring of implementation, assessment of outcomes, and maintenance of knowledge use. At this stage, the expert meeting was employed to adapt the preliminary intervention program to the local context. Qualitative methods were used to identify barriers and facilitators in implementing the evidence-based program. Finally, quantitative methods were applied for preliminary implementation and monitoring of the rehabilitation exercise program’s effectiveness.
 |
Figure 1 Knowledge-to-Action Process. |
Phase 1: Knowledge Creation
An interdisciplinary evidence-based practice team comprising eight members was established, including one chief orthopedic surgeon, one chief nurse specializing in rehabilitation nursing research, one orthopedic surgeon, one exercise rehabilitation expert, one specialty nurse with 20 years of clinical experience, and two postgraduate students.
Literature Search
The literature search was conducted following the “6S” evidence pyramid model, adhering to a top-down approach. Databases searched included UpToDate, Guidelines International Network, National Institute for Health and Care Excellence, Cochrane Library, Joanna Briggs Institute, Embase, Web of Science, Pubmed, China National Knowledge Infrastructure. The search terms included “elderly”, “total knee replacement/total knee arthroplasty”, “exercise therapy/motor activity/early rehabilitation/exercise training/physical activity”, etc. The detailed search strategy and the number of articles retrieved from each database are provided in Supplementary file 1.
Inclusion and Exclusion Criteria for Literature
Inclusion Criteria: (1) The study population consisted of elderly patients undergoing total knee arthroplasty. (2) The study must include postoperative functional exercise components. (3) The study type should be clinical decisions, guidelines, consensus, evidence summaries, systematic reviews, meta-analyses, or randomized controlled trials (RCTs).
Exclusion Criteria: (1) Non-Chinese and non-English literature; (2) Full-text articles not available; (3) Documents such as interpretations, plans, drafts, etc.
Literature Quality Assessment and Evidence Extraction
The critical appraisal for summaries of evidence, AGREE II,21 and the JBI Evidence-Based Healthcare Center’s quality assessment tools were used to evaluate the literature.22 Additionally, two researchers, trained in evidence-based nursing systems, independently extracted relevant evidence. The translation and integration of the evidence were collaboratively discussed and finalized by the research team.
Phase 2: Knowledge Application
Integration of Evidence into Clinical Context
After discussion within the research group, the generated evidence was introduced into the clinical setting through expert meetings to preliminarily formulate a draft of the functional exercise intervention program. Invited experts included clinical specialists in orthopedics, clinical nurses, rehabilitation nurses, and nursing administrators.
Analysis of Barriers
A qualitative study was conducted to identify potential barriers and facilitators perceived by stakeholders (patients and healthcare professionals) in implementing the evidence. Interviews were conducted until data saturation was reached. The interview guide for healthcare professionals included the following questions: (1) How do you perceive the current status of functional exercises for patients following TKA? (2) In your daily practice, how do you recommend functional exercises to patients post-TKA? (3) Could you describe your understanding of evidence related to functional exercises post-TKA? (4) What factors do you think hinder evidence-based practice of functional exercises for post-TKA elderly patients? (5) What factors do you think facilitate the successful implementation of evidence-based practice for functional exercises in elderly patients undergoing TKA?
The interview guide for patients included: (1) Do you think postoperative functional exercise is important/not important to you? (2) Could you describe your feelings during functional exercises? (3) What factors do you think affect your postoperative functional exercises? (4) How do you perceive the guidance provided by healthcare professionals for your postoperative functional exercises? (5) Do you communicate problems encountered during your exercises with healthcare professionals? (6) Regarding your current functional exercise status, do you have any needs or suggestions?
A semi-structured interview23 with open-ended questions was deliberately employed to encourage participants to provide rich, detailed narratives of their experiences and perceptions, rather than limiting their responses to preconceived categories. Follow-up probing questions were used to explore emergent themes in greater depth. Interview data were transcribed within 24 hours after completion and analyzed using Colaizzi’s seven-step analytical approach:24 (1) Repeatedly reading the interview transcripts; (2) Extracting significant statements; (3) Coding key information; (4) Aggregating coded information; (5) Describing detailed information; (6) Developing overarching themes; (7) Returning to participants for verification of uncertain points.
Selection and Tailoring of Interventions
A temporary on-site meeting was held in the learning room of the department where the practice was carried out. Through the form of brainstorming, the initially constructed plan and obstacle factors were discussed, and the intervention plan was selected, tailored and improved. Finally, the final draft of the evidence-based practice plan for rehabilitation exercise after TKA was formed.
Monitoring Knowledge Application and Outcomes
A quasi-experimental study design was adopted to monitor the application and effectiveness of the knowledge intervention. This trial was conducted from August 31 to December 31, 2023, in the orthopedic wards of a tertiary general hospital in China. Wards were divided into intervention and control groups based on their location relative to the nursing stations to minimize interference between groups. Physicians and nurses involved in the wards were aware of an ongoing intervention study but were blinded to the specifics of group assignments and intervention details. The study was conducted in accordance with the Declaration of Helsinki and was approved by the Medical Ethics Committee of Mindong Hospital in Ningde City and the audit of the Chinese Clinical Trial Registration Center (Registration number: ChiCTR2500100693). Participants were fully informed about the study, provided informed consent, and participated anonymously. The consent form explicitly stated that anonymized responses and direct quotes could be used in publications.
Participants
Inclusion Criteria: (1) Patients meeting diagnostic criteria for knee osteoarthritis; (2) Age ≥ 60 years; (3) First-time unilateral total knee arthroplasty recipients; (4) Capable of unimpeded communication.
Exclusion Criteria: (1) Secondary KOA patients; (2) Concurrent hip/knee replacement recipients; (3) Comorbid conditions affecting limb mobility; (4) Comorbid major organ dysfunction (cardiac, pulmonary, or cerebral) or malignancy; (5) History of lower extremity venous thrombosis or primary thrombotic disorders.
Sample Size Calculation: Using the Hospital for Special Surgery Knee Score (HSS) as the primary outcome measure, with a 1:1 allocation ratio between intervention and control groups, sample size was calculated via the formula:25 N1 = N2 = (2σ2(Z_α+Z_β)2)/δ2. In this example, bilateral test is adopted, and the test level is specified as α = 0.05, β = 0.10. The test efficiency is 1-β = 0.90, so Zα= 1.96 and Zβ = 1.282 are obtained by looking up the table According to the reference,26 the above formula was substituted to calculate that N1 = N2 = 27, and considering the loss rate of 15%, there were 32 cases in the experimental group and 32 cases in the control group.
Procedures
Control Group
The control group received standard orthopedic nursing care and functional exercise, which included the following components: (1) Upon admission, patients were provided with orientation education to familiarize them with the hospital environment and alleviate any anxiety; (2) Preoperatively, patients were guided on dietary preparation, personal item management, skin hygiene, and functional exercise techniques; (3) After surgery, patients were instructed to elevate the affected limb and apply ice for swelling control upon returning to the ward; (4) Postoperatively, verbal instructions were given for bed exercises, including ankle pump exercises, quadriceps contractions, straight leg raises, and knee flexion exercises; (5) Nurses demonstrated the proper use of assistive devices and provided guidance for out-of-bed activities; (6) Discharge instructions were provided, which included information on functional exercises and the daily maintenance of prosthetic devices, with a reminder for regular follow-up visits to the clinic.
Intervention Group
On the basis of routine care, combine the evidence-based practice plan of rehabilitation exercise after TKA. Following a comprehensive baseline assessment, a personalized in-hospital and post-discharge exercise regimen was formulated for each patient. The exercise protocol specified the timing, frequency, intensity and type of activities, commencing post-anesthesia with ankle pumps. The regimen progressed systematically: postoperative day one included isometric quadriceps/hamstring contractions, straight leg raises, and assisted gait training. Day two focused on achieving ≥90° knee flexion, followed by resistance training with elastic bands on day three. Prescribed frequency was typically 3–5 times daily for strengthening and 1–2 times daily for flexion, adjusted to patient tolerance. The plan included a comprehensive discharge component, emphasizing at least eight weeks of continued exercise and providing resources like videos and options for remote or supervised outpatient rehabilitation. The complete plan is detailed in Table 1.
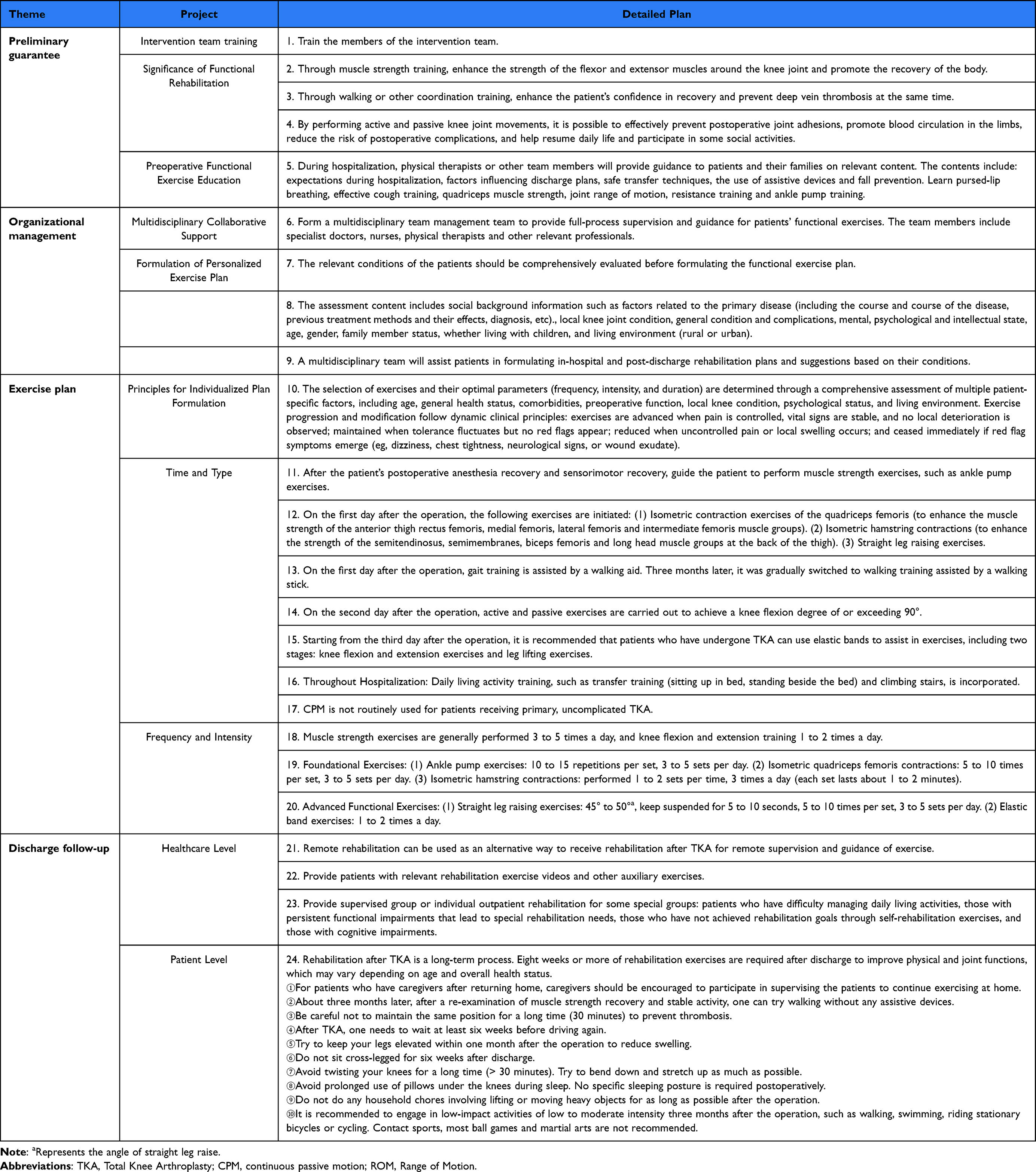 |
Table 1 Evidence-Based Practice Plan for Functional Exercise in Elderly Patients After TKA |
Measurements
Demographic Data
The general demographic data of the two patient groups were collected, including gender, age, height, weight, body mass index (BMI), educational level, employment status, marital status, type of medical insurance, monthly household income, medical history, surgical site, and primary caregiver after discharge.
Observation Indicators
Knee Joint Function
The knee joint function was evaluated using the Hospital for Special Surgery Knee Score (HSS) of the United States.27 The HSS scoring system mainly consists of pain degree, functional status, range of motion, muscle strength, flexion deformity, stability and deduction items. Among them, the use of assistive walking tools, knee flexion contracture deformity and valgus deformity are the items that can be deducted points. The total score is classified into four levels: a score above 85 is considered excellent. 70 to 84 is considered good, and 60 to 69 is considered medium. Less than 60 points is the difference.
Range of Motion of the Knee Joint
Joint range of motion refers to the maximum range of motion that a joint can achieve, which reflects the flexibility and range of motion of the joint. The ROM of the knee joint is determined by measuring the maximum Angle reached by the knee during flexion (bending) and extension (straightening).
Pain
The degree of pain in patients with knee osteoarthritis was evaluated using the Visual Analogue Scale (VAS).28 The method was to draw a 10-centimeter straight line on a piece of paper. The left end (0 points) indicated no pain, and the right end (10 points) indicated extreme pain. Patients marked their pain levels on the scale based on their actual feelings: 0 points for no pain, 1 to 3 points for mild pain that is tolerable, 4 to 6 points for moderate but controllable pain, and 7 to 10 points for severe pain that is unbearable.
Evaluation Timing
The knee joint function was evaluated by this scale one day before the operation and one month after the operation. Pain and knee joint range of motion were evaluated and recorded 1 day before the operation, 7 days after the operation, and 1 month after the operation.
Quality Control
(1) Before the official implementation, the intervention team was trained, and the tasks of the group members and their respective divisions of labor were relatively clear.
(2) Supervision was conducted by the researcher himself/herself and the nursing leaders of the department during the implementation period. The nursing leaders of the department asked questions to the nursing staff and conducted bedside checks on the patients’ knowledge of functional exercise and the progress of exercise twice a day.
(3) Intervention implementation process: Based on evidence-based clinical evidence, the FAME principle of evidence evaluation was applied to formulate quality review indicators for feasibility (F), appropriateness (A), significance (M), and effectiveness (E).29 A total of 17 review indicators were formulated, and the review objects and methods were determined for each one, as shown in Table 2.
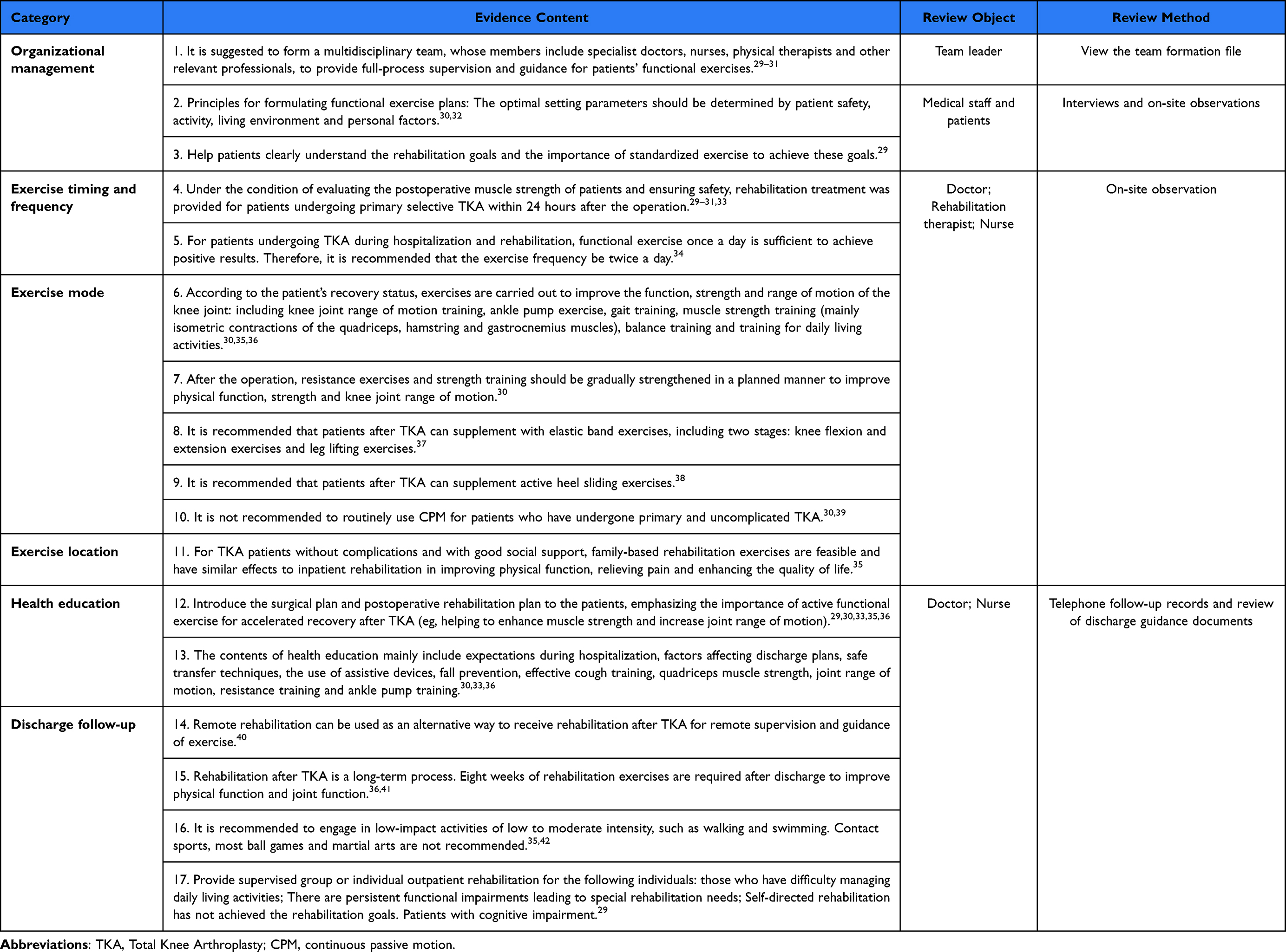 |
Table 2 Review Items and Methods of Functional Exercise for Elderly Patients After TKA |
Data Analysis
The baseline data and outcome indicator data of the research subjects were entered by two people and cross-checked for accuracy. The statistical analysis of the data was conducted using SPSS 26.0 software. The measurement data conforming to the normal distribution were expressed as mean ± standard deviation ( ) and the comparison between the two groups was analyzed using the two independent sample t-test; If the normal distribution is not satisfied, it is expressed as the median and interquartile range [M (P25-P75)], and analyzed using the Mann–Whitney U-test. Counting data were expressed as frequency and composition ratio [n (%)], and the χ2 test or Fisher’s exact test was used. The difference was statistically significant when P < 0.05. Repeated measures analysis of variance was performed when the measurement data conformed to a normal distribution and had uniform variances. If not, the generalized estimating equation was used.
) and the comparison between the two groups was analyzed using the two independent sample t-test; If the normal distribution is not satisfied, it is expressed as the median and interquartile range [M (P25-P75)], and analyzed using the Mann–Whitney U-test. Counting data were expressed as frequency and composition ratio [n (%)], and the χ2 test or Fisher’s exact test was used. The difference was statistically significant when P < 0.05. Repeated measures analysis of variance was performed when the measurement data conformed to a normal distribution and had uniform variances. If not, the generalized estimating equation was used.
Results
Phase 1: Knowledge Creation
As shown in Table 2, through preliminary searches, 3550 articles were identified. After step-by-step screening, 14 articles were eventually included, consisting of 1 clinical decision,30 2 guidelines,31,32 3 evidence summaries,33–35 3 systematic reviews,36–38 2 randomized controlled trials,39,40 and 3 expert consensuses.41–43 Analysis, collation, and synthesis of the extracted evidence resulted in 17 recommendations categorized into six domains: organizational management, timing and frequency of exercise, methods of exercise, locations for exercise, health education, and discharge follow-up.
Phase 2: Knowledge Application
Introducing Evidence into Clinical Context——Expert Meetings
A total of 16 experts were invited, comprising specialists in orthopedic surgery, clinical nursing, rehabilitation nursing, and nursing management. Experts ranged in age from 30 to 50 years, with an average age of 39.1 years and an average work experience of 15.5 years. The retrieved evidence was reviewed, modified, deleted, or supplemented through discussion and brainstorming at the meeting, resulting in an initial draft program that covered four main areas: preliminary assurance, organizational management, exercise program, and discharge follow-up.
Analysis of Barriers——Qualitative Research
We interviewed 7 healthcare providers (5 females, 71.4%; 2 males, 28.6%) and 8 patients (5 females, 62.5%; 3 males, 37.5%). Thematic analysis of the interview data revealed three primary categories of barriers: (1) Systemic and Evidence-Related Barriers, (2) Provider-Related Barriers, and (3) Patient-Related Barriers.
Systemic and Evidence-Related Barriers
Barriers at the systemic and evidence level were twofold. First, some evidence-based recommendations were impractical for local clinical settings, particularly international guidelines misaligned with the Chinese context. Second, significant resource constraints, including high workloads, staffing shortages, and a lack of dedicated space or equipment, severely limited the providers’ capacity for patient education.
Knee recovery is a long process, and exercises after returning home are crucial, but supervising the outcomes is difficult.
Does ‘home rehabilitation’ mean patients go home immediately after surgery.? Most patients here are elderly from rural areas. Communication and supervision are challenging.
Sometimes we perform over ten surgeries daily. We have limited energy for repeatedly guiding patients on exercises.
We lack auxiliary exercise tools. For example, our department doesn’t have elastic bands for patient exercises.
Provider-Related Barriers
Interviews with healthcare providers, who are key to patient guidance, revealed specific professional barriers. Physicians exhibited limited awareness of the evidence’s importance, while nurses expressed concerns about the increased workload and the need for specialized knowledge regarding the exercise programs.
I think surgical technique is paramount; these exercises might only serve an auxiliary purpose.
New evidence seems to significantly increase our clinical workload. We are already short-staffed.
Many patients we see are elderly from rural areas. They might not understand or remember the exercises we recommend.
Patient-Related Barriers
Patient-level barriers were both physical and psychosocial. Physically, acute postoperative pain and swelling were primary deterrents to exercise participation. Psychosocially, this was compounded by a lack of knowledge, low self-efficacy, and a need for more professional guidance, which collectively fueled fears of harm and uncertainty about the rehabilitation process.
The first two or three days after surgery, especially around the incision, were quite painful, making me reluctant to move much.
…after the pain pump was removed, moving became very painful, and my foot was very swollen.
Sometimes I don’t understand why holding a movement for a few seconds is necessary. Isn’t just moving around enough?
I might need more guidance for exercises at home. I’m unsure.
Movement causes pain, and my knee won’t bend easily. I’m worried bending it might damage the prosthetic.
Yesterday, I walked around, maybe too much. Today my leg hurts. Did the surgery fail? Should I have stayed in bed?
Based on the above interview results, the members of the research group, through discussion, analyzed the possible obstacles to the application of evidence from the organizational level, the practitioner level, and the patient level, and formulated change strategies (Table 3).
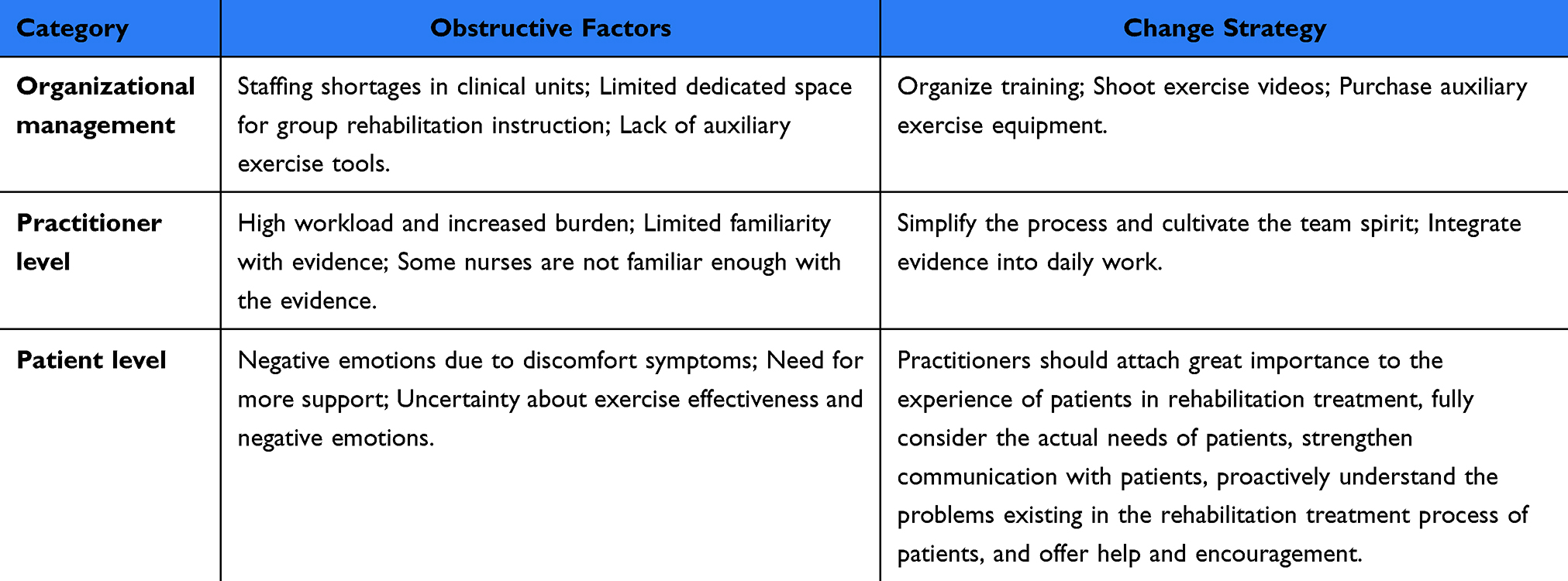 |
Table 3 Obstructive Factors and Reform Strategies of Functional Exercise for Elderly Patients After TKA |
Select and Tailor Intervention Measures - On-Site Meeting
As shown in Table 1, through on-site discussion meetings held in the practical departments, the initially formed intervention plan, the obstructive factors in the qualitative research, and the formulated action strategies were explored. The suitability and clinical feasibility of the plan were evaluated, and finally a clinical practice plan suitable for functional exercise of elderly patients after TKA was constructed.
Monitor the Application and Effect of Knowledge——Quasi-Experimental Study
Study Characteristics
This stage of the study was completed in the Department of Joint Surgery and Sports Medicine of a tertiary hospital from September 2023 to December 2023. A total of 64 patients who underwent unilateral TKA were included, with 32 cases in the experimental group and 32 cases in the control group. During the research process, one case in the control group was excluded on the day of the operation when the family members temporarily decided to cancel the operation after multiple considerations. In the experimental group, one patient had skin ulceration on the day of the operation and was eliminated after the operation was cancelled. One patient was also eliminated after repeated discussions between the patient and the family on the same day of the operation and it was decided to cancel the operation. One patient had part of the uncooperative plan fall off. Therefore, a total of 60 patients were finally included in the study, with 29 in the experimental group and 31 in the control group.
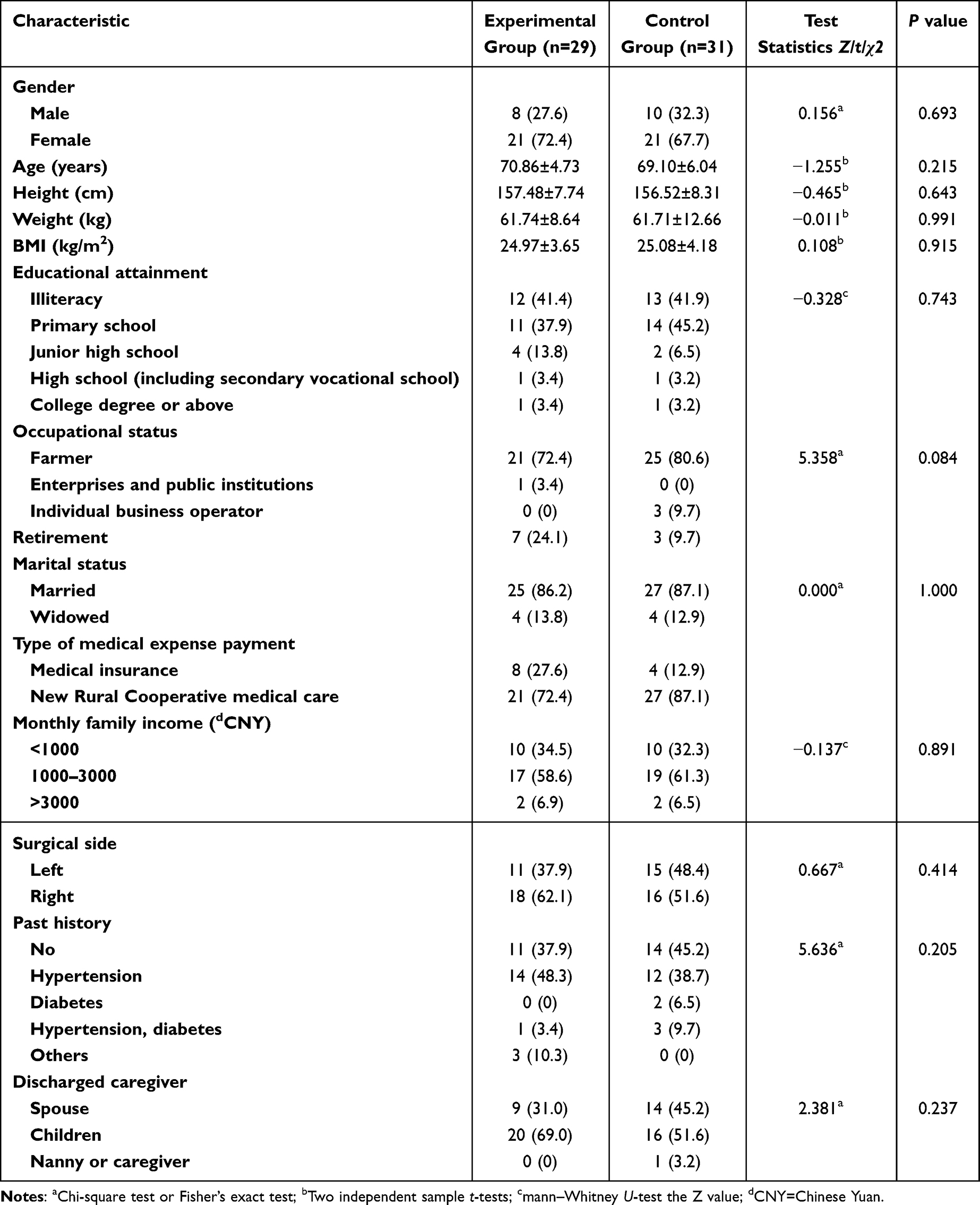
As shown in Table 4, there were no statistically significant differences between the two groups in key demographic data (P > 0.05). As shown in Table 5, Furthermore, the baseline values of the primary outcome measures, including HSS, VAS, and ROM scores, also showed no significant between-group differences at enrollment (P > 0.05). This indicates that despite the quasi-experimental design, the two groups were largely comparable on both demographic and key clinical variables at baseline.
 |

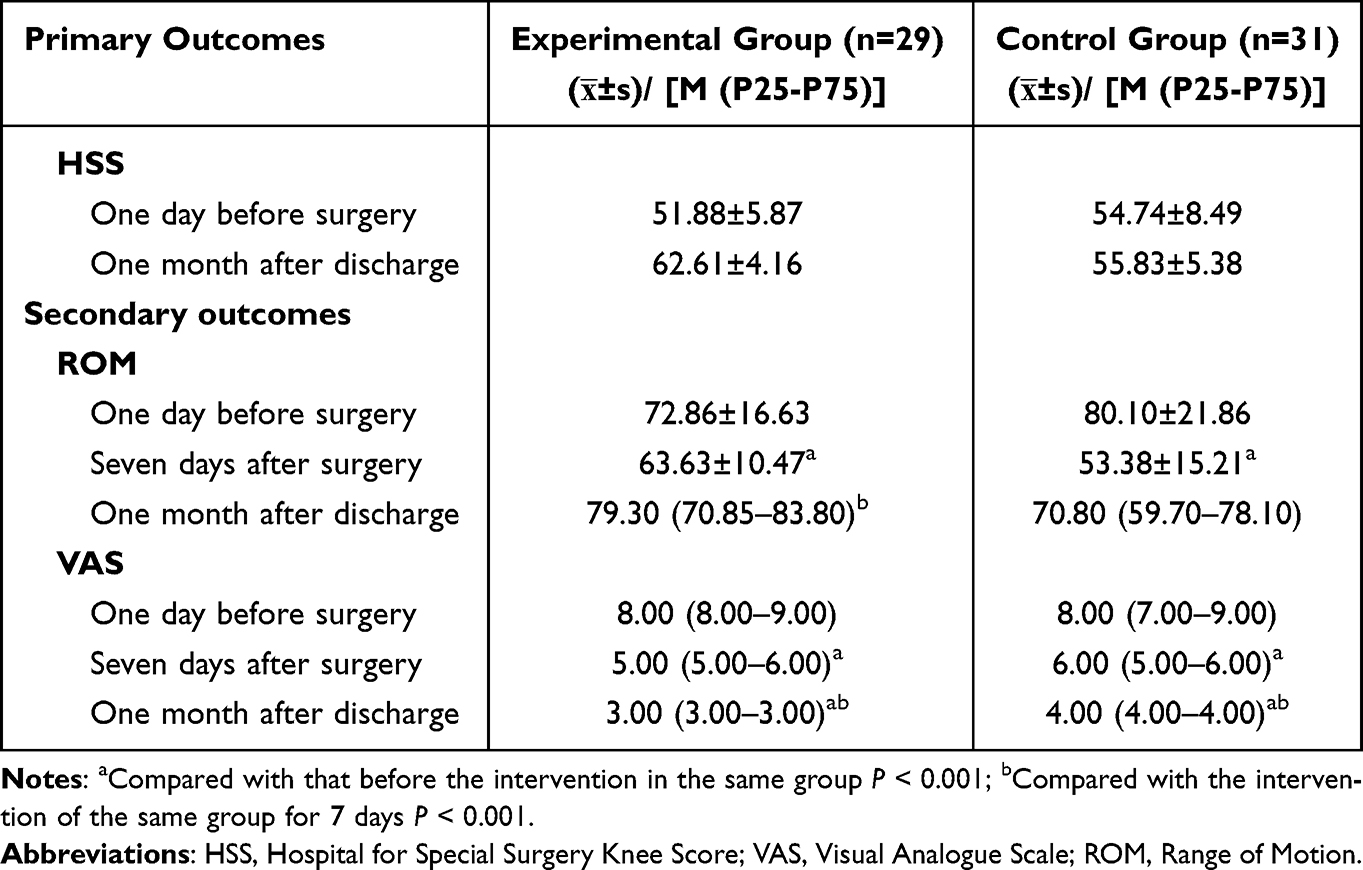 |
Table 5 Comparison of Outcome Indicators Between the Two Groups of Patients |
Primary Outcomes
As shown in Table 5 and Figure 2, the comparison results of the knee joint function status of the two groups of patients before and after the intervention showed that the score of the experimental group was higher than that of the control group, and the difference was statistically significant (P<0.05).
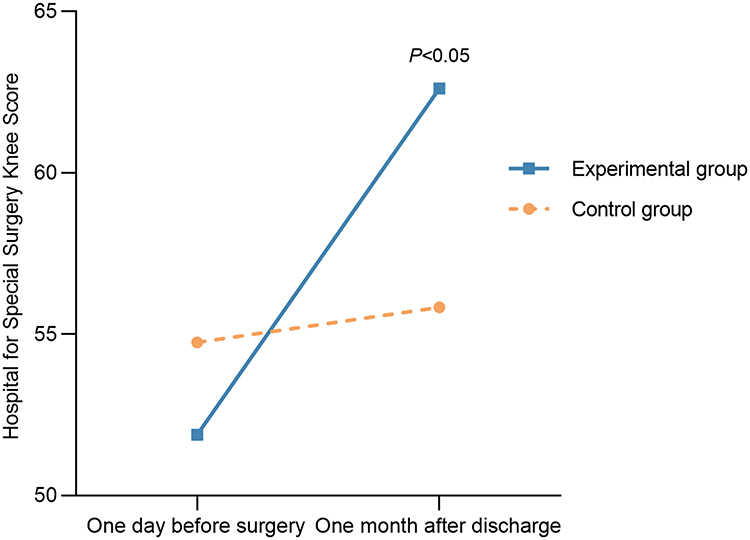 |
Figure 2 The scores of knee joint function before and after the intervention. |
Secondary Outcomes
Knee range of motion outcomes are presented in Table 5 and Figure 3. Generalized Estimating Equation analysis revealed a significant Group-by-Time interaction (Waldχ2 = 12.10, P = 0.002) and a main effect of Time (Waldχ2 = 145.85, P < 0.001), but no main effect of Group (Waldχ2 = 1.241, P = 0.265). This significant interaction indicates that the trajectory of ROM change over the follow-up period differed between the two groups. To further explore this interaction, pairwise comparisons were conducted at each time point. While no significant between-group difference was observed at enrollment, the experimental group exhibited significantly higher ROM than the control group at both 7 days and 1 month postoperatively (P < 0.05).
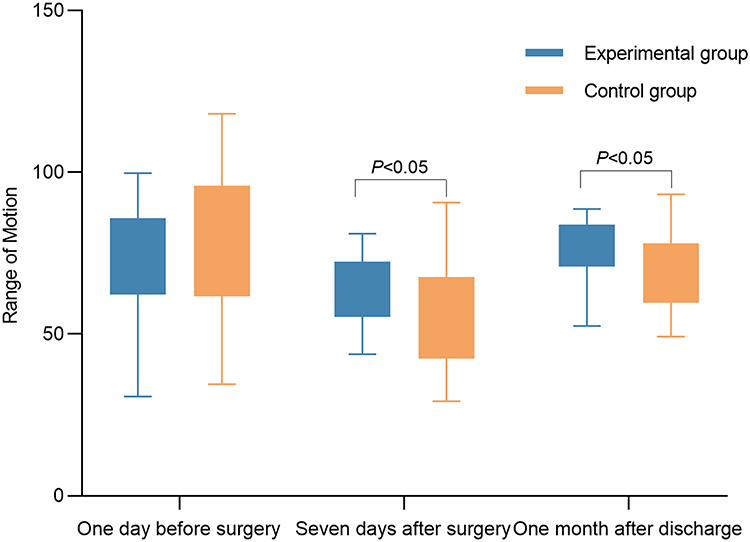 |
Figure 3 Scores of knee joint range of motion before and after the intervention. |
As shown in Table 5 and Figure 4, VAS scores did not differ significantly between groups at enrollment. However, the experimental group demonstrated significantly lower VAS scores than the control group at both 7 days and 1 month postoperatively (P < 0.05). Generalized estimating equation analysis revealed a statistically significant effect of Group (Waldχ2 = 8.159, P = 0.004), indicating that pain scores differed based on the intervention received. A significant effect of Time was also observed (Waldχ2 = 1937.782, P < 0.001), signifying changes in pain scores over time within both groups. Furthermore, the Group-by-Time interaction effect was significant (Waldχ2 = 39.038, P < 0.001), indicating that the pattern of change over time differed between the groups.
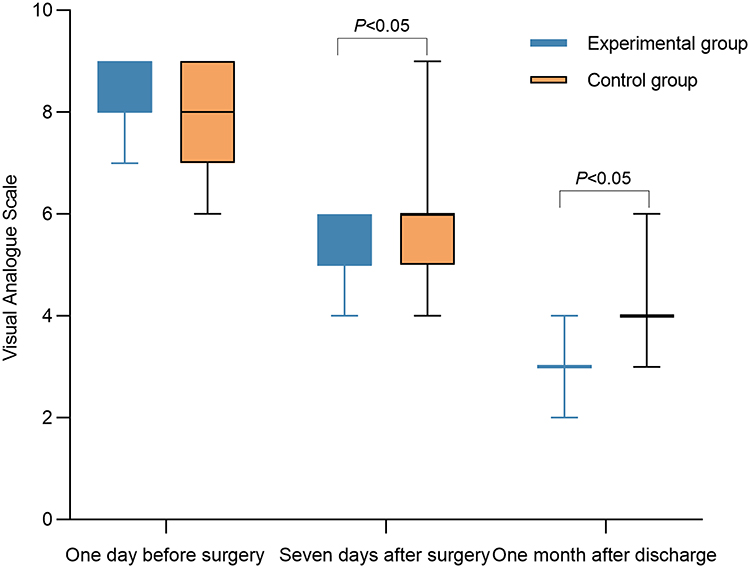 |
Figure 4 Pain scores before and after the intervention. |
Discussion
In this study, we applied the KTA framework to guide the development and implementation of an evidence-based postoperative functional exercise program for elderly patients undergoing TKA. Through interviews with patients and healthcare professionals, we identified key challenges, including patient fear of pain, poor post-discharge adherence, and staff constraints. Aligned with prior implementation studies, these findings highlight recurrent obstacles in evidence-based rehabilitation.44–46 Subsequently, we developed and implemented targeted strategies to address these specific barriers: stakeholder co-design sessions were convened to tailor the intervention, focused training was delivered to staff, and multidisciplinary follow-up was instituted to ensure continuity. The successful execution of this systematic, problem-oriented implementation process was then evaluated. Our findings suggest that the resulting program was associated with improved early recovery outcomes, including enhanced knee function, reduced pain intensity, and increased range of motion.
A key strength of this implementation-focused approach is its adaptability to specific healthcare contexts, such as that of China. While our program was developed by integrating international guidelines, the KTA framework guided its tailoring to local realities. For instance, the emphasis on a multidisciplinary team (MDT) approach is a pragmatic solution to the common constraint of limited, specialized rehabilitation staff in many Chinese hospitals; by integrating specialist doctors, nurses, and available therapists into a coordinated workflow, our model optimizes existing human resources. This MDT would then prescribe exercises in short, manageable sessions (3–5 times per day) rather than a single long session, a method better suited to the tolerance levels of elderly patients and easier to integrate into their daily routines. Furthermore, the program’s strong focus on structured patient education and a detailed post-discharge plan is designed to mitigate challenges such as high patient volume and the heavy reliance on family support for at-home recovery. For example, patients and their caregivers were given access to a series of short instructional videos via WeChat, demonstrating the correct form for each exercise. This approach empowers both patients and their families to manage rehabilitation more independently. To ensure continuity and address issues promptly, a structured follow-up was instituted, often involving a designated nurse conducting a weekly follow-up call or WeChat message exchange during the first month post-discharge to monitor progress and answer questions. This is vital given the constraints on formal outpatient follow-up services in many regions.
Clinically, our data reaffirm that targeted, early exercise initiation is a key component of successful TKA recovery. The statistically significant group differences in HSS scores favor the experimental group, suggesting enhanced functional recovery. These functional benefits likely signify improved joint stability and muscle strength.47 This finding is consistent with research reporting that intensive postoperative rehabilitation can enhance early performance and mobility.48
Consistent with previous research, our findings underscore the importance of early rehabilitation for optimizing knee ROM, a key marker for long-term recovery.48–50 A pivotal finding was the significant Group-by-Time interaction for ROM, which, in the absence of a main group effect, suggests the intervention’s primary influence was on the trajectory of early recovery. This was evidenced by superior outcomes at 7 days and 1 month. While the lack of a main effect may be due to both groups approaching a similar functional plateau, these accelerated early gains may hold clinical promise for facilitating earlier mobilization and mitigating complication risks. A systematic review and meta-analysis found that patient education interventions, particularly those incorporating information technology devices, significantly enhance postoperative ROM and pain management in TKA patients.51 This convergence with technology-supported education studies further validates combining structured exercises with patient-centered learning tools.
Beyond mobility, effective pain management is a cornerstone of early recovery, as uncontrolled postoperative pain is a well-established barrier to mobilization and functional gains.52 Our multimodal pain strategy—pharmacologic analgesia, structured education, and psychological support—yielded significantly lower VAS scores at days 7 and 30. This agrees with Jin et al,53 who found that combining pain relief with motivational techniques enhances recovery. Thus, integrating pharmacologic and psychosocial interventions may help in overcoming pain-related barriers. By incorporating psychological support, our program likely not only reduced pain perception but also eased anxiety, thereby enhancing patient engagement. This underscores the value of a biopsychosocial approach, recognizing that emotional well-being is intrinsically linked to functional recovery, particularly in the post-TKA population where psychological factors like anxiety can hinder progress.53–55 Consequently, our study supports integrating pain management and engagement strategies into rehab protocols to maximize outcomes.
Clinicians should prioritize early mobilization—initiating targeted exercises within days of surgery—alongside comprehensive pain and psychosocial support to promote adherence and support early recovery. Emphasizing patient education and scheduled follow-up visits helps maintain exercise compliance and address individual challenges. While patient responses vary, the structured, patient-centered framework presented here offers a practical and scalable model for routine TKA rehabilitation. Future work could leverage data-driven methods, such as machine learning, to prospectively identify patients at high risk for poor recovery.56 Another promising direction involves integrating such predictive modeling with molecular-level patient data57 and complementary physiological interventions (eg, targeted nutritional support)58 to develop highly precise, multimodal rehabilitation pathways.
Limitations
This single-center, quasi-experimental study used ward-based allocation, introducing potential selection bias and a clustered data structure; although baseline characteristics were comparable, unmeasured confounding (eg, variation in nursing care) cannot be excluded. The initial sample size did not account for intracluster correlation, likely inflating power and limiting precision for smaller effects; findings should therefore be interpreted as associative and preliminary rather than causal. Outcomes were restricted to early postoperative recovery, precluding conclusions about medium- or long-term trajectories, durability of benefit, or full functional reintegration. Qualitative insights were self-reported by patients and staff and may be affected by recall and social desirability biases, potentially underdetecting latent implementation barriers. Despite these limitations, the KTA-guided, evidence-based exercise programme showed feasibility and clinically meaningful signals in pain control, range of motion, and function. Future multicentre, cluster-randomised trials with ICC-adjusted sample sizes, extended follow-up and cost-effectiveness analyses—alongside tele-rehabilitation and data-driven risk stratification—are needed to confirm effectiveness, generalisability, and sustainability. Ultimately, systematic evidence translation strategies, such as those employed here, are vital to advancing the quality and effectiveness of orthopedic rehabilitation practice.
Conclusions
This study systematically integrates the rehabilitation evidence after TKA in the past 10 years and constructs an evidence-based practice program covering organizational management, resource coordination, personalized exercise, health education and continuous care. The application of this structured program was associated with preliminary improvements in patients’ knee joint function and range of motion, and suggested a reduction in postoperative pain. It is important to note that these outcomes were measured only up to one month postoperatively, and therefore do not capture potential medium- or long-term effects on recovery or quality of life. Consequently, while the program provides a practical and operational framework for clinical transformation, the findings on its efficacy should be considered exploratory. This work offers a promising basis for optimizing TKA rehabilitation, warranting further investigation through larger, controlled trials with extended follow-up periods.
Disclosure
The authors declare no competing interests.
References
1. Tang S, Zhang C, Oo WM, et al. Osteoarthritis. Nat Rev Dis Primers. 2025;11(1):10. doi:10.1038/s41572-025-00594-6
2. Mora JC, Przkora R, Cruz-Almeida Y. Knee osteoarthritis: pathophysiology and current treatment modalities. J Pain Res. 2018;11:2189–2196. doi:10.2147/JPR.S154002
3. Safiri S, Kolahi AA, Smith E, et al. Global, regional and national burden of osteoarthritis 1990-2017: a systematic analysis of the global burden of disease study 2017. Ann Rheum Dis. 2020;79(6):819–828. doi:10.1136/annrheumdis-2019-216515
4. Ighani Arani P, Wretenberg P, Ottosson J, W-Dahl A. Pain, function, and satisfaction after total knee arthroplasty, with or without bariatric surgery. Obes Surg. 2022;32(4):1164–1169. doi:10.1007/s11695-022-05912-5
5. Price AJ, Alvand A, Troelsen A, et al. Knee replacement. Lancet. 2018;392(10158):1672–1682. doi:10.1016/S0140-6736(18)32344-4
6. Schwartz AM, Farley KX, Guild GN, Bradbury TL. Projections and epidemiology of revision hip and knee arthroplasty in the United States to 2030. J Arthroplasty. 2020;35(6S):S79–S85. doi:10.1016/j.arth.2020.02.030
7. Fortier LM, Rockov ZA, Chen AF, Rajaee SS. Activity recommendations after total hip and total knee arthroplasty. J Bone Joint Surg. 2021;103(5):446–455. doi:10.2106/JBJS.20.00983
8. Kilgas MA, DenHerder AE, Lytle LLM, Williams CT, Elmer SJ. Home-based exercise with blood flow restriction to improve quadriceps muscle and physical function after total knee arthroplasty: a case report. Phys Ther. 2019;99(11):1495–1500. doi:10.1093/ptj/pzz110
9. Lisi C, Caspani P, Bruggi M, et al. Early rehabilitation after elective total knee arthroplasty. Acta Biomed. 2017;88(4S):56–61. doi:10.23750/abm.v88i4-S.5154
10. Wieczorek M, Rotonda C, Guillemin F, Rat AC. What have we learned about the course of clinical outcomes after total knee or hip arthroplasty? Arthritis Care Res. 2020;72(11):1519–1529. doi:10.1002/acr.24045
11. Gunaratne R, Pratt DN, Banda J, Fick DP, Khan RJK, Robertson BW. Patient dissatisfaction following total knee arthroplasty: a systematic review of the literature. J Arthroplasty. 2017;32(12):3854–3860. doi:10.1016/j.arth.2017.07.021
12. Olsen U, Lindberg MF, Rose C, et al. Factors correlated with physical function 1 year after total knee arthroplasty in patients with knee osteoarthritis: a systematic review and meta-analysis. JAMA Network Open. 2022;5(7):e2219636. doi:10.1001/jamanetworkopen.2022.19636
13. Olsen U, Sellevold VB, Gay CL, et al. Factors associated with pain and functional impairment five years after total knee arthroplasty: a prospective observational study. BMC Musculoskelet Disord. 2024;25(1):22. doi:10.1186/s12891-023-07125-y
14. Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn’t. BMJ. 1996;312(7023):71–72. doi:10.1136/bmj.312.7023.71
15. Graham ID, Logan J, Harrison MB, et al. Lost in knowledge translation: time for a map? J Contin Educ Health Prof. 2006;26(1):13–24. doi:10.1002/chp.47
16. Cahill NE, Heyland DK. Bridging the guideline-practice gap in critical care nutrition: a review of guideline implementation studies. JPEN J Parenter Enteral Nutr. 2010;34(6):653–659. doi:10.1177/0148607110361907
17. Cahill NE, Murch L, Cook D, Heyland DK; Canadian Critical Care Trials Group. Improving the provision of enteral nutrition in the intensive care unit: a description of a multifaceted intervention tailored to overcome local barriers. Nutr Clin Pract. 2014;29(1):110–117. doi:10.1177/0884533613516512
18. Murphy JL, Holmes J, Brooks C. Nutrition and dementia care: developing an evidence-based model for nutritional care in nursing homes. BMC Geriatr. 2017;17(1):55. doi:10.1186/s12877-017-0443-2
19. Munn Z, Lockwood C, Moola S. The development and use of evidence summaries for point of care information systems: a streamlined rapid review approach. Worldviews Evid Based Nurs. 2015;12(3):131–138. doi:10.1111/wvn.12094
20. Khangura S, Konnyu K, Cushman R, Grimshaw J, Moher D. Evidence summaries: the evolution of a rapid review approach. Syst Rev. 2012;1(1). doi:10.1186/2046-4053-1-10
21. Brouwers MC, Kho ME, Browman GP, et al. AGREE II: advancing guideline development, reporting and evaluation in health care. CMAJ. 2010;182(18):E839–842. doi:10.1503/cmaj.090449
22. The Joanna Briggs Institute. JBI Critical Appraisal Tools. 2025. Available from: https://jbi.global/critical-appraisal-tools.
23. Morrissey D, Cotchett M, Said J’Bari A, et al. Management of plantar heel pain: a best practice guide informed by a systematic review, expert clinical reasoning and patient values. Br J Sports Med. 2021;55(19):1106–1118. doi:10.1136/bjsports-2019-101970
24. Colaizzi PF. Psychological research as the phenomenologist views it. In: Valle RS, King M, editors. Existential- Phenomenological Alternatives for Psychology. Vol. 6. Oxford University Press; 1978.
25. Shi Z. Statistics of Traditional Chinese Medicine and Software Application. China Press of Traditional Chinese Medicine; 2017.
26. Zhang Y. Construction and Application of Rehabilitation Exercise Mode for Total Knee Arthroplasty Patients Based on IMB. Qingdao University; 2023; doi:10.27262/d.cnki.gqdau.2022.001585
27. Insall JN, Dorr LD, Scott RD, Scott WN. Rationale of the knee society clinical rating system. Clin Orthop Relat Res. 1989;248(248):13–14. doi:10.1097/00003086-198911000-00004
28. Reginster JY, Deroisy R, Rovati LC, et al. Long-term effects of glucosamine sulphate on osteoarthritis progression: a randomised, placebo-controlled clinical trial. Lancet. 2001;357(9252):251–256. doi:10.1016/S0140-6736(00)03610-2
29. Buccheri RK, Sharifi C. Critical appraisal tools and reporting guidelines for evidence-based practice. Worldviews Evid Based Nurs. 2017;14(6):463–472. doi:10.1111/wvn.12258
30. Martin M, Harris IA. Total knee arthroplasty. Available from: http://update.0000.tsg211.com/contents/total-knee-arthroplasty?search=Total%20knee%20arthroplasty&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1.
31. Excellence NI for H and C. Joint replacement (primary): hip, knee and shoulder. 2020. Available from: https://www.nice.org.uk/guidance/ng157.
32. Jette DU, Hunter SJ, Burkett L, et al. Physical therapist management of total knee arthroplasty. Phys Ther. 2020;100(9):1603–1631. doi:10.1093/ptj/pzaa099
33. Slade S. Hip and knee arthroplasty: acute in-patient rehabilitation. 2022.
34. Moola S, Long KDL. Total knee arthroplasty: continuous passive motion. 2021. Available from: http://ovidsp.ovid.g.yyttgd.top/ovidweb.cgi?T=JS&PAGE=reference&D=jbi&NEWS=N&AN=JBI120.
35. Aginga C. Post lower limb orthopedic surgery: telerehabilitation. 2023. Available from: http://ovidsp.ovid.g.yyttgd.top/ovidweb.cgi?T=JS&PAGE=reference&D=jbi&NEWS=N&AN=JBI25514.
36. Henderson KG, Wallis JA, Snowdon DA. Active physiotherapy interventions following total knee arthroplasty in the hospital and inpatient rehabilitation settings: a systematic review and meta-analysis. Physiotherapy. 2018;104(1):25–35. doi:10.1016/j.physio.2017.01.002
37. Umehara T, Tanaka R. Effective exercise intervention period for improving body function or activity in patients with knee osteoarthritis undergoing total knee arthroplasty: a systematic review and meta-analysis. Braz J Phys Ther. 2018;22(4):265–275. doi:10.1016/j.bjpt.2017.10.005
38. Mooiweer Y, Stevens M, Akker-Scheek IVD, et al. Being active with a total Hip or knee prosthesis: a systematic review into physical activity and sports recommendations and interventions to improve physical activity behavior. Eur Rev Aging Phys A. 2022;19(1):7. doi:10.1186/s11556-022-00285-1
39. Çetinkaya F, Karakoyun A. The effects of elastic band exercise on the pain, kinesiophobia, functional, and psychological status after total knee arthroplasty: a randomized controlled trial. Clin Rheumatol. 2022;41(10):3179–3188. doi:10.1007/s10067-022-06266-0
40. Eymir M, Erduran M, Ünver B. Active heel-slide exercise therapy facilitates the functional and proprioceptive enhancement following total knee arthroplasty compared to continuous passive motion. Knee Surg Sport Tr A. 2021;29(10):3352–3360. doi:10.1007/s00167-020-06181-4
41. Westby MD, Brittain A, Backman CL. Expert consensus on best practices for post-acute rehabilitation after total hip and knee arthroplasty: a canada and united states delphi study: rehabilitation best practices after total joint arthroplasty. Arthritis Care Res. 2014;66(3):411–423. doi:10.1002/acr.22164
42. Zhou Z, Weng X, Qu T, et al. Expert consensus in enhanced recovery after total Hip and knee arthroplasty in China: perioperative management. Chin J Bone Joint Surg. 2016;9(1):1–9.
43. Chinese Aging Well Association. Expert consensus on enhanced rehabilitation during the perioperative period of hip and knee arthroplasty. J Pract Orthopaedics. 2021;27(11):961–965. doi:10.13795/j.cnki.sgkz.2021.11.001
44. Stover AM, Liang D, Mueller D, et al. Pharmacist-facilitated patient reported outcome measure (PROM) monitoring: developing an EHR SmartForm© to monitor side effects of oral oncolytics during routine telehealth encounters. Qual Life Res. 2025;34(1):201–217. doi:10.1007/s11136-024-03789-8
45. Husted RS, Bandholm T, Rathleff MS, Troelsen A, Kirk J. Perceived facilitators and barriers among physical therapists and orthopedic surgeons to pre-operative home-based exercise with one exercise-only in patients eligible for knee replacement: a qualitative interview study nested in the QUADX-1 trial. PLoS One. 2020;15(10):e0241175. doi:10.1371/journal.pone.0241175
46. Bhardwaj A, FitzGerald C, Graham M, MacFarlane A, Kennedy N, Toomey CM. Barriers and facilitators to implementation of an exercise and education programme for osteoarthritis: a qualitative study using the consolidated framework for implementation research. Rheumatol Int. 2024;44(6):1035–1050. doi:10.1007/s00296-024-05590-9
47. Jiao S, Feng Z, Huang J, Dai T, Liu R, Meng Q. Enhanced recovery after surgery combined with quantitative rehabilitation training in early rehabilitation after total knee replacement: a randomized controlled trial. Eur J Phys Rehabil Med. 2024;60(1):74–83. doi:10.23736/S1973-9087.23.07899-1
48. Zhang Q, Chen Y, Li Y, et al. Enhanced recovery after surgery in patients after Hip and knee arthroplasty: a systematic review and meta-analysis. Postgrad Med J. 2024;100(1181):159–173. doi:10.1093/postmj/qgad125
49. Gianola S, Stucovitz E, Castellini G, et al. Effects of early virtual reality-based rehabilitation in patients with total knee arthroplasty: a randomized controlled trial. Medicine. 2020;99(7):e19136. doi:10.1097/MD.0000000000019136
50. Nguyen C, Boutron I, Roren A, et al. Effect of prehabilitation before total knee replacement for knee osteoarthritis on functional outcomes a randomized clinical trial. JAMA Network Open. 2022;5(3):e221462. doi:10.1001/jamanetworkopen.2022.1462
51. Kim TW, Kim SH. Effectiveness of patient education on total knee arthroplasty: a systematic review and meta-analysis. J Clin Nurs. 2023;32(11–12):2383–2398. doi:10.1111/jocn.16324
52. Jenkins C, Lowe CM, Barker KL. Early post-operative physiotherapy rehabilitation after primary unilateral unicompartmental knee replacement: a systematic review. Physiotherapy. 2023;118:39–53. doi:10.1016/j.physio.2022.05.003
53. Larsen JB, Skou ST, Laursen M, Bruun NH, Arendt-Nielsen L, Madeleine P. Exercise and pain neuroscience education for patients with chronic pain after total knee arthroplasty: a randomized clinical trial. JAMA Network Open. 2024;7(5):e2412179. doi:10.1001/jamanetworkopen.2024.12179
54. Gasbjerg KS, Hägi-Pedersen D, Lunn TH, et al. Effect of dexamethasone as an analgesic adjuvant to multimodal pain treatment after total knee arthroplasty: randomised clinical trial. BMJ. 2022;376:e067325. doi:10.1136/bmj-2021-067325
55. Aalders MB, van der List JP, Keijser LCM, Benner JL. Anxiety and depression prior to total knee arthroplasty are associated with worse pain and subjective function: a prospective comparative study. Knee Surg Sports Traumatol Arthrosc. 2025;33(1):308–318. doi:10.1002/ksa.12336
56. Lyu X, Liu J, Gou Y, Sun S, Hao J, Cui Y. Development and validation of a machine learning-based model of ischemic stroke risk in the Chinese elderly hypertensive population. VIEW. 2024;5(6):20240059. doi:10.1002/VIW.20240059
57. Chen W, Yu H, Hao Y, et al. Comprehensive metabolic fingerprints characterize neuromyelitis optica spectrum disorder by nanoparticle-enhanced laser desorption/ionization mass spectrometry. ACS Nano. 2023;17(20):19779–19792. doi:10.1021/acsnano.3c03765
58. Barichella M, Cereda E, Pinelli G, et al. Muscle-targeted nutritional support for rehabilitation in patients with parkinsonian syndrome. Neurology. 2019;93(5):e485–e496. doi:10.1212/WNL.0000000000007858
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.