Back to Journals » Clinical Interventions in Aging » Volume 20
Electroacupuncture Plus Exercise for Sarcopenia in Older Adults: Protocol for a Randomized, Controlled, Assessor-Blinded Trial
Authors Wu W ![]() , Huang X
, Huang X ![]() , Fang L, Hu H
, Fang L, Hu H ![]() , Han D
, Han D
Received 5 June 2025
Accepted for publication 16 October 2025
Published 23 October 2025 Volume 2025:20 Pages 1775—1786
DOI https://doi.org/10.2147/CIA.S545035
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Wenzhe Wu,1,* Xiaohan Huang,2,* Lianqiang Fang,3 Hantong Hu,3 Dexiong Han3
1Cadre Department, The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 2The Third Clinical College, Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 3Department of Acupuncture and Moxibustion, The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hantong Hu, Department of Acupuncture and Moxibustion, The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China, Email [email protected] Dexiong Han, Department of Acupuncture and Moxibustion, The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China, Email [email protected]
Background: The therapeutic effect of conventional therapies (eg, resistance training, nutritional support) for treating sarcopenia show limited efficacy in older individuals with multiple comorbidities. Therefore, this study aims to investigate whether electroacupuncture (EA) combined with standardized exercise therapy improves walking ability and other functional outcomes in older patients with sarcopenia compared to exercise-alone therapy.
Methods: This randomized, controlled, assessor-blinded trial will include 122 older adults diagnosed with sarcopenia. Participants are randomly allocated to either the EA plus exercise group or exercise-only group in a 1:1 ratio. Both groups will follow 12-week Otago Exercise Program, with the EA plus exercise group receiving additional EA treatment targeting lower limb muscle flaccidity. Primary outcome is the Appendicular Skeletal Muscle Mass (ASMM). Secondary outcomes include the Short Physical Performance Battery (SPPB), Timed Up and Go (TUG) Test, 6-minute walk test distance, calf circumference, grip strength, and knee flexion/extension strength. ASMM is selected as the primary endpoint due to its direct relevance as a core diagnostic criterion for sarcopenia and its objective measurement of muscle mass changes. All outcome measures will be evaluated before treatment, at week 6 and week 12 during the treatment course, and at the end of 12-week follow-up (week 24). Adverse events will be monitored during the trial.
Discussion: This trial will provide valuable insights into the combined use of electroacupuncture and exercise for improving walking ability and other functional outcomes in older individuals with sarcopenia. The results could potentially inform clinical practices and offer a new therapeutic option for managing sarcopenia.
Trial Registration: Clinicaltrials.gov under the identifier NCT05431010.
Keywords: electroacupuncture, exercise, sarcopenia, randomized controlled trial, study protocol, walking ability
Introduction
Sarcopenia represents a geriatric syndrome marked by the progressive deterioration of skeletal muscle mass, functionality, and strength.1 Sarcopenia has been a serious public health concern because it often leads to disability, falls, and a lower quality of life for older adults. This issue is not confined to one region; the global aging trend underscores sarcopenia as an international health priority. The prevalence of sarcopenia increases with age, with estimates ranging from 5–13% in individuals aged 60–70 years to 11–50% in those over 80 years.2 The situation is particularly pressing in China, the rapidly aging population is expected to experience a significant increase in the prevalence of sarcopenia. A systematic review and meta-analysis revealed that in China, the prevalence rate of sarcopenia is 45.4% for older adults aged 80 and above, 27.2% for those aged 70–79, and 15.7% for those aged 60–69.3
Sarcopenia predominantly affects the appendicular skeletal muscles, particularly those of the lower extremities, which are critical for maintaining mobility, balance, and functional independence in older adults. With the increasing aging population, finding effective treatments for sarcopenia has become increasingly urgent. Current treatment strategies for sarcopenia primarily include exercise interventions,4 nutritional support,5 and pharmacological approaches.6 Among these, exercise interventions—particularly resistance training and functional exercises targeting lower extremity muscles—have demonstrated effectiveness in improving muscle mass and strength in sarcopenic individuals. The Otago Exercise Program, specifically, has been extensively validated in older adults and has shown benefits in improving lower limb muscle strength, balance, and reducing fall risk. It is a well-validated fall prevention and strength-building program for older adults. However, these conventional therapies often show limited efficacy in older populations with multiple comorbidities.7 This limitation highlights the need for complementary treatment approaches. Traditional Chinese Medicine, particularly acupuncture, presents a potentially valuable adjunctive therapy that may augment the benefits of conventional treatments for sarcopenia.8
Electroacupuncture (EA) is a modern form of acupuncture that combines traditional manual needling with electrical stimulation.9 In past few years, there has been a gradual emergence of research investigating EA as a potential therapeutic approach for sarcopenia.10–12 These studies10–12 suggest that EA can increase cross-sectional area of atrophied muscles, improve muscle mass, maintain appropriate muscle tone, and enhance fatigue resistance.
Despite these promising findings, several critical research gaps limit our understanding of EA’s therapeutic potential in sarcopenia management. First, while exercise interventions—particularly resistance training and programs like the Otago Exercise Program—have established efficacy as the cornerstone treatment for sarcopenia, the comparative effectiveness of EA as an adjunctive therapy remains unclear. Second, most existing EA studies have been conducted in younger populations or animal models, with limited evidence specifically targeting older adults who represent the primary demographic affected by sarcopenia. Third, and most importantly, no studies have directly compared the combined approach of EA plus exercise against exercise alone in older sarcopenic patients. This absence of head-to-head comparisons makes it impossible to determine whether EA provides additional clinical benefits beyond those achieved through exercise interventions alone. To our knowledge, our study is the first randomized trial to evaluate the additive effect of EA on a validated exercise program in older individuals with sarcopenia.
Furthermore, given that exercise therapy is already well-established as an effective treatment for sarcopenia, the critical clinical question is not whether EA works in isolation, but rather whether adding EA to standard exercise protocols can enhance therapeutic outcomes. This distinction is particularly important for clinical practice, where the goal is to optimize treatment effectiveness rather than replace proven interventions. Consequently, the evidence supporting EA’s adjunctive benefit over standard exercise therapy requires rigorous comparative investigation. These research gaps underscore the urgent need for well-designed clinical trials that directly compare combined EA-exercise interventions against exercise alone to establish whether EA provides clinically meaningful additional benefits in sarcopenia management.
To address these critical research gaps and contribute meaningful evidence to this emerging field, we have designed this innovative randomized controlled trial (RCT). Our study aims to evaluate the efficacy and safety of EA, when combined with a standardized exercise program, in improving walking ability and other clinically relevant outcomes in older adults diagnosed with sarcopenia. Through this investigation, we seek to provide robust clinical evidence that may inform future treatment guidelines and improve functional outcomes for this vulnerable population.
Methods
Study Design and Setting
This study is designed as a randomized, controlled, and assessor-blinded trial. The study will enroll a total of 122 eligible participants, who will be randomly assigned to two groups in a 1:1 allocation ratio. The experimental group receives EA plus a standardized exercise program, and the control group receives a standardized exercise program, only.9 Participants in both groups will undergo 12 weeks of treatment and 12 weeks of follow-up. This research is rigorously based on the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT)13 (as shown in supplementary file 1) and the Revised Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA),14 thereby ensuring transparency and methodological rigor. A visual representation of the study flow is provided in Figure 1, while Table 1 outlines the schedule for enrollment, interventions, and outcome measurements.
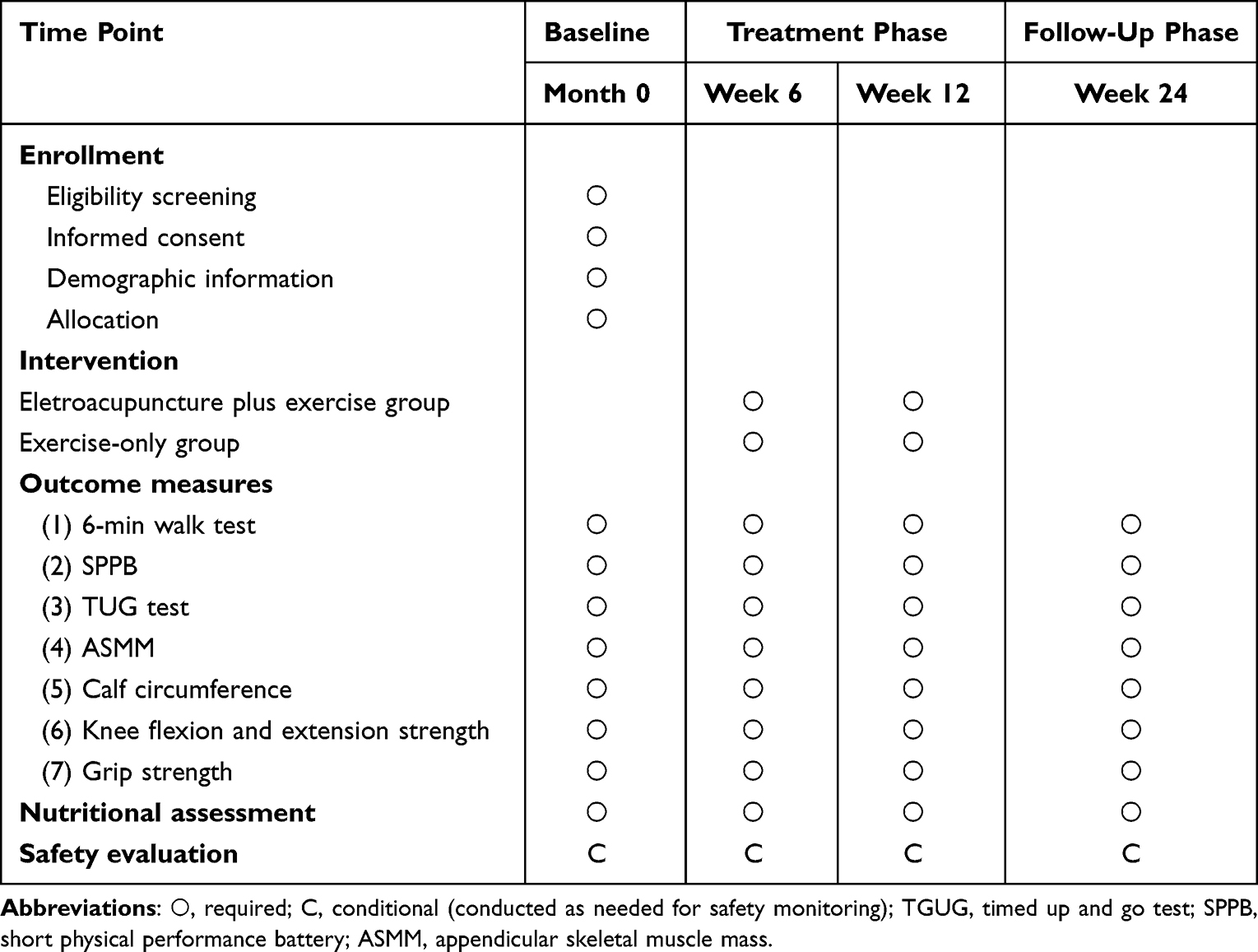 |
Table 1 Schedule of Enrolment, Interventions and Outcome Assessments |
 |
Figure 1 Flow chart of the study process. Abbreviations: TGUG, timed up and go test; SPPB, short physical performance battery; ASMM, appendicular skeletal muscle mass. |
Ethical Approval and Trial Registration
This study has received ethical approval from the Ethics Committee of The Third Affiliated Hospital of Zhejiang Chinese Medical University (approval document No. ZSLL-KY-2022-021-01). Before enrollment, written informed consent will be secured from all participants following a detailed explanation of the study objectives, methodology, potential risks and benefits, and the unequivocal right to withdraw from the study at any time. The study will be conducted in strict adherence to the principles outlined in the Declaration of Helsinki.
For ensuring the transparency of reporting, this RCT has been registered with the Clinicaltrials.gov Registry under identifier NCT05431010.
Participants
Recruitment
The trial will recruit older adults (aged 65 years and above) diagnosed with sarcopenia. Participants will be sourced from the Third Affiliated Hospital of Zhejiang Chinese Medical University and its surrounding communities. Recruitment efforts will encompass a multi-pronged approach, including the distribution of flyers and posters within the hospital and local community centers, online advertisements via WeChat, and presentations at local senior centers. Trained research staff will conduct thorough screenings of potential participants to determine their eligibility.
Inclusion Criteria
Patients will be included if they:
- Meet the diagnostic criteria established by the Asian Working Group for Sarcopenia (AWGS);15
- Are aged 65 years or older, regardless of gender;
- Are able to independently walk, communicate clearly, and complete the standardized exercise program;
- Voluntarily agree to participate and provide written informed consent.
Exclusion Criteria
Patients will be excluded if they:
- Have severe primary diseases of the brain, heart, liver, kidney, or hematopoietic system;
- Exhibit cognitive impairment, severe mental illness, or disorientation;
- Have injuries or conditions preventing participation in the standardized exercise program;
- Are unable to complete the standardized exercise program;
- Have contraindications preventing EA treatment;
- Are concurrently participating in other clinical trials involving drugs, acupuncture, or massage therapy.
Randomization and Assignment Concealment
To account for the heterogeneity in sarcopenia presentation according to the AWGS diagnostic criteria, a stratified randomization approach will be implemented. Participants will first be stratified based on their diagnostic subtype: (1) low muscle mass with reduced grip strength, or (2) low muscle mass with impaired physical performance. Within each stratum, participants will be assigned to either the EA plus exercise group or the exercise-only group in a 1:1 ratio. This will be achieved by using a computer-generated random number sequence with varying block sizes to ensure balanced allocation across the treatment arms within each subtype. An independent statistician, who is uninvolved in participant recruitment or assessment, will generate this sequence. To ensure allocation concealment, sequentially numbered, opaque, sealed envelopes will be adopted. These envelopes will be opened by a research assistant after a participant has completed baseline assessments and has been formally enrolled in the study. The allocation sequence will remain concealed from the outcome assessors throughout the study.
Blinding
While the characteristic of the intervention precludes blinding of acupuncturists and participants, outcome assessors and data analysts will remain blinded to group allocation. To maintain this blinding, participants will be explicitly instructed not to discuss their treatment assignment with the outcome assessors. Additionally, assessors will conduct evaluations in a separate room from where the interventions are delivered, and all participant records will be de-identified and coded with a unique ID number. Furthermore, assessors will receive reminders at each assessment time point to refrain from inquiring about the participant’s treatment. Statistical analyses will be conducted using coded group assignments (eg, Group A and Group B), preserving the blinding of the statistician.
Intervention Procedures
Electroacupuncture (EA) Plus Exercise Group
Acupuncture needles measuring 40 mm in length and 0.3 mm in diameter (Suzhou Medical Supplies Co., Suzhou, China) will be utilized in this study. Electroacupuncture (EA) will be performed using an SDZ-II electronic acupuncture device (Suzhou Medical Appliance Factory, Suzhou New District, China). The anatomical positioning of acupuncture points adheres strictly to the National Standard Nomenclature and Location of Acupuncture Points (GB/T12346-2006).16 Specific points selected and their precise anatomical locations are detailed in Table 2. A visual schematic of acupoint locations is shown in Figure 2.
 |
Table 2 Anatomical Locations and Indication of Acupoints for Treating Sarcopenia* |
 |
Figure 2 A visual schematic of acupoint locations. |
Following expert consensus and referencing prior related research,11 bilateral acupuncture points Biguan (ST31), Futu (ST32), Yanglingquan (GB34), and Zusanli (ST36) were selected. The rationale for selecting these acupuncture points is that Biguan (ST31) specifically targets muscle flaccidity in the proximal thigh, whereas Futu (ST32) is aimed at addressing muscle flaccidity in the distal thigh. Yanglingquan (GB34) is selected for flaccidity affecting the proximal calf, and Zusanli (ST36) targets the distal calf.
Subjects will be positioned supine during treatments. Following routine skin disinfection, acupuncture needles will be inserted at the selected points until Deqi sensations are elicited. Electrodes from the EA device will be attached bilaterally to the needles at Biguan, Futu, Yanglingquan, and Zusanli. A sparse wave stimulation at a frequency of 2 Hz will be applied, with current intensity gradually increased to the highest level comfortably tolerated by each subject.
Each electroacupuncture treatment session will last 30 minutes. Participants in the EA group will receive treatments combined with the Otago exercise program every other day for a duration of 12 weeks. All EA treatments will be administered by the same licensed acupuncturist, possessing a minimum of five years of clinical experience, to ensure consistency and uniformity of the therapeutic approach.
Participants in this group will also participate in the Otago Exercise Program, which is described in detail as below.
Exercise-Only Group
This group only receives the Otago exercise alone. The Otago program is suitable for exercise at home and can strengthen lower limb muscles, improve balance and prevent falls in older adults.17,18 It is an effective exercise program for the treatment of sarcopenia.19 The Otago exercise program comprises a 5-minute warm-up involving gentle stretching and range-of-motion exercises; a 20-minute strengthening component focusing on progressive resistance exercises that target the major muscle groups of the lower extremities (including squats, heel raises, toe raises, knee extensions, and hip abductions), with resistance provided by ankle weights and gradually increased over time as tolerated; a 5-minute balance training segment incorporating exercises like standing on one leg, tandem stance, and heel-to-toe walking, with the difficulty progressively increased; and a 5-minute cool-down period of gentle stretching.
To ensure proper exercise technique and adherence, the Otago exercise program will be supervised by a qualified physiotherapist. In details, participants in both groups will receive initial one-on-one training sessions with a qualified physiotherapist. They will also be provided with a detailed exercise manual and a diary to document their exercise sessions. Weekly phone calls will be made to each participant to monitor adherence and address any concerns. Adherence will be assessed through review of the exercise diary and self-report during phone calls. A specific progression protocol for the resistance exercises will be provided, detailing the initial weight and the increments.
Participants will be instructed to perform the Otago Exercise Program three times per week for 12 weeks.
Nutritional Assessment
Throughout the study period, participants’ dietary intake will be monitored using 3-day food diaries completed at baseline, weeks 6, 12, and 24. Nutritional status will be assessed through anthropometric measurements and basic biochemical parameters (albumin, prealbumin). Participants will be advised to maintain their usual dietary habits and avoid initiating new nutritional supplements during the study period.
Outcomes
Outcome assessments will be conducted at four time points: baseline (prior to randomization), 6 weeks (mid-treatment), 12 weeks (at the end of the treatment course), and 24 weeks (at the end of 12-week follow-up).
Primary Outcome
The primary outcome is defined as the change in Appendicular Skeletal Muscle Mass (ASMM). Appendicular Skeletal Muscle Mass (ASMM) refers to the total muscle mass of the limbs, which plays a crucial role in physical function and mobility. It is often used as an indicator of overall muscle health and is associated with various health outcomes, such as sarcopenia and frailty. ASMM will be assessed using dual-energy X-ray absorptiometry (DXA) scans.20 Participants will undergo standardized whole-body scans with the same technician to minimize variability, and ASMM will be calculated as the sum of lean mass in the arms and legs, reported in kilograms.
Secondary Outcomes
Short Physical Performance Battery (SPPB)
The SPPB is a composite measure of lower extremity function that assesses balance, gait speed, and chair stand ability.21 The SPPB scores range from 0 (worst) to 12 (best), reflecting progressively better physical performance.
Timed Up and Go (TUG) Test
The TUG test measures the time taken to perform a standardized mobility task: rising from a chair, walking 3 meters, turning, walking back, and sitting down.22 A shorter time indicates better mobility and balance.
6-Minute Walk Test (6MWT) Distance
The 6MWT is proved as a reliable and valid assessment of walking capacity in older adults.23 Participants are instructed to walk as far as possible within a 6-minute period along a designated, flat course. The total distance covered is recorded in meters.
Calf Circumference
Calf circumference will be measured at the maximum circumference point using a non-elastic measuring tape with participants seated and knee flexed at 90 degrees.
Knee Flexion and Extension Strength
Knee flexion and extension strength will be evaluated using isokinetic dynamometry with participants performing maximal voluntary contractions at 60°/second angular velocity.
Grip Strength
Grip strength will be assessed using a hand-held dynamometer with participants seated, elbow flexed at 90 degrees, and the highest value from three consecutive measurements on each hand recorded. Although our exercise intervention primarily targets lower extremity muscles, grip strength is included as a secondary outcome measure because: (1) it serves as a well-established indicator of overall muscle strength and sarcopenia severity according to international diagnostic criteria; (2) it provides insight into potential systemic effects of the combined intervention beyond the targeted lower limb muscles; and (3) it enables comparison with established normative values and other sarcopenia studies, enhancing the clinical relevance and interpretability of our findings.
Safety Evaluation
Adverse events (AEs) will be constantly monitored. Participants will be explicitly asked about any new or worsening symptoms at each treatment session and follow-up assessment. The adverse events (AEs) associated with acupuncture primarily include intolerable pain, hematoma, bleeding, skin allergies, and symptoms such as sweating, fainting, or dizziness. AEs occurring throughout the trial will be evaluated and documented in case record forms. Researchers will document treatment measures, extent, duration, and date of AEs in detail. When severe AEs occurs, the investigators must report the case to the Ethics Committee of Third Affiliated Hospital of Zhejiang Chinese Medical University. The Ethics Committee will determine whether to withdraw participants with AEs and will audit every three months.
Strategies to Enhance Intervention Adherence
Subjects can report personal feelings during the research, and appropriate feedback will be given to improve compliance with the intervention. Regular follow-ups will be maintained to promote participant adherence. To enhance adherence, participants will receive a treatment diary to record their home exercise compliance and will be contacted by telephone weekly to address any concerns. Additionally, transportation subsidies will be provided to facilitate attendance at clinic visits. Participants will be asked to maintain their usual dietary habits and to avoid initiating new exercise programs outside the study protocol.
Quality Control
Prior to commencing the trial, all research personnel will undergo comprehensive training on the study protocol, standardized assessment procedures, and documentation requirements. Regular adjustment of all measuring instruments will be carried out to ensure the accuracy of measurements. To maintain consistency, the same evaluators will assess the same participants throughout the study whenever possible. Data quality will be ensured through several measures. Data will be recorded on standardized case report forms by independent personnel. Regular data audits will be conducted. A data management team will verify data authenticity and address any data quality issues.
Sample Size Estimation
The determination of sample size is based on the primary outcome measure, specifically the Appendicular Skeletal Muscle Mass (ASMM), and is conducted using PASS 15 software. Based on our preliminary data, we anticipated a between-group difference of 0.5 kg in ASMM following 12-week treatment, with a pooled standard deviation of 0.9 kg. This assumption is derived from our pilot study data from our pilot study. Assuming α = 0.05 (two-sided) and β = 0.10 (power = 90%), a sample size of 54 participants per group is calculated as necessary. To account for a potential dropout rate, conservatively estimated at 15%, we will recruit a total of 122 participants (61 per group). This sample size ensures adequate statistical power to detect clinically meaningful differences between the two groups.
Statistical Analysis
The primary analytical approach will adhere to the intention-to-treat (ITT) principle, which will analyze all randomized participants regardless of protocol adherence. As a secondary analysis, a per-protocol analysis will also be performed, which will analyze only those participants who completed at least 80% of the assigned treatment sessions. Baseline characteristics and outcome measures will be summarized using descriptive statistical methods, with continuous variables expressed as mean ± standard deviation and categorical variables presented as frequency counts and percentages. A mixed-effects model for repeated measures will be used to analyze the longitudinal data, with treatment group, time, and group-by-time interaction as fixed effects, and participant as a random effect. Multiple imputation techniques will be employed for missing data. Subgroup analyses will explore treatment effects by age group, gender, and baseline sarcopenia severity. Statistical analyses will be conducted in SPSS version 26.0 (IBM Corp., Armonk, NY, USA), with statistical significance set at p < 0.05 (two-tailed).
Discussion
This study protocol establishes a methodological framework of a carefully designed RCT. It aims to investigate the efficacy and safety of EA plus exercise for improving walking ability in older adults with sarcopenia. Sarcopenia is a significant and growing public health concern. It requires the development of effective and accessible interventions. Exercise and nutritional supplementation are the main approaches to sarcopenia management. However, these methods can have limited effectiveness, especially in frail older individuals. EA presents a potentially valuable adjunctive therapy that may improve the benefits of exercise.
Strengths of This Study
First, the selection of acupuncture points in this study is based on both traditional Chinese medicine principles and contemporary anatomical understanding. Points such as Biguan (ST31), Futu (ST32), Yanglingquan (GB34), and Zusanli (ST36) are strategically chosen for their specific associations with lower limb muscle function. This evidence-informed point selection strengthens the treatment’s theoretical foundation and clinical relevance.
Second, the standardization of both the EA protocol and the Otago Exercise Program ensures consistency in treatment delivery. The Otago Exercise Program has been extensively validated for improving lower limb strength and function in older adults, providing a robust comparison condition against which to evaluate the additional benefits of EA.
Third, the comprehensive outcome assessment, which consists of both objective measures of physical function (6MWT, SPPB, TUG, muscle strength, muscle mass) and patient-reported outcomes (SF-36 PF subscale), allows for a comprehensive evaluation of the intervention’s therapeutic effect.
Furthermore, the careful attention to quality control measures, including comprehensive training of research personnel, standardization of assessment procedures, and regular adjustments of measuring instruments, further enhances the reliability and validity of our findings. Our adherence to SPIRIT and STRICTA guidelines also ensures the transparent reporting and methodological rigor of this RCT.
Implications for Clinical Practice and Research
If this trial demonstrates that EA is effective in improving walking ability and other relevant outcomes in older adults with sarcopenia, it could have valuable implications for clinical practice. EA may be considered to be incorporated into comprehensive sarcopenia management programs as a complementary therapy to enhance the benefits of exercise and nutritional interventions. Notably, our findings may inform broader clinical practice, especially in settings where integrative medicine is gaining traction.
This study will also contribute to the growing body of evidence on the use of EA for musculoskeletal conditions. The findings will inform future research on the optimal EA parameters (eg, acupoint selection, stimulation frequency, intensity) for sarcopenia and other age-related conditions. Furthermore, subsequent studies could also explore dose-response relationships, optimal treatment durations, and potential synergistic effects with other interventions such as nutritional supplementation.
Additionally, our findings may stimulate further mechanistic research to investigate the underlying mechanisms of EA in treating sarcopenia. Emerging evidence24,25 suggests that EA may influence muscle protein synthesis, inflammation, and myokine secretion, but these mechanisms remain incompletely understood, particularly in the context of age-related sarcopenia.
Potential Mechanisms of EA for Treating Sarcopenia
Although the exact mechanism of EA for treating sarcopenia remains inconclusive, previous research have suggested possible mechanisms. First, EA may slow aging-related muscle atrophy by modulating the proangiogenic process and protein turnover in the gastrocnemius muscle.26 Second, EA may enhance muscle protein synthesis through stimulation of the AKT/mTOR/p70S6K signaling pathway, which plays a crucial role in regulating muscle growth.27 Additionally, EA potentially improves muscle blood flow by promoting angiogenesis via the HIF1-VEGF pathway, thereby enhancing oxygen and nutrient delivery to muscle tissue.28 EA could suppress oxidative stress, apoptosis, and inflammation markers (IL-6, TNF-α, Atrogin-1, MuRF1) in skeletal muscle cells, supporting the role of EA in reducing chronic inflammation in sarcopenia.29 Furthermore, EA’s direct stimulation of muscle fibers and peripheral nerves could improve neuromuscular function, contributing to increased muscle strength.30
Limitations
Several limitations warrant acknowledgment. First, the lack of a sham acupuncture control group means we cannot fully account for placebo effects, though this design choice reflects the pragmatic nature of the trial comparing EA to standard exercise care. This is an important consideration, as the absence of a sham arm limits the ability to isolate the specific effects of EA from non-specific therapeutic factors such as patient expectation, especially for more subjective outcomes like perceived mobility or fatigue. Second, because of the differences in treatment protocols, this trial could not be blinded to the patients and acupuncture operators. To minimize subjective influence, outcome evaluation is performed by a third party that is confidential about the assignment. Third, due to the lack of enough funds, the 12-week intervention period and 12-week follow-ups, while substantial, may not be sufficient to observe maximal benefits, particularly regarding changes in muscle mass. Longer-term studies may be necessary to fully evaluate the potential of EA as a treatment for sarcopenia. Therefore, we plan to seek funding for future longitudinal studies to track the sustained impact on muscle mass and function over a longer period. Fourth, another important consideration is whether the therapeutic effects of EA combined with exercise operate independently of nutritional factors. While we will monitor dietary intake throughout the study, the complex interplay between EA, exercise, and nutritional status in sarcopenia management requires further investigation in future studies specifically designed to examine these interactions. Last but not the least, our study includes participants from a specific geographical region in China, which will limit generalizability to other countries with different demographic characteristics or cultural attitudes to acupuncture. Future multicenter or international trials are needed to build on this work and confirm the external applicability of our findings.
Conclusion
Given the significant public health burden associated with sarcopenia, particularly in rapidly aging populations such as China and globally, identifying effective interventions represents a research priority with substantial clinical and societal implications. This RCT will provide valuable insights into the combined use of electroacupuncture and exercise for improving walking ability and other functional outcomes in older individuals with sarcopenia. The results could potentially inform clinical practices and offer a new therapeutic option for managing sarcopenia. If successful, this protocol could be integrated into clinical practice in various settings, such as outpatient rehabilitation centers or community health programs, offering a structured, multi-modal approach alongside nutritional counseling. Furthermore, by demonstrating clinical efficacy, this trial will lay the groundwork for future mechanistic studies designed to elucidate the biological pathways through which EA exerts its effects on muscle health.
Ethics Approval and Consent to Participate
This study has received ethical approval from the Ethics Committee of The Third Affiliated Hospital of Zhejiang Chinese Medical University (approval document No. ZSLL-KY-2022-021-01). Written informed consent will be obtained from all participants before enrollment.
Acknowledgments
The authors thank all those involved in the study, including practitioners, assessors and participants. Wenzhe Wu and Xiaohan Huang are co-first authors for this study.
Funding
This study was financially supported by the Zhejiang Provincial Administration of Traditional Chinese Medicine (grant number: 2022ZB186), National Science and Technology Co-construction Project for Traditional Chinese Medicine Comprehensive Reform Demonstration Zone (grant number: GZY-KJS-ZJ-2025-024), Zhejiang Province High-Level Health Talent Project (Zhejiang Health Office 2021 No. 40), and the Fifth National Batch of Outstanding Traditional Chinese Medicine Clinical Talent Training Program (National TCM Education Correspondence 2022 No. 1).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sayer AA, Cooper R, Arai H, et al. Sarcopenia. Nat Rev Dis Primers. 2024;10(1):68. doi:10.1038/s41572-024-00550-w
2. Wang C, Bai L. Sarcopenia in the elderly: basic and clinical issues. Geriatrics Gerontol Int. 2012;12. doi:10.1111/j.1447-0594.2012.00851.x.
3. Meng S, He X, Fu X, et al. The prevalence of sarcopenia and risk factors in the older adult in china: a systematic review and meta-analysis. Front Public Health. 2024;12. doi:10.3389/fpubh.2024.1415398.
4. Martone AM, Marzetti E, Calvani R, et al. Exercise and protein intake: a synergistic approach against sarcopenia. Biomed Res Int. 2017;2017:2672435. doi:10.1155/2017/2672435
5. Morley JE, Argiles JM, Evans WJ, et al. Nutritional recommendations for the management of sarcopenia. J Am Med Dir Assoc. 2010;11:391–396. doi:10.1016/j.jamda.2010.04.014
6. Kwak JY, Kwon K-S. Pharmacological interventions for treatment of sarcopenia: current status of drug development for sarcopenia. Ann Geriatr Med Res. 2019;23:98–104. doi:10.4235/agmr.19.0028
7. Sayer AA, Cruz-Jentoft A. Sarcopenia definition, diagnosis and treatment: consensus is growing. Age Ageing. 2022;51:afac220. doi:10.1093/ageing/afac220
8. Guo C-Y, Ma Y-J, Liu S-T, et al. Traditional Chinese medicine and sarcopenia: a systematic review. Front Aging Neurosci. 2022;14:872233. doi:10.3389/fnagi.2022.872233
9. Mayor D. An exploratory review of the electroacupuncture literature: clinical applications and endorphin mechanisms. Acupunct Med. 2013;31:409–415. doi:10.1136/acupmed-2013-010324
10. Soares Mendes Damasceno G, Teixeira THMM, de Souza VCD, et al. Acupuncture treatment in elderly people with sarcopenia: effects on the strength and inflammatory mediators. J Aging Res. 2019;2019:8483576. doi:10.1155/2019/8483576
11. Li H, Zhou L, Zhang X, et al. Electroacupuncture treatment for sarcopenia: study protocol for a randomized controlled trial. BMC Complement Med Ther. 2024;24(1):428. doi:10.1186/s12906-024-04723-8
12. Ma S-F, Lv W-Y, Zhu Q-Y, et al. Electroacupuncture at acupoints of yangming meridians for sarcopenia: a randomized controlled trial. Zhongguo Zhen Jiu. 2023;43:1114–1117. doi:10.13703/j.0255-2930.20221202-k0001
13. Chan A-W, Tetzlaff JM, Altman DG, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med. 2013;158:200–207. doi:10.7326/0003-4819-158-3-201302050-00583
14. MacPherson H, Altman DG, Hammerschlag R, et al. STRICTA revision group revised standards for reporting interventions in clinical trials of acupuncture (STRICTA): extending the CONSORT statement. Acupunct Med. 2010;28:83–93. doi:10.1136/aim.2009.001370
15. Chen L-K, Woo J, Assantachai P, et al. Asian working group for sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J Am Med Dir Assoc. 2020;21:300–307.e2. doi:10.1016/j.jamda.2019.12.012
16. Wu Z, Wu X, Tan Y, Zhao J, Huang L. Compilation notes for the 2006 national standard “nomenclature and location of acupoints”. Chin Acupuncture Moxibustion. 2009;11:924–926.
17. Yi M, Zhang W, Zhang X, Zhou J, Wang Z. The effectiveness of otago exercise program in older adults with frailty or pre-frailty: a systematic review and meta-analysis. Arch Gerontol Geriatr. 2023;114:105083. doi:10.1016/j.archger.2023.105083
18. Cidoncha-Moreno MÁ, Sancho-Sena MDM, Baraiaetxaburu-Zarandona I, Busto-Santos MT, Ibáñez-Ruiz de Arcaute I, González-Pisano AC. Otago working group effect of the otago exercise programme on the frailty of people between 65 and 80 years old. Enferm Clin. 2022;32:225–233. doi:10.1016/j.enfcle.2021.11.003
19. Vlietstra L, Hendrickx W, Waters DL. Exercise interventions in healthy older adults with sarcopenia: a systematic review and meta-analysis. Australas J Ageing. 2018;37:169–183. doi:10.1111/ajag.12521
20. Lee SY, Ahn S, Kim YJ, et al. Comparison between dual-energy x-ray absorptiometry and bioelectrical impedance analyses for accuracy in measuring whole body muscle mass and appendicular skeletal muscle mass. Nutrients. 2018;10(738). doi:10.3390/nu10060738
21. Welch SA, Ward RE, Beauchamp MK, Leveille SG, Travison T, Bean JF. The short physical performance battery (SPPB): a quick and useful tool for fall risk stratification among older primary care patients. J Am Med Dir Assoc. 2021;22:1646–1651. doi:10.1016/j.jamda.2020.09.038
22. Nightingale CJ, Mitchell SN, Butterfield SA. Validation of the timed up and go test for assessing balance variables in adults aged 65 and older. J Aging Phys Act. 2019;27:230–233. doi:10.1123/japa.2018-0049
23. Enright PL. The six-minute walk test. Respir Care. 2003;48:783–785.
24. Yang J, Min S, Xie F, Chen J, Hao X, Ren L. Electroacupuncture alleviates neuromuscular dysfunction in an experimental rat model of immobilization. Oncotarget. 2017;8:85537–85548. doi:10.18632/oncotarget.20246
25. Shen S, Lin Y, Xu D, et al. Electroacupuncture promotes skeletal muscle myogenic differentiation and protein synthesis by reducing Let-7c-5p levels. Altern Ther Health Med. 2024;30:472–480.
26. Zhu Z-W, Tang C-L, Li X-H, et al. Effects of electroacupuncture on proangiogenesis process and protein turnover in a mouse model of sarcopenia. Zhen Ci Yan Jiu. 2020;45:973–979. doi:10.13702/j.1000-0607.200081
27. Favier FB, Costes F, Defour A, et al. Downregulation of Akt/Mammalian target of rapamycin pathway in skeletal muscle is associated with increased REDD1 expression in response to chronic hypoxia. Am J Physiol Regul Integr Comp Physiol. 2010;298:R1659–1666. doi:10.1152/ajpregu.00550.2009
28. Rhoads RP, Flann KL, Cardinal TR, Rathbone CR, Liu X, Allen RE. Satellite cells isolated from aged or dystrophic muscle exhibit a reduced capacity to promote angiogenesis in vitro. Biochem Biophys Res Commun. 2013;440:399–404. doi:10.1016/j.bbrc.2013.09.085
29. Guo F, Fu L, Lu Z. Effect of electroacupuncture combined with sulforaphane in the treatment of sarcopenia in SAMP8 mice. Iran J Basic Med Sci. 2024;27:560–566. doi:10.22038/IJBMS.2024.71345.15509
30. Wu S-H, Wang Y, Xiang D-L, et al. Effects of electroacupuncture at “Jiaji” (EX-B 2) combined with neurodynamic mobilization on gastrocnemius muscle atrophy and expression of NF-κB and MuRF1 in rabbits after sciatic nerve injury. Zhongguo zhen jiu = Chinese acupuncture & moxibustion. 2023;43(11):1293–1299. doi:10.13703/j.0255-2930.20220722-k0001
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.