Back to Journals » Clinical Ophthalmology » Volume 14
Anesthesia for Intravitreal Injection: A Systematic Review
Authors Han J, Rinella NT, Chao DL
Received 17 July 2019
Accepted for publication 19 December 2019
Published 26 February 2020 Volume 2020:14 Pages 543—550
DOI https://doi.org/10.2147/OPTH.S223530
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jonathan Han, Nicholas T Rinella, Daniel L Chao
Shiley Eye Institute, Viterbi Family Department of Ophthalmology, University of California San Diego, La Jolla, CA, USA
Correspondence: Daniel L Chao
Shiley Eye Institute, 9415 Campus Point Drive, La Jolla, CA 92093, USA
Tel +1 858 534-6290
Fax +1 858 534-7985
Email [email protected]
Background: The intravitreal injection has become one of the most commonly performed procedures in ophthalmology; however, there is no standardized approach to anesthesia during the procedure. The goal of this systematic review is to review approaches to anesthesia for intravitreal injection and look at comparative efficacy between these different anesthetics.
Methods: A systematic review of literature was performed in the MEDLINE, PubMed, Cochrane Library, and Clinicaltrials.gov databases using the key words “anesthesia”, “pain management”, and “intravitreal injection”. Of the initial 239 search matches, 30 articles were found to be relevant to the topic. 18 studies were excluded as they did not include primary data or did not include the visual analog scale as a primary outcome. The remaining 12 articles were assessed to look at the comparative efficacy of anesthesia and adverse events.
Results: The anesthesia techniques reported include topical methods such as anesthetic eyedrops, anesthetic gels, and anesthetic-soaked pledgets as well as subconjunctival injection of anesthetic. Ultimately, no single anesthetic or delivery mechanism was shown to be superior to the others in a statistically significant way and adverse events were largely insignificant. Limitations of these studies include relatively small sizes of the studies, as well as the lack of masking which may introduce bias.
Conclusion: In the current literature, no type of anesthetic method was found to be superior to another for intravitreal injection. Future studies in this area may lead to new insights into the efficacy of different forms of intravitreal anesthesia.
Keywords: intravitreal injection, anesthesia, pain, management, review
Introduction
Intravitreal injection (IVI) has become increasingly accepted as the standard of care delivery method for many retinal diseases including neovascular age-related macular degeneration, macular edema, diabetic retinopathy, and retinal vein occlusion. It has seen a dramatic increase in utilization with the advent of anti-vascular endothelial growth factor (VEGF) medications; in 2013, 19 per 1000 Medicare beneficiaries received IVI in the United States. However, despite the high rate of utilization there is yet to be a standardized approach to pre-injection anesthesia. Needle entry has been suggested to be the single most unpleasant step of the IVI procedure and managing the pain is an important aspect in improving patient comfort.1 A survey of retinal specialists in Canada showed that while the majority used anesthetics, there was a varied distribution of agents utilized.2
This article intends to review the current literature on efficacy of various anesthesia methods for intravitreal injection. These agents will be divided into topical and injectable formulations and assessed by their ease of application, efficacy in managing pain, and notable adverse reactions.
Methods
Literature in the MEDLINE database, PubMed, Cochrane Library, and Clinicaltrials.gov was searched using the terms “anesthesia”, “pain management”, and “intravitreal injection” up to September 2018. The initial search yielded 239 articles. After screening of the title and abstracts, 30 articles were found to be relevant and included in the full-text review. Of these 30 articles, 18 were excluded for reasons including being reviews, editorials, meeting abstracts, or not having visual analog scale (VAS) pain score as the primary outcome measure. A visual analog scale is used to measure subjective experiences or attitudes that may be difficult to assess when there are no fixed boundaries for comparison.3 The VAS is most often portrayed as a 100-mm long line with descriptors anchoring either end to demonstrate the extremes. The responder can then mark a spot along the line that best represents their experience. Studies that did not utilize the VAS were excluded because their results offered less gradation and nuance in their grading of pain; additionally, these studies typically compared the effects of different intravitreal injection medications on pain, rather than anesthetic agents. Reference lists of included articles were hand-searched and an additional 2 relevant articles are found in Figure 1.
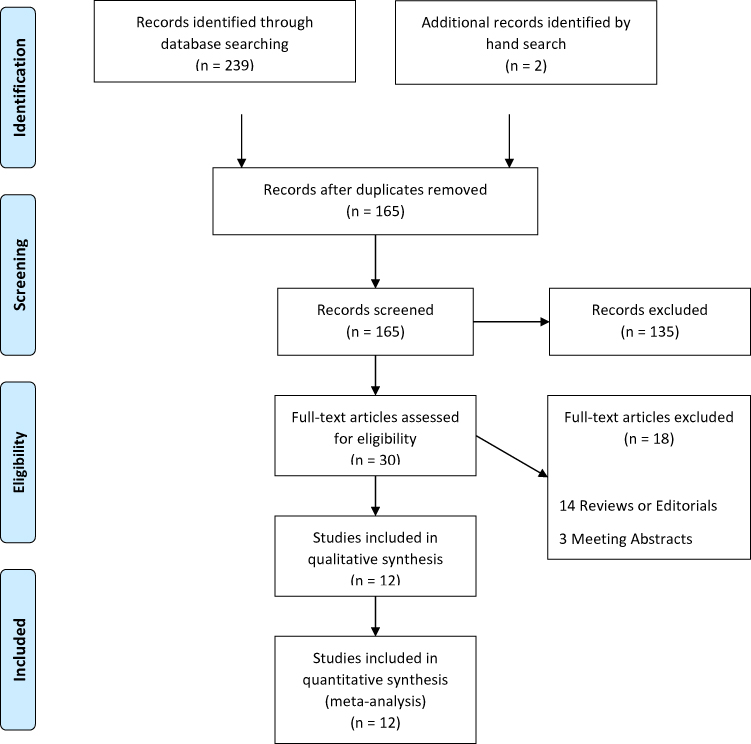 |
Figure 1 Flow diagram for database search. |
Articles reporting the patient’s VAS pain score of the IVI injection for any anesthesia method were included. Studies were excluded from selection if they did not include quantitative analysis of pain or did not have VAS pain score as the primary outcome measure. In the case of uncertainty of the relevance of an article, a senior investigator (DC) was consulted. Conference abstracts were not included in the selection in the event that they were later published and included in this review.
The characteristics of the 12 included studies are summarized in Table 1. Each study was categorized as either topical or injected anesthetic. Topical anesthetics were further subdivided by the formulation of anesthetic used, application method, patient’s reported pain on a 10-point visual analog scale, and whether the investigators found a statistically significant difference in patient pain between anesthetics.
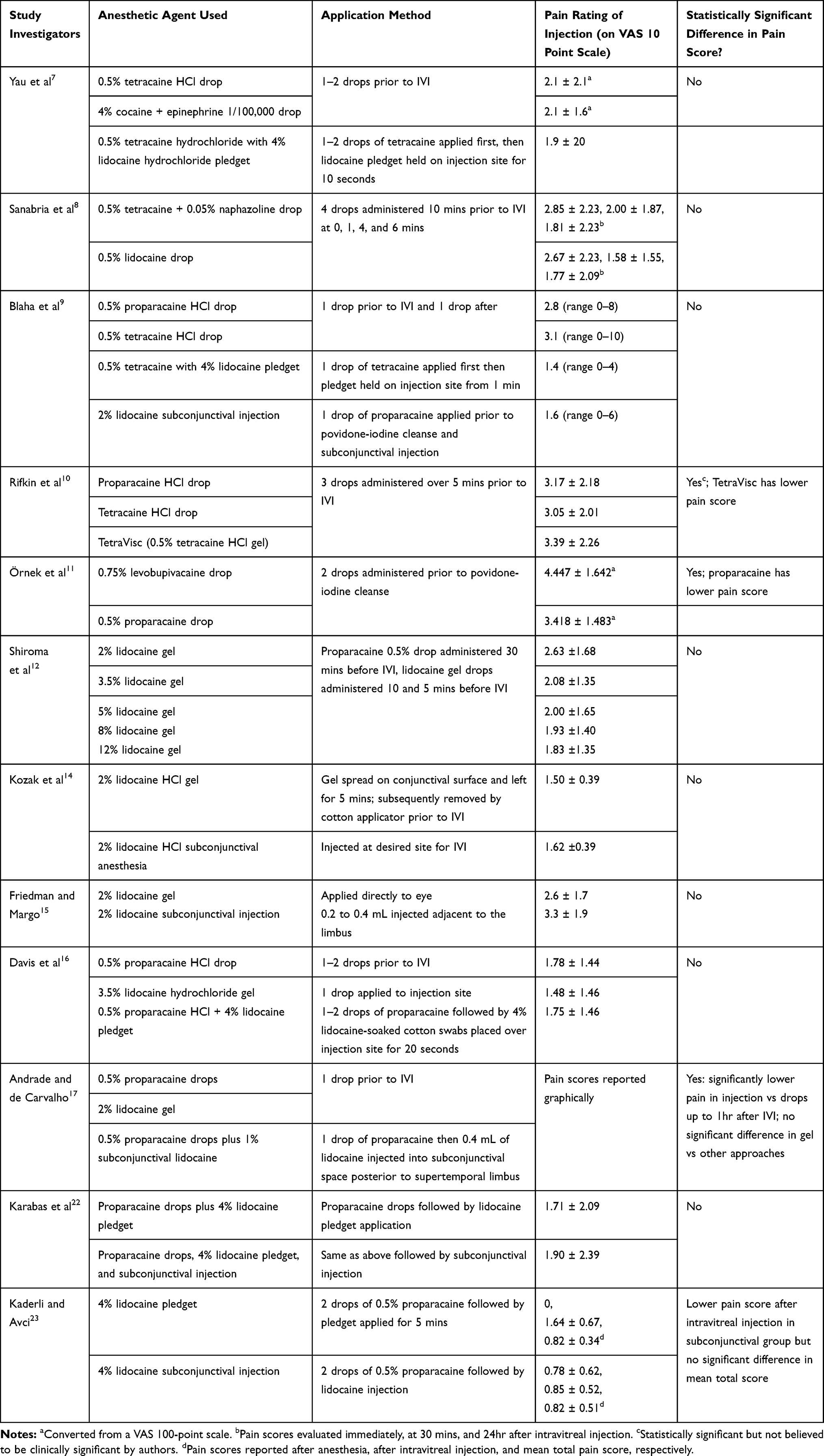 |
Table 1 Summary of Intravitreal Injection Studies |
Topical Anesthetics
Anesthetic Drops
Commonly used formulations of topical anesthetic drops for intravitreal injection include proparacaine hydrochloride, tetracaine hydrochloride, and lidocaine. These drugs decrease the permeability of sodium and ions through the cell membrane of affected cells. This process thus impairs cell membrane depolarization and thus impede pain signaling in the cornea, conjunctiva, and sclera. Tetracaine and lidocaine are typically formulated to a pH of 7.6 to 7.8 in order to penetrate the tear film whereas proparacaine contains benzalkonium chloride to achieve a similar function.4 The drops take effect in 15 to 20 s and typically have an effect lasting for 15 mins. The most common side effect is burning ocular discomfort. Of note, proparacaine can also result in immediate or delayed hypersensitivity reactions. Chronic use of any of the three aforementioned drops can result in decreased corneal epithelial regeneration and cause keratitis, corneal opacification, and loss of visual acuity.5
A survey of Canadian retina specialists by Xing et al in 2014 demonstrated that 90% of those who responded regularly used topical proparacaine, lidocaine, or tetracaine during intravitreal injections.2 Results of a survey in Israel were similar, with all 52 of survey responders using topical anesthetic, 25% of which using only anesthetic drops and 67% using both drops and gel.6 The literature reviewed most commonly saw the use of the above at 0.5% concentration. Additional agents include 4% cocaine + epinephrine 1/100,000 drops used by Yau et al and 0.5% tetracaine + 0.05% naphazoline drops utilized by Sanabria et al.7,8
Five studies compared the efficacy of various topical anesthetics for IVI (Table 1). Among these, there was a slight variation in the methods used to administer the drops. Two studies, by Yau and Blaha et al, used a single drop prior to IVI whereas three, by Sanabria, Rifkin, and Örnek et al, used multiple drops over the span of minutes prior to IVI.7–11 The Blaha study also administered one additional drop of anesthetic after the injection. Each of the above had the patient evaluate the pain of the injection on a 10-point or 100-point visual analog scale immediately after IVI. Three of the five studies did not show a statistically significant difference in pain rating between agents tested. One, the Rifkin and Schaal study noted that the tetracaine solution resulted in a statistically significant improvement in pain as compared to the proparacaine solution.10 However, the authors believed that the small difference in magnitude between the pain scores, 3.05 for tetracaine vs 3.17 for proparacaine did not constitute a clinically significant change. Additionally, this result was not replicated in the Blaha et al study which also compared the same two drops and showed the opposite pattern in pain score. The other, Örnek et al, reported that levobupivacaine resulted in statistically significantly higher pain scores than proparacaine (4.477 vs 3.418, respectively).11 Of note, no other study has reported on the use of levobupivacaine for intravitreal injections and did not appear as a commonly used anesthetic in the surveys among ophthalmologists. Ultimately, no author recommended the use of any one of the anesthetics over another.
None of the five studies reported any significant adverse reactions to the anesthetics used. Shiroma et al did not note any statistically significant differences in the levels of keratitis, conjunctival screening, and hyperemia between differing concentrations of lidocaine gel.12
Anesthetic Gel
Anesthetic gel, including TetraVisc (0.5% tetracaine HCl gel), lidocaine HCl, and Atken (preservative-free lidocaine HCl gel) are also commonly used for ocular pain management. The mechanism of action of these gels and side effect profile are like those of drops. However, it has been proposed that the viscous nature of a gel allows for increased contact with the eye and make it less subject than drops to dilution due to the tear film.4 Early results comparing lidocaine gel to lidocaine drops for cataract surgery showed improved patient experience in favor of the gel.13
The survey by Xing et al reported that 25% of Canadian retinal specialists routinely used lidocaine gel while 16% infrequently used it.2 Among Israeli ophthalmologists surveyed by Segal et al, 8% used anesthetic gel exclusively, with 67% using it in conjunction with drops.6 The most commonly used formulation in the articles reviewed was indeed lidocaine gel, with only one study by Rifkin et al differing and using TetraVisc (0.5% tetracaine HCl gel). Concentrations of lidocaine gel varied from 2% to 12% with 2% being the most commonly used. Application of the gel varied, with earlier studies by Kozak and Friedman electing to spread gel onto the conjunctiva and cleaning it off prior to povidone-iodine sterilization and IVI and the later studies using gel drops immediately prior to injection.10,12,14–17
The use of lidocaine gel was initially shown by Kozak et al in 2005 to have no statistically significant difference in pain score when compared to subconjunctival injection of anesthetic.14 This result has since been supported in studies by Friedman, Davis, and Andrade et al.15–17 Rifkin et al have shown the same result comparing TetraVisc to a subconjunctival injection.10 Shiroma et al further demonstrated that the concentration of lidocaine used, from 2% to 12%, did not have a statistically significant effect on a patient’s pain score.
Although several studies have shown the efficacy of gel-based anesthetics in managing pain, there has been some concern regarding the risks especially regarding the development of endophthalmitis. A 2005 article by Miller et al suggested the use of topical 2% lidocaine gel prior to povidone-iodine preparation as a statistically significant contributor to the development of endophthalmitis in otherwise uncomplicated surgical operations.18 Further, Boden et al demonstrated in 2008 that coating a bacteria-inoculated petri dish with lidocaine gel prior to the application of povidone-iodine resulted in similar numbers of colony-forming units (CFUs) as an inoculated dish without any povidone-iodine; the number of CFUs was two magnitudes greater than the plate treated with povidone-iodine but without lidocaine gel.19 However, a retrospective study of endophthalmitis following intravitreal injection found no significant difference in the incidence of endophthalmitis regardless of whether lidocaine gel was applied before or after povidone-iodine cleansing.20 A review of endophthalmitis after anti-VEGF by Merani and Hunyor in 2015 also saw no significant evidence to indicate that gel led to increased rates of endophthalmitis, concluding that in vivo, the warmth, tears, and the movement of the eye and eyelids prevented the formation of a barrier against povidone-iodine as seen in in vitro studies.21
Anesthetic Pledget
Another method of anesthesia is the use of a pledget soaked with anesthesia and applied with pressure at the site of injection. Xing et al reported that 23% of Canadian retina specialists routinely used a pledget soaked with tetracaine/proparacaine, while 28% infrequently used it.2 Three studies, by Yau, Blaha, and Davis et al, examined the use of pledgets. All three administered a drop of topical anesthetic prior to placement of a pad soaked in 4% lidocaine but the time held on the surface of the eye prior to IVI ranged from 10 s to 1 min. These studies also demonstrated that the use of a pledget resulted in statistically similar pain scores after IVI when compared to drops alone, gel, and subconjunctival anesthetics with no noted significant adverse events.7,9,16 However, no study recommended the use of a pledget over other methods as the anesthetic drops alone achieved equivalent levels of pain control.
Injected Anesthetics
Subconjunctival Anesthetic
The survey of Canadian retina specialists showed that 23% of retina specialists routinely used subconjunctival injections, with 43% infrequently using the technique.2 Seven of the articles reviewed studied subconjunctival injection; all used topical anesthetic drops before injection of lidocaine ranging from 1% to 4%. Andrade et al noted a statistically significant decrease in pain score when comparing subconjunctival injection to topical anesthetic up to 15 mins after IVI.17 However, neither Blaha, Kozak, Friedman, nor Davis found a statistically significant difference in pain score between subconjunctival lidocaine injections and alternative topical anesthetics. Similarly, Karabas et al did not find any notable differences in pain score in patients who received anesthetic pledgets versus pledgets with a subconjunctival anesthetic injection.22 Kaderli et al evaluated pain both after administration of the anesthetic and after the IVI.23 The study found that patients rated the pain of the IVI as statistically significantly lower when given a subconjunctival injection as compared to topical pledget. But, the topical anesthetic was rated as painless while the subcutaneous injection contributed additional pain. When the pain scores for the application of anesthesia and IVI were averaged, there was no significant difference in pain score between the two groups. A later study by Cintra et al also separately scored pain of anesthesia and IVI when evaluating the efficacy of topical versus subcutaneous anesthesia.24 In this study, there was no statistically significant difference in pain score after anesthesia, after IVI, or after combine score.
The main adverse event reported in the context of subconjunctival anesthetic was subconjunctival hemorrhage. In the study by Kaderli et al, 9 of 28 eyes developed hemorrhaging after application of subcutaneous lidocaine, but no hemorrhaging was noted after topical lidocaine which constituted a statistically significant difference.23 Additionally, 11 of 28 eyes in the subconjunctival treatment group developed additional hemorrhaging after IVI whereas 5 of 28 eyes developed a hemorrhage in the topical group, another statistically significant difference. Cintra et al also demonstrated a significantly higher number of subconjunctival hemorrhages with injected anesthesia.
Pain Control Efficacy
Each anesthetic utilized in the 10 studies reviewed resulted in pain after intravitreal injection. Among these, three articles presented an agent which resulted in a statistically significantly lower pain score. In the first, Rifkin et al report a lower pain score with 0.5% tetracaine drops as compared to 0.5% proparacaine and TetraVisc.10 However, the authors make note that the actual scores, 3.05 vs 3.17 and 3.39, do not constitute a medically significant difference. The second, by Andrade et al, reports a lower pain score in the first 15 mins after IVI with the use of subconjunctival lidocaine when compared to 0.5% proparacaine drops but not to 2% lidocaine gel.17 This result was replicated in the third study by Kaderli et al which showed a lower pain score after IVI in the subconjunctival injection group.23 However, when pain scores after anesthesia and IVI were combined, there was no significant difference. Likewise, Blaha, Kozak, Friedman, and Davis also conclude that there is no significant difference in the topical anesthetics tested and subconjunctival lidocaine.
In a review article titled "Patient pain during intravitreal injections under topical anesthesia", Shiroma et al examined eight studies with 847 total subjects through meta-analysis which compared various methods of local anesthesia for intravitreal injection of anti-VEGF or steroids.25 All reported pain was converted to a 0–100 scale and the investigators decided that a difference in pain of 12 or greater was considered clinically significant. Of the original eight, three studies presented with statistically different levels of pain between anesthetic agents. Two resulted in pain score differences less than 12 and were deemed to be medically insignificant. The one article with a medically significant was by Andrade et al which we have shown to be unique amongst studies of similar purpose. Ultimately, no singular anesthetic or method of application in this study has been shown to be significantly more effective than any other.
Adverse Events
Few adverse events were reported in the 10 studies reviewed. The most significant of these is subconjunctival hemorrhage due to subconjunctival injection of anesthetic. No hemorrhaging was reported in any of the topical applications. Indeed, the topical agents presented a safe profile in all 10 studies with the greatest concern being possible increased risk of endophthalmitis with the use of lidocaine gel. However, in vivo studies do not demonstrate any significant increase in endophthalmitis regardless of whether the gel is applied before or after povidone-iodine cleansing.
Discussion
There are numerous approaches to anesthesia for intravitreal injections. In the articles reviewed, the most commonly utilized form of pain management is anesthetic drops which have the fastest and most simple application. Drops have also been shown to have statistically similar pain control to anesthetic gel, pledgets, and subconjunctival injections in all but two studies. However, while both Kaderli et al and Andrade et al reported that subconjunctival anesthetic resulted in a lower initial pain score after intravitreal injection compared to anesthetic drops, there were no significant differences in pain after 15 mins. No anesthetic or application method was ultimately shown to provide superior pain management in a statistically significant manner.
Of note, while there are a variety of methods of application, the pharmaceutical agents utilized during IVI are limited in variety. Lidocaine, proparacaine, and tetracaine were the only anesthetics encountered in this review and are all sodium channel blockers that hinder the depolarization of the cellular membrane. As patient pain scores after IVI do not differ in a statistically significant across the various anesthetics and methods of topical application utilized, it does not appear that the properties of each nor the duration for which they are applied ultimately affect the patient’s comfort. In the one study that assessed the level of pain both after anesthetic administration and after IVI, pain after subconjunctival injection was greater than after topical application. However, the average pain score after anesthesia and IVI did not significantly differ when the two groups were compared, and the subconjunctival injection resulted in a greater number of adverse events. While the studies reviewed did not delve into the specific factors which caused pain in their respective studies, the homogeny of the results seems to indicate that differing applications of similar pharmaceuticals do not act upon these factors in notably different ways.
In terms of adverse events, subconjunctival injections result in a statistically significant increase in the number of subconjunctival hemorrhages after anesthetic applications compared to the other methods, but all adverse event profiles were otherwise similar. Given the insignificant differences in pain management between the various forms of anesthesia but the notably differing time requirements and complications in the case of subconjunctival injections, additional investigation is needed to fully assess the efficacy of each method. To date, there has been no single-randomized clinical trial which has compared all the administration modalities. With the high and still increasing rate of intravitreal injection utilization, it is crucial to conduct such a study in order to identify and standardize the approach which brings the greatest patient comfort.
Disclosure
Daniel L Chao is consultant for Recens Medical, Visgenx, DTx Pharma, and Zilia Health. The authors report no other conflicts of interest in this work.
References
1. Tailor R, Beasley R, Yang Y, Narendran N. Evaluation of patients’ experiences at different stages of the intravitreal injection procedure - what can be improved? Clin Ophthalmol. 2011;5:1499–1502. doi:10.2147/OPTH.S24358
2. Xing L, Dorrepaal SJ, Gale J. Survey of intravitreal injection techniques and treatment protocols among retina specialists in Canada. Can J Ophthalmol. 2014;49(3):261–266. doi:10.1016/j.jcjo.2014.03.009
3. Klimek L, Bergmann KC, Biedermann T, et al. Visual analogue scales (VAS): measuring instruments for the documentation of symptoms and therapy monitoring in cases of allergic rhinitis in everyday health care: position Paper of the German Society of Allergology (AeDA) and the German Society of Allergy and Clinical Immunology (DGAKI), ENT Section, in collaboration with the working group on Clinical Immunology, Allergology and Environmental Medicine of the German Society of Otorhinolaryngology, Head and Neck Surgery (DGHNOKHC). Allergo J Int. 2017;26(1):16–24. doi:10.1007/s40629-016-0006-7
4. Page MA, Fraunfelder FW. Safety, efficacy, and patient acceptability of lidocaine hydrochloride ophthalmic gel as a topical ocular anesthetic for use in ophthalmic procedures. Clin Ophthalmol. 2009;3:601–609. doi:10.2147/opth.s4935
5. Bryant JS, Busbee BG, Reichel E. Overview of ocular anesthesia: past and present. Curr Opin Ophthalmol. 2011;22(3):180–184. doi:10.1097/ICU.0b013e328345974c
6. Segal O, Segal-Trivitz Y, Nemet AY, Geffen N, Nesher R, Mimouni M. Survey of intravitreal injection techniques among retina specialists in Israel. Clin Ophthalmol. 2016;10:1111–1116. doi:10.2147/OPTH.S96452
7. Yau GL, Jackman CS, Hooper PL, Sheidow TG. Intravitreal injection anesthesia–comparison of different topical agents: a prospective randomized controlled trial. Am J Ophthalmol. 2011;151(2):333–337 e332. doi:10.1016/j.ajo.2010.08.031
8. Sanabria MR, Montero JA, Losada MV, et al. Ocular pain after intravitreal injection. Curr Eye Res. 2013;38(2):278–282. doi:10.3109/02713683.2012.758290
9. Blaha GR, Tilton EP, Barouch FC, Marx JL. Randomized trial of anesthetic methods for intravitreal injections. Retina. 2011;31(3):535–539. doi:10.1097/IAE.0b013e3181eac724
10. Rifkin L, Schaal S. Factors affecting patients’ pain intensity during in office intravitreal injection procedure. Retina. 2012;32(4):696–700. doi:10.1097/IAE.0b013e3182252ad3
11. Ornek N, Apan A, Ornek K, Gunay F. Anesthetic effectiveness of topical levobupivacaine 0.75% versus topical proparacaine 0.5% for intravitreal injections. Saudi J Anaesth. 2014;8(2):198–201. doi:10.4103/1658-354X.130713
12. Shiroma HF, Nunes RP, Farah ME, et al. Safety and efficacy of various concentrations of topical lidocaine gel for intravitreal injection. Expert Opin Drug Saf. 2014;13(10):1299–1303. doi:10.1517/14740338.2014.947261
13. Bardocci A, Lofoco G, Perdicaro S, Ciucci F, Manna L. Lidocaine 2% gel versus lidocaine 4% unpreserved drops for topical anesthesia in cataract surgery: a randomized controlled trial. Ophthalmology. 2003;110(1):144–149. doi:10.1016/S0161-6420(02)01562-2
14. Kozak I, Cheng L, Freeman WR. Lidocaine gel anesthesia for intravitreal drug administration. Retina. 2005;25(8):994–998. doi:10.1097/00006982-200512000-00007
15. Friedman SM, Margo CE. Topical gel vs subconjunctival lidocaine for intravitreous injection: a randomized clinical trial. Am J Ophthalmol. 2006;142(5):887–888.
16. Davis MJ, Pollack JS, Shott S. Comparison of topical anesthetics for intravitreal injections: a randomized clinical trial. Retina. 2012;32(4):701–705. doi:10.1097/IAE.0b013e31822f27ca
17. Andrade GC, Carvalho AC. Comparison of 3 different anesthetic approaches for intravitreal injections: a prospective randomized trial. Arq Bras Oftalmol. 2015;78(1):27–31. doi:10.5935/0004-2749.20150008
18. Miller JJ, Scott IU, Flynn HW
19. Boden JH, Myers ML, Lee T, Bushley DM, Torres MF. Effect of lidocaine gel on povidone-iodine antisepsis and microbial survival. J Cataract Refract Surg. 2008;34(10):1773–1775. doi:10.1016/j.jcrs.2008.05.056
20. Lad EM, Maltenfort MG, Leng T. Effect of lidocaine gel anesthesia on endophthalmitis rates following intravitreal injection. Ophthalmic Surg Lasers Imaging. 2012;43(2):115–120. doi:10.3928/15428877-20120119-01
21. Merani R, Hunyor AP. Endophthalmitis following intravitreal anti-vascular endothelial growth factor (VEGF) injection: a comprehensive review. Int J Retina Vitreous. 2015;1:9. doi:10.1186/s40942-015-0010-y
22. Karabas VL, Ozkan B, Kocer CA, Altintas O, Pirhan D, Yuksel N. Comparison of two anesthetic methods for intravitreal ozurdex injection. J Ophthalmol. 2015;2015:861535.
23. Kaderli B, Avci R. Comparison of topical and subconjunctival anesthesia in intravitreal injection administrations. Eur J Ophthalmol. 2006;16(5):718–721. doi:10.1177/112067210601600509
24. Cintra LP, Lucena LR, Da Silva JA, Costa RA, Scott IU, Jorge R. Comparative study of analgesic effectiveness using three different anesthetic techniques for intravitreal injection of bevacizumab. Ophthalmic Surg Lasers Imaging. 2009;40(1):13–18. doi:10.3928/15428877-20090101-05
25. Shiroma HF, Takaschima AKK, Farah ME, et al. Patient pain during intravitreal injections under topical anesthesia: a systematic review. Int J Retina Vitreous. 2017;3:23. doi:10.1186/s40942-017-0076-9
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.