Back to Journals » Clinical Ophthalmology » Volume 12
Analysis of CYP1B1 sequence alterations in patients with primary open-angle glaucoma of Saudi origin
Authors Abu-Amero KK, Sultan T, Al-Obeidan SA, Kondkar AA ![]()
Received 2 April 2018
Accepted for publication 25 May 2018
Published 10 August 2018 Volume 2018:12 Pages 1413—1416
DOI https://doi.org/10.2147/OPTH.S169943
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Khaled K Abu-Amero, Tahira Sultan, Saleh A Al-Obeidan, Altaf A Kondkar
Glaucoma Research Chair, Department of Ophthalmology, College of Medicine, King Saud University, Riyadh, Saudi Arabia
Abstract: Cytochrome P450 Family 1 Subfamily B Member 1 (CYP1B1; OMIM# 601771) gene encodes one of the cytochrome P450 family of enzymes. CYP1B1 mutations have been associated primarily with primary congenital glaucoma (PCG). Similar studies were reported in juvenile open-angle glaucoma, Rieger’s and Peters anomalies. Reports of likely pathogenic sequence alterations in families affected with adult-onset primary open-angle glaucoma (POAG) triggered this investigation. We screened unrelated POAG cases and healthy controls for mutations in CYP1B1 using automated Sanger sequencing to identify five known polymorphisms and one CYP1B1 mutation (p.G61E) in a heterozygous status. The p.G61E mutation is known to cause PCG in a homozygous or compound heterozygous form, and thus, its presence here in a heterozygous form indicates carrier status. These findings suggest that CYP1B1 may have no major role in the pathogenesis of POAG, at least, in the Saudi population. However, further investigations are needed to validate these findings in a larger cohort.
Keywords: CYP1B1, genetics, mutation screening, POAG, Saudi Arabia
Introduction
Cytochrome P450 Family 1 Subfamily B Member 1 (CYP1B1) is a membrane-bound drug-metabolizing enzyme that is also known to be involved in the metabolism of steroids, fatty acids and retinoids that play key roles in cell cycle signaling pathways and apoptosis.1 CYP1B1 has been demonstrated to be highly expressed in the iris and ciliary body of the human eye, and plays an important role in the pathogenesis of anterior segment disorders, including glaucoma.1 There are many postulated theories of how CYP1B1 may contribute to primary congenital glaucoma (PCG) pathogenesis, including the plausibility of mutations in the CYP1B1 gene, which may lead to high intraocular pressure (IOP) in the eye due to increased resistance to aqueous humor outflow pathway through anomalous trabecular meshwork development.1 Mutations in CYP1B1 have been identified in various ethnicities and different glaucoma phenotypes, some of which are population-specific.1,2
Primary open-angle glaucoma (POAG) is a genetically complex multifactorial trait with the plausibility of many genes contributing directly or indirectly to the development/progression of the disease. The genetic basis of POAG is still obscure, and the various disease-causing genes identified by several genetic investigations so far account for <5% of POAG cases in the general population.3 Among many of these genes identified so far, the presence of CYP1B1 mutations has also been reported in families where PCG and POAG coexist, indicating the existence of common or overlapping CYP1B1-mediated pathophysiological mechanism(s) in these two forms of glaucoma.4 Besides, CYP1B1 has been previously indicated for its plausible causative role in early-onset POAG patients from France,5 Germany6 and Spain.7 Furthermore, in vitro functional assay demonstrated that these mutations exhibited none or reduced enzymatic activity, to be classified as null or hypomorphic alleles, respectively, indicating CYP1B1 mutations to be a risk factor for POAG.6,8 In the present study, we investigated whether POAG patients from Saudi Arabia harbor mutation(s) in the CYP1B1 gene.
Patients and methods
The well-defined clinically diagnosed POAG patients (n=50) and healthy controls (n=50) of Saudi origin were recruited to the study at King Abdulaziz University Hospital in Riyadh, Saudi Arabia. POAG patients satisfied the following clinical diagnostic criteria: 1) presence of the disk or retinal nerve fiber layer (RNFL), eg, thinning or notching of disk rim, progressive changes and nerve fiber layer defect; 2) presence of visual field abnormalities (eg, arcuate scotoma, nasal step, paracentral scotoma and generalized depression) in the absence of other causes or explanation; and 3) open angles bilaterally on gonioscopy. Cases with evidence of any secondary form of glaucoma, eg, pigmentary glaucoma, uveitic, pseudoexfoliation and history of steroid use or ocular trauma were excluded. Ethically matched control subjects were selected from ophthalmic screening clinics and individuals with normal IOP (without any anti-glaucoma medication), open angles on gonioscopy and healthy optic disk on examination with no history of ocular disease(s) or previous ophthalmic surgeries. Individuals refusing to participate in the study were excluded. History of the presence or absence of systemic diseases, such as diabetes mellitus, hypertension, coronary artery disease and hypercholesterolemia, and smoking status was procured through medical records of the patients or personal interviews for controls.
Polymerase chain reaction-based automated Sanger sequencing was used to screen for CYP1B1 mutations following the protocol described elsewhere.2 PolyPhen-2 online tool (http://genetics.bwh.harvard.edu/pph2/) was used to assess the possible (damaging/benign) effect of the sequence alterations on the protein structure and/or function as described previously.2
Statistical analysis
Data were represented as mean ± SD for continuous variables and as frequency and percentage for nominal variables. Nominal variables were tested by Pearson’s Chi-square test or Fisher’s exact test (as indicated). Independent samples t-test was used to detect the mean difference across groups. A p-value <0.05 was considered statistically significant. SPSS version 22 (IBM Corporation, Armonk, NY, USA) was used to perform the analyses.
Ethics approval and consent to participate
The study adhered to the tenets of the Declaration of Helsinki and received approval from the institutional review board and research ethics committee of College of Medicine, King Saud University, Riyadh, Saudi Arabia (approval number # 08-657). Written informed consent was obtained from all participants prior to their inclusion in this study.
Results
Table 1 shows the demographic and clinical characteristics of patients and controls selected in this study. Except for family history of glaucoma, there was no significant difference between patients and control groups for age, gender, smoking habit and other systemic co-morbidities.
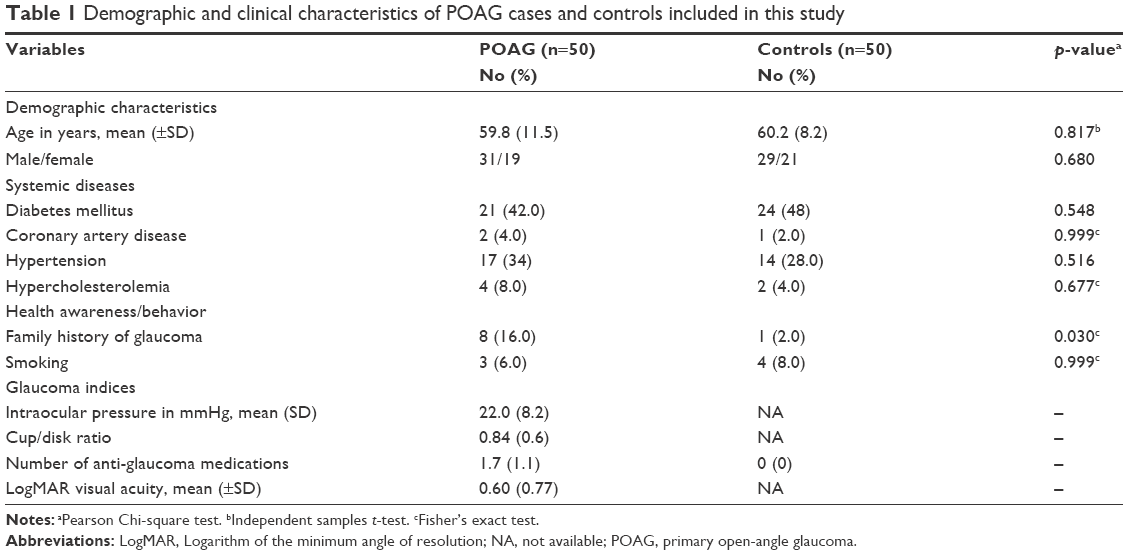 | Table 1 Demographic and clinical characteristics of POAG cases and controls included in this study |
CYP1B1 sequencing revealed a total of five previously reported single nucleotide polymorphisms (SNPs): R48G (rs10012), A119S (rs1056827), L432V (rs1056836), D449D (rs1056837) and N453S (rs1800440). Additionally, we detected one CYP1B1 mutation (G61E) in a heterozygous form as shown in Table 2. Previously, it was reported that the p.G61E mutation was pathogenic in the Saudi PCG patients in a homozygous form.2 However, in this study, the mutation was detected in heterozygous form and accounted for 4% and 2% of the POAG cases and controls, respectively. None of the variants showed any significant association with POAG as compared to controls.
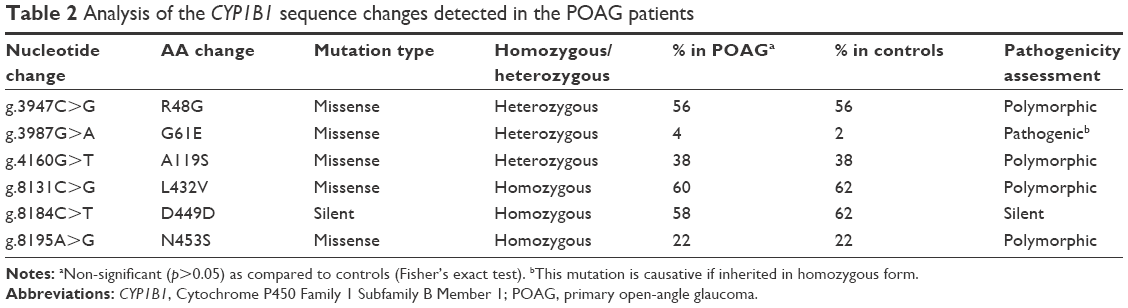 | Table 2 Analysis of the CYP1B1 sequence changes detected in the POAG patients |
Discussion
Genome-wide and candidate gene association studies have so far identified 66 loci harboring 76 different genes in POAG with conflicting findings.3 Many of these studies support the hypothesis that CYP1B1 has a broader significance in POAG.1 However, two meta-analysis studies have found no association between CYP1B1 variants and POAG.9,10 In accordance with these studies, our study also reports a negative association between CYP1B1 and POAG.
Heterozygous CYP1B1 mutations have been reported in French,5 German6 and Spanish7 POAG patients. These mutations have been functionally demonstrated to be hypomorphic or null alleles.6,8 However, heterozygous CYP1B1 variants have also been reported in healthy subjects.5–7 Even in this study we identified a heterozygous p.G61E mutation in CYP1B1 in two POAG patients and one healthy control, which raises questions about its role as a disease-causing mutation.
The gene for CYP1B1 is localized to chromosome 2 and consists of three exons, of which exons 2 and 3 encode the functional protein suggested to be involved in IOP regulation.1 The exact role of CYP1B1 in POAG and/or ocular development is still lacking. However, recent functional studies on characterization of a common homozygous (p.G61E) CYP1B1 mutation in a glaucoma family have demonstrated that this mutation affects the extracellular matrix (ECM) microfibrils, making it less abundant and more fragmented in affected individuals. The authors suggested that disruption of ECM-trabecular meshwork caused increased resistance to aqueous outflow leading to elevated IOP and subsequent development of glaucoma.11 Similarly, missense CYP1B1 mutations reported to be associated with POAG were demonstrated to affect the metabolism of 17β-estradiol, which in turn were implicated to contribute to POAG pathogenesis through MYOC (OMIM# 601652) overexpression or increased oxidative stress and apoptosis.12
Interestingly, our POAG cohorts were previously screened for MYOC and OPTN genes and found to have no mutation(s) in both these genes.13 Taken together, the absence of mutations in the CYP1B1 gene in the Saudi POAG patients suggests that CYP1B1 mutations do not contribute to POAG pathogenesis in the Saudi population. Our finding supports the conclusion reached by the recently conducted meta-analysis studies.9,10 However, as with other complex diseases, including POAG, large sample numbers are needed to ensure sufficient power to identify the underlying genetic causal effect which may be a limiting factor in this study; besides, the presence of rare variants cannot be ruled out in this study, and as such, these findings need further validation in a larger cohort.
In the past 9 years, we have investigated various SNPs with their possible association with POAG in the Saudi population. Among these, we have so far found only two SNPs that were associated with POAG. The first was a “T” allele in the SIX1/SIX6 gene14 and second was an SNP in the GST gene.3 Thus, as far as the genetic cause for POAG in the Saudi population, the jury is still out.
Conclusion
No significant distribution of CYP1B1 mutations or polymorphisms was found in our POAG cohort, indicating that CYP1B1 may not have a major role in POAG, at least, in Saudi population. However, further investigations are needed to confirm these findings.
Acknowledgments
The authors would like to thank the Deanship of Scientific Research and Glaucoma Research Chair of Department of Ophthalmology, College of Medicine, King Saud University for their support and use of laboratory facilities. This work was supported by the Deanship of Scientific Research and Glaucoma Research Chair, College of Medicine, King Saud University, who had no role in the design of the study and collection, analysis and interpretation of data and in writing the manuscript.
Author contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflict of interests in this work.
References
Vasiliou V, Gonzalez FJ. Role of CYP1B1 in glaucoma. Annu Rev Pharmacol Toxicol. 2008;48:333–358. | ||
Abu-Amero KK, Osman EA, Mousa A, et al. Screening of CYP1B1 and LTBP2 genes in Saudi families with primary congenital glaucoma: genotype-phenotype correlation. Mol Vis. 2011;17:2911–2919. | ||
Abu-Amero K, Kondkar AA, Chalam KV. An updated review on the genetics of primary open angle glaucoma. Int J Mol Sci. 2015;16(12):28886–28911. | ||
Micheal S, Ayub H, Zafar SN, et al. Identification of novel CYP1B1 gene mutations in patients with primary congenital and primary open-angle glaucoma. Clin Experiment Ophthalmol. 2015;43(1):31–39. | ||
Melki R, Colomb E, Lefort N, Brezin AP, Garchon HJ. CYP1B1 mutations in French patients with early-onset primary open-angle glaucoma. J Med Genet. 2004;41(9):647–651. | ||
Pasutto F, Chavarria-Soley G, Mardin CY, et al. Heterozygous loss-of-function variants in CYP1B1 predispose to primary open-angle glaucoma. Invest Ophthalmol Vis Sci. 2010;51(1):249–254. | ||
Lopez-Garrido MP, Sanchez-Sanchez F, Lopez-Martinez F, et al. Heterozygous CYP1B1 gene mutations in Spanish patients with primary open-angle glaucoma. Mol Vis. 2006;12:748–755. | ||
Chavarria-Soley G, Sticht H, Aklillu E, et al. Mutations in CYP1B1 cause primary congenital glaucoma by reduction of either activity or abundance of the enzyme. Hum Mutat. 2008;29(9):1147–1153. | ||
Dong S, Yang J, Yu W, Kota P, Xia X, Xu H. No association of genetic polymorphisms in CYP1B1 with primary open-angle glaucoma: a meta- and gene-based analysis. Mol Vis. 2012;18:786–796. | ||
Wang Z, Li M, Li L, Sun H, Lin XY. Association of single nucleotide polymorphisms in the CYP1B1 gene with the risk of primary open-angle glaucoma: a meta-analysis. Genet Mol Res. 2015;14(4):17262–17272. | ||
Safari I, Suri F, Haji-Seyed-Javadi R, Yazdani S, Elahi E. The p.Gly61Glu mutation in CYP1B1 affects the extracellular matrix in glaucoma patients. Ophthalmic Res. 2016;56(2):98–103. | ||
Mookherjee S, Acharya M, Banerjee D, Bhattacharjee A, Ray K. Molecular basis for involvement of CYP1B1 in MYOC upregulation and its potential implication in glaucoma pathogenesis. PLoS One. 2012;7(9):e45077. | ||
Abu-Amero KK, Morales J, Bosley TM. Mitochondrial abnormalities in patients with primary open-angle glaucoma. Invest Ophthalmol Vis Sci. 2006;47(6):2533–2541. | ||
Kondkar AA, Azad TA, Almobarak FA, et al. Polymorphism rs10483727 in the SIX1/SIX6 gene locus is a risk factor for primary open angle glaucoma in a Saudi cohort. Genet Test Mol Biomarkers. 2018;22(1):74–78. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.