Back to Journals » Patient Preference and Adherence » Volume 11
Adherence in ulcerative colitis: an overview
Authors Testa A ![]() , Castiglione F, Nardone OM, Colombo GL
, Castiglione F, Nardone OM, Colombo GL ![]()
Received 8 November 2016
Accepted for publication 11 January 2017
Published 22 February 2017 Volume 2017:11 Pages 297—303
DOI https://doi.org/10.2147/PPA.S127039
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Anna Testa,1 Fabiana Castiglione,1 Olga Maria Nardone,1 Giorgio L Colombo2
1Gastroenterology, University of Naples Federico II, Naples, 2Department of Drug Sciences, University of Pavia, Pavia, Italy
Abstract: Medication adherence is an important challenge while treating chronic illnesses, such as ulcerative colitis (UC), that require a long-term management to induce and maintain clinical remission. This review provides an overview of the role that medication adherence plays in the routine management of UC, with a focus on the results of a recent Italian study reporting the perception of patients with UC regarding adherence to treatment. A literature analysis was conducted on topics, such as measurement of adherence in real practice, causes, risk factors and consequences of non-adherence and strategies, to raise patients’ adherence. Most of the data refer to adherence to 5-aminosalicylic acid, and standard of care for the induction and maintenance of remission in UC. The adherence rate to 5-aminosalicylic acid is low in clinical practice, thus resulting in fivefold higher risk of relapse, likely increased risk of colorectal cancer, reduced quality of life and higher health care costs for in- and outpatient settings. There are various causes affecting non-adherence to therapy: forgetfulness, high cost of drugs, lack of understanding of the drug regimen – which are sometimes due to insufficient explanation by the specialist – anxiety created by possible adverse events, lack of confidence in physicians’ judgment and complex dosing regimen. The last aspect negatively influences adherence to medication both in clinical trial settings and in real-world practice. Regarding this feature, mesalamine in once-daily dosage may be preferable to medications with multiple doses per day because the simplification of treatment regimens improves adherence.
Keywords: adherence, ulcerative colitis, 5-ASA, mesalamine, once-daily
Introduction
Medication adherence is an important challenge in the treatment of chronic illnesses, such as ulcerative colitis (UC), that require a long-term management to induce and maintain clinical remission. Indeed, the course of this disease is generally marked by the alternance of periods of quiescence and symptomatic relapses, which sometimes need hospitalization.1,2
The World Health Organization (WHO) recognizes that adherence in chronic diseases is one of the key factors that contribute to the efficient use of therapies.3 The success of a therapy does not only depend on correct diagnosis and choice of treatment by the physician but also patient’s adherence to therapy is critical, as well as their ability to follow the instructions given during the therapy course. Non-adherence may impact the effectiveness of a cure and determine the worsening of health conditions, the need of examinations or implementation of drugs, and the increase in morbidity and mortality.4–6
According to the WHO definition, the term “adherence” is the extent to which a person’s behavior – taking medication, following a diet and/or executing lifestyle changes – corresponds to agreed recommendations from a health care provider.7,8
In routine clinical practice, therapeutic adherence plays a critical role in the management of UC; therefore, the decision-making process should also include a thorough assessment of risk factors associated with non-adherence, and of patients’ concerns and beliefs.
Physicians have to consider patients’ judgment of their personal need for therapy and their concerns about treatment can be a significant barrier to adherence.9–11 In this setting, interventions should be considered to facilitate adherence to medical treatment among inflammatory bowel disease (IBD) subjects in order to overcome such perceptual barriers.
This non-systematic review provides an overview of the role of medication adherence in the routine management of UC, with a focus on the results of a recent Italian study reporting the perception of patients with UC regarding adherence to treatment. For this purpose, we performed a Medline search for full publications, using the search terms “adherence”, “adherence and ulcerative colitis”, “adherence and inflammatory bowel disease” and “adherence and 5-ASA”. We included only those citations that discussed the impact of adherence on UC.
Burden and measuring adherence in real practice
Most of the data in the literature refer to adherence to 5-aminosalicylic acid (5-ASA), and the standard of care for the induction and maintenance of remission in UC. Different adherence rates were reported according to the study setting in UC patients treated with 5-ASA, also known as mesalamine,4 commonly considered the first-line treatment of mild-to-moderate disease.12
Adherence levels are much lower in community-based studies13,14 than in clinical trials15,16 (40%–60% vs more than 80%), in which participants are generally closely observed and monitored.
In a cohort study of 92 patients with clinically inactive disease who were followed up for more than 48 weeks with appointments occurring every 12 weeks, only 43% of patients were found to be 100% adherent.17 A study that involved 94 UC patients in remission, examining their prescription refill information as a measure of adherence, showed that only 40% of patients were adherent, and the median amount of medication consumed was 71% of the prescribed dose.14 A recent European online survey conducted across six countries showed that 60% of patients with UC (from a total of 372 respondents) had a low adherence based on the Morisky scale, and that only 7% of them had high adherence.18
Low adherence, noticed in the real-world setting, could attenuate benefits of 5-ASA therapy, affect the clinical course of UC and lead to poorer long-term outcomes, with a considerable impact on patients’ quality of life and significant additional costs to society in terms of increased utilization of health care services.14
There are several ways to measure adherence; however, there is not an accepted standard method and it is important to estimate correctly. Direct methods of assessment, including the patient’s observation and the measurement of drug levels or metabolites in blood or urine, are the most accurate ways of estimating medication consumption both in controlled clinical trials and in real clinical practice, even if the tests are not always available. Alternative methods include patient self-report (patient interviews or self-report surveys), the use of electronic monitoring systems of prescription claims or refill history and pill counts.2,19–21
Non-adherence: cause and risk factors
The WHO classifies the determinants of non-adherence to medical plans into five dimensions: social and economical, health system-related, therapy-related, condition-related and patient-related.7,22
In UC, neither clinical nor community studies have consistently identified the same groups of patients as being at high risk for poor adherence.23 Nonetheless, in several studies the factors that appear to affect adherence include younger age, single status, heavy pill burden, perception of lack of benefit and shortage of information about the effect of medication.24
The Manitoba Inflammatory Bowel Disease Cohort Study showed how men with UC were significantly more likely to have poor adherence than those with Crohn’s disease (odds ratio [OR] 4.42, 95% confidence interval [CI]: 1.66–11.75), and that age was a predictive factor for adherence in women: younger women were less adherent than older women (under 30 vs over 50 years: OR 3.64, 95% CI: 1.41–9.43; under 30 vs 40–49 years: OR 2.62, 95% CI: 1.07–6.42).25
Kane et al showed that males were twice as likely as females to be non-adherent with their UC treatment;14,26 in particular, younger men were the least adherent.23,27
Adherence rates are particularly low among patients in symptomatic remission because of the fact that some of them are unable to express their need for medication during periods of symptoms’ quiescence.26,28 In this condition, rather than continuing with the prescribed regimen, patients often forget to take their drugs at the scheduled time; Kane suggested that this forgetfulness may be linked to a form of disease denial: they are in remission and do not wish to be reminded that they have a disease when they feel well.23
In this case, the physician should reassure and instruct the patient on the importance of a continued therapy even in periods of well-being in order to prevent exacerbations.
Lack of medical supervision, concomitant medications, side effects and cost of prescriptions were frequent reasons for treatment non-adherence cited by patients in a North American study.4 However, the most cited factor was the inconvenient dosage schedule of 5-ASA medications, which required a large number of tablets per day.4
Other factors contributing to poor adherence were related to the drugs: the cost (reported by 25% of patients), the concept of therapy as a reminder of illness (13%), the undesirable side effects (13%) and the lack of belief in the effectiveness of the medication (12%).25
The complexity of administration regimen could have a relevant impact on patients’ adherence. Inconvenient and intrusive drug delivery formulations (eg, rectal therapies), pill burden and multiple-daily dosing of oral medications have been shown to be associated with poor levels of therapeutic adherence.4 A literature review conducted by Greenberg has shown that once-daily and twice-daily dosing regimens significantly improve adherence rates (73% and 70%, respectively) than three-times (52%) and four-times-daily dosing (42%) regimens29 Shale and Riley’s study13 demonstrated that three-times-daily dosing and full-time employment were independent predictors of partial non-adherence in patients taking delayed-release mesalamine.
An Italian study15 confirmed all these results: non-adherence was significantly associated with age less than 40 years (43% vs 34%, P=0.041) and the most common reasons for non-adherence versus adherence were as follows: forgetfulness (61% vs 44%, P<0.001), disease remission (25% vs 10%, P<0.001), recent diagnosis (24% vs 15%, P<0.001) and full-time employment (55% vs 26%, P<0.001). Topical therapy with enemas was associated with significantly more non-adherence (68% of users) than oral therapy (40% of users; P=0.001, OR 0.25, CI: 0.11–0.60). Moreover, a significant interaction was found for adherence and patients <40 years who had a good relationship with their doctors. Therefore, good communication with the physician might improve adherence.
Many patients with IBD deliberately decide to stop treatment. A Spanish study on 40 IBD patients has shown that up to 35% of patients are intentionally non-adherent compared with 67% who are unintentionally non-adherent.30 A greater association was found between patients who are intentionally non-adherent and patients who had high depression scores, in patients with long-standing IBD, subjects with high patient–physician discordance and patients who did not consider themselves to be adequately informed about their treatment.30
In Table 1, we have summarized the principle causes of non-adherence.
 | Table 1 Factors of non-adherence in UC |
Consequences of non-adherence
The clinical outcomes of non-adherence can be harmful to patients.
In a cohort of 99 patients with UC in remission, Kane et al prospectively measured clinical outcomes. Non-adherent patients experienced more than a fivefold increased risk of disease relapse compared to those who were adherent (hazard ratio 5.5, 95% CI: 2.3–13, P<0.001).27
In the same way, in a retrospective study, Robinson et al showed that non-adherent subjects had a significantly greater risk of relapse than adherent patients (relative risk =1.44, 95% CI =1.08–1.94; P=0.014).31
Moreover, Moody et al showed a correlation between non-adherence to or discontinuation of sulfasalazine therapy and increased risk of colon cancer; 5 of 152 adherent patients and 5 of 16 non-adherent patients developed colorectal cancer (P<0.001).32 This finding was supported by Eaden et al, who showed in a case-controlled study among 102 cases of colorectal cancer with UC that the risk of colorectal cancer was reduced by 81% in patients receiving regular mesalamine therapy (≥1.2 g/day) compared with those receiving no treatment (P=0.006).33
In addition, poor adherence was associated with a two- to threefold increase in costs for non-hospitalized cases and a 20-fold increase in costs for hospitalized cases compared to quiescent cases of IBD.33 In this study, conducted in the United Kingdom, the authors showed that patients’ costs ranged from £73 to £33.254, with a mean 6-month cost of £1.256 (95% CI: £988, £1.721) per UC subject.34
Strategies to raise patients’ adherence
Patients’ decision to not take medication is a common issue that physicians may not fully understand because many subjects are reluctant to discuss or to give accurate representations of their adherence levels.19 The simplest and most practical suggestion for physicians is to ask patients non-judgmentally how often they miss doses. Patients usually want to please their physicians, so that they say what they think their doctor wants to hear. It can be reassuring to the patient when the physician tells them, “I know it must be difficult to take all your medications regularly. How often do you miss taking them?” This approach makes most patients feel comfortable in telling the truth and facilitates the identification of poor adherence.8
According to some studies, pill burden and multiple-daily dose administration are often associated with non-adherence, and formulations that require less frequent and/or fewer doses may improve patients’ adherence.21 A recent systemic review of interventions to enhance adherence to medications in chronic illnesses found that the only consistent success rates have been with those that aim to simplify dose administration regimen.35 Furthermore, data from an interactive survey of patients with UC showed that, from patients’ perspective, an ideal therapy would have less frequent dosing regimen.36
As stated earlier, once-daily and twice-daily dosing lead to better medication adherence rates than three- or four-times-daily dosing regimens.29
In order to demonstrate improved adherence with a smaller pill burden, a pilot study compared once-daily with conventional dosing of mesalamine.37
The authors observed a significant difference in patients’ adherence between once-daily versus conventional dosing of the drug (respectively, 100% vs 70%): once-daily dosing had the same rate of disease relapse as the conventional dosing group. When a phase III clinical trial demonstrated that once-daily MMX® mesalamine, a new formulation characterized by a polymeric matrix, was effective in inducing remission of active UC, it provided hope that this regimen might also be effective in maintaining disease quiescence: this would combine the benefits of clinical efficacy and ease of use for long-term therapy. The study showed that 96% of patients enrolled were adherent to their medication regimen, as they took more than 80% of their prescribed medication.38
Lachaine et al also reported that the proportion of adherent patients was significantly higher with once-daily mesalamine delayed/extended-release tablets than with any other oral treatments (P<0.001). Therefore, they suggested that
a once daily oral treatment with an extended drug release could be a therapeutic option to improve adherence in UC patients and then to maintain therapy leading to better outcomes and to prevent relapses and complications.26
In the same way, in a randomized trial of maintenance therapy with mesalamine granules 2 g/day in 362 patients, the remission rate after 1 year was significantly higher in the group receiving a single daily dose than in the one receiving 1 g twice daily (74% vs 64%, P=0.024). There was evidence from patients’ questionnaires that adherence was higher in the once-daily group, and this may, in part, explain the unexpected difference, as the trial was designed to show non-inferiority of the once-daily regimen.39
Recently, a meta-analysis evaluated the efficacy, safety and adherence to once-daily and multiple-daily dosing of mesalamine for the induction and the maintenance of remission in mild-to-moderate UC.40 With respect to adherence, no difference was noted between the two doses of 5-ASA.
Another cause of non-adherence is the use of topical therapy; patients often do not accept enemas, which represent the standard of care in case of involvement of the distal colon.12 D’Incà et al showed that topical therapy with foams, suppositories or enemas, is more likely to be associated with non-adherence than oral therapy15 because of discomfort during treatment (68% vs 40%, P=0.001, OR 0.25, CI: 0.11–0.60). A preliminary multicenter trial in patients with left-sided active UC showed that 5-ASA MMX® was comparable to the 5-ASA enema in inducing remission after 8 weeks of treatment (60% vs 50%; 95% CI for the difference, −12 to +32), with a compliance of 97% for oral and 87.5% for topical therapy.16 The authors themselves suggested the need of a larger multicentric trial to confirm these results.
Moreover, in order to improve adherence, some authors use web-based follow-up and patients’ education, considering that the majority of subjects are young.41–43
Pedersen et al studied for 3 months 95 patients with UC receiving mesalamine therapy.41 Once a week, patients registered fecal calprotectin on a web application and completed the simple clinical colitis activity index. A total of 82 (86%) patients were adherent to web therapy, and from week 0 to week 12 subjects experienced clinical and biochemical improvement, thus allowing a reduction in mesalamine dosing due to improved adherence to treatment.
Elkjaer et al evaluated 333 patients with mild/moderate UC in Denmark and Ireland, subjected to treatment with 5-ASA, who were randomized to either a web-group receiving disease-specific education and self-treatment via web or a control group continuing the usual care for 12 months.42 Adherence to 4 weeks of acute treatment was increased by 31% in Denmark and 44% in Ireland compared to the control groups. The number of acute and routine visits to the outpatient clinic was lower in the web than in the control group, resulting in a saving of 189 euro/patient/year.
Moshkovska et al43 organized a tailored approach, consisting of motivational and educational components plus options including simplified dosing regimens and practical reminders, such as pill dispensers. Seventy-one people completed the study. At follow-up, adherence in subjects included in the “tailored” group was 44% greater than in the control group (76% vs 32%, P=0.001).
Patient perception of medication adherence
A recent Italian survey on medication adherence, published as abstract, involved more than 1,000 UC patients with the aim of evaluating the perception of patients with UC regarding adherence to treatment.44
Patients from five regions of Italy (Campania, Lazio, Liguria, Lombardy and Piedmont) were surveyed with a 16 items questionnaire distributed by clinicians of Italian specialized centers. The questionnaire, not validated, consisted of two parts: the first regarding the characteristics of participants (age, sex, marital status and employment status) and the second concerning adherence of the patient to treatment (drugs, visits and family support). A total of 1,045 patients were recruited (male 54%), with a mean age of 48 years (range 5–90 years) and a median duration of disease of 8 years (50% <10 years and 35% <5 years). The extension of the disease was classified as proctitis in 14%, left-sided colitis in 51% and pancolitis in 34% of patients. At the time of compilation, 68% of patients were in remission; 50% of patients assumed mesalamine while 31% were treated with MMX® mesalamine.44
A question was particularly relevant for the assessment of self-perceived adherence of the patients:
Numerous studies show that patients who need continued therapy sometimes do not take medications as prescribed. Is this also true in your case?
To this question, 73% replied that this “never or almost never” had been the case: the perception of the adequate intake of therapy was almost total, with 19% of patients who reported that it had occurred “sometimes”, 5% “often” and 2% “always or almost always” (Figure 1). These adherence rates appear to be higher than those expected and reported by previous studies on patients’ adherence in UC.4,22,45
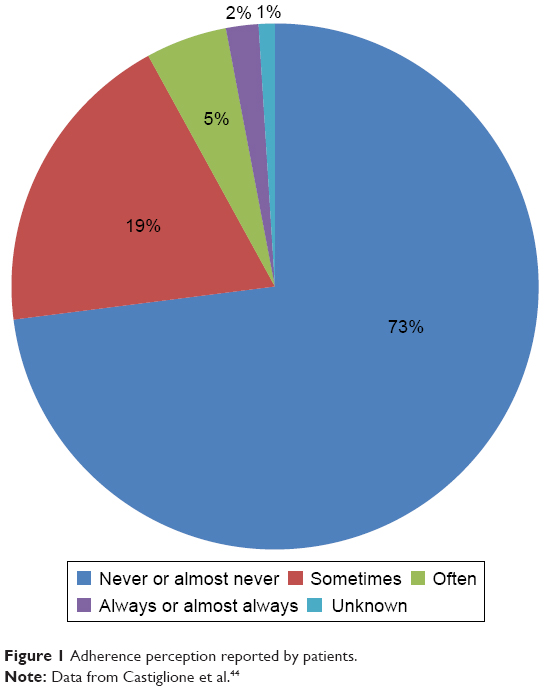 | Figure 1 Adherence perception reported by patients. |
About the type of formulation, the patients did not find any concerns in taking tablets (even if 13% of respondents declared not to take them because they were too busy at work); different attitudes emerged about enemas and suppositories. The main reason for non-adherence to therapy with enemas was “I feel uncomfortable” (29%). In particular, the percentage of this type of response was higher in the active phase of the disease (45%) compared to that of patients in remission (26%). The same applies to suppositories, even if with a lower percentage (about 20% of patients declared “I feel uncomfortable”).
According to the literature, the main reason for non-adherence to treatment, regardless of the formulation prescribed, remains forgetfulness (48%) followed by physical well-being (20%). In case of patients’ forgetfulness, partners have the function of caregivers and serve as reminder therapy, as shown in the study by Kane et al.14
Summary
Even if in the absence of a validated way of assessing adherence, the percentage of adherence detected in this study was greater than those observed in other studies based on objective methods, such as the medication possession ratio.4,6
Conclusion
Adherence to therapy is a key factor in the treatment of chronic illnesses like UC, and most of the data in the literature refer to adherence to 5-ASA, and the standard of care for the induction and maintenance of remission in UC. Since adherence rates to this drug are higher in controlled trials and community setting, it is difficult to apply the data derived from multicentric studies into clinical practice. In the daily management of patients with UC, adherence is low, thus resulting in fivefold higher risk of relapse, reduced quality of life and higher health care costs for both in- and outpatient settings.6,23 For these reasons, the decision-making process should include a thorough assessment of risk factors associated with non-adherence and patients’ concerns, in order to ensure a proper and shared treatment.
According to patients’ judgment, the burden of a complex dosing regimen negatively influences adherence to medication. Therefore, even if in the absence of a strong literature, based on prospective studies in non-adherent patients, several educational (eg, verbal and written) as well as behavioral interventions (reminders, calendar blister packs and dosage implication) have been shown to improve adherence.
Disclosure
The survey was supported by an unrestricted grant of Takeda. The authors report no other conflicts of interest in this work.
References
Bernick SJ, Kane S. Optimizing use of 5-ASA in the treatment of ulcerative colitis: focus on patient compliance and adherence. Patient Relat Outcome Meas. 2010;1:57–63. | ||
Khan N, Abbas AM, Bazzano LA, Koleva YN, Krousel-Wood M. Long-term oral mesalazine adherence and the risk of disease flare in ulcerative colitis: nationwide 10-year retrospective cohort from the veterans affairs healthcare system. Aliment Pharmacol Ther. 2012;36(8):755–764. | ||
Serup J, Lindblad AK, Maroti M, et al. To follow or not to follow dermatological treatment – a review of the literature. Acta Derm Venereol. 2006;86(3):193–197. | ||
Kane SV. Systematic review: adherence issues in the treatment of ulcerative colitis. Aliment Pharmacol Ther. 2006;23(5):577–585. | ||
Hawthorne AB, Rubin G, Ghosh S. Review article: medication non-adherence in ulcerative colitis – strategies to improve adherence with mesalazine and other maintenance therapies. Aliment Pharmacol Ther. 2008;27(12):1157–1166. | ||
Kane S, Shaya F. Medication non-adherence is associated with increased medical health care costs. Dig Dis Sci. 2008;53(4):1020–1024. | ||
Sabate E. Adherence To Long-Term Therapies: Evidence For Action. Geneva: World Health Organization; 2003. Available from: http://www.who.int/chp/knowledge/publications/adherence_report/en/. Accessed August 25, 2016. | ||
Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487–497. | ||
Horne R, Parham R, Driscoll R, Robinson A. Patients’ attitudes to medicines and adherence to maintenance treatment in inflammatory bowel disease. Inflamm Bowel Dis. 2009;15(6):837–844. | ||
Kim SB, Kim KO, Jang BI, et al; Daegu-Gyeongbuk Gastrointestinal Study Group (DGSG). Patients’ beliefs and attitudes about their treatment for inflammatory bowel disease in Korea. J Gastroenterol Hepatol. 2016;31(3):575–580. | ||
Selinger CP, Eaden J, Jones DB, et al. Modifiable factors associated with nonadherence to maintenance medication for inflammatory bowel disease. Inflamm Bowel Dis. 2013;19(10):2199–2206. | ||
Dignass A, Lindsay JO, Sturm A, et al. Second European evidence-based consensus on the diagnosis and management of ulcerative colitis part 2: current management. J Crohns Colitis. 2012;6(10):991–1030. | ||
Shale MJ, Riley SA. Studies of compliance with delayed-release mesalazine therapy in patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2003;18(2):191–198. | ||
Kane SV, Cohen RD, Aikens JE, Hanauer SB. Prevalence of nonadherence with maintenance mesalamine in quiescent ulcerative colitis. Am J Gastroenterol. 2001;96(10):2929–2933. | ||
D’Incà R, Bertomoro P, Mazzocco K, Vettorato MG, Rumiati R, Sturniolo GC. Risk factors for non-adherence to medication in inflammatory bowel disease patients. Aliment Pharmacol Ther. 2008;27(2):166–172. | ||
Prantera C, Viscido A, Biancone L, Francavilla A, Giglio L, Campieri M. A new oral delivery system for 5-ASA: preliminary clinical findings for MMx. Inflamm Bowel Dis. 2005;11(5):421–427. | ||
Riley SA, Mani V, Goodman MJ, Lucas S. Why do patients with ulcerative colitis relapse? Gut. 1990;31(2):179–183. | ||
Vavricka S, Hofmann R, Guillaume X, et al. Prevalence and reasons for drug non-adherence in a European cohort of ulcerative colitis patients: the UCandME survey. J Crohns Colitis. 2015;9(Suppl 1):S327. | ||
Neiheisel MB, Wheeler KJ, Roberts ME. Medication adherence part one: understanding and assessing the problem. J Am Assoc Nurse Pract. 2014;26(1):49–55. | ||
Lam WY, Fresco P. Medication adherence measures: an overview. Biomed Res Int. 2015;2015:217047. | ||
Lee JK, Grace KA, Foster TG, et al. How should we measure medication adherence in clinical trials and practice? Ther Clin Risk Manag. 2007;3(4):685–690. | ||
Costa E, Giardini A, Savin M, et al. Interventional tools to improve medication adherence: review of literature. Patient Prefer Adherence. 2015;9:1303–1314. | ||
Kane SV. Overcoming adherence issues in ulcerative colitis. Gastroenterol Hepatol (N Y). 2007;3(10):795–799. | ||
Kane SV. Strategies to improve adherence and outcomes in patients with ulcerative colitis. Drugs. 2008;68(18):2601–2609. | ||
Ediger JP, Walker JR, Graff L, et al. Predictors of medication adherence in inflammatory bowel disease. Am J Gastroenterol. 2007;102(7):1417–1426. | ||
Lachaine J, Yen L, Beauchemin C, Hodgkins P. Medication adherence and persistence in the treatment of Canadian ulcerative colitis patients: analyses with the RAMQ database. BMC Gastroenterol. 2013;13:23. | ||
Kane S, Huo D, Aikens J, Hanauer S. Medication nonadherence and the outcomes of patients with quiescent ulcerative colitis. Am J Med. 2003;114(1):39–43. | ||
Levy RL, Feld AD. Increasing patient adherence to gastroenterology treatment and prevention regimens. Am J Gastroenterol. 1999;94(7):1733–1742. | ||
Greenberg RN. Overview of patient compliance with medication dosing: a literature review. Clin Ther. 1984;6(5):592–599. | ||
San Roman AL, Bermejo F, Carrera E, Pérez-Abad M, Boixeda D. Adherence to treatment in inflammatory bowel disease. Rev Esp Enferm Dig (Madrid). 2005;97(4):249–257. | ||
Robinson A, Hankins M, Wiseman G, Jones M. Maintaining stable symptom control in inflammatory bowel disease: a retrospective analysis of adherence, medication switches and the risk of relapse. Aliment Pharmacol Ther. 2013;38:531–538. | ||
Moody GA, Jayanthi V, Probert CS, Mac Kay H, Mayberry JF. Long-term therapy with sulphasalazine protects against colorectal cancer in ulcerative colitis: a retrospective study of colorectal cancer risk and compliance with treatment in Leicestershire. Eur J Gastroenterol Hepatol. 1996;8(12):1179–1183. | ||
Eaden J, Abrams K, Ekbom A, Jackson E, Mayberry J. Colorectal cancer prevention in ulcerative colitis: a case-control study. Aliment Pharmacol Ther. 2000;14(2):145–153. | ||
Bassi A, Dodd S, Williamson P, Bodger K. Cost of illness of inflammatory bowel disease in the UK: a single centre retrospective study. Gut. 2004;53(10):1471–1478. | ||
Kripalani S, Yao X, Haynes RB. Interventions to enhance medication adherence in chronic medical conditions: a systematic review. Arch Intern Med. 2007;167(6):540–550. | ||
Loftus EV Jr. A practical perspective on ulcerative colitis: patients’ needs from aminosalicylate therapies. Inflamm Bowel Dis. 2006;12(12):1107–1113. | ||
Kane S, Huo D, Magnanti K. A pilot feasibility study of once daily dosing versus conventional dosing mesalamine for maintenance of ulcerative colitis. Clin Gastroenterol Hepatol. 2003;1(3):170–173. | ||
Kamm MA, Lichtenstein GR, Sandborn WJ, et al. Randomized trial of once- or twice-daily MMX mesalazine for maintenance of remission in ulcerative colitis. Gut. 2008;57(7):893–902. | ||
Dignass A, Veerman H. Once versus twice-daily mesalazine (Pentasa) granules for the maintenance of remission in ulcerative colitis: results from a multinational randomised controlled trial. Gut. 2008;57(Suppl 1):A1. | ||
Li W, Zhan ZM, Jiang XL. Once daily vs multiple daily mesalamine therapy for mild to moderate ulcerative colitis: a meta-analysis. Colorectal Dis. 2016;18(7):O214–O223. | ||
Pedersen N, Thielsen P, Martinsen L, et al. eHealth: individualization of mesalazine treatment through a self-managed web-based solution in mild-to-moderate ulcerative colitis. Inflamm Bowel Dis. 2014;20(12):2276–2285. | ||
Elkjaer M, Shuhaibar M, Burisch J, et al. E-health empowers patients with ulcerative colitis: a randomised controlled trial of the web-guided ‘Constant-care’ approach. Gut. 2010;59(12):1652–1661. | ||
Moshkovska T, Stone MA, Smith RM, Bankart J, Baker R, Mayberry JF. Impact of a tailored patient preference intervention in adherence to 5-aminosalicylic acid medication in ulcerative colitis: results from an exploratory randomized controlled trial. Inflamm Bowel Dis. 2011;17(9):1874–1881. | ||
Castiglione F, Colombo GL, Valentino MC, Di Matteo S, Bruno GM. Patients’ perception of adherence to therapy in ulcerative colitis: results of a survey to specialized centers. Value Health. 2015;18(7):A629. | ||
Mitra D, Hodgkins P, Yen L, Davis KL, Cohen RD. Association between oral 5-ASA adherence and health care utilization and costs among patients with active ulcerative colitis. BMC Gastroenterol. 2012;12:132. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.