Back to Journals » Clinical Ophthalmology » Volume 13
Accelerated Epithelium-Off Corneal Collagen Cross-Linking For Keratoconus: 12-Month Results
Received 27 September 2019
Accepted for publication 22 October 2019
Published 4 December 2019 Volume 2019:13 Pages 2385—2394
DOI https://doi.org/10.2147/OPTH.S232118
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ismail Ahmed Nagib Omar, Hosny Ahmed Zein
Ophthalmology Department, Faculty of Medicine, Minia University, El-Minya, Egypt
Correspondence: Ismail Ahmed Nagib Omar
Ophthalmology Department, Faculty of Medicine, Minia University, P O Box 61519, El-Minya 61111, Egypt
Tel +201002554116
Email [email protected]
Purpose: The main aim of the study was to report visual, refractive, topographic, and aberrometric results of accelerated CXL in patients with keratoconus who were followed for 12 months and to highlight the important parameters that can be used in follow-up.
Settings: It was a prospective interventional non-randomized case series study, in which 40 keratoconus eyes of 40 patients were studied in the period between April 2016 and July 2018.
Methods: All eyes were examined preoperatively and post-accelerated CXL to evaluate visual acuity, refractive state, keratometric values, keratoconus indices, and corneal higher order aberrations (HOAs).
Results: The mean age of the studied patients was 28.4 ± 8.6 years (18–37years). One year after cross-linking, 11.6% of the eyes gained two lines of the UCVA, 26.4% of the eyes gained one line, 49.8% showed no change, 7.1% lost one line, and 5.1% lost two lines. Postoperative BCVA showed 13.7% of the eyes gained at least two lines, 32.5% gained one line, 49.9% had no change, and 3.9% lost one line. The keratometric values changed significantly after CXL; K1 decreased by a mean of 0.41D, K2 by 0.62D while Kmax by 1.57 D. The significant changes in keratoconus indices were in index of vertical asymmetry (IVA), index of surface variance (ISV), and keratoconus index (KI). Vertical coma, spherical aberrations, and trefoil decreased significantly at 12 months compared to baseline values (p = 0.04, 0.017, 0.025, respectively).
Conclusion: Keratoconus indices especially ISV, IVA, and KI along with HOAsparticularly vertical coma, spherical aberrations, and trefoil can add value beside keratometric readings in the follow-up of eyes treated with accelerated CXL.
Keywords: accelerated, cross-linking, keratoconus, aberrations
Introduction
Keratoconus is a degenerative corneal disorder in which there is progressive stromal thinning and conical protrusion that lead to progressive myopia, irregular astigmatism, and diminished vision.1
Collagen corneal cross-linking (CXL) is established as the standard of care for keratoconus and other corneal ectatic disorders, with proved efficacy in halting disease progression.1–3 The procedure induces cross-links between collagen fibrils using photosensitized riboflavin and ultraviolet A (UV-A) irradiation with resultant increased biomechanical rigidity and resistance of the cornea. The original Dresden protocol was the first in vivo clinical report in which instillation of eyedrops (composed of 0.1% riboflavin in 20% dextran) was done for 30 mins after corneal de-epithelization followed by 30 mins of UVA illumination at 3 mW/cm2 (5.4 J/cm2).4 Several modifications have then evolved; such as accelerated protocols in which irradiance is increased and duration shortened, trans-epithelial protocols where the procedure is performed through intact epithelium, and combining cross-linking with ring segment implantation or refractive surgery.2
Recently, accelerated or high-fluence protocols have been developed as an alternative to the lengthy conventional cross-linking procedure. The proposed advantages include decreased exposure time, better patient comfort, and lower risk of infection. High energy settings up to 30 mW/cm2 can shorten the procedure time from 30 to 3 mins with a total energy dose equal to that in conventional cross-linking with similar biological response.5,6 Accelerated CXL may be done in a pulsed or continuous mode. Pulsed mode hypothetically restarts the photo-polymerization reaction so additional oxygen concentration results with more oxygen release for CXL. As a result of intrastromal oxygen diffusion capacity and increased oxygen consumption associated with higher irradiances, there is limited biomechanical strengthening beyond irradiance of 50 mW/cm2 or exposure time less than 2 mins in animal tissue.7
Currently, most studies have reported similar, or even better, treatment efficiency of accelerated CXL compared to conventional CXL, but a few studies have reported the opposite and most of the work done on accelerated CXL was of short term.8–12 The current study aims to report the visual, refractive, topographic, and aberrometric results of accelerated CXL in patients with keratoconus who were followed for 12 months and to highlight the important parameters that can be used in follow-up.
Patients And Methods
This prospective interventional nonrandomized case series was conducted between April 2016 and July 2018 at Roaa Vision Correction Center and Minia University Ophthalmology Department.
We included 40 eyes of 40 consecutive keratoconus patients with age above 18 years, KC grades 1–3 according to Amsler-Krumeich classification and a pachymetry more than 400 microns plus epithelium. Documented signs of progression had to be present including Kmax increase more than one diopter, increase in corneal astigmatism by more than one diopter, increase in manifest refraction spherical equivalent by 0.50 diopter, or decrease in pachymetry more than 15 microns at a 3-month interval follow-up.
Patients with central or paracentral corneal opacities, acute hydrops, atopic disease, herpetic keratitis, evidence of active ophthalmic inflammation, autoimmune diseases, severe dry eye, pregnancy, and patients with previous ocular surgeries were excluded from the study.
The study was approved by the Ethical Committee of Minia University, Faculty of Medicine and adhered to the tenets of the Declaration of Helsinki. An informed written consent was signed by all participants after a thorough explanation of the nature of the study and surgical procedure, possible benefits, and potential complications. The study registration number is UMIN000036817.
Preoperative Evaluation
Careful history taking followed by comprehensive examinations was performed on all patients, including uncorrected distance visual acuity (UDVA) and corrected distance visual acuity (CDVA) measurement, manifest refraction, slit-lamp biomicroscopy, Goldmann applanation tonometry, and dilated fundus examination.
Corneal topography and corneal higher order aberration (HOA) analyses were performed using Scheimpflug-based topography system (Pentacam® HR OCULUS Optikgeräte GmbH). Corneal higher order aberrations were analyzed over a 3-mm zone and decomposed into Zernike polynomials up to the sixth order. Analysis included total HOA, astigmatism, coma, trefoil, quadrafoil, secondary astigmatism, and spherical aberration (Figures 1 and 2). Visual acuity measurements were converted to the minimal angle of resolution (LogMAR) for statistical purposes. The primary outcomes of the study were UDVA, CDVA, spherical equivalent and cylindrical values, keratometry (K) measurements (Kflat, Ksteep, Kaverage, and Kmax), central corneal thickness, and corneal HOA analyses. These parameters were evaluated at baseline and at 1, 3, 6, and 12 months post accelerated CXL.
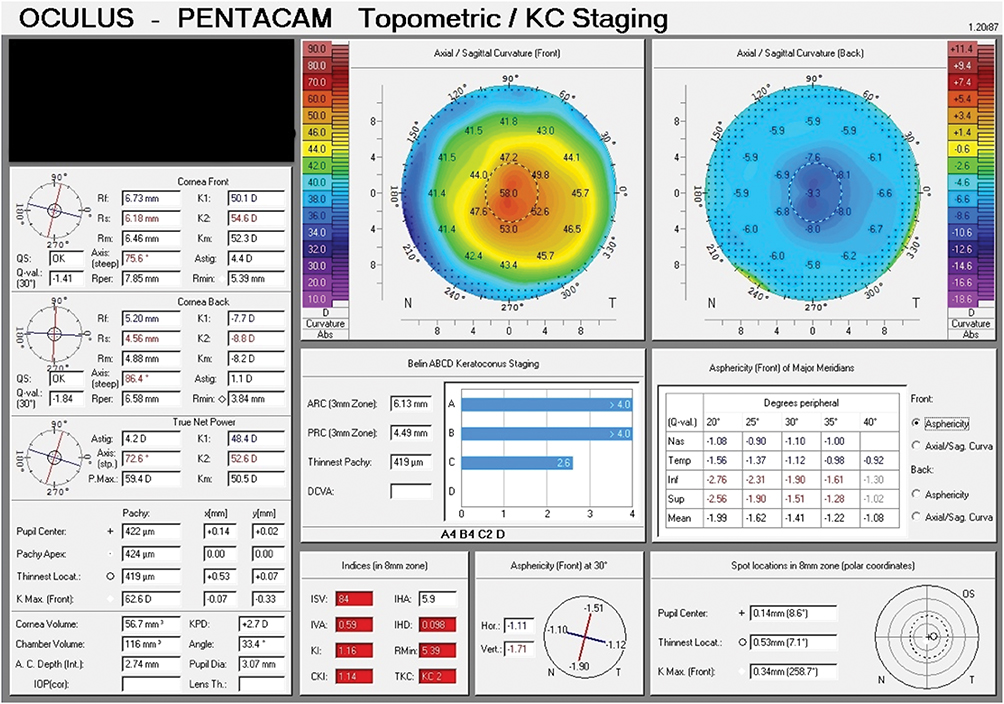 |
Figure 1 Preoperative topometric map of a keratoconus patient showing keratometric values, corneal thickness, and keratoconus indices. |
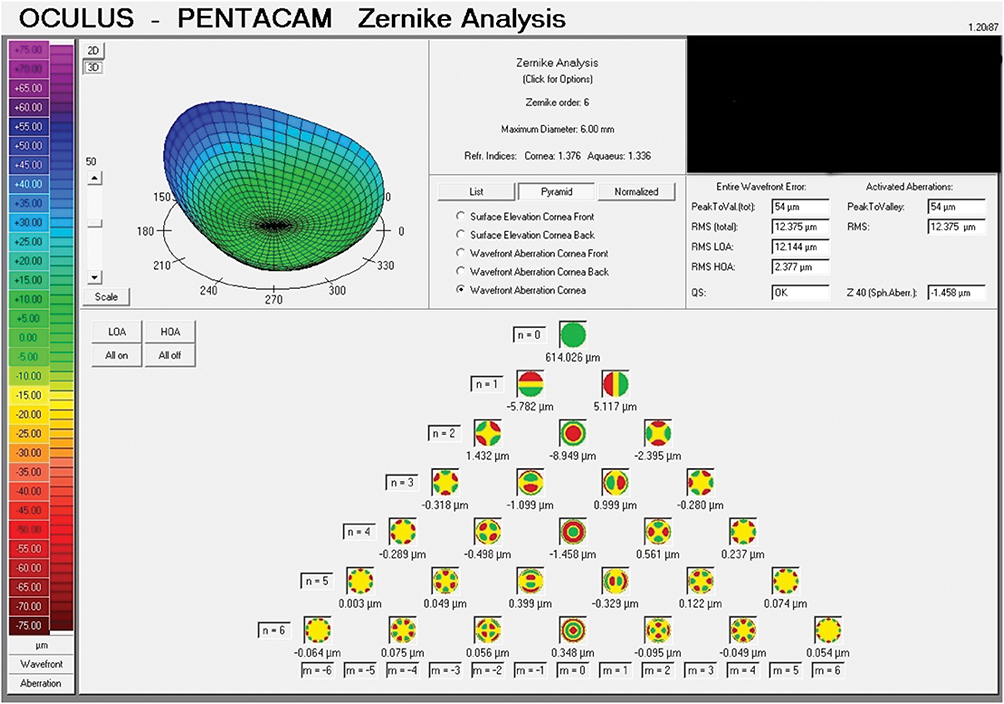 |
Figure 2 Preoperative aberration map showing all corneal aberrations of the same patient in Figure 1. |
Surgical Technique
Epithelium-off accelerated technique was used. The procedure was performed in the operating room under complete aseptic conditions. After topical anesthesia with benoxinate hydrochloride (Benox, EIPICO Ophthalmics, Egypt) eye drops four times 2 mins apart, a blunt spatula was used to debride the central 9 mm of the corneal epithelium. Riboflavin (0.1%solution VibeX; Avedro Inc., Waltham, MA) drops were instilled over the de-epithelized cornea four times every 2 mins. Exposure to 365 nm UVA by the Avedro’s KXL® system (Avedro Inc., Boston, MA) was performed with a total surface dose of 7.2 joules which was pulsed (1 s on, 1 s off) for 5 mins and 20 s, achieving a total delivery of 120 mWatt. A bandage contact lens was then applied.
Following the procedure, moxifloxacin 0.5% (Vigamox, Alcon, USA) eye drops were prescribed four times daily for 1 week, lubricant eye drops (Systane, Alcon, USA) five times daily for 1 month, and tobramycin/dexamethasone combination eye drops (TobraDex, Alcon, USA) three times daily for the first 2 weeks then replaced by fluorometholone acetate (0.1%, Efemyo, Orchidia Pharmaceutical, Egypt) four times daily, which was then tapered over 2 weeks.
Postoperative Evaluation
Patients were examined from the first day postoperatively and after 1 week for assessment of corneal re-epithelization where contact lens was removed. At 1, 3, 6, and 12 months after the procedure, patients were examined according to the study protocol. UCVA, BCVA, refraction, and corneal topography and aberrations were tested and recorded at each visit starting from 3rd month postoperatively to 12th month. Data collected during follow-up periods were used for comparison with baseline preoperative values.
Data Collection And Analysis
Data were collected from 4 maps refractive analysis and Zernike analysis of corneal topography preoperatively and postoperatively for all patients. Statistical analysis was performed using a commercially available software program (SPSS 18; SPSS, Chicago, IL, USA). Values were presented as mean and standard deviation (SD). Data were explored for normality using Kolmogorov–Smirnov test of normality. Paired (dependent) t-test was used to compare preoperative and postoperative values. P-value less than 0.05 was considered statistically significant.
Results
Forty eyes of 40 patients were enrolled in this study with 18 males and 22 females. The mean age of them was 28.4 ± 8.6years (18–37 years).
Visual, Refractive, And Topographic Changes
Postoperative changes in UCVA, BCVA, MRSE (manifest refraction spherical equivalent), K1, K2, corneal astigmatism, and Kmax are displayed in Table 1. There were significant changes in both UCVA and BCVA at 1-year follow-up (P-value 0.01 and 0.02, respectively) where postoperative visual acuity was improved when compared with preoperative values.
 |
Table 1 Visual, Refractive, And Keratometric Changes Before And After Acc CXL |
One year after cross-linking, 11.6% of the studied eyes gained two lines of UCVA, 26.4% gained one line, 49.8% showed no change, 7.1% lost one line, and 5.1% lost two lines. Postoperative BCVA showed 13.7% of the eyes gained at least two lines, 32.5% gained one line, 49.9% had no change, and 3.9% lost one line. MRSE was reduced postoperatively, but this reduction was not of statistical significance.
Keratometric values (K1, K2, and Kmax) decreased significantly 1 year after surgery (P-value 0.002, 0.0001 and 0.029, respectively) compared to baseline values. At 1 year after CXL, K1 decreased by a mean of 0.41D, K2 by 0.62D while Kmax was reduced by 1.57 D. At the 12-month follow-up, Kmax values were stable in 51.3% of the eyes, reduced by 1–2 D in 35.4% of the eyes, and decreased 2 D or more in 14.3% of the eyes. No eye showed an increase of Kmax. As regards corneal astigmatism, it showed statistically significant reduction at the end of one-year post cross-linking (P-value 0.03).
Corneal Thickness And Corneal Volume Changes
Corneal thickness and corneal volume (Table 2) showed significant changes 1 year after accelerated CXL where central corneal thickness decreased by mean of about 10µ (P=0.0001). Thinnest location also decreased significantly by mean difference of 10.38µ (P=0.0001), and corneal volume decreased by one micron (P=0.001) compared to baseline values.
 |
Table 2 Corneal Thickness And Corneal Volume Pre- And Post-CXL |
Keratoconus Indices Changes
There was significant reduction in index of vertical asymmetry (IVA), index of surface variance (ISV), keratoconus index (KI) post cross-linking, while index of height asymmetry (IHA) and index of highest decentration (IHD) showed statistically insignificant changes from baseline values (P-values >0.05) as shown in Table 3.
 |
Table 3 Keratoconus Indices Pre- And Post-CXL |
Corneal HOA Changes
Total corneal aberration, total HOA, and horizontal coma showed insignificant changes at 12 months relative to baseline (P=0.127, 0.131, and 0.665, respectively). Vertical coma, spherical, and trefoil (which causes a point of light to spread in three directions) aberrations decreased significantly at 12 months compared to baseline values (P=0.04, 0.017, and 0.025, respectively) (Table 4). Figures 3 and 4 show postoperative changes in the same patient of Figures 1 and 2, which is one of our studied patients.
 |
Table 4 Higher Order Aberrations Pre- And Post-CXL |
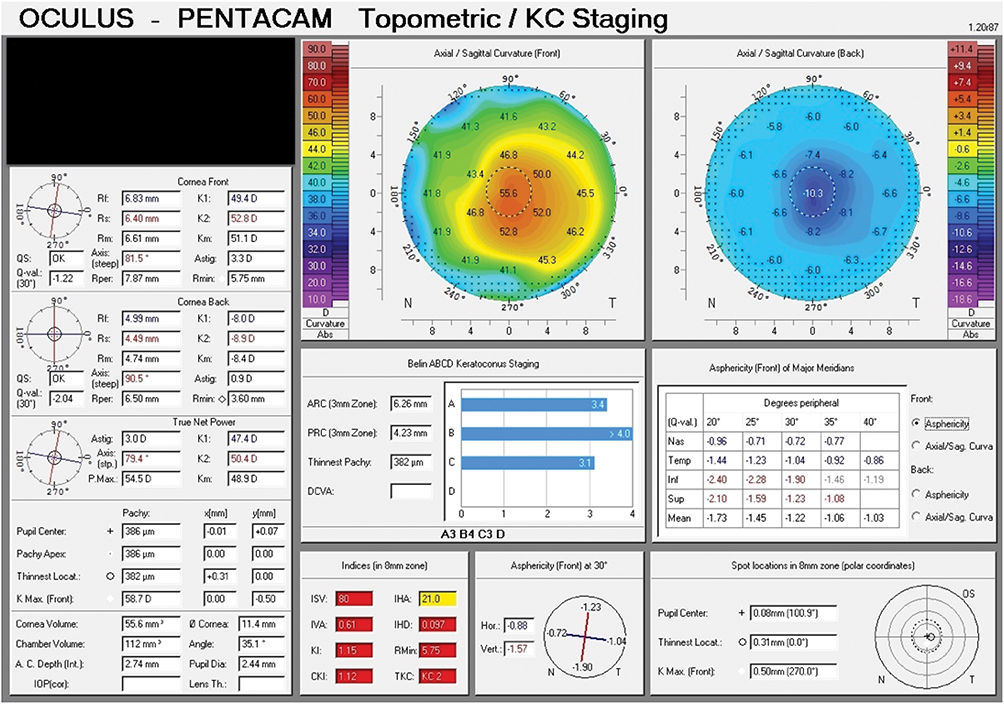 |
Figure 3 Topometric map of the same patient 1 year after CXL. It shows improvements in Kmax and keratoconus indices with decreased corneal thickness. |
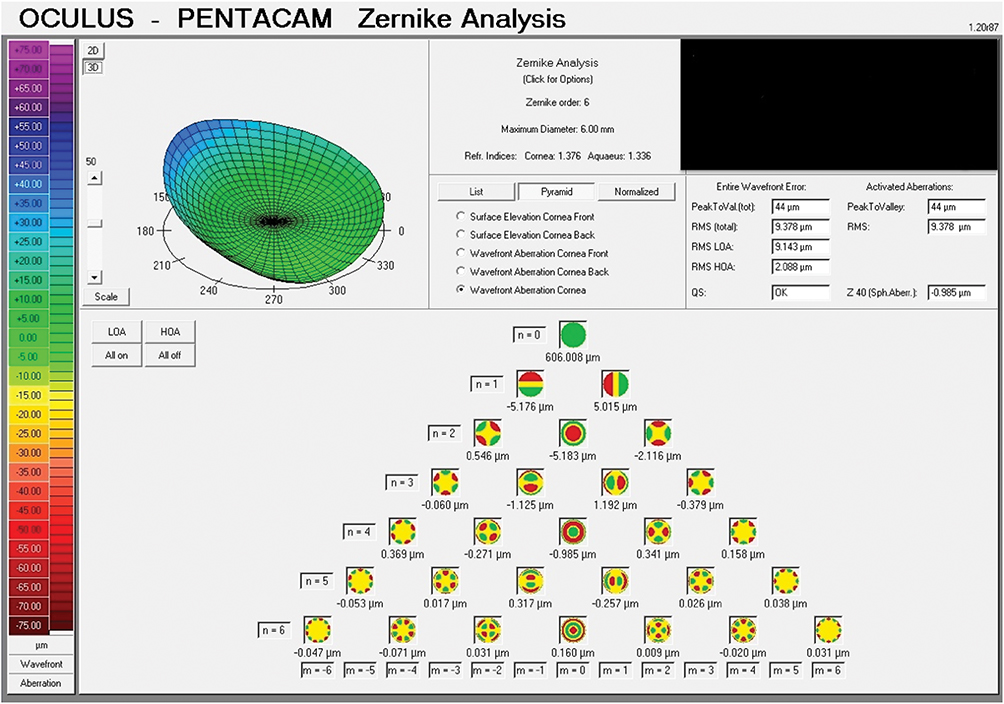 |
Figure 4 One-year postoperative aberration map showing improvement in most of the studied aberrations when compared with Figure 2. |
Complications
Subepithelial haze was noted in 91.5% of the cases which was transient and resolved over 3–6 weeks. Delayed re-epithelialization occurred in 5 eyes (12.5%) where contact lenses were changed until complete healing up to 2 weeks.
Discussion
Corneal collagen cross-linking is a minimally invasive procedure that was introduced to slow down or halt further progression of keratoconus. Recent medical devices with higher energy output settings have shortened CXL treatment time. Higher energy parameters (up to an irradiance of 30 mW/cm2) combined with shorter treatment time (3–10 mins) are utilized in accelerated corneal CXL to obtain the same total radiant energy of standard CXL. This accelerated protocol has shown promising results in stabilization of progressive keratoconus.13,14 The current study evaluated the 12-month results of accelerated CXL with a total dose of 7.2 J/cm2 for cases of progressive keratoconus.
The main effect of CXL as suggested by many authors was consistent stabilization effect, but also variable degree of corneal flattening was addressed in most patients.15–17 However, other studies did not find statistically significant differences between preoperative and postoperative refractive, keratometric, and pachymetric data.18
The current study found statistically significant improvement in both UCVA and BCVA in agreement with a study done by Bozkurt et al, who reported that both BCVA and UCVA improved significantly when compared with pre-cross-linking values. Also, their detailed analysis about BCVA was approximately similar to our results as they found an improvement in BCVA by two lines in 14.8%, one line in 31.9%, 48.9% had no change, and 4.2% lost one line at the end of follow-up period of 2 years.19
Elbaz et al evaluated 1-year results of accelerated cross-linking (irradiance of 9 mW/cm2 for 10 mins) in keratoconus-affected eyes and they did not find statistically significant changes in the mean BCVA, but significant improvement in the mean UCVA at 12 months after CXL.14 Also, Mita et al found the same results after 6 months of accelerated CXL of eyes with keratoconus.20 However, other studies did not show any significant improvement in either UCVA or BCVA at the end of their follow-up periods.21,22
In a study done by El-Massry et al, they found a statistically significant reduction in mean K reading. The preoperative mean K was 47.21±3.18 D and changed to 44.14±2.09 D with a difference of means of about 3D.23 This finding was also addressed by Caporossi et al, who recorded topographic mean reduction in dioptric power of about 2 D, but they reported initial worsening of keratometric readings in the first month which might have been due to transient haze and corneal edema.24 The current study results reported that keratometric values (K1, K2, and Kmax) had significantly lower values 1 year after the surgery compared to baseline values. In other studies that analyzed the changes of Kmax after cross-linking, a significant improvement of 1.12 D was reported after 4 years of follow up in a study published in 2017.25
An improvement of 1.6 D in Kmax was reported 1 year after cross-linking in a multicenter trial performed in the US.26
In agreement with our study, Greenstein et al conducted a prospective randomized controlled clinical trial on 71 eyes of keratoconus and post-lasik ectasia and reported significant improvements in the ISV, IVA, and KI at 1 year compared with baseline.27 In another study, they found significant reduction in ISV and IHD, but in ours, there was no improvement in IHD.28
In this work, we recorded the corneal thickness before and after the procedure. Statistically significant corneal thinning was found after the procedure as reported by many other previous studies.23,29 This thinning can be explained by postoperative keratocyte apoptosis and structural changes in corneal collagen fibrils and extracellular matrix in the anterior stroma.
One of the optical sequelae of keratoconus is increased HOAs that result in vision deterioration and visual dysfunction.30 Eyes treated with corneal cross-linking showed significant improvement in HOAs when compared to untreated eye in patients with bilateral keratoconus.31
In a study performed recently, statistically significant improvement in HOAs was observed in two different types of accelerated corneal cross-linking using different power settings.32 In an earlier study performed using epi-on technique, they found an initial improvement in corneal HOAs in the first 6 months followed by insignificant changes in HOAs.33 However, a later study showed significant improvement in all elements of HOAs except trefoil after transepithelial corneal collagen cross-linking.34 Greenstein et al found general improvements in HOAs after CXL. In particular, they found that total HOAs and coma significantly improved after CXL.35
In the current study, we found a statistically significant improvement in spherical aberrations, vertical coma, and trefoil while improvement in total aberrations and HOAs was nonsignificant. These results are relatively different from the results found by El-Massry et al who found that total HOAs and total coma were significantly reduced at 6 months by 25% and 18%, respectively. Significant improvement was seen in spherical aberration by 8.71%, while no significant change was observed in trefoil.23 As stated before, the main changes in HOAs after corneal cross-linking were in the coma, particularly vertical coma, and spherical aberrations. Also, this study adds the importance of trefoil.
Although our results were encouraging and largely agree with both published evidence on standard CXL and with recently published studies on accelerated CXL, it has some limitations as small number of eyes, needs longer period of follow-up with different energy settings in a larger number of eyes to validate these results.
It can be concluded that keratoconus indices especially ISV, IVA, and KI along with HOAs particularly vertical coma, spherical aberrations, and trefoil can add value beside keratometric readings in the follow-up of eyes treated with accelerated CXL.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42:297–319. doi:10.1016/S0039-6257(97)00119-7
2. Konstantopoulos A, Mehta JS. Conventional versus accelerated collagen cross-linking for keratoconus. Eye Contact Lens. 2015;41(2):65–71. doi:10.1097/ICL.0000000000000093
3. Mastropasqua L. Collagen cross-linking: when and how? A review of the state of the art of the technique and new perspectives. Eye Vis (Lond). 2015;2:19. doi:10.1186/s40662-015-0030-6
4. Wollensak G, Spoerl E, Seiler T. Riboflavin/ultraviolet-a-induced collagen crosslinking for the treatment of keratoconus. Am J Ophthalmol. 2003;135(5):620–627. doi:10.1016/S0002-9394(02)02220-1
5. Schumacher S, Oeftiger L, Mrochen M. Equivalence of biomechanical changes induced by rapid and standard corneal cross-linking, using riboflavin and ultraviolet radiation. Invest Ophthalmol Vis Sci. 2011;52(12):9048–9052. doi:10.1167/iovs.11-7818
6. Hammer A, Richoz O, Arba Mosquera S, Tabibian D, Hoogewoud F, Hafezi F. Corneal biomechanical properties at different corneal cross-linking (CXL) irradiances. Invest Ophthalmol Vis Sci. 2014;55(5):2881–2884. doi:10.1167/iovs.13-13748
7. Wernli J, Schumacher S, Spoerl E, Mrochen M. The efficacy of corneal cross-linking shows a sudden decrease with very high intensity UV light and short treatment time. Invest Ophthalmol Vis Sci. 2013;54(2):1176–1180. doi:10.1167/iovs.12-11409
8. Hashemian H, Jabbarvand M, Khodaparast M, Ameli K. Evaluation of corneal changes after conventional versus accelerated corneal cross-linking: a randomized controlled trial. J Refract Surg. 2014;30(12):837–842. doi:10.3928/1081597X-20141117-02
9. Shetty R, Pahuja NK, Nuijts RM, et al. Current protocols of corneal collagen cross-linking: visual, refractive, and tomographic outcomes. Am J Ophthalmol. 2015;160(2):243–249. doi:10.1016/j.ajo.2015.05.019
10. Ng AL, Chan TC, Cheng AC. Conventional versus accelerated corneal collagen cross-linking in the treatment of keratoconus. Clin Experiment Ophthalmol. 2016;44(1):8–14. doi:10.1111/ceo.12571
11. Hashemi H, Fotouhi A, Miraftab M, et al. Short-term comparison of accelerated and standard methods of corneal collagen crosslinking. J Cataract Refract Surg. 2015;41(3):533–540. doi:10.1016/j.jcrs.2014.07.030
12. Chow VW, Chan TC, Yu M, Wong VW, Jhanji V. One-year outcomes of conventional and accelerated collagen crosslinking in progressive keratoconus. Sci Rep. 2015;5:14425. doi:10.1038/srep14425
13. Fard AM, Sorkhabi RD, Khazaei M, Nader ND. The effects of collagen cross-linking on corneal density: a comparison between accelerated and conventional methods. Int Ophthalmol. 2019;39(7):1559–1566. doi:10.1007/s10792-018-0961-8
14. Elbaz U, Shen C, Lichtinger A, et al. Accelerated (9-mW/cm2) corneal collagen crosslinking for keratoconus—A 1-year follow-up. Cornea. 2014;33(8):769–773. doi:10.1097/ICO.0000000000000154
15. Hoyer A, Raiskup‑Wolf F, Spörl E, Pillunat LE. Collagen cross‑linking with riboflavin and UVA light in keratoconus. Results from Dresden. Ophthalmologe. 2009;106(2):133–40.
16. Sadoughi MM, Feizi S, Delfazayebaher S, Baradaran-Rafii A, Einollahi B, Shahabi C. Corneal changes after collagen crosslinking for keratoconus using dual scheimpflug imaging. J Ophthalmic Vis Res. 2015;10(4):358–363. doi:10.4103/2008-322X.176894
17. Kim TG, Kim KY, Han JB, Jin KH. The long-term clinical outcome after corneal collagen cross-linking in Korean patients with progressive keratoconus. Korean J Ophthalmol. 2016;30(5):326–334. doi:10.3341/kjo.2016.30.5.326
18. Mora M, Rosenstiehl S, Rios HA, Lonngi M. Refractive changes after two years accelerated corneal cross-linking in patients with keratoconus. Vis Pan-Am. 2017;16(4):114–117.
19. Bozkurt E, Ozgurhan EB, Akcay BI, et al. Refractive, topographic, and aberrometric results at 2-year follow-up for accelerated corneal cross-link for progressive keratoconus. J Ophthalmol. 2017;2017:5714372.
20. Mita M, Waring GO
21. Ozgurhan EB, Akcay BI, Kurt T, Yildirim Y, Demirok A. Accelerated corneal collagen cross-linking in thin keratoconic corneas. J Refract Surg. 2015;31(6):386–390. doi:10.3928/1081597X-20150521-11
22. Waszczykowska A, Jurowski P. Two-year accelerated corneal cross-linking outcome in patients with progressive keratoconus. Biomed Res Int. 2015;2015:325157. doi:10.1155/2015/325157
23. El-Massry AA, Dowidar AM, Massoud TH, Tadros BGD. Evaluation of the effect of corneal collagen cross-linking for keratoconus on the ocular higher-order aberrations. Clin Ophthalmol. 2017;9(11):1461–1469. doi:10.2147/OPTH.S142167
24. Caporossi A, Mazzotta C, Baiocchi S, Caporossi T. Long-term results of riboflavin ultraviolet a corneal collagen cross-linking for keratoconus in Italy: the Siena eye cross study. Am J Ophthalmol. 2010;149(4):585–593. doi:10.1016/j.ajo.2009.10.021
25. Toosi LS, Khakshour H, Esmaily H, Daneshvar R. Long-term outcome of corneal cross-linking for the treatment of progressive keratoconus. Int J Med Res Health Sci. 2017;6(9):45–49.
26. Hersh PS, Stulting RD, Muller D, Durrie DS, Rajpal RK. United States multicenter clinical trial of corneal collagen crosslinking for keratoconus treatment. Ophthalmology. 2017;124(9):1259–1270. doi:10.1016/j.ophtha.2017.03.052
27. Greenstein SA, Fry KL, Hersh PS. Corneal topography indices after corneal collagen crosslinking for keratoconus and corneal ectasia: one-year results. J Cataract Refract Surg. 2011;37(7):1282–1290. doi:10.1016/j.jcrs.2011.01.029
28. Steinberg J, Ahmadiyar M, Rost A, et al. Anterior and posterior corneal changes after crosslinking for keratoconus. Optom Visc Sci. 2014;91(2):178–186.
29. Sedaghat M, Bagheri M, Ghavami S, Bamdad S. Changes in corneal topography and biomechanical properties after collagen cross linking for keratoconus: 1-year results. Middle East Afr J Ophthalmol. 2015;22(2):212–219. doi:10.4103/0974-9233.151877
30. Schlegel Z, Lteif Y, Bains HS, Gatinel D. Total, corneal, and internal ocular optical aberrations in patients with keratoconus. J Refract Surg. 2009;25:951–957. doi:10.3928/1081597X-20090915-10
31. Filippello M, Stagni E, O’Brart D. Transepithelial corneal collagen crosslinking: bilateral study. J Cataract Refract Surg. 2012;38:283–291. doi:10.1016/j.jcrs.2011.08.030
32. Kirgiz A, Eliacik M, Yildirim Y. Different accelerated corneal collagen cross-linking treatment modalities in progressive keratoconus. Eye Vis (Lond). 2019;6:16. doi:10.1186/s40662-019-0141-6
33. Caporossi A, Mazzotta C, Paradiso AL, Baiocchi S. Marigliani D and Caporossi T. Transepithelial corneal collagen crosslinking for progressive keratoconus: 24-month clinical results. J Cataract Refract Surg. 2013;39(8):1157–1163. doi:10.1016/j.jcrs.2013.03.026
34. Mo’mena AA, Moamen S, Ahmed A, Tamer EM, Rafeek EG. Assessment of corneal higher order aberrations before and after corneal collagen cross-linking in patients with keratoconus. Egypt J Hospital Med. 2018;72(3):4100–4104. doi:10.21608/ejhm.2018.9123
35. Greenstein SA, Fry KL, Hersh MJ, Hersh PS. Higher-order aberrations after corneal collagen crosslinking for keratoconus and corneal ectasia. J Cataract Refract Surg. 2012;38(2):292–302. doi:10.1016/j.jcrs.2011.08.041
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.