Back to Journals » Clinical Ophthalmology » Volume 14
A Unique Experience of Retinal Diseases Screening in Nepal
Authors Shrestha A ![]() , Khatri B
, Khatri B ![]() , Naito T
, Naito T ![]()
Received 24 April 2020
Accepted for publication 2 July 2020
Published 21 July 2020 Volume 2020:14 Pages 2037—2042
DOI https://doi.org/10.2147/OPTH.S259274
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Arjun Shrestha,1 Bijay Khatri,2 Takeshi Naito3
1Department of Ophthalmology, BP Eye Foundation, Hospital for Children, Eye, ENT & Rehabilitation Services, Bhaktapur, Bagmati Province, Nepal; 2Academic and Research Department, BP Eye Foundation, Hospital for Children, Eye, ENT & Rehabilitation Services, Bhaktapur, Bagmati Province, Nepal; 3Department of Ophthalmology, Tokushima University Hospital, Tokushima, Japan
Correspondence: Arjun Shrestha
Department of Ophthalmology, BP Eye Foundation, Hospital for Children, Eye, ENT & Rehabilitation Services, Bhaktapur, Bagmati Province, Nepal
Tel +977 1 6631705
Fax + 977 1 6639735
Email [email protected]
Background: Recently, the number of retinal patients is increasing in Nepal. The retinal problems are the second common cause of blindness in Nepal. Retinal diseases are challenging to manage due to the lack of simple and cost-effective screening methods, limited human resources, poverty, and lack of awareness in Nepal. Hospital for Children, Eye, ENT & Rehabilitation Services (CHEERS), Nepal conducted retina screening camps and education in communities through Retina Eye Care of Nepal project (RECON) in the years 2017 and 2018.
Materials and Methods: We screened retinal patients with an indirect ophthalmoscope coupled with plus 20 Dioptre lens and portable fundus camera. We referred the patients needing interventions to the base hospital (CHEERS) using a screening algorithm, where they received retinal laser and surgery. Besides, we also provided on-site educational programs for retinal disease awareness to the community.
Results: Retinal problems found from two static outreach clinics (SORC) and a day screening and treatment service (DSTS) were 18.3%, 20%, and 20%, respectively, while from a remote rural health camp (RRHC) was 2.61%. Likewise, patients referred to CHEERS for retinal laser or other retinal interventions were 15%, 16.6%, 16%, and 1.96% from 2 SORCs, 1 DSTS, and 1 RRHC, respectively.
Conclusion: Retina camp is a cost-effective approach to early detection and referral for retinal-related vision impairment patients. It is also one opportunity to educate the community. The purpose of the project was to provide retina care to the community who otherwise could not afford it. We recommend a similar screening model on a large scale in a low-resource setting for the maximum benefits to the rural community.
Keywords: screening, retina camp, Nepal, outreach
Introduction
The number of people blind because of retinal diseases like diabetic retinopathy (DR), age-related macular degeneration (AMD), and others are increasing in Nepal. The posterior segment eye diseases (PSED) are now the second common cause of blindness in Nepal.1 Early diagnoses, prompt treatment, and referral are very crucial to prevent retina related visual morbidity. Unless a fact of public health importance of PSED reach to a level of policymakers, VISION 2020: The Right to Sight’s aims of alleviating suffering from avoidable blindness cannot be addressed.2
Retinal diseases are emerging as the challenging threat of vision-loss globally. AMD and DR contributed to the third and fifth causes of global visual impairment and blindness, respectively.3–6 Retinal diseases are the second cause of blindness after cataracts in developing countries and this is a serious issue because of low-resource setting.7 PSED should now be considered as of particular public health significance; which has impaired the quality of life, productivity and economy in the community. The poverty, socioeconomic issues, illiteracy, lack of awareness, difficult access to eye and health care are other hindering factors to reach the unreached in the poor countries.8
To address this problem, Hospital for Children, Eye, ENT & Rehabilitation Services (CHEERS), a tertiary eye hospital located at Bhaktapur, Nepal, started a community-based novel method of PSED screening, education, counseling, and referral system. This was one of the objectives of the Retina Eye Care of Nepal (RECON) project.
Materials and Methods
This study was a part of the RECON project. We adhered to the tenet of the Helsinki declaration. The project implementing organization, BP Eye Foundation approved the permission to publish project output. Ethical approval was obtained from the hospital’s local ethical review committee, and informed consent was waived off in this retrospective study, where the participants were de-identified or could not be contacted. (Reference No. 522–076/077).
Screening Clinics
The hospital conducts three types of outreach programs:
Remote Rural Health Camp (RRHC)
The Surgical eye camp is a very successful model in Nepal. We conduct this free cataract surgery focused camp in a rural and remote area, which typically lasts five days trip. The first day is dedicated to the preparation of the clinic and the temporary operating room. Screening and surgery are conducted side by side on the second and third day, postoperative patient’s examination and discharge are done on the fourth day, and the fifth day is a returning day.
We conduct this type of surgical clinic in coordination and partnership with local organizers. These organizers play a crucial role in advertising the upcoming clinic activities through pamphlets, flex prints, and radio broadcasting. The hospital provides technical support like human resources, diagnostic and surgical equipment, free medications and cataract, and other minor surgeries at the temporary surgical clinic. RRHC can expand its services with additional “opportunistic” retina screening care. We conducted retina camp in Risthe in Ramechhap, 8 hours drive from the base hospital as a part of RRHC from May 26 to 30, 2017.
Day Screening and Treatment Services (DSTS)
Screening camps are organized within the Kathmandu valley for people who cannot come to the hospital. They are conducted weekly in partnership with a health post, village health committee, local clubs, and community-based organizations in different locations. We organized retina camp in Lele, Lalitpur 1 and ½ hour drive from the base hospital in partnership with a local health club on January 8, 2018.
Static Outreach Clinic (SORC)
The hospital conducts regular static satellite clinics at Chapagaun (Lalitpur district), Bode (Bhaktapur district), and Pharping (Kathmandu district) one day per week. All these clinics are within an hour’s drive from the base hospital. A trained ophthalmic assistant from the hospital runs the clinic with other supporting staff. The patients are referred to the hospital if patients are not amenable to be managed at the local clinic. Among them, we used two static satellite clinics for the retina screening program.
Bajrabarahi Primary Health Centre and Godawari Municipality, Lalitpur conducted the free extensive health camp one week before the proposed Retina camp day. They informed the patients with a history of diabetes and hypertension about the opportunity for screening retinal diseases on free retina camp. The flex posters mentioning the Retina Camp date and venue were displayed in front of the health center, in Bus Park and in front of the Godawari Municipality office, which is just located in front of the health center. We conducted the retina screening in Chapagun SORC on June 28, 2018.
Maternal and Child Health Clinic, Bode, Bhaktapur is one of the static satellite Eye and ENT clinics of CHEERS. This clinic runs general comprehensive health services every day. This was an opportunity to conduct an outreach-based retina camp for diabetic and hypertensive patients visiting this clinic. They informed the patients with a history of diabetes and hypertension about the opportunity for screening retinal diseases on free retina camp to be held two weeks later. They also displayed the flex poster mentioning the Retina Camp date and venue in front of the clinic. We conducted the retina screening in Bode SORC on September 26, 2018.
Retina Screening Algorithm
Figure 1 shows a retina screening algorithm followed in the screening of retinal patients in outreach retina camps conducted by the hospital.
 |
Figure 1 Showing Retina Screening Algorithm. Abbreviations: FEUM, fundus evaluation under mydriasis; CHEERS, Hospital for Children, Eye, ENT & Rehabilitation Services; ACD, anterior chamber depth; mg/dl, milligrams/decilitres. |
We developed a proforma based on the algorithm to screen the patients coming to the camp. We inquired the patients about their age, status of diabetes, hypertension, and any retinal diseases and advised for fundus evaluation. We also enquired them about awareness of diabetic retinopathy and the status of the previous dilation of pupils.
The patients above 30 years of age were given the opportunity for free random blood sugar test (rapid test). If random blood sugar was above 200 mg/dl, the patient was labeled as Diabetic Mellitus (DM) as per definition from the American Diabetic Association and advised for fundus evaluation.9 Patients above 50 years of age were counseled for fundus examination under mydriasis (FEUM) to detect possible AMD.10 Eye drop Tropicamide 1% and Phenylephrine 2.5% was used to dilate pupils of both eyes of the patient unless the patient is hypertensive for whom Eye drops 1% Tropicamide was used for FEUM. FEUM was not done if Van Herrick Grading shows grade I or II shallow anterior chamber depth (ACD). In such a case, a nonmydriatic fundus camera (Visuscout 100, Zeiss company, Germany) was used to capture the fundus image. A portable fundus camera was also used to capture the image of fundus if positive findings suggestive of retinal problems. Patients needing intervention like a retinal laser, intravitreal antivascular endothelial growth factor (VEGF) injection, or surgery were referred to the hospital. The additional piece of equipments required in retinal screening was indirect ophthalmoscope and 20 Diopter lens.
Information and education materials in the form of a small booklet for common retinal diseases like diabetic retinopathy were distributed to the patients and visitors. Posters and flex prints were hanged in the wall of screening venue about the importance of eye check-up. A community eye health worker was also answering any queries among the visitors.
Result
Table 1 shows the total numbers of patients screened by a single retina specialist in one-day SORC and DSTS at Chapagaun, Bode, and Lele were 60, 60, and 65, respectively. One hundred fifty-three patients were examined in two days at Risthe RRHC. Female outnumbered males in service utilization in screening camps. Distribution of DM and Hypertension was almost similar in DSTS and SORC but relatively low in RRHC. Awareness about DM causing vision problems was found in 43.3–49% of diabetic patients, but FEUM was done previously only in 34.48–45.45% of those aware patients in SORC and DSTS. Likewise, patients referred to CHEERS for retinal laser or other retinal interventions were 15%, 16.6%, 16%, and 1.96% from 2 SORCs, 1 DSTS, and 1 RRHC, respectively.
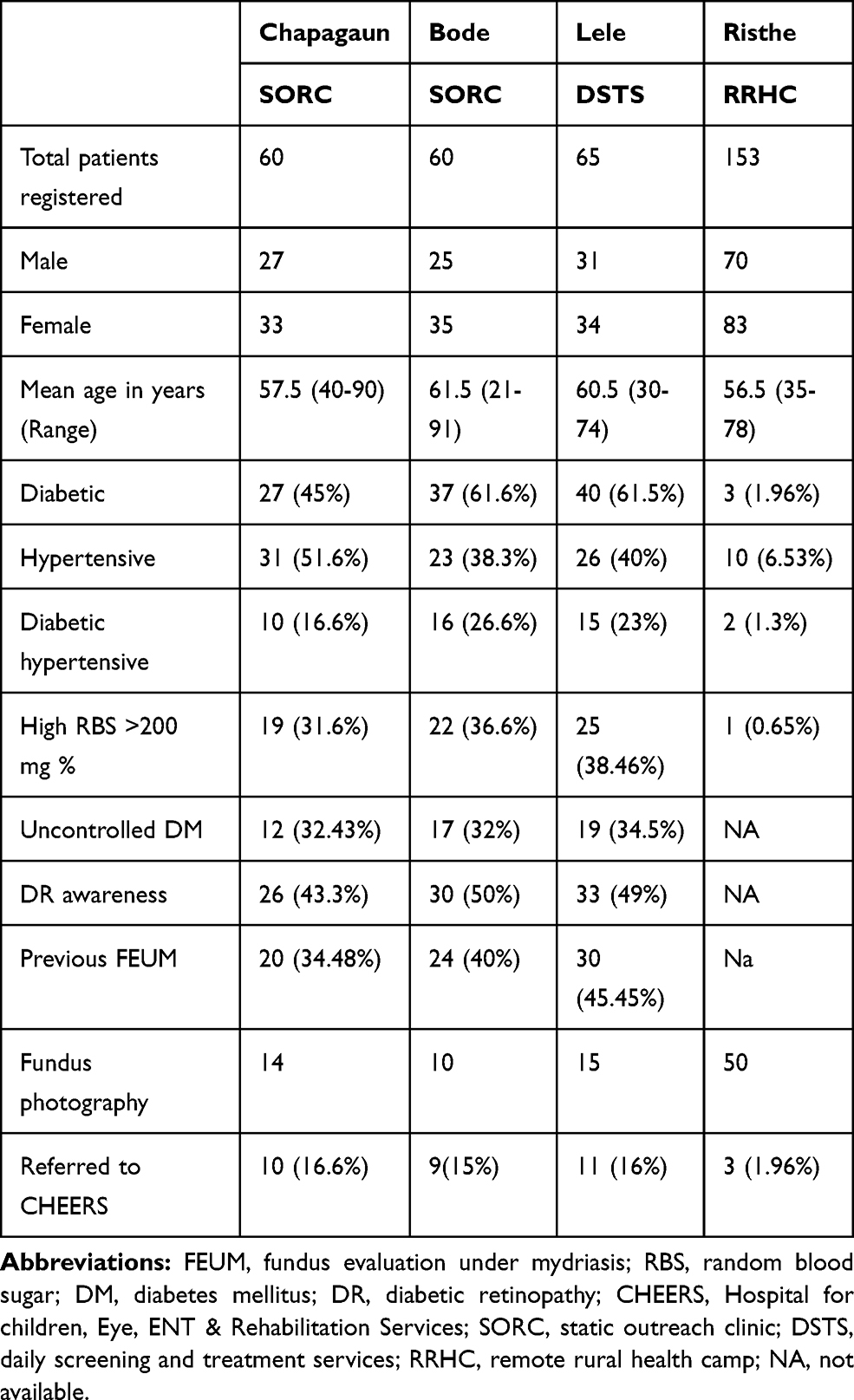 |
Table 1 Data of Retina Screening Patients |
Table 2 depicts about 20% of patients had retinal problems at SORC and DSTS, while only 2.61% of retinal issues were found at RRHC.
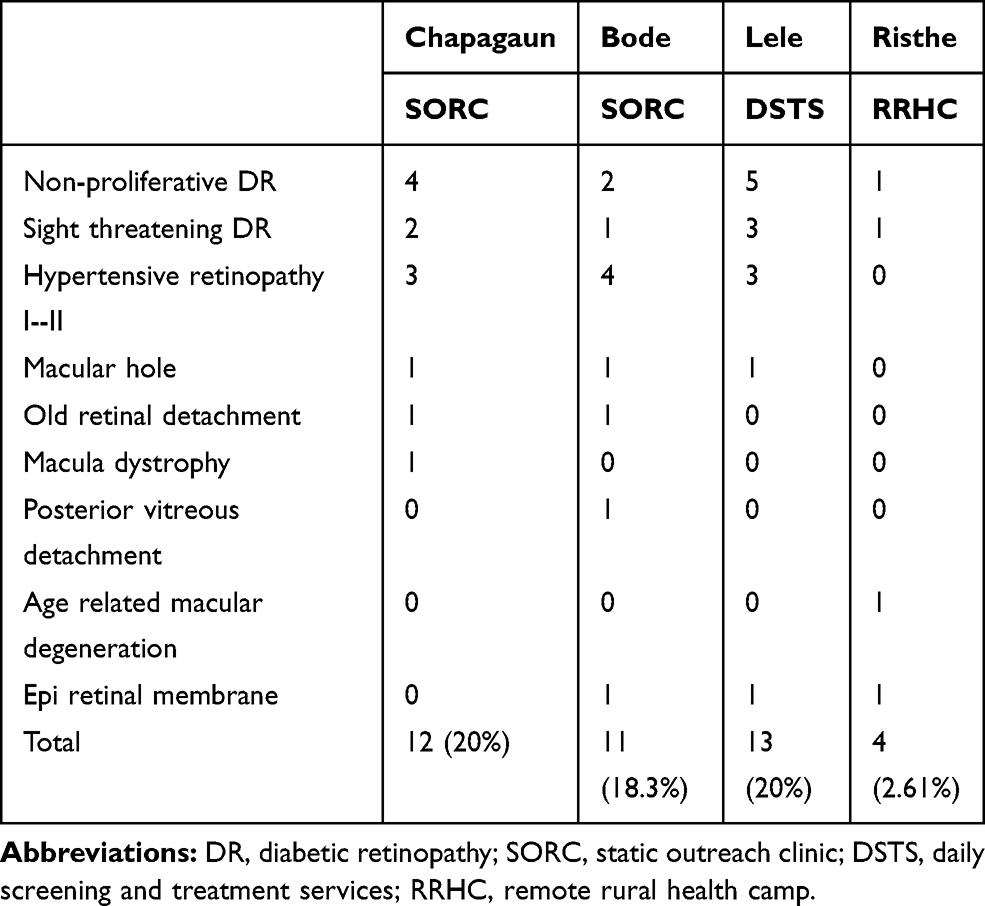 |
Table 2 Data of Retinal Diseases Distribution |
Discussion
We found awareness about DM causing vision problems in 43.3–49% of diabetic patients in this study. There are varying reports on the level of awareness in Nepal. According to the Bhaktapur retina study, only 11.5% of study subjects were aware of DR, and 40% of subjects with diabetes were aware of DR.11 Other studies conducted in Nepal among the diabetic population revealed that almost 50% were aware of DR.12
We are so much focused on finding retinal lesions for us to treat with laser, intravitreal Bevacizumab, or vitreous surgery, while these are important for educating patients is even more critical, simultaneously. Unfortunately, we have little time during the camps. However, we should develop an alternative. That half the patients who knew they had DM did not realize about DR, probably because their doctors treating their DM did not tell them that an eye examination is necessary or told them only casually. Many people with diabetes had high or uncontrolled DM, which is also significant observation because it is not diabetes per se that causes retinal damage, but it is unchecked DM that leads to retinopathy. Another important observation was the association of DM with Hypertension. Life-threatening cardiovascular events increase further when DM and hypertension coexist together.13
It is interesting that in our retina camps, females accounted for more presentations than males. Shrestha et al also noted similar observations in another study in Nepal. Nepal is still a male-dominant country and females have less access to health care in the hospital. They are not free from household chores and socially restricted on social mobility most of the time. To address this issue, we should promote rural eye camps to increase female participation and utilization of health facilities by them.14
The number of patients visiting SORC and DSTS differed from RRHC. This is explainable because SORC and DSTS had targeted retina patients, and they were within an hour trip from the base hospital while RRHC was more cataract surgery focused. However, patients from RRHC were in the hilly and remote region, and their lifestyles were probably protective of the tendency of diabetes and hypertension. We could have improved the number of retinal screening at RRHC by informing all diabetes and hypertension patients as in SORC and DSTS. There could have more retinal patients screening even in SORC and DSTS by appointing two retina specialists and increasing the clinic hours or clinic day. As the project had appointed a single retina specialist in outreach camps, the number of screening target set was optimal for a single retina specialist. Retinal diseases pattern showed very low patients with AMD. It could be because of low life expectancy and not genetically predisposed in Nepal. This study was neither a population-based study nor a hospital-based study. This study had also suffered from selection biases as patients with diabetes and hypertension were informed for retina check-up.
Using indirect ophthalmoscopy as a screening tool is popular because of its portability. However, seven‐field stereoscopic photographs are considered as a gold standard tool for retinal documentation. The latter has a drawback of being expensive and not portable.15 According to the British Diabetic Association, the sensitivity and specificity should be around 80,95%, respectively, to standardize the diabetic retinopathy screening protocol.16 An ophthalmoscopy was more specific but not sensitive to detect diabetic retinopathy grading; more than mild retinopathy while compared with non-mydriatic photography.17,18 However, mydriatic retinal photography was reported to have more sensitive compared with ophthalmoscopy for the detection of worse than mild retinopathy.16–19
The portable non-mydriatic fundus camera costs around United States dollar (USD) 6000, and the binocular indirect ophthalmoscope costs around USD 2000. One time investment to purchase these devices should not be an issue; considering the consequences of permanent vision loss; loss of job and immense family burden to take care of patients due to lack of this screening devices.21
There was a need of 15–16.6% screened patients referred to the hospital for retinal laser or other retinal interventions from SORC and DSTS, but only 1.96% of patients from RRHC needed a referral. Outreach programs should target for screening and conduct an awareness campaign. Outreach program should also encourage patients to visit the static eye centers for improved and further eye care from the sustainability point of view.20 In contrast to our study, referral patterns in other studies varied from 5.9% to 29%, depending on both the prevalence of sight-threatening DR 5–27.6%, and other criteria for referral.15,22-24
The limitation of our study is the limited data of four retina screening camps only. We were successful in identifying previously undiagnosed retinal patients and helping the marginalized and poor community who otherwise could not afford the retina care.
Conclusion
There are limited trained human resources, limited facilities for tackling retinal diseases in Nepal. These factors would lead to an increase in undiagnosed retinal diseases in the future. Retinal diseases are asymptomatic in the majority of subjects and can lead to irreversible visual impairment on delayed treatment. With the increasing prevalence of retinal diseases and low levels of awareness on these diseases; the consequences can be further catastrophic. So, the campaign should be on large scale retina screening programs enhancing skills of mid-level eye care workers and improved use of fundus camera.
Abbreviations
ACD, Anterior chamber depth; AMD, Age-related macular degeneration; CHEERS, Hospital for Children, Eye, ENT and Rehabilitation Services; DM, Diabetic Mellitus; DR, diabetic retinopathy; DSTS, daily screening and treatment services; FEUM, fundus evaluation on mydriasis; PSED, posterior segment eye disorder; RECON, Retina Eye Care of Nepal; SORC, static outreach clinic; RRHC, rural remote health camp, USD, United States dollar; VEGF; vascular endothelial growth factor.
Acknowledgments
The authors wish to thank Prof. Madan P Upadhyay for encouraging the innovative concept of outreach camps. We are also grateful to Mrs. Miki Upreti and Mrs. Pujan Khanal for the smooth co-ordination of the camp.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Rapid Assessment of Avoidable Blindness Survey. The epidemiology of blindness in Nepal. Nepal Netra Jyoti Sangh. 2012;1–72.
2. Bastawrous A. Posterior segment eye diseases: a growing problem. British J Ophthalmol. 2012.
3. Resnikoff S, Pascolini D, Etya’ale D, et al. Global data on visual impairment in the year 2002. Bull World Health Organization. 2004;82:844–851.
4. Eye Diseases Prevalence Research Group. Prevalence of age-related macular degeneration in the United States. Arch Ophthalmol. 2004;122:564–572. doi:10.1001/archopht.122.4.564
5. American Academy of Ophthalmology. Preferred practice pattern: diabetic retinopathy. Am Acad Ophthalmol. 1998. San Francisco, Calif.
6. The eye diseases prevalence research group. The prevalence of diabetic retinopathy among adults in the United States. Arch Ophthalmol. 2004;122:552–563. doi:10.1001/archopht.122.4.552
7. West S, Sommer A. Prevention of the blindness and priorities for the future. Bull World Health Organ. 2001;79:244–248.
8. Yorston D. Retinal diseases and vision 2020. Community Eye Health. 2003;16(46):19–20.
9. American Diabetes Association: Diabetes Overview. https://www.diabetes.org. Accessed April 20, 2020.
10. Nirmalan PK, Katz J, Robin AL, et al. Prevalence of vitreoretinal disorders in a rural population of Southern India: the aravind comprehensive eye study. Arch Ophthalmol. 2004;122:581–586. doi:10.1001/archopht.122.4.581
11. Thapa R. Retinal diseases pattern and prevention of blindness in Nepal. 2019. Acta Scientific Ophthalmol. 11–12. 2.6.
12. Paudyal G, Shrestha MK, Meyer JJ, Thapa R, Gurung R, Ruit S. Prevalence of diabetic retinopathy following a community screening for diabetes. Nepal Med Coll J. 2008;10(3):160–163.
13. Mancia G. The association of hypertension and diabetes: prevalence, cardiovascular risk, and protection by blood pressure reduction. ActaDiabetol. 2005;42(Suppl 1):S1725.
14. Shrestha MK, et al. Gender equity in eye health. Nepal J Ophthalmol. 2012;4(8):277–281. doi:10.3126/nepjoph.v4i2.6544
15. Rani PK, et al. Analysis of a comprehensive diabetic retinopathy screening model for rural and urban diabetics in developing countries. Br J Ophthalmol. 2007;91(11):1425–1429. doi:10.1136/bjo.2007.120659
16. British Diabetic Association. Retinal Photography Screening for Diabetic Eye Disease. London: BDA; 1997.
17. Pugh JA, Jacobson JM, Van Heuven WAJ, et al. Screening for diabetic retinopathy: the wide-angle retinal camera. Diab Care. 1993;16:889–895. doi:10.2337/diacare.16.6.889
18. Buxton MJ, Sculpher MJ, Ferguson BA, et al. Screening for treatable diabetic retinopathy: a comparison of different methods. Diabet Med. 1991;8:371–377. doi:10.1111/j.1464-5491.1991.tb01612.x
19. Gibbins RL, Owens DR, Allen JC, Eastman L. Practical application of the European field guide in screening for diabetic retinopathy by using ophthalmoscopy and 35mm retinal slides. Diabetologia. 1998;41:59–64. doi:10.1007/s001250050867
20. Namperumalsamy P, et al. Developing a screening program to detect sight-threatening diabetic retinopathy in South India. Diab Care. 2003;26(6):1831–1835. doi:10.2337/diacare.26.6.1831
21. Frick KD, Foster A. The magnitude and cost of global blindness: an increasing problem that can be alleviated. Am J Ophthalmol. 2003;135(4):471–476. doi:10.1016/S0002-9394(02)02110-4
22. Mash B, Powell D, Du Plessis F, van Vuuren U, Michalowska M, Levitt N. Screening for diabetic retinopathy in primary care with a mobile fundal camera evaluation of a South African pilot project. S Afr Med J. 2007;97:1284–1288.
23. Ding J, Zou Y, Liu N, et al. Strategies of digital fundus photography for screening diabetic retinopathy in a diabetic population in urban China. Ophthalmic Epidemiol. 2012;19(19):414–419. doi:10.3109/09286586.2012.716895
24. Gupta V, Bansal R, Gupta A, Bhansali A. Sensitivity and specificity of nonmydriatic digital imaging in screening diabetic retinopathy in Indian eyes. Indian J Ophthalmol. 2014;62:851–852. doi:10.4103/0301-4738.141039
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.