Back to Journals » Clinical Ophthalmology » Volume 14
A Review on Different Tonometers for Intraocular Pressure Measurement After Photorefractive Keratectomy or Small Incision Lenticule Extraction
Received 21 August 2020
Accepted for publication 22 September 2020
Published 14 October 2020 Volume 2020:14 Pages 3305—3323
DOI https://doi.org/10.2147/OPTH.S278167
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Shing Chuen Chow, Barry Yat Ming Yeung
CAP Medical Center, Hong Kong
Correspondence: Barry Yat Ming Yeung
CAP Medical Center, Rm 501-502, Hang Shing Building, 363 Nathan Road, Hong Kong
Tel +852 23329830
Fax +852 23326896
Email [email protected]
Abstract: This paper aims to review different tonometers for intraocular pressure measurement in eyes after photorefractive keratectomy or small incision lenticule extraction. An Entrez Pubmed search was performed on July 19th, 2020. There were 32 eligible articles investigated in the use of tonometers or biomechanical properties of cornea in post photorefractive keratectomy eyes and 11 articles investigated in post small incision lenticule extraction eyes. Corvis ST and dynamic contour tonometry were found to be accurate for intraocular pressure measurement in post photorefractive keratectomy eyes. For post small incision lenticule extraction eyes, Corvis ST was found to be more accurate than other tonometers. Other tonometers such as Goldmann applanation tonometer, noncontact tonometry, Tonopen, ocular response analyzer can also be used in post photorefractive keratectomy or small incision lenticule extraction eyes in clinical practice; however, it is important for ophthalmologists to take note of the chances of discrepancies.
Keywords: tonometry, tonometer, glaucoma, photorefractive keratectomy, small incision lenticule extraction
Introduction
Uncorrected refractive error is one of the major causes of visual impairment.1 It is the second leading cause of worldwide blindness, caused by a mismatch between the axial length and optical power.2 Spectacles, contact lens are most commonly used for the correction of refractive errors. Surgical treatment such as photorefractive keratectomy (PRK), laser assisted in situ keratomileusis (LASIK) and small incision lenticule extraction (SMILE) can be used for correction.3,4
Intraocular pressure (IOP) is one of the major risk factors for the development of glaucoma.5 Therefore, it is important to measure the accurate intraocular pressure for screening or treatment of glaucoma. Studies have shown that in eyes after LASIK, PRK or SMILE may be difficult to obtain an accurate intraocular pressure.6–8 With regard to the importance of measurement of accurate intraocular pressure, this review will mainly focus on the use of different tonometers in post PRK eyes or post SMILE eyes.
Methodology
An Entrez Pubmed search was performed on July 19th, 2020, using the keywords “photorefractive keratectomy”, “PRK”, “SMILE”, “Small Incision lenticule Extraction”, “tonometry”, “tonometer”. The search was limited to human studies. A total of 93 articles were found using this search strategy. These articles were then manually curated by S. C. Chow to include those concerning the use of tonometers or biomechanical properties of cornea in post PRK or post SMILE eyes. Articles on animal research, in non-English language with no English abstract, review articles were excluded. Furthermore, studies concerning the use of tonometers in eyes performed with other surgery, not performed with PRK or SMILE, were excluded. The references of the curated articles were also checked to yield further relevant articles.
Results
A total of 42 relevant articles were reviewed after manual curation. A total of 29 prospective studies and 13 retrospective studies were curated (Table 1). There were 32 articles investigated in the use of tonometers or biomechanical properties of cornea in post PRK eyes8–39 and 11 articles investigated in the use of tonometers or biomechanical properties of cornea in post SMILE eyes.38,40–49
 |  | 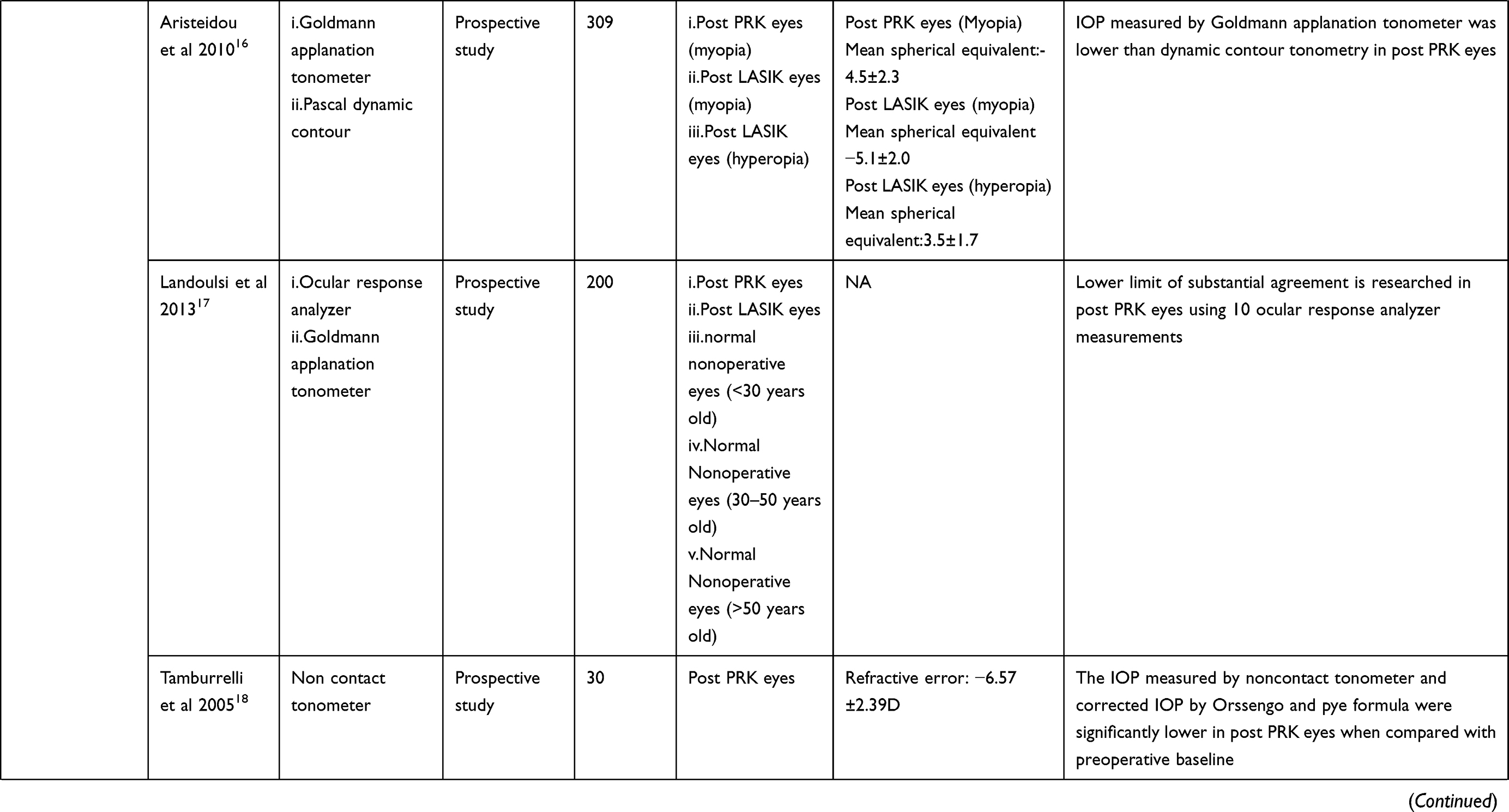 |  |  |  |  |
Table 1 Summary of Selected Relevant Studies |
Photorefractive Keratectomy
Corneal Biomechanical Properties After PRK
After PRK, the central corneal thickness (CCT) will decrease significantly when compared with pre-surgery.11,12,31,36,37,39 Study by Hamed Azzam has demonstrated a significant reduction of mean CCT by 75.5μm in post PRK eyes, when compared with the mean CCT before operation.12 Munger showed that the measured change in CCT is found to be dependent on the amount of spherical correction during PRK in hyperopic eyes, but not on the cylindrical correction.31 Six months after PRK, every diopter of applied spherical correction will result in 5.0± 0.9μm of corneal thinning. After 12 months of PRK, 4.1 ± 1 μm per diopter of spherical correction was reported. After 18 months, 2.5± 1.2 μm of CCT change per diopter was reported.31 A significant reduction in keratometry of 5.56 D was also reported (P<0.05).12 Another study by Zare demonstrated a significant reduction in corneal resistance factor and corneal hysteresis in post PRK eyes when compared with their preoperative baseline.37 The study also compared the effect of PRK with or without adjunctive mitomycin C on postoperative IOP readings and corneal biomechanical properties, which were measured by Goldmann applanation tonometry and ocular response analyzer. The result showed that the use of mitomycin C intraoperatively in PRK did not significantly affect the postoperative IOP readings and corneal biomechanics.
Goldmann Applanation Tonometer in Post PRK Eyes
Goldmann applanation tonometry is a device for measuring IOP. It is based on the Imbert Fick principle. The principle states that the pressure within a flexible elastic, thin and dry sphere equals to the force required to flatten its surface divided by the flattened area. The thickening of cornea will result in falsely high reading while its thinning will result in falsely low readings.9,13 Eyes after performing PRK may affect the corneal thickness and hence, this will result in inaccurate results for IOP measurement using Goldmann applanation tonometer.
A total of 15 studies have demonstrated a significant reduction in the measured IOP by Goldmann applanation tonometer in post PRK eyes when compared with the baseline before operation.9,12,13,15,16,20,24,29–32,35,38,39,50 Aristeidou demonstrated a fall in measured IOP value by Goldmann applanation tonometer before and after PRK. The preoperative measurement of IOP was 12.9± 2.8 mmHg, which was then reduced to 11.4 ±2.9mmHg after one month, 11.1 ±2.3 mmHg after three months, 11.1 ±2.5 mmHg after 6 months and 11.0 ±2.8 after 12 months.16 A similar result was also demonstrated by Rosa, showing a significant underestimation in post PRK eyes by Goldmann applanation 1 month, 6 months and 12 months when compared to the baseline of preoperative eyes.32
The significant reduction of IOP by Goldmann applanation tonometer in post PRK eyes was shown to be related to the CCT and corneal curvature.9,13,15,29,37,50 Garzozi found a significant correlation between the percentage change in IOP by Goldmann applanation tonometer and the percentage change in keratometry and CCT.9 In post PRK eyes, 4% reduction in CCT will not result in a change in IOP measured by Goldmann applanation tonometer. However, for eyes showing more than 4% drop in CCT, there will be a 1:1 reduction in Goldmann applanation tonometer measured IOP9. Another study by Sadigh illustrated that in every 1 μm of reduction in CCT, the measured IOP by Goldmann applanation tonometer will decrease by 0.03 mmHg by the univariate linear regression.13 In the study by Munger, there was a significant correlation between the change in CCT and change in measured IOP by Goldmann applanation tonometer (decrease of 2.1mmHg per 100 microns of corneal thinning)(P<0.05).29
Another study by Munger has demonstrated that the relationship between CCT and measured IOP by Goldmann applanation tonometer will increase at different time intervals after PRK.31 A significant relationship was found between the measured CCT and IOP measured by Goldmann applanation tonometer. The relationship increased from preoperation 1.7mmHg/100 μm to 2.11 mmHg/100 μm 6 months postoperation. This shows that CCT is a significant predictor of IOP measured by Goldmann applanation tonometer.31 However, an insignificant correlation between the changes in IOP and changes in CCT in postoperative eyes is not found at any time point. The change in measured IOP in different eyes on a given change in CCT varied greatly at any time point.31
Schipper demonstrated that the mean IOP measured at the temporal cornea by Goldmann applanation tonometer was significantly higher than the central after one and three months PRK (P<0.0001).10 No significant difference was found between the measured IOP by Goldmann tonometer over the central cornea and temporal cornea before operation, showing that PRK may affect the CCT and hence affect the accuracy of measured IOP by Goldmann applanation tonometer.
Gimeno suggested that by observation, a greater number of diopter before surgery may have a greater decrease in tonometry.33 In the cases of eyes less than −5D before surgery, 63.5% of eyes have a decrease in tonometry by Goldmann applanation tonometer after PRK. Meanwhile, as for eyes more than −5D, 78.4% of eyes have a decrease in tonometry after PRK. However, no significant difference was found when comparing the two groups (P=0.173).33
Noncontact Tonometer in Post PRK Eyes
Noncontact tonometer is based on the principle of applanation. The deformation of corneal apex is caused by a jet of air. It measures the time required to flatten the cornea for the measurement of IOP.9 Because of its convenience, sterility and safety, it is common in clinical practice, especially for screening.19 It is yet important to note that it is accurate only when the IOP is in low to middle range.9 A total of ten studies have investigated the use of noncontact tonometer in eyes that had undergone PRK.8,9,12,18–24
Four studies have demonstrated a significant reduction in the measured IOP by noncontact tonometer in postoperative PRK eyes when compared with preoperative measured baseline IOP.18–20,23 Garzozi has demonstrated a significant reduction of measured IOP by noncontact tonometer when comparing preoperative and 12 months postoperative eyes (13.51 mmHg vs 12.074 mmHg).9 Chatterjee demonstrated the change in IOP before and after operation in eyes performed with PRK and eyes were not performed with PRK, measured by non-contact tonometry. As concluded in this study, eyes performed with PRK had a greater reduction in IOP (3.5±2.7mmHg vs 0.3 ± 2.4 mmHg).23 Another study performed by Tamburrelli compared measured IOP by noncontact tonometer and corrected IOP by Orssengo and Pye formula (IOPC), which takes corneal curvature and CCT into account, in post 6-month PRK eyes during a water drink test.18 The measured IOP and IOPC were significantly lower than in postoperative eyes when compared with their preoperative baseline by multivariate analysis of variance.
The reduction of measured IOP in eyes after PRK may be due to the reduction of corneal thickness and curvature and tissue softening after healing.20 Cernak and Zhang have demonstrated a significant correlation between the reduction of IOP before and after operation and corneal thickness and curvature (P<0.05).21,22
Three studies have demonstrated different results by comparing the reduction of measured IOP in Goldmann applanation tonometer and noncontact tonometer before and after PRK operation.9,12,24 Garzozi has shown that a greater reduction in measured IOP was found in Goldmann applanation tonometer when compared to noncontact tonometer (1.504mmHg vs 1.436 mmHg).9 However, Abbasoglu et al and Hamed-Azzam suggested that there is no significant difference between the measured IOP by the two tonometers in post PRK eyes.12,24
Abbasoglu has measured IOP by Goldmann tonometry and pneumotonometry at the central and peripheral cornea in eyes in post PRK eyes at different time intervals, including 1 week, 1 months and 3 months after surgery.24 No significant difference was found between central or peripheral measured IOP.
Myopic eyes underwent PRK or LASIK were found to have a greater difference in preoperative and postoperative measurement of IOP when compared to hyperopic eyes by non-contact tonometer. Schallhorn performed a retrospective study, demonstrating that eyes performed with either LASIK or PRK had a lower IOP measured by noncontact tonometer, when compared to pre-operation.8 Myopic eyes performed with LASIK has a greater decrease in mean IOP when comparing preoperative and one month after surgery (4.57mmHg vs 2.28 mmHg). Similar trend is also demonstrated in eyes after performing PRK (preoperative 0.83mmHg vs 1-month postoperative 2.28 mmHg). The study also showed that for every 1Diopter correction of myopic correction, the postoperative measured IOP will be decreased by 0.4mmHg in eyes performed with LASIK and PRK. In hyperopic eyes performed with LASIK, for every 1 Diopter correction, the IOP measured post-operation will be lowered by 0.063mmHg at one month.8
To determine the true IOP in eyes performed PRK by noncontact tonometer, correction will be needed to prevent underestimation of the IOP. Montes-Mico suggested that a correction of adding 0.5mmHg/D of myopic correction is needed, while another study by Chatterjee suggested an equation: IOP drop (mmHg) = 1.6-(0.4 x treatment MSE diopters), in which the measured IOP drop must be added to the measured IOP by tonometer in post PRK eyes.20,23
Tonopen in Post PRK Eyes
Tonopen is a device based on the principle of Mackay-Marg tonometer. It is a handheld, portable and miniaturized electronic contact tonometer.9 It works by the use of probe tip with a transducer in contact with the cornea. A total of four studies had investigated on the measurement of IOP in eyes performed with PRK by Tonopen, showing a decrease in the measured IOP after PRK when compared with preoperative measured IOP.9–12
IOP can be measured by Tonopen at the central (Tonopen-C) or temporal peripheral (Tonopen-P) of the cornea.9 Two studies demonstrated that Tonopen C tends to have a greater difference between the measured IOP before and after PRK than Tonopen P, while one study did not demonstrate significant difference.9–11 Garzozi has shown that the reduction of measured IOP by Tonopen C is higher than TonoPen P, when comparing pre PRK with 1 month post PRK (1.295mmHg vs 0.227mmHg).9 A similar result was shown in the study by Schipper et al, showing that the postoperative mean IOP measured by Tonopen C was lower than Tonopen P (P<0.0001).10 The preoperative mean IOP has no significant difference between the two groups. However, Hamed Azzam has demonstrated an insignificant difference between Tonopen C and Tonopen P in the change of delta IOP after the operation (0.99mmHg vs 0.92mmHg, respectively).12
Two studies have investigated the correlation between measured IOP by Tonopen and corneal thickness.9,12 Hamed Azzam and Garzozi have demonstrated significant correlation between CCT and the change in IOP after operation by Tonopen.12 A less prominent correlation between change of IOP by Tonopen P and percentage change in CCT and keratometry was found when compared with Tonopen C.
All studies suggested that the difference in measured IOP before and after PRK was greater in Goldmann applanation tonometer when compared with Tonopen P and Tonopen C.9–12 The study by Levy found that the mean measured IOP by Goldmann applanation tonometer was significantly lower than Tonopen C in post PRK eyes (P=0.012).11 This suggests that the IOP measurement by Tonopen is more accurate than Goldmann tonometer in eyes after performing PRK.
Dynamic Contour Tonometry in Post PRK Eyes
Dynamic contour tonometry is a device for the measurement of IOP by a non-applanating method.13 The measurement is based on corneal contour matching and a solid state sensor. The measurement is independent from the corneal factors and can be mounted on a slip lamp for the measurement of IOP13. A total of five studies have studied the use of dynamic contour tonometry in eyes performed with PRK.13–16,38
No significant change in the measured IOP by dynamic contour tonometry was found when comparing pre-PRK eyes and 3 months post PRK eyes in the study by Chen.38
No significant correlation between the change in CCT and the change in IOP measured by dynamic contour tonometry was reported in two studies.13,15 Sadigh has shown that there was no significant correlation between CCT changes and IOP measured by dynamic contour tonometry, but a significant correlation was found between CCT changes and changes in IOP measured by Goldmann applanation tonometer, before and 6 months after operation (P=0.44 vs P<0.001).13 A similar result was also shown in Roshowska, showing that the measurement of IOP by dynamic contour tonometry is independent from CCT.
All studies had demonstrated that the measured IOP in post PRK eyes by Goldmann applanation tonometer was lower than dynamic contour tonometry 13–16,38. The result is within expectation as dynamic contour tonometry is theoretically independent from corneal factors. Study performed by Aristeidou showed that the mean IOP measured by Goldmann applanation tonometer was significantly lower than IOP measured by dynamic contour tonometry after the 1st month, 3rd month, 6th month and 12th month after PRK, showing that dynamic contour tonometry may be a better device for IOP measurement when compared with Goldmann applanation tonometer 16. Furthermore, there was a lack of agreement between Goldmann applanation tonometer and dynamic contour tonometry measured IOP in 6 months postoperative eyes, showing a mean difference of −2.4mmHg.15
Roszhowska compared the measured IOP in eyes performed with PRK by different devices, showing that no significant difference in measured IOP was found between dynamic contour tonometry and Corvis ST, but a significant difference was found between the IOP measured by Goldmann applanation tonometer and Corvis ST.15
Dynamic Scheimpflug Analyser (Corvis ST) in Post PRK Eyes
Corvis ST is a new noncontact tonometer, which uses a 455 nm wavelength light-emitting diode and 4330 frames per second Scheimpflug camera to record the dynamic reaction of cornea to a high-intensity air impulse.27 Various dynamic corneal response parameters measured by the dynamic Scheimpflug analyzer will be used to analyse the loading and unloading pattern of deformation of cornea at the highest concavity and applanation.26 New corneal biomechanical response parameters such as deformation amplitude ratio 2.0mm, integrated inverse radius, stiffness parameter at first applanation and Ambrosio relational thickness are introduced recently. The parameters will be used for calculation of biomechanically corrected IOP.26,27 A total of five studies investigating the use of Corvis ST in post PRK eyes were found14,26,27,38,39.
No significant difference is found in biomechanically corrected IOP measured by Corvis ST in post PRK eyes when compared with the baseline (P=0.101).26,38 Chen 2020 has demonstrated an insignificant change in the biomechanically corrected IOP (bIOP) when comparing preoperative and 3 months postoperative eyes (P=0.6784).38 Hassan demonstrated significant differences in pachymetry, second applanation velocity, radius in 1-month post PRK eyes when compared with preoperative baseline. However, no significant differences in found in other parameters such as IOP, first applanation time, first applanation velocity.28 The study also suggests that Corvis ST is a handy and accurate device for assessing ocular biomechanical properties and biomechanically corrected IOP after PRK.
Lee and Lanza had compared Corvis ST with other tonometers.14,26 Lanza has demonstrated that the measured IOP by Goldmann applanation tonometer is significantly lower than the corneal properties corrected IOP by Corvis ST in post PRK eyes (P<0.014).14 No significant difference is found between the IOP measured by dynamic contour tonometry and Corvis ST14. Lee has compared the biomechanically corrected IOP measured by Corvis ST and IOP measured by noncontact tonometer in post PRK eyes, showing that the corrected IOP by Corvis ST has a significantly smaller difference between pre and post PRK when compared with the measured IOP by noncontact tonometer.26
Chen studied about Corvis ST’s the intraobserver and interobserver as well as their repeatability and reproducibility of Corvis ST in post PRK eyes.27 The results suggested good intraobserver and interobserver reproducibility in the IOP, CCT and first applanation time. A good or close to good repeatability and reproducibility were reported in terms of deformation amplitude. For the second applanation time, a close to good repeatability and yet a not good reproducibility were reported.27
Tonopachymetry in Post PRK Eyes
Tonopachymetry is a combination of non-contact tonometry and pachymetry. The CCT is measured by Scheimpflug camera system while the IOP is measured by non-contact tonometry.25 The IOP is then corrected by the measured CCT automatically. Hahn demonstrated a higher repeatability in terms of CCT and IOP measured by tonopachymetry when compared with US pachymetry and Goldmann applanation tonometer 25. Significant difference is found between the corrected IOP by tonopachymetry and corrected IOP by US pachymetry and Goldmann applanation tonometer in nonsurgical and post PRK eyes. The average CCT measured by tonopachymetry was found to be significantly thicker than US pachymetry in both post PRK eyes and nonsurgical eyes (7.35µm vs 17.76µm). The overestimation in CCT was found to be greater in post PRK eyes than non-surgical eyes (P<0.001). However, a close agreement with clinically acceptable range of limits of agreement between the corrected IOP and CCT by tonopachymetry and US pachymetry was reported in the Bland Altman plot, which shows that tonopachymetry is one of the alternatives for US pachymetry and Goldmann applanation tonometer for measuring corrected IOP in post PRK eyes.25
Ocular Response Analyser in Post PRK Eyes
Ocular response analyser is a form of pneumotonometer for the measurement of IOP. It uses an electro-optical detector to measure two applanation pressure for the measurement of corneal hysteresis so as to compensate for the corneal biomechanical properties.17 A limited number of studies have investigated the use of ocular response analyzer in post PRK eyes.14,17,38
Chen has demonstrated a significant reduction in the corneal compensated IOP by ocular response analyzer in 3 months post PRK eyes when compared with pre PRK eyes. The study demonstrated an insignificant change in the IOP measured by Corvis ST and Dynamic Contour tonometry, showing that ocular response analyzer may not be as accurate as the IOP measured by the two aforementioned tonometers.38
Another study performed by Lanza showed that the measured IOP by ocular response analyzer in post PRK eyes was found to be significantly higher than Goldmann applanation tonometer (P<0.0001).14 No significant correlation between CCT measures, corneal curvature and ocular response analyzer measures were found in eyes performed with PRK.14 Further studies are required to investigate the use of ocular response analyzer in terms of accuracy for measurement of IOP in post PRK eyes.
The study performed by Landoulsi had underwent 10 ocular response analyzer measurements in the included eyes for the calculation of intraclass correlation coefficients, which is for the assessment of the agreement level.17 It showed that in post PRK patients, none of the parameters have reached 0.6, the lower limit of substantial agreement.17
Small Incision Lenticule Extraction
Corneal Biomechanical Properties After SMILE
Eight studies have demonstrated the change in corneal biomechanical properties in post SMILE eyes. However, the resulting conclusion of corneal biomechanical properties varies in different studies.40–42,45–49
Hosny, Li and Shen demonstrated a significant decrease in corneal hysteresis and corneal resistance factor in post SMILE eyes when compared with preoperative eyes.40–42 Pedersen demonstrated that CH and CRF in post SMILE eyes were significantly lower when compared with healthy eyes by ocular response analyzer.45 However, the study by Fu only showed a significant decrease in corneal resistance factor but an insignificant change in corneal hysteresis when comparing post SMILE eyes with pre-SMILE eyes.49
For CCT, Li and Shen demonstrated a significant reduction in post SMILE eyes.41,42 For flat keratometry, steep keratometry, mean keratometry, Li demonstrated a significant reduction in 1 month, 3 months and 6 months after SMILE when compared with pre-operation.41
Both Fu and Pedersen have found an insignificant difference in the first applanation time, deformation amplitude of corneal apex at highest concavity phase.45,49 Pedersen also suggested that there was an insignificant difference in the highest concavity radius, the highest concavity deflection length, the first and second applanation time between post SMILE eyes and healthy eyes.45 Fernandez and Mastropasqua demonstrated a significant change in the first and second applanation time in post SMILE eyes.46,47 Shen demonstrated an insignificant change in peak distance, applanation time at the highest concavity, the second applanation time, the first applanation length, and the second applanation length in post 1 day SMILE eyes.42
A significant increase in deformation amplitude was reported in post SMILE eyes by Shen, Pedersen, Mastropasqua and Fernandez.42,45–47 Yu demonstrated that in eyes performed with SMILE, the surrounding cornea would move slightly forward and the central posterior cornea would move slightly backward and return to normal gradually.48
Goldmann Applanation Tonometry in Post SMILE Eyes
Three studies have investigated into the measured IOP by Goldmann applanation tonometer in post SMILE eyes, all showing a significant reduction in the measured IOP by Goldmann applanation tonometry.38,40,43 Hosny has demonstrated a significant reduction in measured post SMILE IOP by Goldmann applanation tonometer when compared with preoperative IOP (P<0.001). The change in Goldmann applanation tonometer was found to be −5.30±2.67 mmHg.40 Chen demonstrated that the Goldmann applanation tonometer measured IOP has shown a significant reduction in measured IOP at 1 month, 3 months and 6 months after operation when compared with preoperative baseline IOP (P<0.001) (43). Another study by Chen has demonstrated a significant reduction in measured IOP by Goldmann applanation tonometer in eyes 3 months after SMILE when compared with the baseline IOP, a reduction of mean −2.83 mmHg was reported.38
A significant correlation between postoperative IOP by Goldmann applanation and CCT was reported in post SMILE eyes.43
Noncontact Tonometer in Post SMILE Eyes
A limited number of studies have investigated the use of noncontact tonometer in post SMILE eyes. A significant decrease in IOP measured by noncontact tonometer at 1 month, 3 months and 6 months after SMILE was demonstrated in study by Li (P<0.001).41 Similar results were also demonstrated in Fu, showing a significant reduction in measured IOP by noncontact tonometer in eyes at 1 week, 1 month and 3 months after SMILE when compared with preoperative measured IOP (P=0.006).49 By the multiple linear regression models, definite regression coefficients were reported between the change in IOP by noncontact tonometer and other influencing factors, including postoperative corneal resistant factor, corneal hysteresis, Kf and preoperative IOP.41 Another study by Shen showed a similar result of the IOP by noncontact tonometer, having a significant decrease in measured IOP after the SMILE procedure.42
When compared with bIOP by Corvis ST, IOP by noncontact tonometer showed a greater reduction in measured IOP in eyes at 1 month and 3 months after SMILE. It has a smaller reduction when compared with Goldmann corrected IOP and cornea compensated IOP by ocular response analyzer at 1 week, 1 month and 3 months after SMILE.49
Ocular Response Analyzer in Post SMILE Eyes
A significant reduction of corneal compensated intraocular pressure (IOPcc) by ocular response analyzer in post SMILE eyes was found when compared with pre-SMILE eyes.27,38,41 The ocular response analyzer used in the study by Li included parameters including corneal resistance factor, corneal hysteresis, Goldmann correlated IOP (IOPg), and corneal compensated IOP (IOPcc).41 Corneal compensated IOP is the estimated IOP by compensating corneal properties to produce a more accurate value in post-refractive surgery eyes. Both IOPg and IOPcc have a significant reduction when comparing post 1 month, 3 months, 6 months with the baseline preoperative values (P<0.001).41
No significant correlation was found between changes in IOPcc in post SMILE eyes and changes in CCT, flat keratometry, steep keratometry, mean keratometry, and corneal resistant factor by Li.41 Only significant correlation was found between the change in IOPcc in post SMILE eyes and the change in corneal hysteresis. Similar results were demonstrated in Hosny, showing the decline of post SMILE IOP and the post SMILE pachymetry, lenticule thickness or CCT.40
Fu showed that both Goldmann correlated IOP and cornea compensated IOP by ocular response analyzer had a significant decrease in post SMILE eyes at 1 week, 1 month and 3 months (49). The reduction was shown to be greater than bIOP by Corvis ST and IOP by noncontact tonometer.49 Hosny has demonstrated a significantly lower postoperative IOP than the preoperative IOP by Goldmann applanation tonometer and ocular response analyzer (IOPcc).40 The measured IOP by Goldmann applanation tonometer was significantly lower than ocular response analyzer in post SMILE eyes (P<0.001).40
Pentacam Scheimpflug Images with Noncontact Tonometer in Post SMILE Eyes
The study by Li has used the measured IOP by noncontact tonometer, with the measured corneal thickness and curvature by Pentacam to calculate the corrected IOP in post SMILE eyes, using the five different formulas.41 The five formulae include Ehlers, Shah, Dresden, Kohlhaas, Orssengo/Pye formulae. All of the IOP by the formulae showed an insignificant reduction in IOP at 1 month after SMILE, except for Ehlers. An insignificant reduction in IOP at 3 months and 6 months after SMILE was reported in Dresden, Orssengo, and Kohlhaas while a significant reduction was reported in Ehlers and Shah.
Dynamic Contour Tonometer in Post SMILE Eyes
A study performed by Chen has demonstrated a significant reduction in measured IOP by dynamic contour tonometry in post 3 months SMILE eyes when compared with pre-operation.38 Further studies are required to investigate into the use of Dynamic contour tonometer for the measurement of IOP in post SMILE eyes.
Dynamic Scheimpflug Analyzer Tonometry (Corvis ST) in Post SMILE Eyes
The IOP measured by the standard dynamic Scheimpflug analyzer was shown to have a significant reduction after SMILE when compared with preoperative baseline IOP.43–46 Shen investigated into the change in IOP measured by Corvis ST in the early phase after SMILE. A significant reduction in the measured IOP by Corvis ST at 20 minutes and 24 hours after SMILE was recorded, when comparing with preoperative baseline. The study also suggested that the main predictors of postoperative Corvis ST IOP value were postoperative first applanation time value, preoperative CCT value and postoperative PD value. No significant association was found between postoperative Corvis ST IOP and age, postoperative CCT, manifest refraction spherical equivalent, corneal curvature or other parameters.42
As for the biomechanically corrected IOP, which makes use of the new algorithm by Corvis ST, studies have shown that it was better in measuring the IOP after SMILE when compared with the IOP measured by the standard Scheimpflug analyzer.43 Chen reported an insignificant correlation between post SMILE bIOP and CCT, but a significant correlation between the postoperative IOP by conventional Scheimpflug analyzer.43 No significant reduction of bIOP in post SMILE eyes, when compared with preoperative baseline bIOP, was reported by Chen.43 However, Fernandez demonstrated that biomechanically corrected IOP showed a significant difference after SMILE. bIOP showed a smaller reduction when compared with conventional IOP measured with dynamic Scheimpflug analyser.46
Another study by Chen demonstrated that the biomechanically corrected IOP has a significant reduction of −1.46 mmHg after SMILE when compared with preoperative bIOP. When compared with Goldmann applanation and ocular response analyzer measured IOPcc, the IOP measured by dynamic contour tonometry has a smaller reduction.38 Fu also showed that bIOP has no significant difference between pre-SMILE eyes and post SMILE eyes, while IOP measured by the noncontact tonometer, ocular response analyzer showed significant reduction after SMILE.49
Discussion
IOP was found to be major risk factors for glaucoma.5,51 Studies have shown that in eyes performed photorefractive keratectomy or small incision lenticule extraction, the corneal biomechanical properties will be altered.12,31,37,40–42,45–49 The measured IOP of tonometers such as Goldmann applanation tonometry, noncontact tonometer, Tonopen were found to be correlated with the corneal biomechanical properties such as central corneal thickness and corneal curvature.9–13,21,22 This suggest that accuracy for measuring IOP in eyes performed with PRK or SMILE is of paramount importance. Therefore, this review will focus on discussing the accuracy of different tonometers in post PRK or SMILE eyes.
In post PRK eyes, previous studies have shown that a significant change in the measured IOP by Goldmann applanation tonometer, noncontact tonometer, Tonopen and ocular response analyser. Dynamic contour tonometry and Corvis ST are found to have no significant changes in eyes performed with PRK. This shows that Corvis ST and Dynamic contour tonometry have a better performance in terms of accuracy. The result is expected as the two devices corrected the measured IOP by the biomechanical properties of the cornea, which is a major cause of inaccuracy.
In post SMILE eyes, similar results are also obtained, showing that Goldmann applanation tonometer, noncontact tonometer, ocular response analyser and dynamic contour tonometer have a significant change in measured IOP after operation. The biomechanically corrected IOP by Corvis ST was found to be more accurate and have less reduction in measured IOP than the aforementioned devices.
Despite there may be inaccuracy in the measurement of IOP using tonometers other than Corvis ST and Dynamic contour tonometry, other tonometers also have their own advantages and shall be considered for the measurement of IOP in post PRK eyes or post SMILE eyes. Goldmann applanation tonometer is the gold standard in IOP measurement and is commonly used for the measurement of IOP. Ophthalmologists may have an easier access to the device. Study by Schipper has demonstrated the IOP measured by Goldmann applanation tonometer at the temporal cornea may have a better accuracy when compared to central corneal in post one and three months PRK eyes.10 Furthermore, ophthalmologists can take the results from pachymetry of the operated eye into consideration while interpreting the IOP measured by Goldmann applanation tonometer in operated eyes.
Noncontact tonometry is known for its convenience and safety, hence it is commonly used for screening. Tonopen is also commonly used due to its portable size and its inaccuracy can be improved by measuring the IOP at the temporal peripheral region of the cornea instead of the central cornea.12 A greater difference in measured IOP before and after PRK was found in Goldmann applanation tonometer when compared with Tonopen P and Tonopen C.9–12 This shows that Tonopen may have a more accurate result in measured IOP in post PRK eyes. Ocular response analyzer is also demonstrated to have a better accuracy in terms of IOP measurement when compared with Goldmann applanation tonometer in post PRK and post SMILE eyes.14
Accurately knowing the IOP value is helpful for diagnosing glaucoma and glaucoma screening as it is a major risk factor. It is important for ophthalmologists to appreciate the chances of discrepancies in the measurement of IOP in eyes performed with PRK or SMILE. Dealing with this, Corvis ST or dynamic contour tonometry might be able to provide a more accurate IOP value. Other measures such as indirect fundoscopy, visual field assessment, ocular coherence tomography should also be performed once there is a raise of suspicion of glaucoma. While for following post PRK or SMILE eyes with glaucoma over time, any IOP tool, such as Goldmann applanation tonometry or noncontact can be used, because the change of IOP during follow-up matters for monitoring glaucoma cases. By reducing the IOP by 30–50% from baseline, the progression of glaucoma would usually stop.52 Therefore, the change of IOP is more important during glaucoma follow-up. During the use of noncontact tonometer, ophthalmologists should also be aware of the chances of inaccuracy in high IOP eyes, as previous studies have shown that noncontact tonometer was found to be less reliable between 20 and 30 mmHg.53
Conclusion
The biomechanically corrected IOP measured by Corvis ST and IOP measured by Dynamic contour tonometry were found to be accurate in post PRK eyes. For eyes performed with SMILE, Corvis ST was found to be more accurate for measuring IOP than other tonometers. Other tonometers such as Goldmann applanation tonometer, noncontact tonometry, Tonopen, ocular response analyzer can also be used for measuring IOP in eyes performed photorefractive keratectomy or small incision lenticule extraction in clinical practice; however, it is important for ophthalmologists to take note of the chances of discrepancies.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Casas Luque L, Naidoo K, Chan VF, et al. Prevalence of refractive error, presbyopia, and spectacle coverage in Bogotá, Colombia: a rapid assessment of refractive error. Optom Vis Sci. 2019;96(8):579–586. doi:10.1097/OPX.0000000000001409
2. Harb EN, Wildsoet CF. Origins of refractive errors: environmental and genetic factors. Annu Rev Vis Sci. 2019;5:47–72. 1 doi:10.1146/annurev-vision-091718-015027
3. Spadea L, Giovannetti F. Main complications of photorefractive keratectomy and their management. Clin Ophthalmol. 2019;13:2305–2315. doi:10.2147/OPTH.S233125
4. Wong AHY, Cheung RKY, Kua WN, Shih KC, Chan TCY, Wan KH. Dry eyes after SMILE. Asia Pac J Ophthalmol (Phila). 2019;8(5):397–405. doi:10.1097/01.APO.0000580136.80338.d0
5. Sihota R, Angmo D, Ramaswamy D, Dada T. Simplifying “target” intraocular pressure for different stages of primary open-angle glaucoma and primary angle-closure glaucoma. Indian J Ophthalmol. 2018;66(4):495–505. doi:10.4103/ijo.IJO_1130_17
6. Wang KJ, Wang WW, Tsai CL, Wang IJ. Intraocular pressure changes in eyes with small incision lenticules and laser in situ keratomileusis. Clin Exp Optom. 2019;102(4):399–405. doi:10.1111/cxo.12861
7. Tsai AS, Loon SC. Intraocular pressure assessment after laser in situ keratomileusis: a review. Clin Exp Ophthalmol. 2012;40(3):295–304. doi:10.1111/j.1442-9071.2011.02641.x
8. Schallhorn JM, Schallhorn SC, Ou Y. Factors that influence intraocular pressure changes after myopic and hyperopic LASIK and photorefractive keratectomy: a large population study. Ophthalmology. 2015;122(3):471–479. doi:10.1016/j.ophtha.2014.09.033
9. Garzozi HJ, Chung HS, Lang Y, Kagemann L, Harris A. Intraocular pressure and photorefractive keratectomy: a comparison of three different tonometers. Cornea. 2001;20(1):33–36. doi:10.1097/00003226-200101000-00006
10. Schipper I, Senn P, Oyo-Szerenyi K, Peter R. Central and peripheral pressure measurements with the Goldmann tonometer and tono-pen after photorefractive keratectomy for myopia. J Cataract Refract Surg. 2000;26(6):929–933. doi:10.1016/S0886-3350(99)00461-7
11. Levy Y, Zadok D, Glovinsky Y, Krakowski D, Nemet P. Tono-pen versus Goldmann tonometry after excimer laser photorefractive keratectomy. J Cataract Refract Surg. 1999;25(4):486–491. doi:10.1016/S0886-3350(99)80044-3
12. Hamed-Azzam S, Briscoe D, Tomkins O, Shehedeh-Mashor R, Garzozi H. Evaluation of intraocular pressure according to corneal thickness before and after excimer laser corneal ablation for myopia. Int Ophthalmol. 2013;33(4):349–354. doi:10.1007/s10792-012-9701-7
13. Sadigh AL, Fouladi RF, Hashemi H, Beheshtnejad AH. A comparison between Goldmann applanation tonometry and dynamic contour tonometry after photorefractive keratectomy. Graefes Arch Clin Exp Ophthalmol. 2013;251(2):603–608. doi:10.1007/s00417-012-2142-1
14. Lanza M, Iaccarino S, Mele L, et al. Intraocular pressure evaluation in healthy eyes and diseased ones using contact and non contact devices. Cont Lens Anterior Eye. 2016;39(2):154–159. doi:10.1016/j.clae.2015.10.001
15. Roszkowska AM, De Grazia L, Cirone M, Ferreri G. Comparison of Goldmann applanation tonometry and dynamic contour tonometry in the measurement of intraocular pressure in eyes with different corneal thicknesses. Ophthalmologica. 2009;223(4):244–249. doi:10.1159/000209253
16. Aristeidou AP, Labiris G, Katsanos A, Fanariotis M, Foudoulakis NC, Kozobolis VP. Comparison between Pascal dynamic contour tonometer and Goldmann applanation tonometer after different types of refractive surgery. Graefes Arch Clin Exp Ophthalmol. 2011;249(5):767–773. doi:10.1007/s00417-010-1431-9
17. Landoulsi H, Saad A, Haddad NN, Guilbert E, Gatinel D. Repeatability of ocular response analyzer waveform parameters in normal eyes and eyes after refractive surgery. J Refract Surg. 2013;29(10):709–714. doi:10.3928/1081597X-20130919-04
18. Tamburrelli C, Giudiceandrea A, Vaiano AS, Caputo CG, Gullà F, Salgarello T. Underestimate of tonometric readings after photorefractive keratectomy increases at higher intraocular pressure levels. Invest Ophthalmol Vis Sci. 2005;46(9):3208–3213. doi:10.1167/iovs.04-1240
19. Cennamo G, Rosa N, La Rana A, Bianco S, Sebastiani A. Non-contact tonometry in patients that underwent photorefractive keratectomy. Ophthalmologica. 1997;211(6):341–343. doi:10.1159/000310825
20. Montés-Micó R, Charman WN. Intraocular pressure after excimer laser myopic refractive surgery. Ophthalmic Physiol Opt. 2001;21(3):228–235. doi:10.1046/j.1475-1313.2001.00581.x
21. Zhang X, Pan C, Li L, Ding J. Correlations between factors and intraocular pressure following photorefractive keratectomy. Zhonghua Yan Ke Za Zhi. 1998;34(5):385–387.
22. Cernák A, Sisková E, Durcová T, Cernák M. Is it possible to accurately measure intraocular pressure after refractive surgery?. Cesk Slov Oftalmol. 2003;59(6):397–401.
23. Chatterjee A, Shah S, Bessant DA, Naroo SA, Doyle SJ. Reduction in intraocular pressure after excimer laser photorefractive keratectomy. Correlation with pretreatment myopia. Ophthalmology. 1997;104(3):355–359. doi:10.1016/S0161-6420(97)30308-X
24. Abbasoglu OE, Bowman RW, Cavanagh HD, McCulley JP. Reliability of intraocular pressure measurements after myopic excimer photorefractive keratectomy. Ophthalmology. 1998;105(12):2193–2196.
25. Hahn IK, Kim JY, Kim MJ, Tchah H, Moon CH. Validity of tono-pachymetry for measuring corrected intraocular pressure in non-surgical and post-photorefractive keratectomy eyes. Korean J Ophthalmol. 2017;31(1):44–51. doi:10.3341/kjo.2017.31.1.44
26. Lee H, Roberts CJ, Kim TI, Ambrósio R
27. Chen X, Stojanovic A, Hua Y, et al. Reliability of corneal dynamic scheimpflug analyser measurements in virgin and post-PRK eyes. PLoS One. 2014;9(10):e109577. doi:10.1371/journal.pone.0109577
28. Hassan Z, Modis L
29. Munger R, Hodge WG, Mintsioulis G, Agapitos PJ, Jackson WB, Damji KF. Correction of intraocular pressure for changes in central corneal thickness following photorefractive keratectomy. Can J Ophthalmol. 1998;33(3):159–165.
30. Mardelli PG, Piebenga LW, Whitacre MM, Siegmund KD. The effect of excimer laser photorefractive keratectomy on intraocular pressure measurements using the Goldmann applanation tonometer. Ophthalmology. 1997;104(6):945–948. doi:10.1016/S0161-6420(97)30202-4
31. Munger R, Dohadwala AA, Hodge WG, Jackson WB, Mintsioulis G, Damji KF. Changes in measured intraocular pressure after hyperopic photorefractive keratectomy. J Cataract Refract Surg. 2001;27(8):1254–1262. doi:10.1016/S0886-3350(01)00971-3
32. Rosa N, Cennamo G, Breve MA, La Rana A. Goldmann applanation tonometry after myopic photorefractive keratectomy. Acta Ophthalmol Scand. 1998;76(5):550–554. doi:10.1034/j.1600-0420.1998.760508.x
33. Gimeno JA, Muñoz LA, Valenzuela LA, Moltó FJ, Rahhal MS. Influence of refraction on tonometric readings after photorefractive keratectomy and laser assisted in situ keratomileusis. Cornea. 2000;19(4):512–516. doi:10.1097/00003226-200007000-00022
34. Wu F, Jin X, Xu Y, Yang Y. Treatment of corneal perforation with lenticules from small incision lenticule extraction surgery: a preliminary study of 6 patients. Cornea. 2015;34(6):658–663. doi:10.1097/ICO.0000000000000397
35. Faucher A, Grégoire J, Blondeau P. Accuracy of Goldmann tonometry after refractive surgery. J Cataract Refract Surg. 1997;23(6):832–838. doi:10.1016/S0886-3350(97)80239-8
36. Tamburrelli C, Vaiano AS, Salgarello T, Caputo CG, Scullica L. Tonometric changes of latanoprost-induced intraocular pressure reduction after photorefractive keratectomy. Invest Ophthalmol Vis Sci. 2004;45(3):846–850. doi:10.1167/iovs.03-0625
37. Zare M, Feizi S, Azimzadeh A, Esfandiari H. Effect of photorefractive keratectomy with mitomycin-C on corneal biomechanical features. Curr Eye Res. 2012;37(6):457–462. doi:10.3109/02713683.2012.660594
38. Chen S, Lopes BT, Huang W, et al. Effectiveness of four tonometers in measuring intraocular pressure following femtosecond laser-assisted LASIK, SMILE and transepithelial PRK. J Cataract Refract Surg. 2020. doi:10.1097/j.jcrs.0000000000000204
39. Svedberg H, Chen E, Hamberg-Nyström H. Changes in corneal thickness and curvature after different excimer laser photorefractive procedures and their impact on intraocular pressure measurements. Graefes Arch Clin Exp Ophthalmol. 2005;243(12):1218–1220. doi:10.1007/s00417-005-0072-x
40. Hosny M, Aboalazayem F, El Shiwy H, Salem M. Comparison of different intraocular pressure measurement techniques in normal eyes and post small incision lenticule extraction. Clin Ophthalmol. 2017;11:1309–1314. doi:10.2147/OPTH.S132578
41. Li H, Wang Y, Dou R, et al. Intraocular pressure changes and relationship with corneal biomechanics after SMILE and FS-LASIK. Invest Ophthalmol Vis Sci. 2016;57(10):4180–4186. doi:10.1167/iovs.16-19615
42. Shen Y, Su X, Liu X, Miao H, Fang X, Zhou X. Changes in intraocular pressure values measured with noncontact tonometer (NCT), ocular response analyzer (ORA) and Corvis Scheimpflug technology tonometer (CST) in the early phase after small incision lenticule extraction (SMILE). BMC Ophthalmol. 2016;16(1):205. doi:10.1186/s12886-016-0381-3
43. Chen KJ, Joda A, Vinciguerra R, et al. Clinical evaluation of a new correction algorithm for dynamic Scheimpflug analyzer tonometry before and after laser in situ keratomileusis and small-incision lenticule extraction. J Cataract Refract Surg. 2018;44(5):581–588. doi:10.1016/j.jcrs.2018.01.023
44. Sefat SM, Wiltfang R, Bechmann M, Mayer WJ, Kampik A, Kook D. Evaluation of changes in human corneas after femtosecond laser-assisted LASIK and small-incision lenticule extraction (SMILE) using non-contact tonometry and ultra-high-speed camera (Corvis ST). Curr Eye Res. 2016;41(7):917–922. doi:10.3109/02713683.2015.1082185
45. Pedersen IB, Bak-Nielsen S, Vestergaard AH, Ivarsen A, Hjortdal J. Corneal biomechanical properties after LASIK, ReLEx flex, and ReLEx smile by Scheimpflug-based dynamic tonometry. Graefes Arch Clin Exp Ophthalmol. 2014;252(8):1329–1335. doi:10.1007/s00417-014-2667-6
46. Fernández J, Rodríguez-Vallejo M, Martínez J, Tauste A, Piñero DP. Corneal thickness after SMILE affects scheimpflug-based dynamic tonometry. J Refract Surg. 2016;32(12):821–828. doi:10.3928/1081597X-20160816-02
47. Mastropasqua L, Calienno R, Lanzini M, et al. Evaluation of corneal biomechanical properties modification after small incision lenticule extraction using Scheimpflug-based noncontact tonometer. Biomed Res Int. 2014;2014:290619. doi:10.1155/2014/290619
48. Yu CJ, Wang Y, Su XL, Wu WJ, Wu ZQ, Wu YN An analysis of changes in posterior corneal elevation and relevant factors after small incision lenticule extraction. Zhonghua Yan Ke Za Zhi. 2016;52(7):494–498.
49. Fu D, Li M, Knorz MC, Wei S, Shang J, Zhou X. Intraocular pressure changes and corneal biomechanics after hyperopic small-incision lenticule extraction. BMC Ophthalmol. 2020;20(1):129. doi:10.1186/s12886-020-01384-2
50. Wu X, Liu S, Huang P, Wang P. Analysis of intraocular pressure after myopic photorefractive keratectomy. Zhonghua Yan Ke Za Zhi. 2002;38(10):603–605.
51. Jonas JB, Weber P, Nagaoka N, Ohno-Matsui K. Glaucoma in high myopia and parapapillary delta zone. PLoS One. 2017;12(4):e0175120. doi:10.1371/journal.pone.0175120
52. Jonas JB, Aung T, Bourne RR, Bron AM, Ritch R, Panda-Jonas S. Glaucoma. Lancet.2017;390(10108):2183–2193. doi:10.1016/S0140-6736(17)31469-1
53. Lagerlöf O. Airpuff tonometry versus applanation tonometry. Acta Ophthalmol (Copenh) 1990;68(2):221–224. doi:10.1111/j.1755-3768.1990.tb01909.x
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.