Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 7
A randomized, double-blind, placebo-controlled clinical trial evaluating Dermytol® cream for the treatment of actinic keratoses
Authors Evans M, Kalman D, Alvarez P, Paquet M, Guthrie N
Received 24 May 2014
Accepted for publication 3 July 2014
Published 7 August 2014 Volume 2014:7 Pages 215—224
DOI https://doi.org/10.2147/CCID.S63067
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Malkanthi Evans,1 Douglas Kalman,2 Patricia Alvarez,3 Maryse Paquet,4 Najla Guthrie1
1KGK Synergize Inc., London, ON, Canada; 2Miami Research Associates, South Miami, FL, USA; 3Latin American Research, Santo Domingo, Dominican Republic; 4Department of Medicine, Western University, London, ON, Canada
Purpose: Actinic keratosis lesions (AKs) have the potential to develop into squamous cell carcinoma (SCC) and thus therapies to prevent SCC development from AKs are warranted. The aim of this study was to assess the effects of a 3 month application of a canola phenolic acid-based cream (CPA) on AK lesions.
Patients and methods: This was a randomized, double-blind, placebo-controlled, 12 week clinical study conducted at a single-center in Santo Domingo, Dominican Republic. Forty-five subjects (30 CPA and 15 placebo), aged 45–85 years with 3–10 AKs within a 20 cm2 treatment area (scalp, forehead, dorsal forearm, neck, or back of hand) were enrolled. The primary outcome was complete or partial lesion clearance and the secondary outcome was safety of CPA.
Results: Although complete AK lesion clearance was not seen in this study, a significant reduction in the mean change from baseline in the average lesion area was observed at weeks 3 (P=0.002), 6 (P<0.001), and 12 (P<0.001) in the CPA group, but only at weeks 6 and 12 in the placebo group (P=0.005 and P=0.002, respectively). Furthermore, the proportion of participants with a ≥10% decrease in average lesion area was significantly higher in the CPA group than the placebo group at weeks 3 (P=0.05) and 6 (P=0.02), and showed a trend at week 12 (P=0.06). A subset analysis of the change in average lesion area based upon the total lesion area at baseline revealed that CPA elicited a greater reduction than placebo (2×) in participants with a baseline total AK lesion area of 100–500 mm2 than in participants with a total area <100 mm2 (1.3×).
Conclusion: The results of this study and previous in vitro studies suggest a potential role for CPA in the treatment of AK lesions and the prevention of SCC development.
Keywords: actinic keratosis, precancerous lesion, canola phenolic acid-rich extract, squamous cell carcinoma, Dermytol®
Introduction
Actinic keratoses (AKs), also referred to as solar keratoses, are lesions of keratinocytic dysplasias that arise from ultraviolet (UV)-induced changes to the skin. Chronically sun-exposed areas such as the face, ears, neck, forearms, and dorsal hands are most commonly affected.1 AKs are inflamed lesions characterized by erythema associated with scaling.2 In the US, 55% of adults aged 65 to 75 years have AKs, making them one of the most commonly treated dermatological conditions.3,4 Advanced age, fair skin, and living at lower latitudes are independent risk factors that increase the prevalence of AKs.5
AKs are precancerous epidermal lesions and patients presenting with AKs have been found to be 6× more likely to develop melanoma and non-melanoma skin cancer.6 The progression of AKs to invasive squamous cell carcinoma (SCC) has been reported to be quite variable and occurs at a rate of 0.096% to 16% per lesion each year; however, AKs tend to present as multiple lesions and a given patient has an average of 6 to 8 lesions.4,7,8 The 10 year risk factor for AKs to progress to SCC is an estimated 6.1% to 10.2% for an individual with an average of 7.7 lesions.4 While the risk of progression is low, 60% to 97% of SCCs are considered to have developed from AKs,9 and with a 1% mortality rate, development of effective therapies that resolve AKs or cease their transformation into SCC is warranted.10
Current treatment options for AKs consist of lesion- or field-directed therapies. Lesion-directed therapies include cryosurgery, photodynamic therapies and curettage with electrodessication.5 Cryosurgery is the most commonly used treatment for AKs, however this treatment may be contraindicated if the diagnosis is uncertain. A decreased treatment response is expected for thicker lesions or lesions located on the dorsal hand.11 Photodynamic therapies administered in combination with photosensitizers such as methyl-aminolevulinic acid are superior to placebo.12,13 Effective treatment of larger lesions may involve surgery to shave or curette the AK lesions. Lesion-directed therapies are most appropriate for the relief of bleeding and aesthetic improvement.14
Field-directed therapies are most appropriate for cancer prevention as they are used on areas with significant sun damage that are potential sites for the development of AKs.14 The application of 5-fluorouracil or diclofenac cream is a less invasive form of treatment, however, inflammatory changes, such as erythema, necrosis, blistering, and erosion are common and are not well-tolerated.15 A recent meta-analysis of eight interventions for AKs determined that for complete clearance of lesions, 5-fluorouracil was the most effective treatment, with other field-directed therapies, such as imiquimod and ingenol mebutate, along with lesion-directed photodynamic therapy being somewhat effective,14 and topical retinoids and dermabrasion being of limited effectiveness.16,17 While surgery is the most commonly used treatment strategy, it is not the most effective. Surgery is highly invasive, causes pain, and may result in scarring. The increased risk of adverse events (AEs) associated with pharmaceutical and phototherapies necessitates the development of a highly effective, non-invasive therapy for the treatment of AKs.
Canola phenolic acid-based cream (CPA) is rich in sinapic acid (>50%) and possesses anti-proliferative activity. The anti-proliferative properties of CPA are more potent and longer lasting when compared to pure sinapic acid in vitro, using B16-F1 cells (unpublished data). CPA has demonstrated anti-proliferative activity both in vitro and in vivo as it has been shown to significantly decrease tumor multiplicity and total tumor weight in an inducible non-melanoma skin cancer mouse model and reduce melanoma tumor cell growth in male mice.18,19 Orally-treated mice subcutaneously injected with B16-F1 malignant melanoma tumor cells, demonstrated an average 44.5% decrease of tumor volume while tumor volume was decreased by 61.2% in topically-treated mice.19 CPA also reduced the occurrence of colonic polyps in a rat model of colon carcinogenesis.20 Therefore, the purpose of this study was to assess the efficacy and safety of a 3 month administration of 7.8% CPA on the complete or partial clearance of AK lesions.
Materials and methods
Study design
This was a single-center, randomized, double-blind, placebo-controlled, 12 week clinical trial conducted by Miami Research Associates (MRA; South Miami, FL, USA) in collaboration with Latin American Research at an MRA site in the Dominican Republic (Santo Domingo, Dominican Republic). Ethical approval for this study was obtained from the Institutional Review Board (Consejo Nacional de Bioética en Salud, CONABIOS, Santo Domingo) on December 12, 2007. The study was conducted in accordance with the Declaration of Helsinki and its subsequent amendments. Informed consent was obtained from each subject at the screening visit prior to any study-related activities. The first screening visit of the first subject was performed on June 18, 2008 and the last visit of the last participant took place on January 6, 2009.
Participants
Male and female subjects between 45 and 85 years of age with 3 to 10 AK lesions in a treatment area (scalp, forehead, dorsal forearm, neck, back of the hand) not exceeding 20 cm2 in total area were eligible for this study. Subjects were excluded if they were pregnant, breastfeeding, or planning on becoming pregnant during the course of the trial, had a history of alcohol or drug abuse within the past year, were living with someone being treated with imiquimod, had known allergies or sensitivities to components of the vehicle cream, or had cardiovascular, hematological, hepatic, renal, endocrine, vascular or gastrointestinal abnormalities or diseases, or any other conditions which may have adversely affected their ability to complete the study. Prior to randomization, a washout period of 4 weeks was required for interferon inducers, immunomodulators, immunosuppressants, cytotoxic drugs, or investigational drugs and a washout period of 2 weeks was required for topical therapies. The use of other natural health products or vitamin D supplements required a washout of 3 weeks prior to baseline. Subjects diagnosed with a bacterial or viral infection less than 2 weeks prior to randomization were also excluded.
Randomization and blinding
Study participants were randomized to receive the active product CPA or placebo in a 2:1 proportion using a block-3 randomization scheme. The study product was packaged in the form of single-application squeeze sachets containing either CPA or placebo. A four-digit randomization code was applied to each sachet and a randomization schedule was prepared showing the correspondence between the product and randomization code. Study participants, clinical staff, and assessors were all blinded to treatment allocation.
Investigational product
The investigational product, Dermytol® (KGK Synergize Inc., London, ON, Canada) (CPA) is a phytonutrient extract rich in phenolic acids isolated from defatted canola meal (a residual fraction obtained during the processing of canola oil; Grain Processing Corp., Muscatine, IA, USA). The final product, a brown powder rich in sinapic acid (>50%) is the principal active ingredient in Dermytol® (CBI Laboratories, Inc., Fort Worth, Texas, USA). The powder was mixed into a hydrophilic cream base producing a 7.8% cream for dermatological use. CPA contains 30% maltodextrin which acts as an inert excipient during the manufacturing process. The placebo cream was made using the same formulation but without the active ingredient.
Study protocol
At screening, informed consent was obtained and the medical history, height, weight, and vital signs of the subjects were recorded. Blood samples were taken for routine laboratory tests. The study dermatologists performed a lesion evaluation and selected three to ten visible AK lesions within an area less than 20 cm2 to be measured throughout the study. At the randomization visit (baseline), concomitant therapies were reviewed, a physical examination was performed and weight and vital signs were recorded. Lesions were evaluated and were also photographed. Study lesions were classified as mild, moderate or severe at baseline by the investigational dermatologist. Lesion severity was monitored and documented at week 3, 6, 12, and 36. A 6 week supply of CPA or placebo was dispensed along with application instructions and AE recording forms to monitor product use. Participants were instructed to apply the content of one sachet of cream on the preselected skin area twice a day, after showering in the morning and again in the evening for 12 weeks. At the week 3, 6, and 12 visits, AK lesions were evaluated and classified, photographed, AE forms collected, the incidence and severity of erythema, edema, induration, vesicles, erosion, ulceration, excoriation, and scabbing were graded, and systemic reactions were assessed. Participants who experienced any severe adverse reactions were allowed rest periods of up to 2 weeks in which the frequency of application was reduced to once per day. Participants who discontinued treatment were not replaced. Blood samples were taken for routine laboratory safety tests at the week 12 visit. At the follow-up end of treatment visit (6 months post-treatment), the lesion areas in the CPA group were again photographed and assessed.
Sample size estimation
The minimum number of participants needed for statistical significance was based on previously published studies.21–23 With projected clearance rates of 70% for treatment and 8% for placebo, approximately 24 treatment and 12 placebo participants were needed to provide 95% power to detect a significant difference in complete clearance rates. Based on an expected 20% dropout rate, approximately 45 subjects were required to initiate the study if 36 were expected to complete the study.
Outcomes
The primary objective of this study was to evaluate whether CPA promoted complete or partial clearance of AK lesions. Complete clearance was defined as an area of inflamed skin that no longer had signs of inflammation and appeared similar to the surrounding skin. Partial clearance was defined as a reduction in the quantity (defined as mild, moderate or severe and a measurement was provided for the lesion description) and quality (induration, erythematic, scaling, telangiectasia and hemorrhagic zones) of inflammation characteristics. An investigating dermatologist calculated the area of individual lesions by multiplying the maximum length by the width and provided an assessment of AK lesion improvement; “complete resolution”, “partial resolution”, “no change”, or “worsening”. Two categorical measures of improvement, mean change and percentage change in lesion size at various visits were tabulated and the two groups compared.
As no participants achieved complete lesion clearance, an overall numerical measure of improvement was developed by assigning values of +2, +1, 0, and −1 to the investigator’s assessment of lesion improvement, as being “completely resolved”, “partially resolved”, “unchanged”, or “worse”, respectively. These values were averaged and compared between products in the same way as other numerical endpoints. In addition, two categorical measures of improvement, average change, and percentage change in lesion size (>10% decrease, >25% decrease, and >50% decrease) at various visits, were tabulated and the two groups compared.
The total lesion area was dependent on the number and area of the individual lesions and as there was a large variation in the number and area of lesions at baseline (total lesion area ranged from 13 mm2 to 840 mm2), average lesion area produced a more accurate assessment of response to treatment and was calculated by multiplying the maximum length by the width of individual lesions. The following exploratory analyses were also performed: 1) a subset analysis of reduction in average lesion area based on baseline total lesion area (<100 mm2, 101–250 mm2, and 251–500 mm2); 2) prevalence of scabbing; and 3) the effect of lesion age on response to treatment.
Statistical analyses
The analytical population consisted of all participants who completed the 12 week treatment period within each study arm, with no protocol violations that in the judgment of the principal investigator would have rendered their efficacy data unreliable, and who were suitably compliant (80% to 120% overall) with the dosing regimen. The mean changes in lesion clearance from baseline and between CPA- and placebo-treated groups were tested for significance with a paired Student’s t-test or the non-parametric Wilcoxon signed-rank test as appropriate. Data were log-transformed prior to statistical analysis to improve normality of the lesion measurement data.
The safety population, consisted of all participants who received at least one application of study product and who had any subsequent safety evaluations. Mean changes in safety variables from baseline were tested for significance by the paired Student’s t-test or by the non-parametric Wilcoxon signed-rank test as appropriate. Between-product differences in mean changes from baseline were tested for significance by the unpaired Student’s t-test or by the non-parametric Mann–Whitney U test as appropriate. AEs were listed, MedDRA-coded, and grouped by system organ class (cardiac, gastrointestinal, neurologic, etc). The proportion of participants experiencing one or more AEs in each MedDRA system organ class was compared between products by Fisher’s exact test.
Results
Participant disposition
Forty-five eligible subjects (four male and 41 female) were randomized and 42 completed the study (Figure 1). Three of the 45 participants did not complete the entire treatment period because of loss to follow-up (N=1) or AEs (N=2) (Figure 1). All enrolled participants were white Hispanic except for one participant of Asian ethnicity. Participants ranged from 45 to 82 years of age and the mean age of those on CPA was 60.0±10.8 years and those on placebo 55.7±9.1 years (Table 1). All study participants had mild AK lesions and two participants in the CPA group had two moderate lesions along with mild lesions. There was no difference in body mass index, average AK lesion area or total lesion area between the treatment groups at baseline (Table 1).
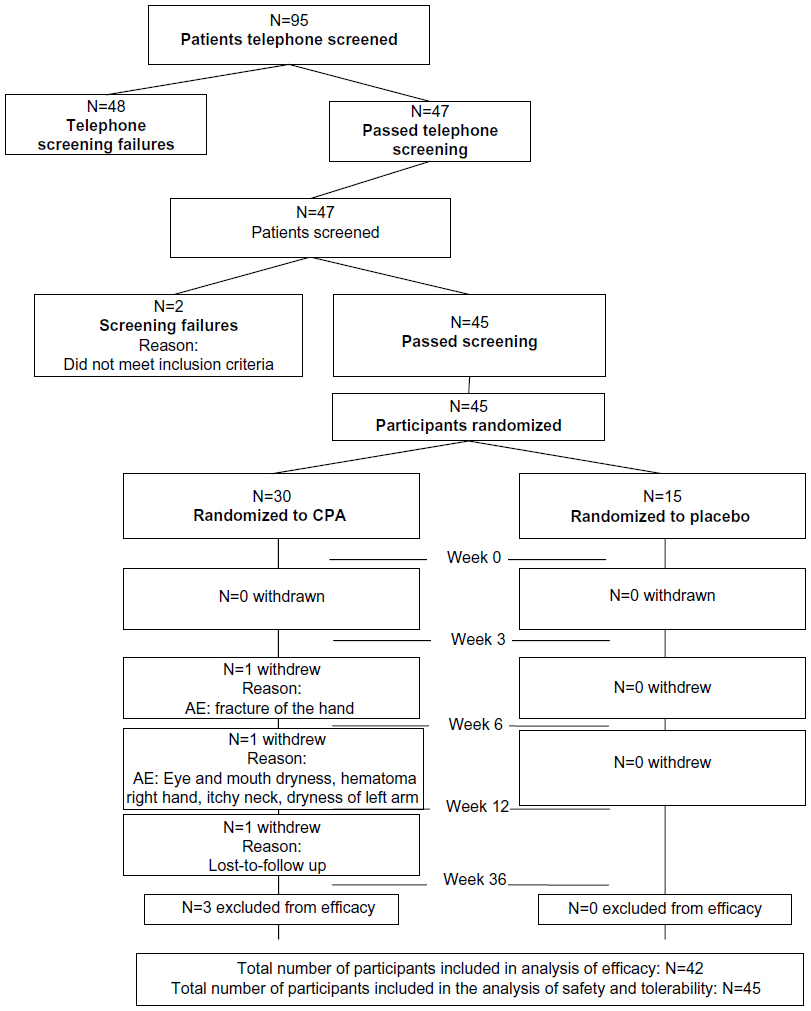 | Figure 1 Illustration of the disposition of all participants screened and enrolled into the study. |
 | Table 1 Baseline demographics of study participants |
Efficacy of CPA
Although none of the study participants achieved complete clearance, decreases in average lesion area were seen with both CPA and placebo treatment (Figure 2). The CPA group showed almost twice the decrease in lesion size as the placebo group (Figure 3). The reduction was significant for both CPA and placebo groups at 6 (P<0.001 and P=0.005, respectively) and 12 weeks (P<0.001 and P=0.002, respectively), but only significant in the CPA group at 3 weeks (P=0.002). The difference in the week 6 change between the CPA and placebo groups approached statistical significance (P=0.09). There was a decrease in average lesion area from week 12 to week 36 (post-treatment) in the CPA group (week 36 assessment was not performed in the placebo group), indicating that the improvement in the CPA group persisted beyond the treatment period (Figures 2 and 3). In the two participants with moderate lesions in the CPA group, lesions decreased to mild in severity at week 6, week 12, and follow-up at week 36.
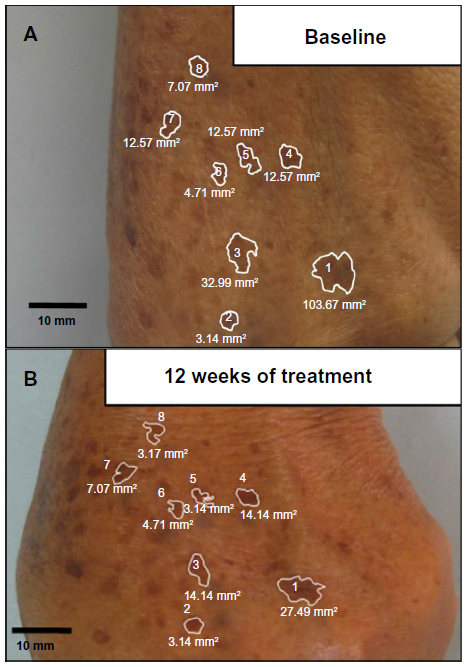 | Figure 2 Forearm AK lesions. |
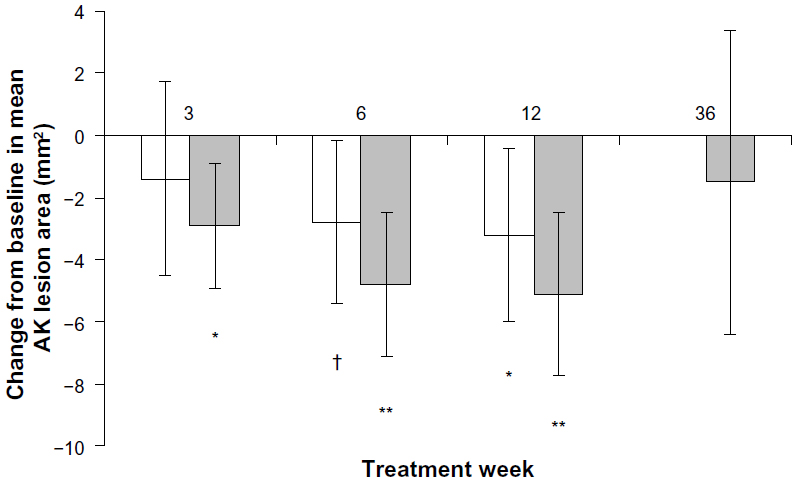 | Figure 3 The mean change in lesion size from baseline at 3, 6 and 12 weeks of treatment and after follow-up at 36 weeks. |
A greater proportion of participants in the CPA group than the placebo group showed a >10% decrease in average lesion size at week 3 (P=0.05) and week 6 (P=0.02) and showed a trend toward significance at week 12 (P=0.06) (Figure 4). No difference was seen between the groups in the proportion of participants with >25% reduction in the average lesion size, but >50% reductions were observed only in the CPA group (Figure 4).
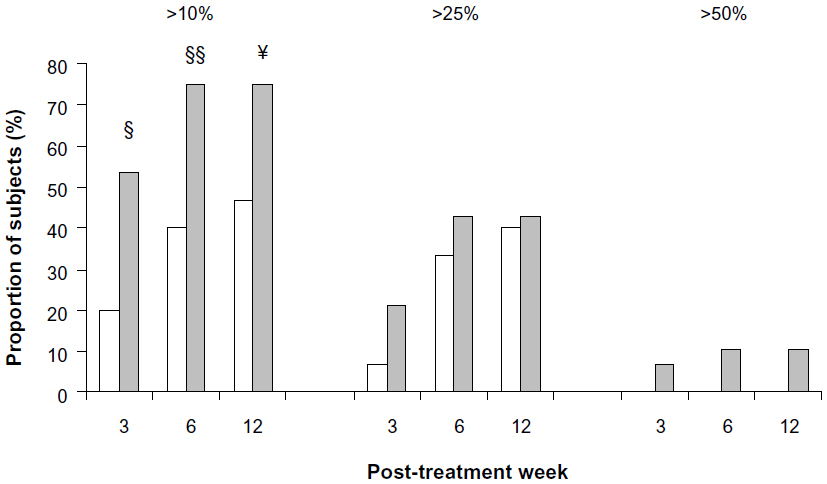 | Figure 4 Proportion of subjects exhibiting >10%, >25% and >50% reductions in average lesion size. |
Subset analyses based upon the baseline total lesion area (<100 mm2, 100–249 mm2 and 250–499 mm2) showed differences in treatment response within certain total lesion size groups. Participants in the CPA group with a total lesion area <100 mm2 demonstrated a 1.3× greater mean reduction in average lesion size than placebo (data not shown). Similarly, greater responses were observed for participants in the CPA group compared to placebo for total lesion areas 101–250 mm2 (1.9× reduction) and 251–500 mm2 (2.0× reduction). The CPA group showed a trend toward higher prevalence of lesion scabbing, a sign of healing, after 12 weeks of treatment (6.8%) than those treated with placebo (1.3%, P=0.09). An analysis of lesion age on responsiveness to treatment suggests that CPA and placebo had comparable reductions in the average lesion area. Although these differences were not statistically significant, the number of years since lesion onset was found to influence the extent of lesion resolution. Average lesion area was examined for participants with lesion onset of ≤5 years, 5–10 years, ≤10 years, and >10 years. Greater reductions in lesion size were seen in the CPA group than the placebo group for all subsets and was found to be more pronounced in participants with lesion onset ≤10 years compared to those with onset >10 years (data not shown).
Safety analysis
One serious adverse event, a parasitic amoeba infection was reported during this study in a participant receiving placebo. A total of 56 AEs (45 CPA, eleven placebo) were reported in 30 (20 CPA, ten placebo) out of the 45 participants in the safety population (30 CPA, 15 placebo). There were ten events (nine CPA, one placebo) among four participants (three CPA, one placebo) that were judged by the principal investigator to be probably or possibly related to the study product. Of these, five were skin-related, and the other five were eye, gastrointestinal, general, immune, and vascular disorders. The skin-related disorders occurred in three participants, two in the CPA group, and one in the placebo group. This difference was not statistically significant.
Blood pressure was significantly reduced compared to baseline by a mean of 7.8 mmHg for systolic blood pressure (P=0.01) and a mean of 4.7 mmHg for diastolic blood pressure (P<0.001) after 6 weeks of treatment with CPA. These changes were not clinically significant. No between-group differences were noted for heart rate, blood pressure or safety laboratory parameters with the exception of sodium concentration and red blood cell count. Sodium and red blood cell count were both significantly decreased in the CPA group as compared to the placebo group (P=0.02 and P=0.03, respectively). However, these changes were of small magnitude and not clinically important. No safety concerns were raised throughout the course of this study.
Discussion
The annual direct cost of AK management in the US was estimated in 2004 to be $1.2 billion, with indirect costs totaling $295 million. These costs stand to increase as the baby boomer generation matures. Common forms of treatment for AKs include prophylaxis (ie, reducing solar exposure), lesion elimination, and preventative maintenance.24 Development of field-directed treatments for AK with less adverse side effects may reduce both the treatment and indirect costs of AK management and lower the risk of skin cancer. The current study investigated the efficacy and safety of an alternative treatment for AKs, CPA, in a population of immunocompetent AK patients.
Although complete clearance was not achieved, participants treated with CPA showed a greater decrease in the average AK lesion area than those treated with placebo. This difference was not statistically significant, likely due in part to the reduction in the average area of lesions in the placebo-treated group and to an insufficient sample size. Twenty-five percent of AK lesions spontaneously regress without active treatment, accounting for the placebo effect observed in this study and strengthening the case for conservative treatment of AKs.2 Marks et al followed subjects with AK lesions who were not provided with treatment, for 12 months, and reported that some AKs were self-resolving as a result of the innate immune response triggered by the lesions. AK lesions have a risk of recurrence, however, whether recurrence may be prevented by preventative treatment is yet to be determined.2 The immune response to AK lesions has been documented histologically to be an inflammatory response that may be fairly dense, comprised mainly of lymphocytes and plasma.25 If the immune response is sufficient, the lesions regress and spontaneous remission may occur. The percentage of participants experiencing a >10% reduction in average lesion area was significantly greater with CPA than placebo at 3 and 6 weeks and showed a trend toward significance at 12 weeks. This suggests that CPA induces regression of AK lesions beyond what occurs spontaneously. Moreover, the sustained reduction of average lesion area in the CPA-treated participants at 36 weeks further supports the efficacy of the treatment.
Although complete AK clearance was not achieved during this study, participants treated with CPA showed a greater decrease in the average AK lesion area than those treated with placebo. This observation is crucial due to the association between lesion size and SCC development. Two histological studies demonstrated that AK progression to SCC is not a rare event.26,27 Ehrig et al biopsied 220 AK lesions and Carag et al 69 AK lesions, and reported 3.2% and 13% of these lesions to be SCC in situ, while 1.4% and 3% of lesions were invasive SCC.26,27 The higher rate reported by Carag et al was attributed to the fact that larger lesions were biopsied in their study. AK lesions with a diameter greater than 1 cm and rapid enlargement has been associated with increased risk of SCC.28 Additionally, Cook et al reported an association between changes in lesion size and SCC.29 Therefore, the greater reduction in AK lesion area observed in the CPA group in this study is promising.
The sustained reduction of average lesion area in the CPA-treated participants at 36 weeks suggests a long term effect of CPA. It is possible that a longer treatment period (greater than 12 weeks) may be necessary to achieve resolution of AK lesions with CPA.
Average lesion area was identified as the most accurate measure of a treatment effect as there was high variability between participants in the baseline values of the number and total area of lesions. When stratified by baseline lesion size (<100 mm2, 100–249 mm2, 250–499 mm2), CPA displayed a 1.3, 1.9, and 2.0× greater reduction in average lesion size than the placebo cream. A subset analysis revealed that treatment was more effective in decreasing the size of younger (<10 years since onset) than older (>10 years since onset) AK lesions. The implication of this finding is unclear, as little is known about the characteristics of the AK lesions that are more susceptible to develop into SCC; therefore it is difficult to predict which lesions will become invasive.4,30 Also, spontaneous resolution of younger lesions may have confounded the effectiveness of CPA.
Future studies may consider larger sample sizes that permit more extensive analyses (ie, baseline total lesion area ≥250 mm2 and <500 mm2). The difficulty in distinguishing the effects of treatment on less prominent or preclinical lesions due to spontaneous regression could potentially be overcome by stratifying the study population. Furthermore, as CPA is a field-directed treatment, suppressing the development of satellite lesions is an important aspect of preventative therapy that was not investigated in this study. By monitoring the appearance of new lesions, another measure of efficacy may be captured. Interestingly, all but one of the CPA-treated lesions that underwent an observable change in area were located on the participants’ arms, suggesting that skin location may play a role in treatment efficacy. Although a recent Cochrane review showed differential efficacy dependent upon skin location,31 it is unclear whether there is a general effect. Future studies should include a subset analysis of the relevance of lesion location.
Dosing studies may also be warranted for future investigations of CPA. The dose of 7.8% CPA was derived from a previous animal study of 6% CPA with the inclusion of a 1.8% increase to account for dilution by excipients. However, cutaneous absorption of drugs delivered through creams may be lower in man than in mice.32 One of the greatest obstacles to topical treatment is the absorption of the active ingredient through the stratum corneum; which can vary greatly with the vehicle used for delivery.33 Two similar phenolic acids that are used in photo-protective creams have been shown to readily permeate human skin.34 Although it has not been investigated, a similar absorption profile may exist with CPA and an increased dose may increase the effectiveness of treatment while still maintaining a safety profile devoid of the dermatological side effects associated with current topical treatments.
Chronic skin inflammation and oxidative stress from UV exposure are directly involved in the pathogenesis of SCC.35,36 During chronic inflammation free radicals and aldehydes are produced which induce gene mutations and post-translational modifications of key cancer-related proteins.37 UV radiation alters enzymatic and non-enzymatic antioxidants in the human skin thereby affecting the antioxidant defense of various skin layers.38–40 An antioxidant superoxide dismutase has been reported to protect human keratinocytes against UVB-induced injury.41,42
Sinapic acid possesses potent anti-oxidative activity, scavenges free radicals, and protects against neuron and hepatocyte cell death in vivo.43,44 A recent study demonstrated that subcutaneous injections of sinapic acid significantly reduced the occurrence of colonic polyps in the 1,2-dimethylhydrazine rat model of colon carcinogenesis.20 Other studies have shown that sinapic acid possesses anti-inflammatory properties and reduces expression of pro-inflammatory cytokines.45 Together the anti-inflammatory and free radical scavenging properties have been shown to reduce the extent of fibrosis in a rat model of chronic liver injury by decreasing the expression of fibrosis-related factors such as α-smooth muscle actin and transforming growth factor-β1.46 It is possible that CPA resolves AK lesions through a combined mechanism: scavenging free radicals induced by sun damage, reducing the expression of pro-inflammatory cytokines, and reducing the expression of fibrosis-related factors. These mechanisms may allow CPA to be used in conjunction with other pharmaceutical treatments and to itself act both as a treatment for established lesions and to prevent the progression of preclinical lesions in the surrounding skin field.
Conclusion
AK lesion size is associated with increased risk of SCC. Results from the current study show that CPA effectively reduces lesion size in mild AK; therefore, CPA holds potential as an alternative field-directed therapy for AKs. CPA may be most appropriate as a prophylactic treatment for skin chronically exposed to the sun. Concomitant use with other therapies is a novel avenue for study as CPA has anti-inflammatory and anti-oxidative properties and may reduce the need for use of aggressive synthetically-derived products. Future dosing studies and larger clinical trials are required to further establish the efficacy of this alternative treatment.
Acknowledgments
We would like to thank the participants of this study for their willingness and diligence in complying with the study protocol. This study was conducted by Miami Research Associates under the supervision of the medical director and co-author, Patricia Alvarez, MD and dermatologists Ana Gonzalez, MD, Rosa Rojas, MD of Latin American Research (Santo Domingo, Dominican Republic) and Marisela Fernandez, MD and Idelina Sanchez, MD of Clinica Dermatologica de Herrera (Santo Domingo). This study was supported by KGK Synergize Inc. (London, ON, Canada). We acknowledge the technical contributions of Josh Baisley, and thank Nicole Jackson and Andrew Charrette for their editorial contributions and also thank Hui Jun Chew for reviewing and editing the final manuscript.
Disclosure
ME and NG are employees of KGK Synergize, Inc. DK, PA, and MP have no conflicts of interest to disclose.
References
Marks R. Solar keratoses. Br J Dermatol. 1990;122 Suppl 35:49–54. | |
Marks R, Foley P, Goodman G, Hage BH, Selwood TS. Spontaneous remission of solar keratoses: the case for conservative management. Br J Dermatol. 1986;115(6):649–655. | |
Neidecker MV, Davis-Ajami ML, Balkrishnan R, Feldman SR. Pharmacoeconomic considerations in treating actinic keratosis. Pharmacoeconomics. 2009;27(6):451–464. | |
Feldman SR, Fleischer AB Jr. Progression of actinic keratosis to squamous cell carcinoma revisited: Clinical and treatment implications. Cutis. 2011;87(4):201–207. | |
Martin G, Swanson N. Clinical findings using ingenol mebutate gel to treat actinic keratoses. J Am Acad Dermatol. 2013;68(1 Suppl 1):S39–S48. | |
Chen GJ, Feldman SR, Williford PM, et al. Clinical diagnosis of actinic keratosis identifies an elderly population at high risk of developing skin cancer. Dermatol Surg. 2005;31(1):43–47. | |
Glogau RG. The risk of progression to invasive disease. J Am Acad Dermatol. 2000;42(1 Pt 2):23–24. | |
Marks R, Rennie G, Selwood TS. Malignant transformation of solar keratoses to squamous cell carcinoma. Lancet. 1988;1(8589):795–797. | |
Ceilley RI, Jorizzo JL. Current issues in the management of actinic keratosis. J Am Acad Dermatol. 2013;68(1 Suppl 1):S28–S38. | |
Einspahr JG, Stratton SP, Bowden GT, Alberts DS. Chemoprevention of human skin cancer. Crit Rev Oncol Hematol. 2002;41(3):269–285. | |
Jeffes EWB 3rd, Tang EH. Actinic keratosis: Current treatment options. Am J Clin Dermatol. 2000;1(3):167–179. | |
Jeffes EW, McCullough JL, Weinstein GD, et al. Photodynamic therapy of actinic keratosis with topical 5-aminolevulinic acid: A pilot dose-ranging study. Arch Dermatol. 1997;133(6):727–732. | |
Szeimies RM, Karrer S, Radakovic-Fijan S, et al. Photodynamic therapy using topical methyl 5-aminolevulinate compared with cryotherapy for actinic keratosis: A prospective, randomized study. J Am Acad Dermatol. 2002;47(2):258–262. | |
Gupta AK, Paquet M. Network meta-analysis of the outcome ‘participant complete clearance’ in nonimmunosuppressed participants of eight interventions for actinic keratosis: A follow-up on a Cochrane review. Br J Dermatol. 2013;169(2):250–259. | |
[No authors listed] New treatment for actinic keratosis. Med Lett Drugs Ther. 2002;44:57–58. | |
Coleman WP 3rd, Yarborough JM, Mandy SH. Dermabrasion for prophylaxis and treatment of actinic keratoses. Dermatol Surg. 1996;22(1):17–21. | |
Kang S, Goldfarb MT, Weiss JS, et al. Assessment of adapalene gel for the treatment of actinic keratoses and lentigines: A randomized trial. J Am Acad Dermatol. 2003;49(1):83–90. | |
Kurowska EM, Guthrie N, Muir A, Westcott N, Ferguson PJ, Morley K. Chemopreventive effect of canola phenolic acid-enriched extract on 7,12-dimethylbenz[a]anthracene/12-O-tetradecanolylphorbol 12-acetate (DMBA/TPA)-induced mouse skin carcinogenesis. AICR International Research Conference on Food, Nutrition and Cancer; July 17, 2003; Washington DC. | |
Mukherjee R, Chaturvedi P, Baisley J, et al. A phenolic acids rich extract from canola meal: Potential candidate for melanoma skin cancer prevention. Proc Amer Assoc Cancer Res. 2006;47: (Abstract 282):66. | |
Balaji C, Muthukumaran J, Nalini N. Chemopreventive effect of sinapic acid on 1,2-dimethylhydrazine-induced experimental rat colon carcinogenesis. Hum Exp Toxicol. Epub February 14, 2014. | |
Rivers JK, Arlette J, Shear N, Guenther L, Carey W, Poulin Y. Topical treatment of actinic keratoses with 3.0% diclofenac in 2.5% hyaluronan gel. Br J Dermatol. 2002;146(1):94–100. | |
Gupta AK, Davey V, Mcphail H. Evaluation of the effectiveness of imiquimod and 5-fluorouracil for the treatment of actinic keratosis: Critical review and meta-analysis of efficacy studies. J Cutan Med Surg. 2005;9(5):209–214. | |
Siller G, Gebauer K, Welburn P, Katsamas J, Ogbourne SM. PEP005 (ingenol mebutate) gel, a novel agent for the treatment of actinic keratosis: results of a randomized, double-blind, vehicle-controlled, multicentre, phase IIa study. Australas J Dermatol. 2009;50(1):16–22. | |
Roberts WE. Dermatologic problems of older women. Dermatol Clin. 2006;24(2):271–280. | |
Pinkus H, Jallad M, Mehregan AH. The inflammatory infiltrate of precancerous skin lesions. J Invest Dermatol. 1963;41:247–248. | |
Ehrig T, Cockerell C, Piacquadio D, Dromgoole S. Actinic keratoses and the incidence of occult squamous cell carcinoma: a clinical-histopathologic correlation. Dermatol Surg. 2006;32(10):1261–1265. | |
Carag HR, Prieto VG, Yballe LS, Shea CR. Utility of step sections: demonstration of additional pathological findings in biopsy samples initially diagnosed as actinic keratosis. Arch Dermatol. 2000;136(4):471–475. | |
Goldberg LH, Chang JR, Baer SC, Schmidt JD. Proliferative actinic keratosis: three representative cases. Dermatol Surg. 2000;26(1):65–69. | |
Cook BA, Gravely AA, Nelson DB, Warshaw EM. Is tenderness a reliable predictor for differentiating squamous cell carcinomas from actinic keratoses? J Am Acad Dermatol. 2011;65(1):211–212. | |
Roewert-Huber J, Stockfleth E, Kerl H. Pathology and pathobiology of actinic (solar) keratosis – an update. Br J Dermatol. 2007;157 Suppl 2:18–20. | |
Gupta AK, Paquet M, Villanueva E, Brintnell W. Interventions for actinic keratoses. Cochrane Database Syst Rev. 2012;12: CD004415. | |
Dvorakova K, Dorr RT, Valcic S, Timmermann B, Alberts DS. Pharmacokinetics of the green tea derivative, EGCG, by the topical route of administration in mouse and human skin. Cancer Chemother Pharmacol. 1999;43(4):331–335. | |
Kamuhabwa AR, Geboes KR, de Witte PA. Investigation of the absorption of hypericin into the skin of hairless mice. J Pharm Pharmacol. 2000;52(5):487–494. | |
Saija A, Tomaino A, Trombetta D, et al. In vitro and in vivo evaluation of caffeic and ferulic acids as topical photoprotective agents. Int J Pharm. 2000;199(1):39–47. | |
Sander CS, Hamm F, Elsner P, Thiele JJ. Oxidative stress in malignant melanoma and non-melanoma skin cancer. Br J Dermatol. 2003;148(5):913–922. | |
Kostyuk VA, Potapovich AI, Lulli D, et al. Modulation of human keratinocyte responses to solar UV by plant polyphenols as a basis for chemoprevention of non-melanoma skin cancers. Curr Med Chem. 2013;20(7):869–879. | |
Sander CS, Chang H, Hamm F, Elsner P, Thiele JJ. Role of oxidative stress and the antioxidant network in cutaneous carcinogenesis. Int J Dermatol. 2004;43(5):326–335. | |
Poswig A, Wenk J, Brenneisen P, et al. Adaptive antioxidant response of manganese-superoxide dismutase following repetitive UVA irradiation. J Invest Dermatol. 1999;112(1):13–18. | |
Meewes C, Brenneisen P, Wenk J, et al. Adaptive antioxidant response protects dermal fibroblasts from UVA-induced phototoxicity. Free Radic Biol Med. 2001;30(3):238–247. | |
Shindo Y, Hashimoto T. Time course of changes in antioxidant enzymes in human skin fibroblasts after UVA irradiation. J Dermatol Sci. 1997;14(3):225–232. | |
Sasaki H, Akamatsu H, Horio T. Protective role of copper, zinc superoxide dismutase against UVB-induced injury of the human keratinocyte cell line HaCaT. J Invest Dermatol. 2000;114(3):502–507. | |
Sasaki H, Akamatsu H, Horio T. Effects of a single exposure to UVB radiation on the activities and protein levels of copper-zinc and manganese superoxide dismutase in cultured human keratinocytes. Photochem Photobiol. 1997;65(4):707–713. | |
Shin DS, Kim KW, Chung HY, Yoon S, Moon JO. Effect of sinapic acid against carbon tetrachloride-induced acute hepatic injury in rats. Arch Pharm Res. 2013;36(5):626–633. | |
Kim YO, Lee SW, Oh MS, Lee HJ. Effects of sinapic Acid of 4 vessel occlusion model-induced ischemia and cognitive impairments in the rat. Clin Psychopharmacol Neurosci. 2011;9(2):86–90. | |
Yun KJ, Koh DJ, Kim SH, et al. Anti-inflammatory effects of sinapic acid through the suppression of inducible nitric oxide synthase, cyclooxygase-2, and proinflammatory cytokines expressions via nuclear factor-kappaB inactivation. J Agric Food Chem. 2008;56(21):10265–10272. | |
Shin DS, Kim KW, Chung HY, Yoon S, Moon JO. Effect of sinapic acid against dimethylnitrosamine-induced hepatic fibrosis in rats. Arch Pharm Res. 2013;36(5):608–618. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.