Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 9
A placebo-controlled, double-blind clinical trial to evaluate the efficacy of Imedeen® Time Perfection® for improving the appearance of photodamaged skin
Authors Stephens T, Sigler M, Herndon J, Dispensa L, Le Moigne A
Received 21 October 2015
Accepted for publication 18 December 2015
Published 15 March 2016 Volume 2016:9 Pages 63—70
DOI https://doi.org/10.2147/CCID.S98787
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jeffrey Weinberg
Thomas J Stephens,1 Monya L Sigler,1 James H Herndon Jr,2 Lisa Dispensa,3 Anne Le Moigne3
1Thomas J. Stephens and Associates, Inc., Richardson, TX, 2Dermatology Center of Dallas, Dallas, TX, 3Pfizer Consumer Healthcare, Madison, NJ, USA
Objective: To assess the efficacy of Imedeen Time Perfection for improving the appearance and condition of photoaged skin in healthy women.
Methods: This randomized, double-blind, placebo-controlled clinical trial enrolled healthy women, 35–60 years of age, with Fitzpatrick I–III and Glogau II–III skin types and mild-to-moderate facial fine lines/wrinkles. The eligible subjects were randomized to receive two tablets daily of either Imedeen Time Perfection (Imedeen) or a matching placebo for 12 weeks. Efficacy assessments included investigator rating of 16 photoaging parameters (ie, global facial appearance and 15 individual facial parameters and the average of all parameters), instrumentation (ie, ultrasound dermal density, moisture level of the stratum corneum, transepidermal water loss, cutometry), and subjects' self-assessment. Differences in the mean change from baseline to week 12 values on these outcomes were compared between Imedeen and placebo using analysis of variance or a paired t-test.
Results: Seventy-four subjects with primarily Fitzpatrick skin type III (78%–79%) and Glogau type III (53%–58%) completed the study (Imedeen: n=36; placebo: n=38). The mean difference in change from baseline to week 12 for global facial assessment significantly favored Imedeen over placebo (−0.52; P=0.0017). Additionally, the mean differences in the average of all facial photoaging parameters (−0.29), mottled hyperpigmentation (−0.25), tactile laxity (−0.24), dullness (−0.47), and tactile roughness (−0.62) significantly favored Imedeen over placebo (P≤0.05). Significantly greater increases in ultrasound dermal density (+11% vs +1%; P≤0.05) and stratum corneum moisturization (+30% vs +6%; P≤0.05) were also observed for Imedeen than for placebo. There were no significant differences on other instrumental outcomes.
Conclusion: The results of this study suggest that Imedeen Time Perfection can positively affect the appearance of photoaged skin, moisturization, and skin density over 12 weeks of treatment.
Keywords: photoaging, dietary supplement, marine complex
Introduction
Among the intrinsic and extrinsic factors that contribute to the signs of aging skin (eg, fine lines, wrinkles, and discoloration, including lentigines and ephelides),1,2 the primary extrinsic cause is exposure to ultraviolet (UV) radiation.2 Certain nutrients when consumed either through the diet or in the form of dietary supplements can have positive effects on the appearance of aging skin.3 Antioxidant nutrients, including vitamins C and E, selenium, and zinc, can ameliorate the negative effects of UV radiation on the skin by reducing oxidative stress.4,5 Vitamin C is also known to impact the skin in other ways, including supporting collagen synthesis.6,7 Orally consumed plant extracts, such as those from green tea, tomato, and grape seed, can improve the skin’s appearance, provide protection from UV radiation, and reduce oxidation and inflammation.8–12
Imedeen® Time Perfection® (Ferrosan Laboratories S/A, Søeborg, Denmark, which was acquired by Pfizer in December 2011) is an oral dietary supplement formulated with vitamin C, zinc, plant extracts, and the proprietary Imedeen marine complex. The Imedeen marine complex has been shown to improve the structure of basement membrane and the dermis using a human skin equivalent in vitro model.13 Two open-label, noncomparative clinical trials conducted with women of age 35–60 years showed that Imedeen Time Perfection significantly improved a number of photoaging parameters from the start of treatment to the end of the 4- and 12-month study periods.14,15 The current study was designed to evaluate Imedeen Time Perfection for improving the appearance of photodamaged skin in otherwise healthy women using a randomized, placebo-controlled design.
Methods
Study design
The current study was a double-blind, placebo-controlled, 12-week trial conducted at a single center (Thomas J. Stephens and Associates, Inc., Dallas Texas Research Center) located in Carrollton, TX, USA, between December 2002 and March 2003. All subjects were required to provide written, informed consent and to sign a photographic release form. The protocol and informed consent agreement for the study were reviewed and approved by the IntegReview Institutional Review Board. The study was performed in accordance with federal regulations and Good Clinical Practice guidelines.
Study treatment
The subjects were instructed to take two tablets of Imedeen Time Perfection (Imedeen) or placebo daily in the morning for 12 weeks with no specific instructions regarding the timing of meals. The total daily dose of Imedeen contained the proprietary Imedeen marine complex 210 mg, tomato and grape seed extracts ~57 mg total, and vitamin C 60 mg. The placebo tablets were formulated with inert ingredients, primarily maltodextrin, microcrystalline cellulose, and iron oxide.
The subjects were required to replace their current facial cleanser and moisturizer with Purpose® soap (Valeant Consumer Products, Bridgewater, NJ, USA) and Cetaphil® moisturizing lotion (Galderma Laboratories LP, Cranbury, NJ, USA), which were to be used on their faces and legs throughout the duration of the study. The use of any other products on their faces, besides their regularly used color cosmetics, was prohibited. The subjects were provided daily diaries to record study treatment usage times and any relevant comments.
Participants
Inclusion/exclusion criteria
Approximately 90 subjects were screened. The subjects were required to be women of age 35–60 years and have Fitzpatrick skin classification types I–III, a modified Glogau classification II–III, and moderate fine lines or wrinkles on at least one side of the face with a grade of at least 3.5 to a maximum of 6 on a 0–9 scale, where higher scores indicated more severe wrinkling (mild: 0–<3, moderate: 3.5–<6, severe: 6–<9). Subjects were required to be the current users of facial moisturizers ≥3 times/week and in generally good health. The subjects with histories of or current diseases of the skin, including atopic skin diseases, that were deemed by the investigator to be inappropriate for participation in the study were excluded. The subjects were requested to avoid daily sun exposure and use of tanning beds and to not begin using any new personal care products throughout the study. The subjects were also restricted from using supplements or topical products indicated for improving the appearance or condition of the skin; use of a daily multivitamin was permitted.
Other restricted skin treatments and procedures included facial peels or other facial treatments, oral or topical retinoids, or routine use of alpha-, beta-, or polyhydroxy acid products. The subjects were permitted to use current color cosmetic products if they had been used for ≥1 month before the start of the study. The subjects were restricted from initiating or changing hormonal treatments (including birth control) within 3 months prior to the start of the study. Subjects with allergies or sensitivities to seafood, skin care products, or oral dietary supplements were excluded.
Study procedures
Initial eligibility screening was conducted by telephone prior to conducting clinical evaluation procedures (rating of Fitzpatrick skin type, Glogau score, and appearance of fine lines and wrinkles) at the study site. Candidate subjects signed an informed consent agreement. Those who met the visual qualification requirements completed a health and eligibility questionnaire, a confidentiality agreement, and a photographic release form. Those who met all qualification requirements were then issued a subject number and provided with the standardized facial cleanser and moisturizer. At visit 1 and all subsequent visits, women were required to completely remove any facial makeup ≥30 minutes prior to study procedures being performed. Women who had not removed their makeup prior to arriving at the study site were required to do so upon arrival and wait ≥30 minutes before being evaluated.
Approximately 1 week following the screening visit, the subjects returned to the study site for baseline assessments (clinical grading, photography, and instrumentation measurements). They then underwent randomization and distribution of study products. Randomization and blinding of study materials were performed by an independent third party. Neither the investigator nor the subjects were aware of treatment assignments until the study ended and the data were locked for statistical analysis. The subjects were randomized in a balanced manner based on Fitzpatrick skin classification, Glogau categorization, age, and baseline severity of fine lines and wrinkles. The subjects were provided with a 4-week supply of study materials and usage instructions. Approximately 1 week after the baseline visit, clinic personnel contacted the subjects by telephone to assess treatment compliance. The subjects returned to the study site ~4 weeks (visit 3) and 8 weeks (visit 4) from baseline for compliance checks and self-assessments. The subjects returned empty product packaging, unused test materials, and daily diaries and were provided with another 4-week supply of test materials and new diaries. Clinic personnel counted remaining test materials and reviewed diaries to assess compliance. Noncompliant subjects were discontinued from the study.
The subjects returned to the study site at approximately week 12 (visit 5) for compliance assessments and efficacy evaluations, including clinical grading, photography, instrumentation, and self-assessments. The subjects were rated by the same evaluator at baseline and subsequent study visits. Assessment rooms had their temperature and humidity controlled and maintained at a temperature of 64°F–73°F and relative humidity between 32% and 55% to limit the impact of environmental conditions on the outcomes of interest. Temperature and humidity readings were monitored using calibrated external temperature and humidity devices, and adjustments were made as required to maintain these ranges, which were based on the study sponsor’s specifications and guidelines put forth by manufacturers of the biophysical equipment. Any out-of-range readings were documented as protocol violations.
Outcomes
Visual scoring assessments
The subjects were assessed by investigators at baseline and week 12 for the following photoaging parameters: global assessment, periocular fine lines/wrinkles, coarse wrinkles on the cheek, periorbital/crow’s feet wrinkles, mottled hyperpigmentation, pore size, tactile and visual laxity/sagging, dull/matte/sallow or radiant appearance, tactile and visual roughness/texture, undereye dark circles and bags, telangiectasia, skin dryness, and blotchiness. Clinical grading was rated on the following scale: mild: 0–3.0, moderate: 3.5–6.0, and severe: 6.5–9.0.
Standardized facial photographs were taken of each subject at the baseline and week 12 visits to provide photodocumentation of the observed changes in skin aging and for use by the evaluator when performing clinical grading assessments. Full-face digital photographs were taken. The subject’s face was turned to the right or left side (at a 45° angle oriented toward the side of the face qualified by the grader) in one pose and directly faced the camera for a front view (0° angle) in a second pose. A Nikon D100 digital camera body and a Nikkor AF 75–300 mm lens with a Nikon 5T close-up diopter attachment was used for all photography. Digital images (RAW; 12 bits per channel) were recorded using Nikon Capture version 3.5 software.
The subjects performed self-assessments at baseline and at weeks 4, 8, and 12. The self-assessment questionnaire characterized skin on a scale of 1–10, where higher scores (6–10) denoted positive ratings and lower scores (1–5) denoted negative ratings. Week 12 results for facial skin (texture, dryness, softness, fine lines/wrinkles, deep wrinkles, firmness, discoloration, dilated capillaries, and overall appearance) and body skin (skin texture, appearance of varicose veins, dryness overall, dryness of lower legs, and overall appearance) were reported.
Instrumental assessments
Prior to instrumental assessments being performed, the subjects rested for ≥20 minutes to acclimate to the temperature and humidity of the instrumentation room.
Skin resiliency was assessed by cutometry using the Cutometer SEM 575 (Courage + Khazaka Electronic GmbH, Cologne, Germany). Cutometry measures the degree of skin deformation and rate of return as negative pressure is applied and released. An 8 mm probe is placed on the skin, and 400 mbar of negative pressure is applied and released through it. Movement of the skin into and out of the probe is recorded during the application and release of suction. Standardized calculations were used to report skin resiliency and recoil. One cutometer measurement was taken on the center of each subject’s qualified cheek at the midpoint between the lateral level of the eye and the bottom of the nose.
Dermal density was measured using ultrasound. A DUB 20 ultrasound unit (Taberna Pro Medicum, AG, Lüneburg, Germany) was used to take a B scan of each subject’s cheek at the intersection of the “lines” that extend vertically downward from the middle of the eye and horizontally across the bottom of the nose. The system used a standard 20-MHz transducer with a focal distance of 15 mm and amplification of 40 dB.
Moisturization
The moisture content of the stratum corneum was determined using the NOVA Dermal Phase Meter (DPM) 9003 (NOVA Technology Corp., Meredith, NH, USA). The NOVA DPM uses an electrical capacitance method; the measurement is proportional to the dielectric constant of the skin’s surface layers and increases as the skin becomes more hydrated. Duplicate NOVA DPM measurements were taken on the center of each subject’s qualified cheek at the midpoint between the lateral edge of the eye and bottom of the nose. NOVA DPM measurements were also taken on the lateral aspect of each subject’s lower leg.
The integrity of the skin’s barrier function was assessed through transepidermal water loss (TEWL) measurements using the ServoMed Evaporimeter EP2 (ServoMed AB, Stockholm, Sweden). A handheld probe placed on the skin surface sampled relative humidity at two points above the skin’s surface. The rate of water loss was calculated from the measured humidity gradient. Each TEWL measurement is recorded as the average value taken over ~20 seconds after site stabilization. One TEWL measurement was taken on the center of each subject’s qualified cheek at the midpoint between the lateral edge of the eye and the bottom of the nose.
Safety
The occurrence of adverse events (AEs) was assessed based on questioning by site staff and spontaneous reporting.
Statistics
Between-group comparisons of clinical grading and mean percent change scores and percent improvement for other outcomes at week 12 were performed using analysis of variance with a significance level of P≤0.05. Self-assessment scores were analyzed using the top box/bottom box method. Scores of 6–10 were counted as the most positive/favorable responses and scores of 1–5 as the most negative/unfavorable responses. The proportions of subjects responding positively for a given parameter were statistically compared with the proportions of subjects responding negatively, and vice versa.
Results
Subject disposition and demographics
Of the 91 subjects who were enrolled, 17 subjects discontinued and 74 subjects completed the study. The reasons for discontinuation were unable to attend scheduled visit (n=10), voluntary discontinuation (n=3), enrolled in concurrent photoaging study (n=2), AE (n=1), and noncompliance with the study supplement (n=1). The subjects were primarily white (91%–92%), had Fitzpatrick skin classifications of type III (78%–79%), and were more likely to have a modified Glogau classification of type III (53%–58%; Table 1).
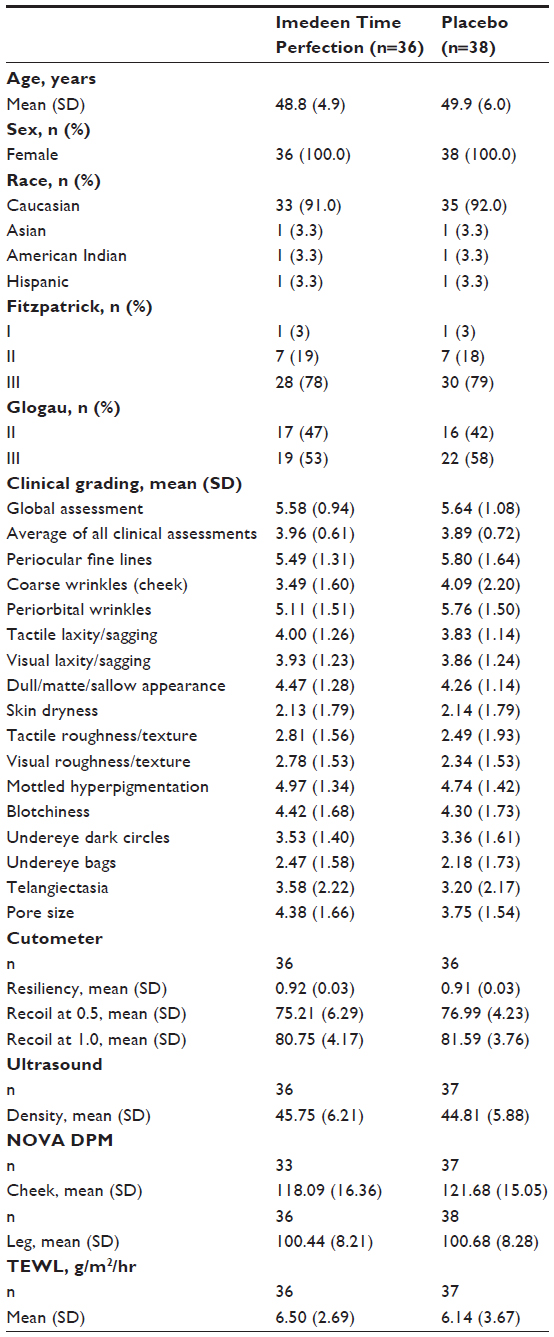 | Table 1 Subject demographics and baseline characteristics |
Investigator ratings
The mean changes in global assessment from baseline to week 12 as rated by the investigators were significantly greater for Imedeen than placebo (P=0.0017). The subjects receiving Imedeen had significantly greater reductions from baseline to week 12 than those receiving placebo for the average of all parameters (−0.29) (Figure 1). Likewise, at week 12, the subjects receiving Imedeen had significantly greater reductions for mottled hyperpigmentation (−0.25), dull appearance (−0.47), tactile roughness (−0.62), and tactile laxity (−0.24; P≤0.05). Between-group differences on the other investigator-rated endpoints did not reach statistical significance (Figure 2).
 | Figure 1 Week 12 mean change from baseline values for the average of all clinical grading parameters and the global assessment. |
 | Figure 2 Week 12 mean change from baseline values for skin color and texture (A), wrinkles and sagging (B), and undereye circles and bags, pore size, telangiectasia, and blotchiness (C). |
Subject self-assessments
The proportion of subjects favorably rating their overall facial skin appearance was not significantly different between Imedeen (61.1%) and placebo (55.3%). Of subjects receiving Imedeen, a significantly greater proportion reported favorable improvement in facial skin texture, dryness, and softness at week 12; the corresponding proportions of subjects receiving placebo who reported favorable improvements on these parameters were not significantly different. Similarly, a significantly greater proportion of subjects who received Imedeen reported favorable improvements in body skin texture and overall dryness, while those receiving placebo did not. No differences were observed on the remaining parameters, including fine lines and deep wrinkles, firmness, discoloration, and dilated capillaries of the facial skin; overall appearance and varicose veins of the body skin; and lower leg dryness.
Instrumental measures
A significantly greater increase (improvement) was observed for Imedeen compared with placebo for NOVA DPM values on the cheek at week 12 (Table 2). No significant between-group differences were found in TEWL at week 12. Ultrasound dermal density showed a significantly greater increase from baseline to week 12 in subjects receiving Imedeen (+11.2%) compared with placebo (+1.0%; P<0.01). No significant between-group differences were found in cutometry assessments at week 12.
 | Table 2
Instrumental measurements |
Safety
During the study, one subject reported two AEs that led to discontinuation, neither of which was deemed to be related to the study material. After taking one dose of Imedeen at baseline, the subject was diagnosed with diverticulitis, treated with antibiotics and analgesics, and allowed to continue in the study. During week 2, the subject developed headache, nausea, and redness on the chest and neck and was discontinued from further participation in the study.
Discussion
When used for 12 weeks, Imedeen Time Perfection was effective in improving the appearance and condition of photodamaged skin. The subjects receiving Imedeen had significantly greater decreases than those receiving placebo for clinical grading of global facial appearance, mottled hyperpigmentation, laxity, clarity, and roughness and for the average of all investigator-rated parameters. Subjects’ self-assessments also demonstrated significant improvement from baseline in the texture, dryness, and softness of the facial skin and texture and dryness of body skin in the Imedeen group but not in the placebo group. Subjects’ self-assessed improvements in skin dryness were supported by instrumentation measurements, where NOVA DPM scores for the Imedeen group were significantly greater than placebo. The change in TEWL was not significantly different from placebo, which suggests that the stratum corneum remained healthy and intact for both groups throughout the study period. This effect is expected since the enrolled subjects had normal, healthy skin at baseline. The significant increase in dermal density observed in the Imedeen group in the current study, as determined by echogenicity, was shown in a previous study that demonstrated the positive effects of Imedeen Time Perfection upon epidermal and dermal structure in vitro.16 The lack of supporting cutometry data for skin resiliency could be attributed to variation in facial location of the two measurements.
Two open-label clinical trials have been conducted with Imedeen Time Perfection that demonstrate significant improvements from baseline on outcomes related to photoaging, including investigator rating of overall facial appearance, ultrasound-measured dermal density, and moisturization.14,15 Previous placebo-controlled clinical trials conducted with different Imedeen formulations (ie, Prime Renewal and Derma One) have demonstrated significant differences versus placebo on numerous photoaging parameters.17,18 Clinical trials with other oral dietary supplements containing combinations of ingredients have also demonstrated some improvements in the appearance of photodamaged skin using various endpoints.19–21
The strengths of this study include its randomized, double-blind, placebo-controlled design; the even distribution of women across skin types, degree of photoaging, and age; the relatively large study population; and utilization of standardized facial cleanser and moisturizer throughout the study to provide a consistent level of skin care between all subjects. A limitation of the study is that although it included standardized facial photography to assist with making clinical assessments, more sophisticated imaging technologies, such as the VISIA Complexion Analysis System (Canfield Imaging Systems, Fairfield, NJ, USA), are now available that were not when this study was conducted. The VISIA system uses technologies that standardize the assessment of numerous skin aging parameters, including spots, wrinkles, and pores.22 Additionally, the clinical relevance of the instrumental measures of skin hydration and TEWL in a population of subjects with healthy skin is unclear.
Conclusion
The results of this study demonstrate that Imedeen Time Perfection improved the appearance and condition of photoaged skin across a range of clinical scoring and instrumentation parameters compared with placebo following 12 weeks of treatment.
Acknowledgments
This study was sponsored by Ferrosan Laboratories S/A, Søeborg, Denmark, which was acquired by Pfizer in December 2011. Medical writing support was provided by Dennis Stancavish, MA, of Peloton Advantage, LLC and was funded by Pfizer.
Disclosure
Thomas J Stephens and Monya L Sigler are employees of Thomas J. Stephens and Associates, Inc., and do not have a financial interest in Pfizer Consumer Healthcare. James H Herndon Jr has no conflicts of interest to disclose. Lisa Dispensa and Anne Le Moigne are employees of Pfizer Consumer Healthcare and own stock and/or stock options in the company. The authors report no other conflicts of interest in this work.
References
Fisher GJ, Wang ZQ, Datta SC, Varani J, Kang S, Voorhees JJ. Pathophysiology of premature skin aging induced by ultraviolet light. N Engl J Med. 1997;337(20):1419–1428. | |
Kohl E, Steinbauer J, Landthaler M, Szeimies RM. Skin ageing. J Eur Acad Dermatol Venereol. 2011;25(8):873–884. | |
Draelos ZD. Cosmetics, diet, and the future. Dermatol Ther. 2012;25(3):267–272. | |
Fuchs J, Kern H. Modulation of UV-light-induced skin inflammation by D-alpha-tocopherol and L-ascorbic acid: a clinical study using solar simulated radiation. Free Radic Biol Med. 1998;25(9):1006–1012. | |
Leccia MT, Richard MJ, Beani JC, et al. Protective effect of selenium and zinc on UV-A damage in human skin fibroblasts. Photochem Photobiol. 1993;58(4):548–553. | |
Boyera N, Galey I, Bernard BA. Effect of vitamin C and its derivatives on collagen synthesis and cross-linking by normal human fibroblasts. Int J Cosmet Sci. 1998;20(3):151–158. | |
Traber MG, Stevens JF. Vitamins C and E: beneficial effects from a mechanistic perspective. Free Radic Biol Med. 2011;51(5):1000–1013. | |
Aust O, Stahl W, Sies H, Tronnier H, Heinrich U. Supplementation with tomato-based products increase lycopene, phytofluene, and phytoene levels in human serum and protects against UV-light-induced erythema. Int J Vitam Nutr Res. 2005;75(1):54–60. | |
De Spirt S, Sies H, Tronnier H, Heinrich U. An encapsulated fruit and vegetable juice concentrate increases skin microcirculation in healthy women. Skin Pharmacol Physiol. 2012;25(1):2–8. | |
Janjua R, Munoz C, Gorell E, et al. A two-year, double-blind, randomized placebo-controlled trial of oral green tea polyphenols on the long-term clinical and histologic appearance of photoaging skin. Dermatol Surg. 2009;35(7):1057–1065. | |
Kopcke W, Krutmann J. Protection from sunburn with beta-carotene – a meta-analysis. Photochem Photobiol. 2008;84(2):284–288. | |
Nichols JA, Katiyar SK. Skin photoprotection by natural polyphenols: anti-inflammatory, antioxidant and DNA repair mechanisms. Arch Dermatol Res. 2010;302(2):71–83. | |
Rietveld M, Janson D, Siamari R, Vicanova J, Andersen MT, El Ghalbzouri A. Marine-derived nutrient improves epidermal and dermal structure and prolongs the life span of reconstructed human skin equivalents. J Cosmet Dermatol. 2012;11(3):213–222. | |
Costa A, Pegas Pereira ES, Favaro R, et al. Treating cutaneous photoaging in women with an oral supplement based on marine protein, concentrated acerola, grape seed extract and tomato extract, for 360 days. Surg Cosmet Dermatol. 2011;3(4):302–311. | |
Costa A, Lindmark L, Arruda LH, et al. Clinical, biometric and ultrasound assessment of the effects of daily use of a nutraceutical composed of lycopene, acerola extract, grape seed extract and Biomarine Complex in photoaged human skin. An Bras Dermatol. 2012;87(1):52–61. | |
Vicanova J, Bouez C, Lacroix S, Lindmark L, Damour O. Epidermal and dermal characteristics in skin equivalent after systemic and topical application of skin care ingredients. Ann N Y Acad Sci. 2006;1067:337–342. | |
Heule F. The improvement of the consequences of cutaneous aging: a double-blind analysis of the effect of the marine protein formula IMEDEEN [abstract]. J Eur Acad Dermatol Venereol. 1994;3(2):224. | |
Skovgaard GR, Jensen AS, Sigler ML. Effect of a novel dietary supplement on skin aging in post-menopausal women. Eur J Clin Nutr. 2006;60(10):1201–1206. | |
Beguin A. A novel micronutrient supplement in skin aging: a randomized placebo-controlled double-blind study. J Cosmet Dermatol. 2005;4(4):277–284. | |
Fanian F, Mac-Mary S, Jeudy A, et al. Efficacy of micronutrient supplementation on skin aging and seasonal variation: a randomized, placebo-controlled, double-blind study. Clin Interv Aging. 2013;8:1527–1537. | |
Udompataikul M, Sripiroj P, Palungwachira P. An oral nutraceutical containing antioxidants, minerals and glycosaminoglycans improves skin roughness and fine wrinkles. Int J Cosmet Sci. 2009;31(6):427–435. | |
Goldsberry A, Hanke CW, Hanke KE. VISIA system: a possible tool in the cosmetic practice. J Drugs Dermatol. 2014;13(11):1312–1314. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.