Back to Journals » Clinical Ophthalmology » Volume 14
A Multicenter, Cross-Sectional Study of the Incidence of Major Macular Diseases That Cause Visual Impairment and Require Therapeutic Intervention in Greece: The ADVICE Study
Authors Karagiannis DA, Lygerou M ![]() , Papadopoulos G, Kabanarou SA
, Papadopoulos G, Kabanarou SA ![]() , Aspiotis M, Dardabounis DC
, Aspiotis M, Dardabounis DC ![]() , Minakakis PG, Spai SI, Koutsandrea C, Oikonomidis P, Pantelopoulou GN
, Minakakis PG, Spai SI, Koutsandrea C, Oikonomidis P, Pantelopoulou GN ![]() , Kousidou OC
, Kousidou OC ![]() , Tsilimbaris M
, Tsilimbaris M ![]()
Received 28 November 2019
Accepted for publication 24 March 2020
Published 25 May 2020 Volume 2020:14 Pages 1417—1426
DOI https://doi.org/10.2147/OPTH.S240417
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Dimitrios A Karagiannis,1 Meropi Lygerou,2 Georgios Papadopoulos,3 Stamatina A Kabanarou,4 Miltiadis Aspiotis5,†, Doukas C Dardabounis,6 Panagiotis G Minakakis,7 Sofia I Spai,8 Chrysanthi Koutsandrea,9 Panagiotis Oikonomidis,10 Georgia N Pantelopoulou,11 Olga C Kousidou,11 Miltiadis Tsilimbaris12 On Behalf of the ADVICE study group
1Ophthalmiatrio Athens Hospital, Athens 10672, Greece; 2OMMA, Ophthalmological Institute of Athens, Athens 11525, Greece; 3Ophthalmology Clinic, General Hospital of Aigio, Aigio, Greece; 4Retina Department, Korgialeneio Benakeio Hellenic Red Cross Hospital, Athens 11526, Greece; 5Ophthalmology Department, University of Ioannina, Ioannina 45500, Greece; 6Ophthalmology Clinic, University Hospital of Alexandroupolis, Dragana 68100, Alexandroupolis, Greece; 7Ophthalmological Clinic, General Hospital of Nikea-Piraeus, Nikea 18545, Greece; 8Ophthalmology Clinic, Sismanogleio General Hospital of Athens, Athens, Greece; 9National and Kapodistrian University of Athens, Filothei, Athens 15237, Greece; 10Ophthalmology Clinic, University General Hospital of Thessaloniki AHEPA, Thessaloniki, Greece; 11Novartis Hellas, Medical Department, Athens, Greece; 12Ophthalmological Clinic, University Hospital of Heraklion, Heraklion, Greece
Correspondence: Olga C Kousidou
Novartis Hellas, Medical Department, 12th Klm National Road No. 1, Athens, Greece
Email [email protected]
Purpose: This multicenter, epidemiological, cross-sectional study aimed to estimate the annual cumulative incidence of major macular diseases that cause visual impairment and require therapeutic intervention in the routine care of Greece.
Methods: The study was carried out between December 2012 and May 2015 in 20 ophthalmology clinics. Over a one-year recruitment period per study site, all treatment naïve adult patients newly diagnosed with wet age-related macular degeneration, visual impairment due to diabetic macular edema or macular edema secondary to retinal vein occlusion requiring therapeutic management and who had not been diagnosed or treated for the same disease in the past were enrolled after providing informed consent. Study data were collected during the single study visit.
Results: A total of 1532 incident cases were enrolled. The estimated annual cumulative incidence of wet age-related macular degeneration, diabetic macular edema and macular edema secondary to retinal vein occlusion requiring therapeutic management was 0.82 [95% confidence interval (CI): 0.76, 0.88; n=723], 0.63 (95% CI: 0.58, 0.69; n=559), and 0.29 (95% CI: 0.25, 0.32; n=250) per 10,000 cases, respectively.
Conclusion: The study provides estimates of the incidence of major macular diseases causing visual impairment and requiring treatment in outpatient hospital settings in Greece, indicating a considerable socioeconomic burden to the healthcare system.
Keywords: anti-VEGF, diabetic macular edema, epidemiology, incidence, retinal vein occlusion, wet age-related macular degeneration
Introduction
Wet age-related macular degeneration (wAMD), diabetic macular edema (DME) and macular edema secondary to retinal vein occlusion (RVO) are the most common ocular disorders leading to vision loss.1–3 The prevalence of late (wet and dry) AMD has been estimated at 0.50% in 45–85 year-old Europeans.4 AMD prevalence increases from 0.41% among the 60–69 year-old group, to 1.71% among the 70–79, and 4.56% in the 80–84 year-old group.4 DME prevalence has been reported to range between 3.8–7.0% among diabetic patients.2,5,6 On the other hand, the global prevalence of branch RVO among persons greater than 30 years of age has been reported to be 0.44%, while the prevalence of central RVO has been reported to be 0.08%.7 Macular edema has been reported to develop in about 5–15% of branch RVO cases within the first year of diagnosis, while most central RVO diagnoses are accompanied by signs of macular edema.3
Vision disturbances, which are frequent among wAMD, DME and RVO patients, can have an impact on the patients’ quality of life. Moreover, these diseases have been associated with work productivity loss, impairment of daily living activities, and high healthcare costs.8–13
The management of wAMD, DME and macular edema secondary to RVO has significantly advanced with the introduction of anti-vascular endothelial growth factor (anti-VEGF) therapies, which provide a therapeutic option that can prevent vision deterioration and in many cases restore vision loss.1,14–16 Due to the high medical costs associated with anti-VEGF therapies, several studies have examined whether the burden such therapies place upon patients and the healthcare system are balanced against the derived benefits. Various such cost-effectiveness analyses in the Greek healthcare setting support that anti-VEGF therapy costs and need for intravitreal administrations are balanced against savings related to improvement in visual acuity and reduction of cases progressing to legal blindness.17–20
Estimates of the incidence of these diseases at a country level are required, since aside from evidence that the incidence varies on a country and race/ethnicity basis, the potential economic impact on the national healthcare system due to the resources needed for management of these diseases is also country-dependent.2,7,21,22 In light of the above, and under the consideration that data on the incidence of macular diseases requiring treatment in Greece were unavailable at the time of study planning, the present study primarily aimed to estimate the annual cumulative incidence of wAMD, visual impairment due to DME and of macular edema secondary to RVO requiring therapeutic management in outpatient settings.
Patients and Methods
Study Design and Setting
This was an epidemiological, multicenter cross-sectional study with a single visit data collection schedule. The study population was recruited by 20 ophthalmology hospital-based outpatient medical retinal clinics, diversely distributed across seven geographical regions of Greece and covering the majority of the ophthalmology clinics in the country (Figure 1). Each study site could recruit patients for an approximate 1-year enrolment period with an up to 7-day allowable extension (i.e. the recruitment length per site could not exceed 372 days). Study data, generated as part of the routine course of care and through medical record review, were collected with the use of a web-based electronic data capture system.
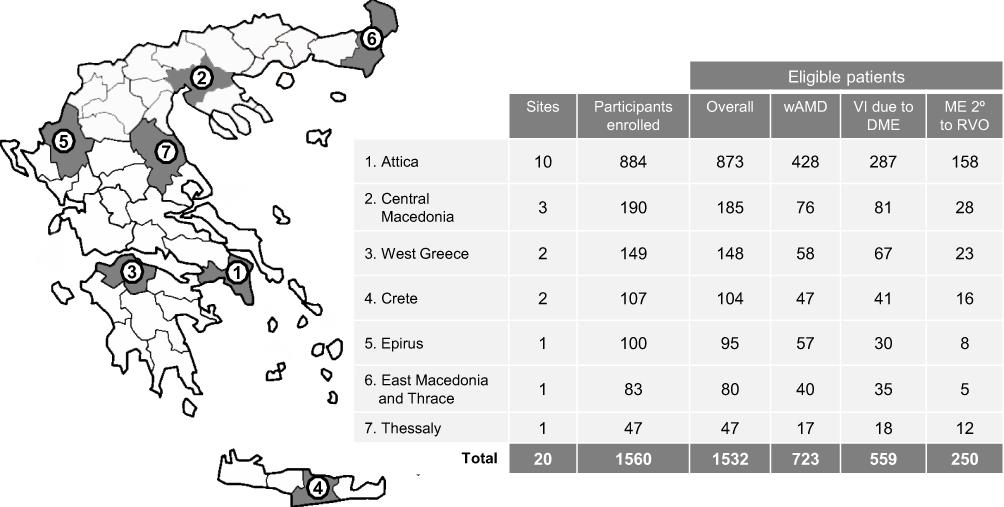 |
Figure 1 Patient disposition per macular disease diagnosis and geographic region of Greece. Abbreviations: wAMD, wet age-related macular degeneration; VI due to DME, visual impairment due to diabetic macular edema; ME 2° to RVO, macular edema secondary to retinal vein occlusion. |
In alignment with the study’s epidemiological nature, potential patient selection bias was controlled by enrolling all patients that fulfilled eligibility criteria and attended the hospital/clinic throughout each site’s 1-year recruitment period. Moreover, the cross-sectional design minimized potential bias from a high drop-out/non-eligible rate.
Comorbid and past medical conditions that according to the physicians’ judgment could affect progression of the macular diseases of interest abstracted from the patients’ medical history or identified during the on-site clinical examination are presented by the Medical Dictionary for Regulatory Activities (MedDRA; version 18.0) terminology preferred term.
This study was designed and implemented in accordance with the principles of the International Conference on Harmonization Good Clinical Practice, the guidelines for Good Pharmacoepidemiology Practices, the ethical principles laid down in the Declaration of Helsinki, as well as all applicable national regulatory requirements. For each participating Hospital site, the study was initiated after obtaining approval by the competent Institutional Review Boards (Scientific Committee/Administrative Council). Prior to the conduct of any study-related procedure, each patient signed a written informed consent form. The study has been registered in the electronic Registry of Non-Interventional Studies posted on the website of the Hellenic Association of Pharmaceutical Companies (https://www.dilon.sfee.gr).
Study Population
The population eligible for study participation, consisted of male and female adult patients over 18 years of age, newly-diagnosed with wAMD, visual impairment due to DME or macular edema secondary to RVO, for whom treatment was indicated at the time of attending the participating outpatient clinics and who had not received treatment for the same disease in the past.
The same patient could be enrolled in the study for two separate incident diagnoses of interest as long as the eligibility criteria were met for both diagnoses. Therefore, incident diagnoses are comprised of first-affected “eyes” rather than patients and will therefore be referred to as incident cases. Furthermore, for patients diagnosed at the same time with the same disease in both eyes, only one eye was enrolled, comprising one incident case.
Study Objectives
The study primarily aimed to determine the annual incidence of wAMD, visual impairment due to DME and of macular edema secondary to RVO requiring therapeutic management, in Greece. In addition, the study captured patient characteristics, diagnostic imaging modalities and therapeutic patterns employed in the routine care setting.
Statistical Methods
Continuous variables have been summarized with the use of descriptive statistical measures [mean, standard deviation (SD)], while categorical variables are displayed as frequencies and percentages (n, %). No imputation of missing data was performed. The primary endpoint was evaluated as the number and percentage of incident cases with the respective 95% confidence interval (CI) based on a binomial distribution. The annual cumulative incidence has been defined as the sum of the annualized number of incident cases for each study site (i.e. the ratio of the actual number of eligible incident cases for the specific site divided by the actual recruitment period for the specific study site multiplied by 365.25) divided by the total Greek adult population [i.e., 8,812,747 according to the ELSTAT 2011 Census (23)]. The 95% CI for the annual cumulative incidence was calculated using normal approximation of Poisson distribution. Association of gender and intravitreal anti-VEGF treatment with the macular disease type has been examined using the Pearson’s chi-square test. Multinomial logistic regression was applied in order to assess the association of the pharmacological treatment/therapeutic modality and best corrected visual acuity (BCVA) on the diagnosis of the three different macular diseases. All statistical tests were two-sided and were performed at a 0.05 significance level. Statistical analyses have been conducted using the statistical software package SAS® v9.3 (SAS Institute, Cary, NC).
Results
Patient Disposition
A total of 1560 cases were registered in the web-based electronic data capture system, of which 1532 were assessed as eligible cases diagnosed with one of the three macular diseases of interest. Twenty-seven cases were non-eligible based on the study’s eligibility criteria, while one patient was enrolled after the 372-day study site recruitment period (Figure 2).
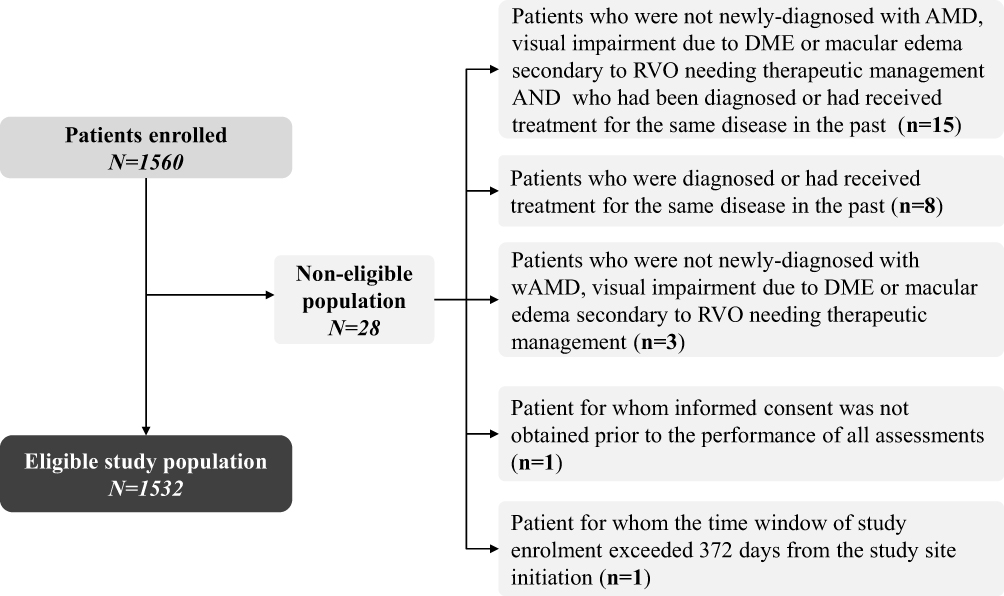 |
Figure 2 Flow-chart of study eligibility and reasons for not being included in the eligible patient population. |
For 17 of the 20 study sites the recruitment period was 372 days, while for the remaining 3 study sites recruitment was prematurely terminated (at 246, 325 and 358 days) for administrative reasons. The earliest study site initiation date was 18-December-2012, while the latest study site close-out date was 30-May-2015; the first case was enrolled on 16-January-2013 and the last on 28-May-2015.
Annual Cumulative Incidence of the Macular Diseases
Of the eligible incident cases enrolled in the study (n=1532), 47.2% (723/1532; 95% CI: 44.7, 49.7) were diagnosed with wAMD, 36.5% (559/1532; 95% CI: 34.1, 38.9) with visual impairment due to DME, and 16.3% (250/1532; 95% CI: 14.5, 18.2) with macular edema secondary to RVO. The distribution of cases per geographic region is presented in Figure 1.
The annual cumulative incidence of wAMD, visual impairment due to DME and macular edema secondary to RVO was 0.82 (95% CI: 0.76, 0.88), 0.63 (95% CI: 0.58, 0.69), and 0.29 (95% CI: 0.25, 0.32) per 10,000 cases, respectively, in an adult population.
Characteristics of Patients Diagnosed with wAMD
The mean (SD) age at disease diagnosis for patients with wAMD was 77.1 (8.3) years. At diagnosis, the mean (SD) BCVA (Snellen equivalent) in the eye with the incident wAMD diagnosis was 2.7/10 (2.2/10) among patients with available data (n=691). As part of the diagnostic imaging screening, fundoscopy was performed in 95.3% (689/723) of the patients, optical coherence tomography in 83.3% (602/723); and fluorescein angiography in 63.6% (460/723). The frequencies of the patterns of imaging examinations performed as part of the diagnostic screening are displayed in Table 1. Intravitreal anti-VEGF injections, with or without other therapeutic modalities, was the treatment of choice for 99.4% (719/723) of the patients (Table 1). The most frequently recorded comorbidities, which according to the physicians’ judgment would impact progression of wAMD, were hypertension (10.0%; 72/723), followed by diabetes mellitus (3.5%; 25/723) and dyslipidemia (2.9%; 21/723).
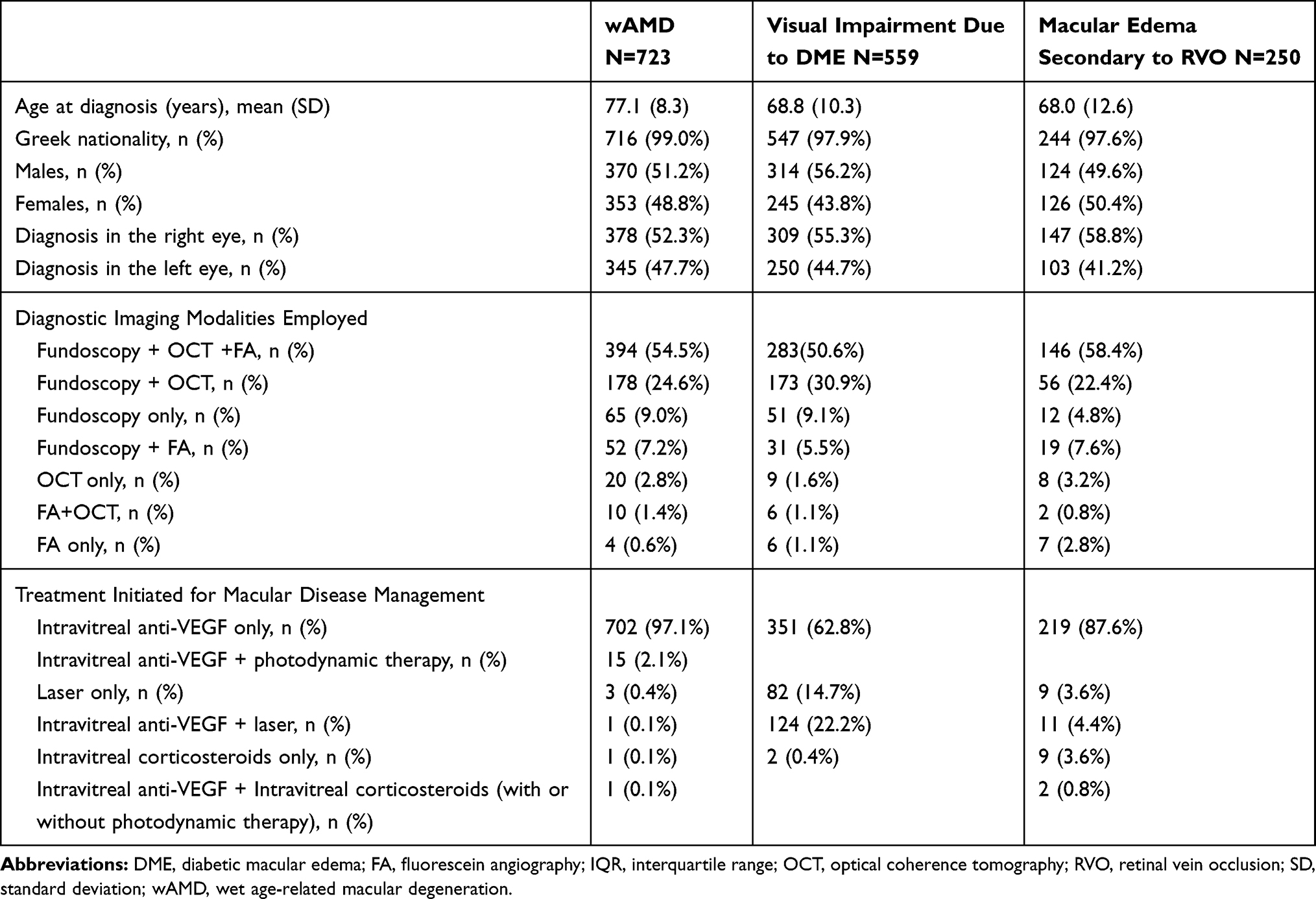 |
Table 1 Patient Characteristics per Macular Disease Diagnosis |
Characteristics of Patients Diagnosed with Visual Impairment Due to DME
The mean (SD) age at diagnosis of visual impairment due to DME was 68.8 (10.3) years. At diagnosis, the mean (SD) BCVA (Snellen equivalent) in the eye with the incident diagnosis was 3.5/10 (2.3/10) among patients with available data (n=533). The diagnostic imaging algorithms are presented in Table 1. Fundoscopy was performed in 96.2% (538/559) of the patients, optical coherence tomography in 84.2% (471/559); and fluorescein angiography in 58.3% (326/559). Intravitreal anti-VEGF injections with or without other therapeutic modalities was the preferred management strategy for 85.0% (475/559) of the patients diagnosed with visual impairment due to DME (Table 1). The most frequently recorded comorbidities, which according to the physicians’ judgment would impact disease progression, were hypertension (9.5%; 53/559), dyslipidemia (2.1%; 12/559) and coronary artery disease (1.1%; 6/559).
Characteristics of Patients Diagnosed with Macular Edema Secondary to RVO
The mean (SD) age at diagnosis of macular edema secondary to RVO was 68.0 (12.6) years, and the mean BCVA (SD) (Snellen equivalent) in the eye with the incident diagnosis among patients with available data (n=234) was 2.7/10 (2.1/10). As part of the diagnostic imaging screening, fundoscopy was performed in 93.2% (233/250) of the patients, optical coherence tomography in 84.8% (212/250), and fluorescein angiography in 69.6% (174/250) (Table 1). Intravitreal anti-VEGF injections with or without other therapeutic modalities was the preferred management strategy for 92.8% (232/250) of the patients (Table 1). The most frequently recorded comorbidities, which according to the physicians’ judgment would impact disease progression, were hypertension (19.6%; 49/250), dyslipidemia (6.4%; 16/250) and diabetes mellitus (6.4%; 16/250), while other comorbidities recorded at a frequency greater than 1% included coronary artery disease (2.0%; 5/250), glaucoma (2.0%; 5/250) and retinal ischemia (1.2%; 3/250).
Association of Gender and Treatment Modality with the Type of Macular Disease
Gender was not shown to be associated with the type of macular disease diagnosis (chi-square P = 0.114). On the other hand, treatment modality (anti-VEGF injections as monotherapy; anti-VEGF injections in combination; and laser monotherapy or intravitreal corticosteroids only) was observed to be associated with the type of macular disease (chi-square P < 0.001). Specifically, utilization of intravitreal anti-VEGF injections as monotherapy was more common among patients with wAMD (97.1%) and macular edema secondary to RVO (87.6%) compared to patients with incident visual impairment due to DME (62.8%) (Table 1). The aforementioned association was also confirmed through multinomial logistic regression analysis. Specifically, the odds of indicating monotherapy with intravitreal anti-VEGF injections were found to be approximately 18 times higher for patients with wAMD vs. visual impairment due to DME [odds ratio (OR): 18.65 (95% CI: 11.54, 30.14); P < 0.001] and approximately 4 times higher for macular edema secondary to RVO vs visual impairment due to DME [OR: 4.42 (95% CI: 2.83, 6.91); P < 0.001] after adjusting for BCVA.
Discussion
The ADVICE study has provided evidence that more than 1500 incident cases of wAMD, visual impairment due to DME and macular edema secondary to RVO requiring therapeutic management are diagnosed annually in outpatient settings in the major hospitals/clinics of Greece with dedicated retina centers, suggesting a sizeable socioeconomic burden of these diseases, which are considered leading causes of vision loss and blindness, and are associated with impaired quality of life and work productivity loss.8–13
Importantly, the incidences reported in ADVICE represent cases requiring treatment, and pertain to patients diagnosed in an outpatient clinic setting who were not diagnosed with the same disease in the past in the non-study eye and were willing to provide written informed consent for study participation. Therefore, incidences reported in ADVICE are likely to be lower than those reported in other studies with a broader population than ours. This point should be kept in mind when interpreting the outcomes and comparing them with those of studies with different designs.
The annual cumulative incidence of wAMD was estimated to be 0.82 per 10,000 (or 0.0082%) in the adult population of Greece.23 Additionally, taking into consideration that 96.4% (697/723) of incident wAMD cases were diagnosed in patients aged greater than 60 years, an incidence of 2.5 per 10,000 (i.e. 0.025%) would be derived in our study for a population >60 years of age.23 These estimates considerably differ from annual incidence estimates reported in the literature, which range from 0.13% to 0.31%.21,22,24–28 Specifically, an annual incidence of 0.29% for wAMD patients >60 years has reported in the study of Geirsdottir et al,24 a 3-year incidence of 0.94% (i.e. an approximate annual incidence of 0.31% if it was to be assumed that the incidence per year is steady) has been reported in a US study using insurance claims data of a Medicare-age population 65 years and older,25 while a 15-year cumulative incidence of 2.0% in patients 43–86 years of age was reported in the Beaver-Dam population cohort study (roughly corresponding to an annual incidence of 0.13%).26 Similarly, meta-analyses of published studies have reported an annual incidence of wAMD of 0.14% among men and 0.23% among women ≥50 years of age residing in the UK21 and of 0.18% among American whites aged ≥50 years.22 However, none of the previously mentioned studies specifically examined incident cases requiring treatment, which may account for the observed variation. This is further supported by the fact that the UK Royal College of Ophthalmologists reports that each year in the UK approximately 26,000 people diagnosed with wAMD are eligible for treatment,27 which when taking into consideration an adult UK population of approximately 52 million28 would translate to an annual incidence of wAMD requiring treatment with anti-VEGFs of 0.05%. This figure is much closer to our estimate of 0.025% in a population > 60 years of age than those described above from other studies, likely because, similarly to our study, it is specific to cases requiring treatment.
Moreover, in the present study, the annual incidence of macular edema secondary to RVO was estimated to be 0.0029%. In the Blue Mountains Eye study, the frequency of macular edema among cases with branch RVO ≥49 years of age was reported to be 18.5%.29 Therefore, by extrapolation, the annual cumulative incidence of macular edema due to branch RVO could be roughly estimated at 0.022% (based on the study’s reported 10-year incidence of 1.2%), but the small number of cases with macular edema (n=5) limits the weight of this evidence. Furthermore, in the study of Petrella et al30 the annual incidence of visual impairment due to macular edema secondary to RVO among patients 49 years and older was reported to be 0.077% (0.056% for branch and 0.021% for central RVO). Taking into consideration that the annual cumulative incidence of macular edema secondary to RVO in a population 50 years and older in the ADVICE study is estimated to be 0.0056% (based on a population of 4,126,475 residents >50 years old in Greece23), some similarity with the findings of Petrella et al30 emerges.
Finally, the annual cumulative incidence of visual impairment due to DME in the ADVICE study was estimated to be 0.0063%. Comparison of this finding to other studies is hindered by the following factors: our study has specifically focused on incident cases with visual impairment due to DME and with no prior diagnosis of this condition; and secondly, published data on the incidence of DME are reported for patients with diabetes rather than the general population, and most published evidence stems from population-based cohort studies with diabetics free of diabetic retinopathy at baseline, a factor which is not present in ADVICE. However, if we were to take into consideration that diabetics comprise about 7.0% of the Greek population,31 the incidence of visual impairment due to DME requiring therapeutic management in our study would be estimated at approximately 0.09% among diabetics.
Treatment of these ocular diseases with anti-VEGF monotherapy was the most commonly indicated treatment practice, supporting the evidence on the benefit of this therapeutic category in the aforementioned diseases in terms of preventing progression to blindness but also of improving visual acuity.1,14–16,32 Interestingly, fundoscopy was performed in nearly all patients regardless of type of diagnosis, but optical coherence tomography was performed in nearly 8 out of 10 patients. The reasons behind the fact that optical coherence tomography was not part of the diagnostic algorithm for the remaining patients merits further investigation.
ADVICE is the largest study to date to report on the incidence of macular diseases requiring therapeutic management in Greece. Nonetheless, the study has certain limitations, which ought to be mentioned. First, due to the fact that the recruitment period for three of the study sites was lower than one year (246, 325 and 358 days, respectively), the sum of the annualized number of newly diagnosed cases per year for each study site was used as the numerator in the calculation of the annual cumulative incidence, potentially compromising the accuracy of the derived incidence. It should be stated that under the assumption that the incidence is steady throughout the year, there would be no limitation from the aforementioned concern. Moreover, the study sites recruited cases during both overlapping and non-overlapping time periods, spanning from 18 December 2012 to 30 May 2015, thus the incidence rate does not correspond to a particular year examined. Additionally, the following factors may have precluded enrollment of all cases across Greece during the study recruitment period: i) patients diagnosed in the private office-based practices, inpatient settings, or elderly patients residing in nursing homes or too frail to visit an outpatient clinic were not included in the study; ii) the list of participating ophthalmology centers/clinics covers the 20 largest ophthalmology clinics in Greece, which treat the majority of, but not all, cases with macular diseases at a national level; and iii) only seven of the 13 geographical regions of Greece, are represented in the study. Nonetheless, it is important to mention that these geographic regions are residence to about 80% of the Greek population, and that they include the two most populous regions of Greece. This, combined with the fact that most patients residing in rural and semi-urban regions of Greece usually visit major hospital sites represented in this study, minimizes the size of the potential underestimation of the study outcome, and strengthens the representativeness of the study results. Moreover, since there are no referral centers for diabetic screening in Greece and patients with diabetes are likely to attend hospitals due to disease-related complications, patient referral to an ophthalmologist within the same hospital/clinic is likely to be high, enriching identification of patients with DME. In addition, among our study’s strengths is the inclusion of a rather broad patient population of either gender, any age above 18 years, including the elderly, and specifically as it pertains to DME regardless of the type of diabetes.
Conclusion
In summary, the present study is the first large-scale study in Greece to report on the incidence of wAMD, visual impairment due to DME and macular edema secondary to RVO requiring therapeutic management in an outpatient population of Greece who has not been diagnosed or treated for the same disease in the past. The study outlines a sizeable socioeconomic burden of these diseases and has important implications for healthcare decision-makers, in terms of reimbursement policies related to therapies indicated for the management of the examined diseases and policies related to reducing the number of cases progressing to legal blindness.
Abbreviations
anti-VEGF, anti-vascular endothelial growth factor; BCVA, best corrected visual acuity; DME, diabetic macular edema; RVO, retinal vein occlusion; wAMD, Wet age-related macular degeneration.
Acknowledgments
The authors are indebted to the study participants and the following principal and sub-investigators (in alphabetical order) which are part of the ‘ADVICE study group’: Dr. Anastasopoulos Eleftherios, Dr. Asteriadis Solon, Dr. Brazitikos Periklis, Dr. Charonis Alexandros, Dr. Chatziralli Eirini, Dr. Chatzispasou Efterpi, Dr. Christodoulou Katerina, Dr. Datseris Ioannis, Dr. Dimitrakos Stavros, Dr. Dimopoulou Anastasia, Dr. Doumouchtsis Evaggelos, Dr. Douvali Maria, Dr. Droutsas Konstantinos, Dr. Exarchou Artemis, Dr. Farmakakis Nikolaos, Dr. Feretis Ilias, Dr. Fotiou Pantelis, Dr. Georgakopoulos Constantinos, Dr. Gourgouli Ioanna, Dr. Kalfa Marietta, Dr. Kalogeropoulos Christos, Dr. Kalogeropoulou Maria, Dr. Kandarakis Artermios, Dr. Kanellas Dimitrios, Dr. Kanellopoulos Spyridon, Dr. Kapsala Zoi, Dr. Karamitsos Thanos, Dr. Kartsani Olga, Dr. Kasimatis Nikolaos, Dr. Katsimpris Ioannis, Dr. Kotoula Maria, Dr. Kotsolis Athanasios, Dr. Koukoula Stavrenia, Dr. Kourentis Christina, Dr. Kouris Anastasios, Dr. Kozompolis Vasilios, Dr. Lake Simeon, Dr. Lamprinakis Ioannis, Dr. Lamprou Lampros, Dr. Lekkas Anestis, Dr. Liarakos Vasilios, Dr. Makri Olga, Dr. Makris Georgios, Dr. Malamos Panagiotis, Dr. Markopoulos Konstantinos, Dr. Mela Iphigenia, Dr. Mersinoglou Adreana, Dr. Miltsakakis Dimitrios, Dr. Mitropoulos Panagiotis, Dr. Mitsopoulou Maria, Dr. Mpourantani Steliana, Dr. Nanos Panagiotis, Dr. Nikolidaki Paraskevi, Dr. Papaefthimiou Ioannis, Dr. Papageorgiou Dimitrios, Dr. Paparnaki Aikaterini, Dr. Paragioudaki Elissavet, Dr. Pappas Georgios, Dr. Parikakis Efstratios, Dr. Pavlakis Kosmas, Dr. Rantza Irene, Dr. Roumpi Ioanna, Dr. Rouvas Alexandros, Dr. Simeonidis Chrisanthos, Dr. Sokolakis Thomas, Dr. Sousouras Thanos, Dr. Theodosiadis Panagiotis, Dr. Tservakis Ioannis, Dr. Tsironi Evangelia, Dr. Stefaniotou Maria, Dr. Tranos Paris, Dr. Tzetzi Despoina, Dr. Vachtsevanos Thanos, Dr. Vaikoussis Emmanouil, Dr. Vakalis Athanasios, Dr. Xirou Tina. Special thanks to the study CRAs Kokkou Eleni and Skarmoutsou Ioanna. The authors also wish to thank Qualitis Ltd. for medical writing support funded by Novartis Hellas, S.A.C.I.
List of Study Sites
University Ophthalmology Clinic, General Hospital of Athens “G. Gennimatas”, Athens, Greece; State Ophthalmology Clinic, General Hospital of Athens “G. Gennimatas”, Athens, Greece; Ophthalmiatrio of Athens, A’ Ophthalmology Clinic, Athens, Greece; Ophthalmiatrio of Athens, B’ Ophthalmology Clinic, Athens, Greece; “Korgialenio-Mpenakio” E.E.S. General Hospital of Athens, Athens, Greece; University General Hospital “Attikon”, Athens, Greece; OMMA, Ophthalmological Institute of Athens, Athens, Greece; University General Hospital of Alexandroupoli, Alexandroupoli, Greece; General Hospital of Thessaloniki, “G. Papageorgiou”, Thessaloniki, Greece; AHEPA, University General Hospital of Thessaloniki, Thessaloniki, Greece; University General Hospital of Ioannina, Ioannina, Greece University General Hospital of Heraklion (PAGNI), Heraklion, Greece; “Venizeleio-Pananio” General State Hospital of Heraklion, Heraklion, Greece; University General Hospital of Larissa, Larissa, Greece; University General Hospital of Patras, Patras, Greece; General Hospital of Aigion, Aigion, Greece; Athens Vision, Athens, Greece; Ophthalmica Clinic of Thessaloniki, Thessaloniki, Greece; General Hospital of Nikea, Piraeus, Greece; Amalia Fleming Hospital of Athens, Athens, Greece.
Presentation at Meetings
Presented in part at the 49th Panhellenic Congress of Ophthalmology, Thessaloniki, May 2016.
Funding
The study was supported by Novartis Hellas, S.A.C.I.
Disclosure
Dimitrios A. Karagiannis, Stamatina A. Kabanarou, Doukas C. Dardabounis, Panagiotis Oikonomidis and Miltiadis Tsilimbaris declare a financial interaction with Novartis Hellas (in terms of consultancy services). Georgia N. Pantelopoulou is a former employee of Novartis Hellas and Olga C. Kousidou is an employee of Novartis Hellas. Sofia I. Spai reports grants from Sismanogleio-Am. Fleming General Hospital of Athens, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Buckle M, Lee A, Mohamed Q, et al. Prevalence and incidence of blindness and other degrees of sight impairment in patients treated for neovascular age-related macular degeneration in a well-defined region of the United Kingdom. Eye (Lond). 2015;29(3):403–408. doi:10.1038/eye.2014.296
2. Varma R, Bressler NM, Doan QV, et al. Prevalence of and risk factors for diabetic macular edema in the United States. JAMA Ophthalmol. 2014;132(11):1334–1340. doi:10.1001/jamaophthalmol.2014.2854
3. Laouri M, Chen E, Looman M, Gallagher M. The burden of disease of retinal vein occlusion: review of the literature. Eye (Lond). 2011;25(8):981–988. doi:10.1038/eye.2011.92
4. Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014;2(2):e106–e116. doi:10.1016/S2214-109X(13)70145-1
5. Ding J, Wong TY. Current epidemiology of diabetic retinopathy and diabetic macular edema. Curr Diab Rep. 2012;12(4):346–354. doi:10.1007/s11892-012-0283-6
6. Yau JW, Rogers SL, Kawasaki R, et al.; Meta-Analysis for Eye Disease (META-EYE) Study Group. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care. 2012;35(3):556–564. doi:10.2337/dc11-1909
7. Rogers S, McIntosh RL, Cheung N, et al; International Eye Disease Consortium. The prevalence of retinal vein occlusion: pooled data from population studies from the United States, Europe, Asia, and Australia. Ophthalmology. 2010;117(2):313–319. doi:10.1016/j.ophtha.2009.07.017
8. Abraldes MJ, Pareja A, Roura M; en representación del grupo del estudio OBSERVAR. Analysis of costs associated with the management and morbidity of diabetic macular oedema and macular oedema secondary to retinal vein occlusion. Arch Soc Esp Oftalmol. 2016;91(6):273–280. doi:10.1016/j.oftal.2015.11.019
9. Brook RA, Kleinman NL, Patel S, et al. United States comparative costs and absenteeism of diabetic ophthalmic conditions. Postgrad Med. 2015;127(5):455–462. doi:10.1080/00325481.2014.994468
10. Fekrat S, Shea AM, Hammill BG, et al. Resource use and costs of branch and central retinal vein occlusion in the elderly. Curr Med Res Opin. 2010;26(1):223–230. doi:10.1185/03007990903439046
11. Gopinath B, Liew G, Burlutsky G, Mitchell P. Age-related macular degeneration and 5-year incidence of impaired activities of daily living. Maturitas. 2014;77(3):263–266. doi:10.1016/j.maturitas.2013.12.001
12. Hodgson N, Wu F, Zhu J, et al. Economic and quality of life benefits of anti-VEGF therapy. Mol Pharm. 2016;13(9):2877–2880. doi:10.1021/acs.molpharmaceut.5b00775
13. Wallick CJ, Hansen RN, Campbell J, et al. Comorbidity and health care resource use among commercially insured non-elderly patients with diabetic macular edema. Ophthalmic Surg Lasers Imaging Retina. 2015;46(7):744–751. doi:10.3928/23258160-20150730-09
14. Bressler NM, Doan QV, Varma R, et al. Estimated cases of legal blindness and visual impairment avoided using ranibizumab for choroidal neovascularization: non-hispanic white population in the United States with age-related macular degeneration. Arch Ophthalmol. 2011;129(6):709–717. doi:10.1001/archophthalmol.2011.140
15. Varma R, Bressler NM, Doan QV, et al. Visual impairment and blindness avoided with ranibizumab in hispanic and non-hispanic whites with diabetic macular edema in the United States. Ophthalmology. 2015;122(5):982–989. doi:10.1016/j.ophtha.2014.12.007
16. Gerding H, Monés J, Tadayoni R, et al. Ranibizumab in retinal vein occlusion: treatment recommendations by an expert panel. Br J Ophthalmol. 2015;99(3):297–304. doi:10.1136/bjophthalmol-2014-305041
17. Athanasakis K, Fragoulakis V, Tsiantou V, et al. Cost-effectiveness analysis of ranibizumab versus verteporfin photodynamic therapy, pegaptanib sodium, and best supportive care for the treatment of age-related macular degeneration in Greece. Clin Ther. 2012;34(2):446–456. doi:10.1016/j.clinthera.2012.01.005
18. Kourlaba G, Chatzikou M, Pantelopoulou G, Maniadakis N. Health and economic outcomes related to delay between medical indication and treatment with ranibizumab in age-related macular degeneration in Greece. Value Health. 2015;18(7):A423. doi:10.1016/j.jval.2015.09.557
19. Kourlaba G, Tzanetakos C, Datseris J, et al. Cost-effectiveness analysis of intravitreal aflibercept in the treatment of neovascular age-related macular degeneration in Greece. Value Health. 2015;18(7):A421. doi:10.1016/j.jval.2015.09.557
20. Kourlaba G, Relakis J, Mahon R, et al. Cost-utility of ranibizumab versus aflibercept for treating Greek patients with visual impairment due to diabetic macular edema. Cost Eff Resour Alloc. 2016;14(1):7. doi:10.1186/s12962-016-0056-1
21. Owen CG, Jarrar Z, Wormald R, et al. The estimated prevalence and incidence of late stage age related macular degeneration in the UK. Br J Ophthalmol. 2012;96(5):752–756. doi:10.1136/bjophthalmol-2011-301109
22. Rudnicka AR, Kapetanakis VV, Jarrar Z, et al. Incidence of late-stage age-related macular degeneration in American whites: systematic review and meta-analysis. Am J Ophthalmol. 2015;160(1):85–93.e3. doi:10.1016/j.ajo.2015.04.003
23. Hellenic Statistical Authority. General population census 2011. Available from: http://www.statistics.gr/portal/page/portal/ESYE/PAGE-census2011. Accessed November 7, 2015.
24. Geirsdottir A, Jonsson O, Thorisdottir S, et al. Population-based incidence of exudative age-related macular degeneration and ranibizumab treatment load. Br J Ophthalmol. 2012;96(3):444–447. doi:10.1136/bjophthalmol-2011-300304
25. Javitt JC, Zhou Z, Maguire MG, et al. Incidence of exudative age-related macular degeneration among elderly Americans. Ophthalmology. 2003;110(8):1534–1539. doi:10.1016/S0161-6420(03)00495-0
26. Klein R, Klein BEK, Knudtson MD, et al. Fifteen-year cumulative incidence of age-related macular degeneration: the Beaver Dam Eye Study. Ophthalmology. 2007;114(2):253–262. doi:10.1016/j.ophtha.2006.10.040
27. The Royal College of Ophthalmologists – Scientific Department: Age-Related Macular Degeneration: guidelines for Management. September, 2013. Available from: https://www.rcophth.ac.uk/standards-publications-research/clinical-guidelines/.
28. Office for National Statistics. 2011 census: population estimates for the United Kingdom. March, 2011. Available from: http://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/bulletins/2011censuspopulationestimatesfortheunitedkingdom/2012-12-17.
29. Cugati S, Wang JJ, Rochtchina E, Mitchell P. Ten-year incidence of retinal vein occlusion in an older population. The Blue Mountains eye study. Arch Ophthalmol. 2006;124(5):726–732. doi:10.1001/archopht.124.5.726
30. Petrella RJ, Blouin J, Davies B, Barbeau M. Incidence and characteristics of patients with visual impairment due to macular edema secondary to retinal vein occlusion in a representative Canadian cohort. J Ophthalmol. 2012;2012:723169.
31. International Diabetes Federation. IDF Diabetes Atlas.
32. Lally DR, Shah CP, Heier JS. Vascular endothelial growth factor and diabetic macular edema. Surv Ophthalmol. 2016;61(6):759–768. doi:10.1016/j.survophthal.2016.03.010
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.