Back to Journals » Clinical Ophthalmology » Volume 12
A clinical assessment of visual performance of combining the TECNIS® Symfony Extended Range of Vision IOL (ZXR00) with the +3.25 D TECNIS Multifocal 1-piece IOL (ZLB00) in subjects undergoing bilateral cataract extraction
Authors Black S
Received 13 June 2018
Accepted for publication 29 August 2018
Published 23 October 2018 Volume 2018:12 Pages 2129—2136
DOI https://doi.org/10.2147/OPTH.S175901
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sondra Black
Crystal Clear Vision Canada, ON, Canada
Purpose: To combine the increased depth of focus of the TECNIS® Symfony intraocular lens (IOL) with a TECNIS Multifocal (MF) low-add IOL (+3.25) to enable a patient to be less dependent on corrective lenses.
Setting: Clinic in Canada.
Design: Single-center, prospective, open-label.
Materials and methods: Fifty patients were enrolled for bilateral surgery. Patients were implanted with TECNIS Symfony Extended Range of Focus lens in the dominant eye, and TECNIS low-add +3.25 MF IOL in the non-dominant eye. Patients were ≥18 years of age and had best-corrected visual acuity >20/30 in both eyes, pupil size >3.5 mm, and <1.5 D of corneal astigmatism. Patients were evaluated preoperatively, operatively, and postoperatively on Day 1, Day 7, Month 1, and Month 3. Postoperative evaluations at Month 3 were completed by 32 of 50 patients enrolled, and included distance, intermediate and near visual acuity (VA), and subjective outcomes.
Results: Three months postoperatively, binocular results without correction revealed 97% (29/30) of patients had distance VA of 20/20 or better, 97% (29/30) had intermediate VA of 20/25 or better, and 94% (28/30) had near VA of 20/25 or better. At Month 3, the majority of patients reported “none” for visual symptoms of glare (30/30, 100%), halo (29/30, 96.6%), starbursts (29/30), or other – blur (30/30, 100%).
Conclusion: Three months postoperatively, the combination of the increased depth of focus of the TECNIS Symfony IOL with a TECNIS MF low-add (+3.25) IOL may provide excellent uncorrected VA at near, intermediate, and far distances with minimal ocular symptoms.
Keywords: extended range of vision, TECNIS Symfony, multifocal IOL, low-add IOL, ZXR00, ZLB00, contralateral, blended vision
Introduction
Previously, patients undergoing cataract surgery and implantation with a monofocal intraocular lens (IOL) needed to wear glasses, either bifocals or reading glasses, postoperatively in order to see objects from near to intermediate distances. Recent multifocal intraocular lens (MIOL) technologies offer at least 2 or 3 focal points for near to distance vision, providing pseudoaccomodation.1 Lens replacement surgery with MIOL technology can offer patients with cataracts the opportunity to be less dependent on, or even free of, eyeglasses, readers, or bifocals after cataract surgery.2,3 This flexibility provides not just a solution to eliminate glasses, but a functional convenience that allows patients with cataracts to conduct their daily living activities in an unencumbered manner.
However, a common downside of MIOLs is the creation of more than 1 image on the retina, creating an out-of-focus image or blur that may be perceived as halo or glare by the patient.4 Not all patients perceive these symptoms, but they can contribute to patient complaints. For patients desiring a high-quality full range of vision with potential for minimal contrast loss and visual disturbances, the TECNIS® Symfony Extended Range of Vision IOL (Package Insert TECNIS Symfony IOL; Abbott Medical Optics, Inc., Santa Ana, CA, USA) represents a new segment in presbyopia-correcting IOLs. Complementary technologies of the TECNIS Symfony IOL include an achromatic diffractive echelette optic designed to elongate the IOL focus, giving continuous vision from distance through intermediate and correct chromatic aberration. The approach of correcting chromatic aberration and spherical aberration has been shown to improve retinal image quality and maintain depth of focus.5 These features are intended to provide spectacle-free vision over a range of distances, and reduce chromatic aberration for better contrast vision, and decreased rate and intensity of glare and halos.
Combining MIOLs for a blended or contralateral approach has been a topic of interest. The selection of the add power of an MIOL can provide different visual advantages for near vs intermediate distance needs.6,7 In some studies, bilateral implantation with 2 different MIOL design concepts has been evaluated for potential visual and subjective benefits of combining technologies and shown promising results.8–10
The objective of the study was to evaluate the distance, intermediate, and near visual acuities (VAs), and assess spectacle independence and satisfaction in patients undergoing bilateral cataract extraction with implantation of a TECNIS Symfony IOL (ZXR00) in their dominant eye and a +3.25 D TECNIS MF 1-piece IOL (ZLB00) in their fellow eye.
Materials and methods
This study was a single-center, non-comparison, evaluator-masked clinical study. The first study patient was screened on 01/14/2016 and the last study visit occurred on 12/21/2016. Patients meeting eligibility criteria were enrolled consecutively. Fifty qualified study patients (100 eyes) received a TECNIS Symfony IOL (ZXR00) (Abbott Medical Optics, Inc., Santa Ana, CA, USA) in their dominant eye and a +3.25 D (ZLB00) TECNIS® MF 1-piece IOL (Abbott Medical Optics, Inc.) in their non-dominant eye. The study was approved by Veritas Institutional Review Board and was conducted in accordance with the principles outlined in the Declaration of Helsinki and Good Clinical Practice. All study participants provided written and informed consent.
Inclusion criteria of the study included adults older than 21 years at the time of the preoperative examination, in good general health with bilateral cataracts, who had clear lenses and desired spectacle independence, and for whom phacoemulsification extraction and a posterior multifocal IOL implantation were planned for both eyes. Participants had to be willing to have surgery on their second eye within 1–2 days of their first eye; be able to read, comprehend, and give informed consent; and comply with study instructions, agree to make all office appointments, and complete the entire course of the study. In addition, participants must have visual postoperative potential of 20/32 or better in each eye; a preoperative corneal astigmatism of ≤1.5 D in each eye; a postoperative astigmatism target of ≤0.5 D in each eye; clear ocular media; normal macula in each eye; and naturally dilated pupil sizes of ≥3.5 mm, in dim light, in each eye.
Exclusion criteria precluded enrollment of eyes with retinal, ocular, or systemic pathology that could affect VA; amblyopia or strabismus; capsular or zonular abnormalities affective IOL centration; pupil abnormalities or dilation <3.5 mm in dim light; evidence of Epithelial Basement Membrane Dystrophy on slit-lamp exam in either eye; keratoconus or significant irregular astigmatism on preoperative topography; history of ocular trauma; ocular or refractive surgery prior to or during the study; use of poly(methyl methacrylate) lenses within 6 months, gas permeable lenses within 1 month, or extended-wear or daily soft contact lens within 7 days of scheduled surgery; and concurrent or recent (within 30 days) participation in a drug or other investigational research study.
Study lenses
The IOLs used in this study were the TECNIS Symfony IOL (ZXR00) in the dominant eye and a +3.25 D (ZLB00) TECNIS MF 1-piece IOL in the non-dominant eye. Both models are posterior, 1-piece, soft-foldable acrylic, UV-absorbing, diffractive IOLs (Package Insert TECNIS Symfony IOL, Package Insert ZLB00 IOL; Abbott Medical Optics, Inc.). Both lenses also have a biconvex optic that incorporates a wavefront-designed aspheric optic to compensate for corneal spherical aberration, and both have a square posterior edge design with a frosted optic edge. The IOLs differ in the posterior optic design in that the ZXR00 IOL posterior optic includes an achromatic diffractive surface on the posterior optic to correct chromatic aberration and a unique echelette feature to extend the range of vision, including far, intermediate, and near, while maintaining the corneal spherical aberration compensation. This format creates an achromatic diffractive pattern that elongates a single focal point and compensates for the chromatic aberration of the cornea. In contrast, the ZLB00 IOL is a diffractive multifocal IOL with a +3.25 D add power that does not include the echelette feature, instead splitting light between multiple foci.
Treatment
Each study patient underwent the same routine cataract extraction procedure for each eye, with the second eye scheduled to undergo cataract extraction within 1 to 2 days after the first eye. All surgeries were performed by a single surgeon using the Stellaris Phaco System (Bausch and Lomb, Rochester, NY, USA). Study patients received a TECNIS Symfony IOL (ZXR00) in their dominant eye and a +3.25 D (ZLB00) TECNIS MF 1-piece IOL in their non-dominant eye. The dominant eye was determined using the hand triangle method focusing on a distant object binocularly and then determining which eye was actually focusing. All patients received the same open-label preoperative, operative, and postoperative medications over the course of the study period. Clear cornea incision was performed in all patients.
Study endpoints were assessed preoperatively, operatively, and postoperatively on Day 1, Day 7, Day 30, and Day 90. VAs were evaluated using logMAR charts at far (6 m), intermediate (66 cm), and near (40 cm) distances. Subjective outcomes for patient satisfaction, visual symptoms, and spectacle wear were assessed by subjective questionnaire administered postoperatively on Day 7, Day 30, and Day 90. Patient experience with photic phenomena (glare, halo, starburst, or other) was evaluated by asking respondents, “Over the last 7 days have you experienced any problems with your vision?” If yes, the symptom was specified and rated as mild, moderate, or severe.
Statistical analyses were calculated using JMP 10 (SAS Institute, Inc.). Paired t-test was used to calculate if any statistical differences existed between the IOL models. Statistical significance was set at 0.05.
Results
A total of 32 patients of 50 enrolled completed the 3-month visit. Five patients discontinued the study due to personal reasons (2), missed visits (2), or other (car accident), and 13 were excluded from analysis due to Nd:YAG (YAG) and/or enhancement (3 enhancements, 3 enhancements with YAG, and 7 YAG). Enhancements performed were photorefractive keratectomy (PRK) for remaining refractive error. The patients who required YAG were experiencing a decrease in VA and visual quality between the 1-month and 3-month visits; therefore, they were scheduled for the YAG. These patients were excluded from the analysis as vision was better at the 1-month visit and declined due to clouding of the capsule. At 90 days postoperatively, 32 of 45 patients completed the visit and underwent complete evaluations. Of the 32 patients, 53.1% (17/32) were male, 87.5% (28/32) were Caucasian, and the average age was 32 years (range 44–62). The right eye received the first implant for all patients and was the dominant eye in 68.8% (22/32) of patients. Eye dominance was able to be determined for all patients. Average pupil size in both IOL groups was approximately 4.0 mm at baseline and Day 90 postoperatively.
Visual acuities
At 90 days postoperatively, 97% of patients had a binocular uncorrected distance VA (UCDVA) of 20/20 or better (Figure 1). Mean logMAR UCDVA at 3 months postoperatively was −0.06±0.08 (n=30). For binocular uncorrected intermediate VA (UCIVA), 97% of patients had a VA of 20/25 or better (Figure 2). Mean logMAR UCIVA was 0.00±0.07 (n=30). For binocular uncorrected near VA (UCNVA), 94% of patients had a VA of 20/25 or better (Figure 3). Mean logMAR UCNVA was 0.05±0.08 (n=30). Patient-selected best near distance was 37.6±3.6 cm (n=30), and patient-selected best near VA averaged 20/22 (Snellen).
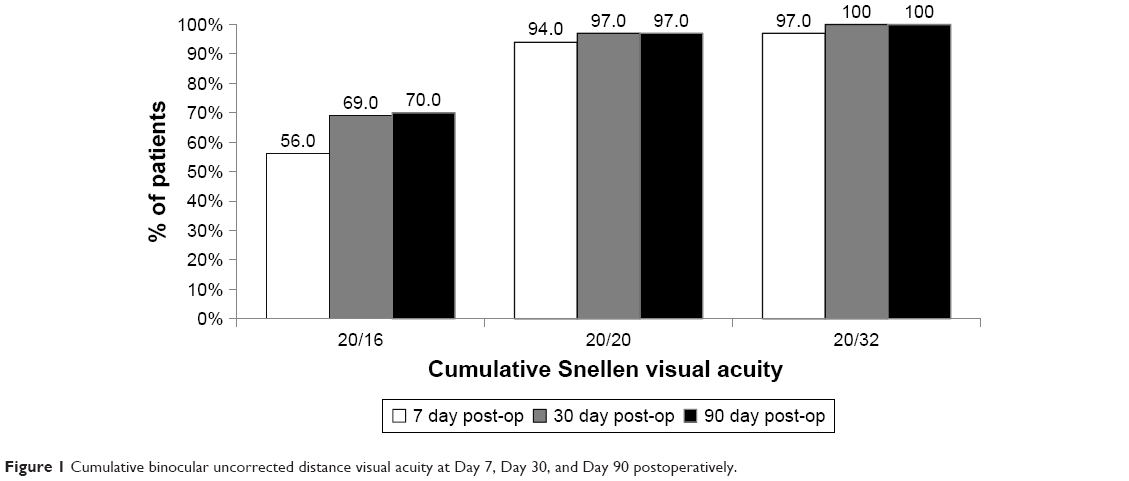 | Figure 1 Cumulative binocular uncorrected distance visual acuity at Day 7, Day 30, and Day 90 postoperatively. |
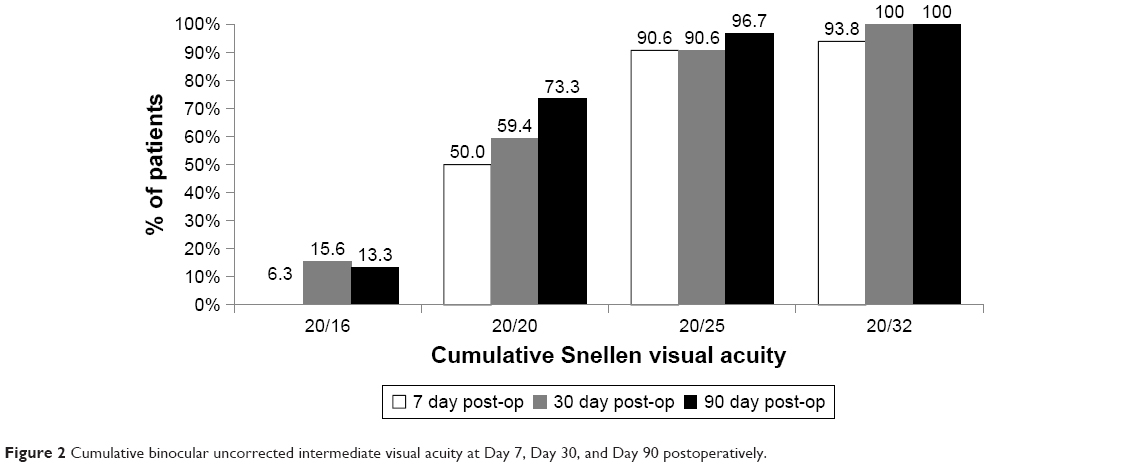 | Figure 2 Cumulative binocular uncorrected intermediate visual acuity at Day 7, Day 30, and Day 90 postoperatively. |
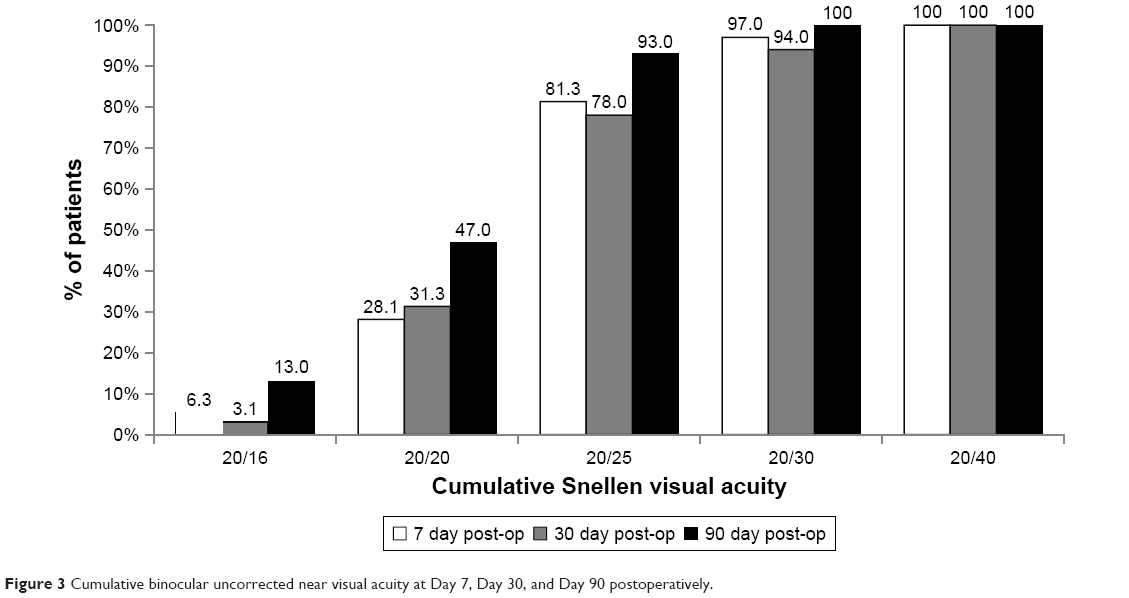 | Figure 3 Cumulative binocular uncorrected near visual acuity at Day 7, Day 30, and Day 90 postoperatively. |
Best-corrected visual acuity (binocular and monocular)
Mean monocular and binocular best-corrected logMAR visual acuities (BCVAs) are shown in Table 1. Monocular BCVA differed significantly between IOL groups (P<0.05). Differences in monocular VAs between the IOL groups ranged from 1 to 2.5 lines and were most notable at near distance. Binocular BCVA averaged 20/20 or better.
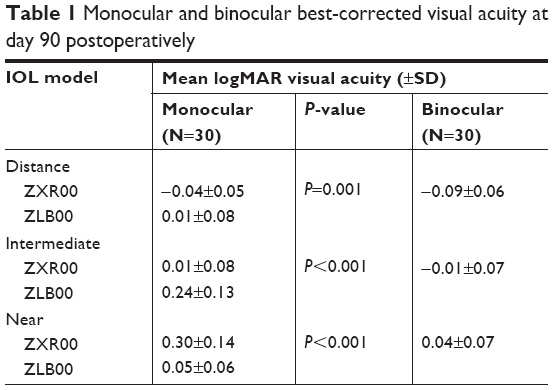 | Table 1 Monocular and binocular best-corrected visual acuity at day 90 postoperatively |
Refraction
Manifest refraction outcomes comparing baseline to Day 90 are shown in Table 2. The ZXR00 IOL group and the ZLB00 IOL group had statistically significant improvements in spherical equivalent from baseline to Day 90. There were no statistically significant differences for cylinder. Refraction was stable across visits (Figure 4).
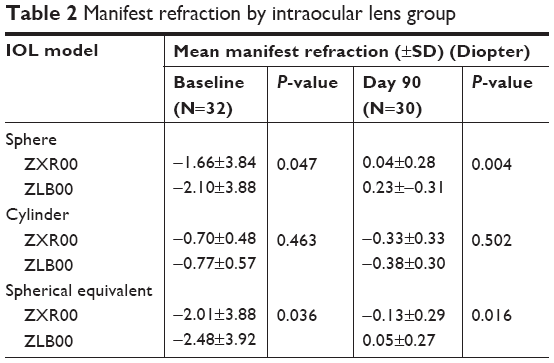 | Table 2 Manifest refraction by intraocular lens group |
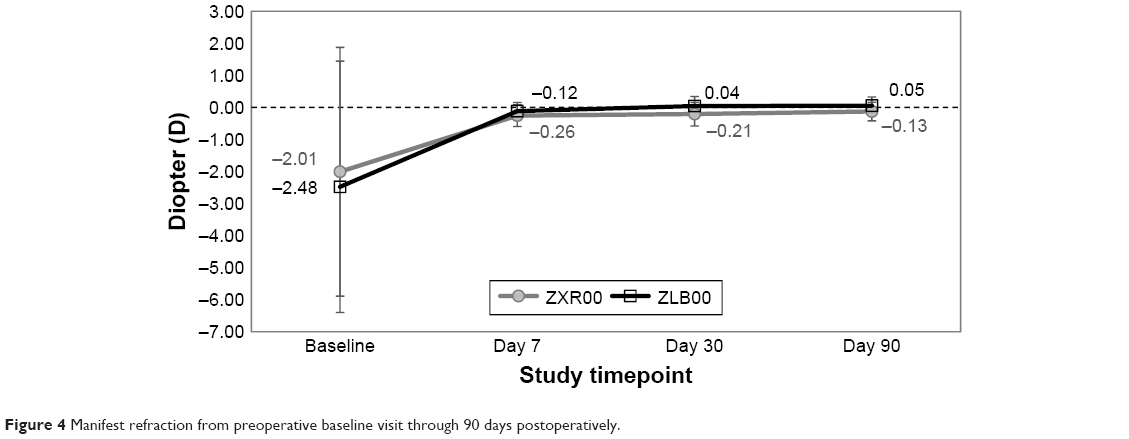 | Figure 4 Manifest refraction from preoperative baseline visit through 90 days postoperatively. |
Safety outcomes
All IOLs were placed within the capsular bag, and there were no surgical complications for any of the IOL implantations. There were no abnormal findings for slit lamp, OCT macula, corneal topography, intraocular pressure, or fundus exam. Two adverse events occurred during the course of the study (1 each in the ZXR00 IOL and ZLB00 IOL groups), both of which were due to postoperative increased intraocular pressure and resolved with medication.
Patient-reported outcomes
Patients completed a subjective questionnaire regarding visual symptoms at Day 7, Day 30, and Day 90 after the second eye surgery was completed. Most patients reported no visual symptoms or mild symptoms when queried about halos, glare, starburst, or other blur (Figure 5).
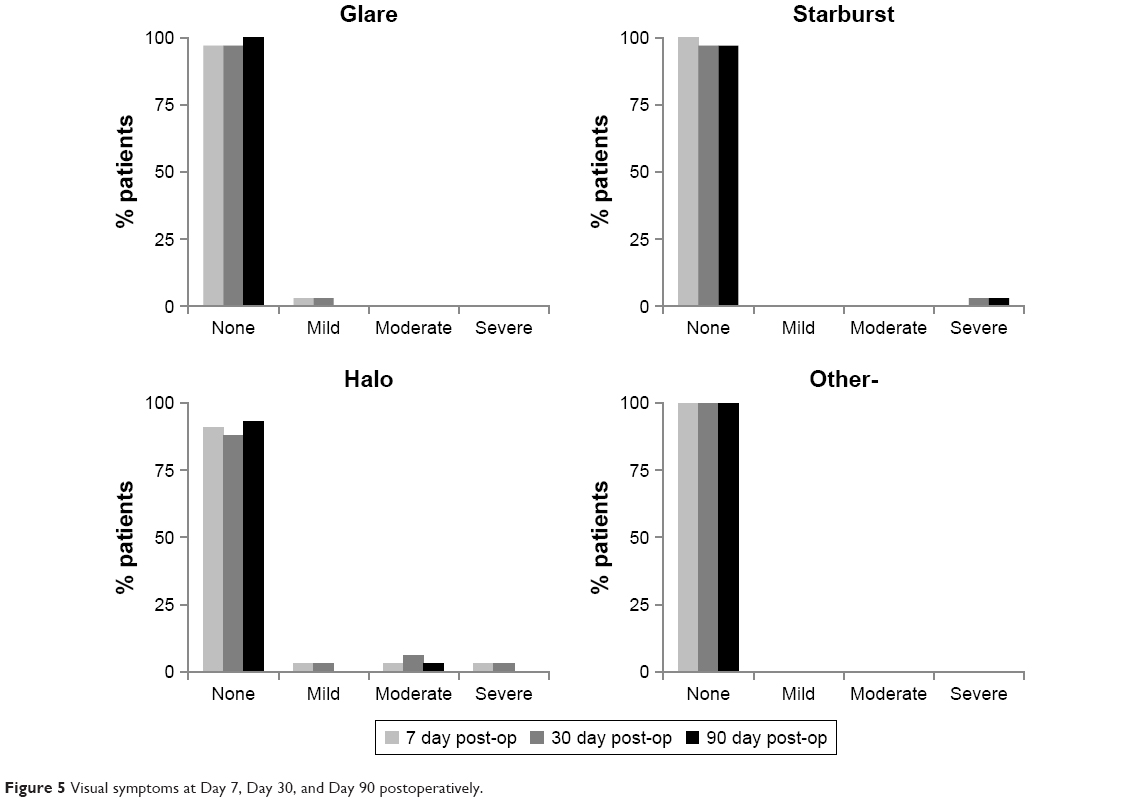 | Figure 5 Visual symptoms at Day 7, Day 30, and Day 90 postoperatively. |
Conclusion
Patient outcomes with the combined IOL technologies demonstrated excellent uncorrected and best-corrected binocular VAs at near, intermediate, and far distances. Minimal visual symptoms were reported by patients and satisfaction was high.
Findings from this study of the Symfony IOL were consistent with other published outcomes for the ZXR00 extended range of vision IOL. Other studies have also shown good VA from near to far distances, particularly in the far and intermediate ranges.8,11–14 Visual symptoms reported in other studies have also been minimal with the ZXR00 IOL, and patient satisfaction has been high.8,14,15 Additionally, reports for contrast sensitivity have been good with the extended range of focus multifocal technology.8,15 The unique echelette design, which elongates a single focus point, may be responsible for the relatively low visual symptoms observed in this study as compared with traditional multifocal IOLs with multiple focal points. In addition, the patients were well counseled preoperatively about the potential for visual symptoms, which may have influenced the perception of visual symptoms.
Postoperative outcomes reported for the ZLB00 low-add IOL have also shown good VAs at near and intermediate distances in the range of 20/25 Snellen or better, and patients reported satisfaction with the outcomes of the surgery.16 The same study found only few patients requiring postoperative use of spectacles for some daily activities, and they reported mild perception of halos. In another study, the ZLB00 had the best distance-corrected near VA among 5 different MIOLs.17
The contralateral or blended IOL approach has been studied with other multifocal and trifocal IOL technologies.1,9 Results have shown good outcomes for VA across a range of distances from near through far. In a study blending ZXR00 and ZLB00 MIOLs, results were consistent with the current study relative to UCDVA, BCVA, UCIVA, and UCNVA.1 In another study, a trifocal IOL was compared with blended bifocal IOLs with an intermediate add in the dominant eye and a near add in the nondominant eye.4 Both IOL groups had excellent binocular near and distance vision and intermediate VA was similar between groups at viewing distances from 60 to 40 cm, corresponding to computer or reading distance.4 Patients in both IOL groups also reported similar low rates of visual disturbances and good functional vision.4
Results from this study would benefit eye care practitioners who have patients seeking information about the use of combined or blended IOL technologies. Although this study included a non-randomized, modest sample size, these results describe outcomes from patients treated in a typical clinic setting, who underwent bilateral implantation with current MIOL technologies. The exclusion of patients with additional postoperative procedures (ND:Yag or PRK) should be noted, and future studies could include those patients as these types of procedures may be necessary after some IOL surgeries. Future studies could also evaluate contrast sensitivity with this blended technology approach, as well as long-term results beyond 3 months, particularly relative to satisfaction after neuroadaptation. In addition, subjective outcomes could be further explored using a validated questionnaire, as data from the non-validated subjective queries in this study showed promising outcomes. Future studies could evaluate other factors which might attribute to the low incidence of photic phenomenon with this IOL, such as good preoperative VAs or lack of medical or ocular conditions, and patient counseling. Another topic of interest would be later onset of dry eye in patients with cataracts, and potential effect of optimizing tear film before surgery on patient satisfaction.
In conclusion, this study of patients with combined IOL implantation of an increased depth of focus IOL (Symfony IOL) and a low-add IOL (TECNIS MF +3.25) demonstrated excellent uncorrected and corrected VAs from near through far distances, low dependence on glasses at all distances, and minimal or mild reports of visual symptoms at 3 months postoperatively.
Acknowledgments
This study was funded by an unrestricted grant from J&J Vision. Medical writing assistance was provided by Suzie Webster, BSN. Previously presented in part as a poster at the COS Annual Meeting (2017/Montreal).
Disclosure
Dr Sondra Black reports grants from AMO during the conduct of the study, as well as from Johnson & Johnson, Acufocus, Labtician, VGC, and from Shire, outside the submitted work. The author reports no other conflicts of interest in this work.
References
de Medeiros AL, de Araújo Rolim AG, Motta AFP, et al. Comparison of visual outcomes after bilateral implantation of a diffractive trifocal intraocular lens and blended implantation of an extended depth of focus intraocular lens with a diffractive bifocal intraocular lens. Clin Ophthalmol. 2017;11:1911–1916. | ||
Nuzzi R, Tridico F. Comparison of visual outcomes, spectacles dependence and patient satisfaction of multifocal and accommodative intraocular lenses: innovative perspectives for maximal refractive-oriented cataract surgery. BMC Ophthalmol. 2017;17(1):12. | ||
Crispim J, Nose R, Yogi M, Nose W. Refractive and visual outcomes of different intraocular lenses with femtosecond laser cataract surgery: the expectation of independence from spectacles. Open Ophthalmol J. 2015;9:145–148. | ||
Gundersen KG, Potvin R. Comparison of visual outcomes and subjective visual quality after bilateral implantation of a diffractive trifocal intraocular lens and blended implantation of apodized diffractive bifocal intraocular lenses. Clin Ophthalmol. 2016;10:805–811. | ||
Weeber HA, Piers PA. Theoretical performance of intraocular lenses correcting both spherical and chromatic aberration. J Refract Surg. 2012;28(1):48–52. | ||
Kim JS, Jung JW, Lee JM, Seo KY, Kim EK, Kim TI. Clinical outcomes following implantation of diffractive multifocal intraocular lenses with varying add powers. Am J Ophthalmol. 2015;160(4):702–709. | ||
Esteve-Taboada JJ, Domínguez-Vicent A, del Águila-Carrasco AJ, Ferrer-Blasco T, Montés-Micó R. Effect of large apertures on the optical quality of three multifocal lenses. J Refract Surg. 2015;31(10):666–676. | ||
Ruiz-Mesa R, Abengózar-Vela A, Aramburu A, Ruiz-Santos M. Comparison of visual outcomes after bilateral implantation of extended range of vision and trifocal intraocular lenses. Eur J Ophthalmol. 2017;27(4):460–465. | ||
Vilar C, Hida WT, de Medeiros AL, et al. Comparison between bilateral implantation of a trifocal intraocular lens and blended implantation of two bifocal intraocular lenses. Clin Ophthalmol. 2017;11:1393–1397. | ||
Mastropasqua R, Pedrotti E, Passilongo M, Parisi G, Marchesoni I, Marchini G. Long-term visual function and patient satisfaction after bilateral implantation and combination of two similar multifocal IOLs. J Refract Surg. 2015;31(5):308–314. | ||
Kaymak H, Höhn F, Breyer DR, et al. Functional Results 3 Months after Implantation of an “Extended Range of Vision” Intraocular Lens. Klin Monbl Augenheilkd. 2016;233(8):923–927. | ||
Pedrotti E, Bruni E, Bonacci E, Badalamenti R, Mastropasqua R, Marchini G. Comparative analysis of the clinical outcomes with a monofocal and an extended range of vision intraocular lens. J Refract Surg. 2016;32(7):436–442. | ||
Monaco G, Gari M, di Censo F, Poscia A, Ruggi G, Scialdone A. Visual performance after bilateral implantation of 2 new presbyopia-correcting intraocular lenses: Trifocal versus extended range of vision. J Cataract Refract Surg. 2017;43(6):737–747. | ||
Black S. Successful Restoration of Visual Acuity with an Extended Range of Vision Intraocular Lens after Multifocal Laser Ablation. Case Rep Ophthalmol. 2016;7(3):193–197. | ||
Cochener B, Group CS, Concerto Study Group. Clinical outcomes of a new extended range of vision intraocular lens: International Multicenter Concerto Study. J Cataract Refract Surg. 2016;42(9):1268–1275. | ||
Kretz FT, Koss MJ, Auffarth GU, ZLB00 Study Group. Intermediate and near visual acuity of an aspheric, bifocal, diffractive multifocal intraocular lens with +3.25 D near addition. J Refract Surg. 2015;31(5):295–299. | ||
Cardona G, Vega F, Gil MA, Varón C, Buil JA, Millán MS. Visual acuity and image quality in 5 diffractive intraocular lenses. Eur J Ophthalmol. 2018;28(1):36–41. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.