Back to Journals » Clinical Ophthalmology » Volume 9
A case of WAGR syndrome in association with developmental glaucoma requiring bilateral Baerveldt glaucoma implants and subsequent tube repositioning
Authors Akagi T ![]() , Yoshikawa M
, Yoshikawa M ![]() , Nakanishi H
, Nakanishi H ![]() , Yoshimura N
, Yoshimura N
Received 6 January 2015
Accepted for publication 11 February 2015
Published 15 June 2015 Volume 2015:9 Pages 1081—1084
DOI https://doi.org/10.2147/OPTH.S80444
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Tadamichi Akagi, Munemitsu Yoshikawa, Hideo Nakanishi, Nagahisa Yoshimura
Department of Ophthalmology and Visual Sciences, Kyoto University Graduate School of Medicine, Kyoto, Japan
Abstract: Glaucoma drainage device implantation is efficacious for the treatment of pediatric glaucoma patients when multiple angle surgeries fail. However, tube touching of the corneal endothelium is one of the major postoperative complications to deal with. A 15-month-old male patient with Wilms’ tumor, aniridia, genitourinary anomalies, and mental retardation (WAGR) syndrome was diagnosed with bilateral developmental glaucoma. He underwent Baerveldt glaucoma implant (BGI) surgeries in both eyes after multiple failed trabeculotomies. The tube in his right eye was touching the cornea 15 months after BGI surgery. To avoid corneal endothelium damage, BGI tube repositioning with scleral fixation was performed without serious complications. The bilateral BGI surgeries achieved successful intraocular pressure reduction for over 2 years and tube repositioning with scleral fixation of BGI tube was successful for BGI tube malposition. Although careful attention to intraocular pressure and tube malposition is essential after glaucoma drainage device implantation, especially in pediatric cases, BGI surgery is effective in the management of developmental glaucoma following unsuccessful angle surgeries.
Keywords: Baerveldt glaucoma implant, developmental glaucoma, WAGR syndrome, tube repositioning, glaucoma drainage device
Introduction
In eyes with developmental glaucoma, surgical therapies such as trabeculotomy or goniotomy are usually essential to control intraocular pressure (IOP). Although these angle surgeries have high success rates in primary developmental glaucoma,1,2 secondary developmental glaucoma, with associated ocular/systemic anomalies, including aniridia, has a poor prognosis, probably because of maldevelopment of the angle structures and Schlemm’s canal.1,2 Wilms’ tumor, aniridia, genitourinary anomalies, and mental retardation (WAGR) syndrome is caused by heterozygous contiguous gene deletions that involve at least PAX6 and Wt1, which has a risk of a developmental glaucoma.3
Even when the first trabeculotomy is unsuccessful, a subsequent trabeculotomy may be effective in lowering IOP.1 However, when multiple angle surgeries fail, further surgical procedures such as trabeculectomy with mitomycin-C, cyclodestructive surgery, and glaucoma drainage device (GDD) implantation are needed.2,4 Trabeculectomy in younger children has many problems: a rapid healing response, postoperative bleb management, and a high rate of bleb-associated endophthalmitis.2 Cyclodestructive procedures require multiple retreatments and have a possible risk for a serious complication, phthisis bulbi. It has been reported that the success rate is significantly higher after Ahmed glaucoma valve or Baerveldt glaucoma implant (BGI) (87%) versus trabeculectomy with mitomycin-C (36%) in children.4 GDD implantation, such as BGI, is suggested as the most predictable and possibly the safest procedure after failed angle surgery.
Here, we report a case of WAGR syndrome in association with developmental glaucoma requiring bilateral BGIs and subsequent tube repositioning. This is the first report of tube repositioning with scleral fixation of BGI tube in a pediatric case.
Case report
A 15-month-old male patient was referred to Kyoto University Hospital. He was diagnosed with bilateral (OU) aniridia and developmental glaucoma in his right eye (OD) at 1 month of age and subsequently with WAGR syndrome. He had undergone three OD trabeculotomies before 1 year of age. At the initial visit to our hospital, he was using three types of glaucoma eyedrops; his IOP was 11 mmHg OD and 24 mmHg in the left eye (OS). Fundus examination showed macular hypoplasia OU; a tilted disc with 0.9 cup to disc ratio OD; and an oval disc with 0.6 cup to disc ratio OS. Figure 1 and 2 show pre- and postoperative photographs and IOP throughout the follow-up period, respectively. Briefly, after three failed OD and two failed OS trabeculotomies, BGI surgeries were performed in both eyes.
 | Figure 1 Pre- and postoperative photographs. |
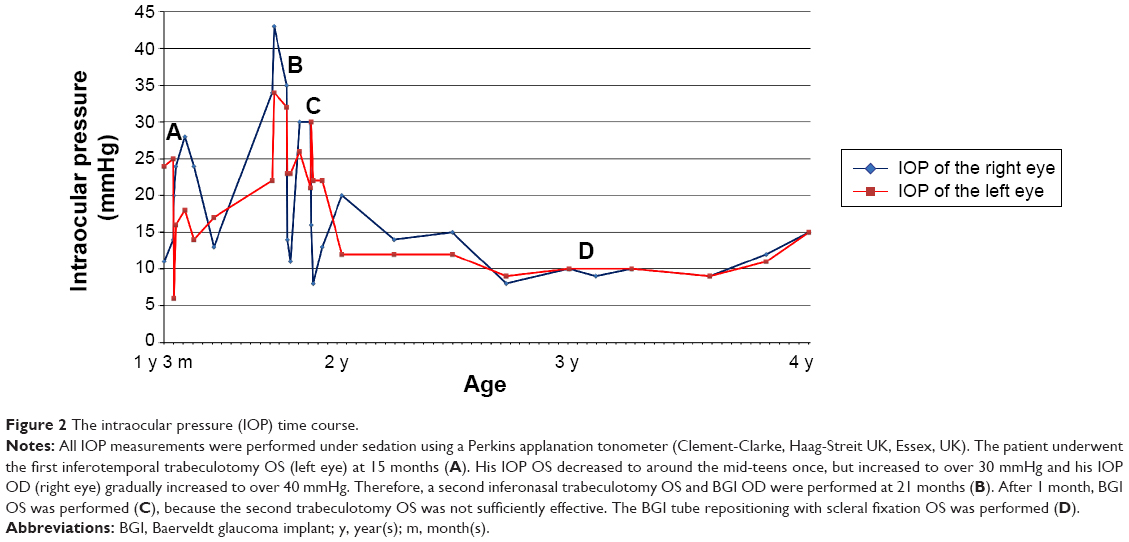 | Figure 2 The intraocular pressure (IOP) time course. |
A BGI103-250 implant was placed in the superior temporal quadrant with a fornix based conjunctival flap (Figure 1A–D). The plate was secured with 9-0 nylon sutures 9 mm posterior to the limbus. The tube was ligated with 7-0 Vicryl and was slit to manage the transient hypertensive phase. The tube was placed at a level intermediate between the cornea and the lens, because both tube-cornea and tube-lens touch should be prevented. Preserved donor sclera was used to cover the tube.
The IOPs (OU) became stable 2–3 months after the surgeries (Figure 2) and the optic disc findings improved (Figure 1E and F). The tube positions OU were at the level intermediate between the cornea and the lens until 1 year postoperative. The OD tube was touching the cornea 15 months after BGI surgery (Figure 1G and H). To avoid corneal endothelium damage, BGI tube repositioning with scleral fixation was performed as previously described.5 Briefly, a conjunctival incision and triangular-shaped scleral flap were made at the inferior temporal area (Figure 1I and J, green arrows). The end of the tube was pulled out through the corneal side port punctured immediately above the tube using capsulorhexis forceps (Figure 1I and J). A double-armed 10-0 Prolene straight needle bent using two needle-holders penetrated through the tube end and pulled under the scleral flap using the 27-gauge leading needle (Figure 1K). The second needle with a 10-0 Prolene was also pulled under the scleral flap and the tube end was extended parallel to the corneal surface (Figure 1L and M). The scleral flap was sutured with a 10-0 nylon suture and the incised conjunctiva was closed with 8-0 Vicryl sutures. After the procedure, the patient maintained good tube positioning OD and good IOP without serious complications (Figure 1N and P). The tube OS has not shown tube touching of the corneal endothelium without tube repositioning so far (Figure 1O and Q).
Discussion
Tube positioning in the anterior chamber is especially important in pediatric cases due to the growth of the eyeball. Because tube retraction is a possible postoperative complication in pediatric GDD surgeries, we left a longer tube in the anterior chamber than in adults (Figure 1C and D). Tube touching of the corneal endothelium is another postoperative complication. Beck et al4 reported that tube repositioning was needed in 34.8% of 46 GDD-implanted pediatric eyes. Cutting the tube end or repositioning through a new scleral pathway is a possible choice. However, cutting the tube would be palliative, because it would not change the tube insertion angle. Reopening the conjunctiva and sclera for removal and tube reinsertion through a new pathway might cause insufficient wound closure and disturb the function of the BGI. Our choice was a novel technique of repositioning the tube with scleral fixation, which Ma et al5 reported in adult patients.
The bilateral BGI surgeries achieved successful IOP reduction for over 2 years. This is the first report of tube repositioning with scleral fixation of BGI tube in a pediatric case. This procedure was good for BGI tube malposition even in a pediatric case, at least for a short period. Although careful attention to IOP and tube malposition is essential after GDD implantation, especially in pediatric cases, BGI surgery is effective in the management of developmental glaucoma following unsuccessful angle surgeries.
Disclosure
The authors report no conflicts of interest in this work.
References
Ikeda H, Ishigooka H, Muto T, Tanihara H, Nagata M. Long-term outcome of trabeculotomy for the treatment of developmental glaucoma. Arch Ophthalmol. 2004;122(8):1122–1128. | ||
Ou Y, Caprioli J. Surgical management of pediatric glaucoma. Dev Ophthalmol. 2012;50:157–172. | ||
Han JC, Liu QR, Jones M, et al. Brain-derived neurotrophic factor and obesity in the WAGR syndrome. N Engl J Med. 2008;359(9):918–927. | ||
Beck AD, Freedman S, Kammer J, Jin J. Aqueous shunt devices compared with trabeculectomy with Mitomycin-C for children in the first two years of life. Am J Ophthalmol. 2003;136(6):994–1000. | ||
Ma KT, Kim JH, Seong GJ, Jang DS, Kim CY. Scleral fixation of Ahmed glaucoma valve tube tip for adjustment of cornea-touching malposition. Eye (Lond). 2014;28(1):23–25. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.