")
Back to Journals » Medical Devices: Evidence and Research » Volume 17
Value and Limitations of Urethrotech Catheterisation Device to Manage Difficult Urethral Catheterisation in Male Spinal Cord Injury Patients
Authors Subramanian V , Soni BM
Received 16 February 2024
Accepted for publication 8 April 2024
Published 16 April 2024 Volume 2024:17 Pages 143—150
DOI https://doi.org/10.2147/MDER.S457784
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Vaidyanathan Subramanian, Bakulesh Madhusudan Soni
Northwest Regional Spinal Injuries Centre, Southport and Formby District General Hospital, Southport, UK
Correspondence: Vaidyanathan Subramanian, Email [email protected]
Methods: We used a Urethrotech catheterisation device in 57 male patients with spinal cord injury, in whom urethral catheterisation was unsuccessful or previous catheterisation was difficult.
Results: Urethrotech catheter could be inserted in 51 patients. No patient developed urinary tract infection. In one patient, the guidewire could not be introduced into the bladder, and a coude Foley catheter was inserted. In two patients, the guidewire was inserted into the bladder, but a 16 CH catheter could not be advanced over the guidewire. Emergency suprapubic cystostomy was performed in one case; in the other, urethral stricture was dilated; a size 12 CH catheter was inserted. In three patients, the guidewire curled back into the urethra because of severe spasm of the urethral sphincter. Catheterisation with a Tiemann catheter was successful after administration of diazepam and/or stretching of the anal sphincter by another health professional, which caused reflex relaxation of the urethral sphincter. Complications of Urethrotech catheterisation included urethral bleeding, haematuria, pain, doubling back of the guidewire due to spasm of the urethral sphincter or from an empty bladder. We adopted variations in technique, eg filling the bladder with saline prior to catheterisation when feasible, insertion of the guidewire by the side of the old catheter, use of Tiemann tip catheters, administration of antibiotics, diazepam to control spasms, nifedipine to control autonomic dysreflexia, analgesics, stretching of the anal sphincter to induce reflex relaxation of the urethral sphincter, urgent imaging studies to confirm correct positioning of the catheter, omitting anticoagulants and monitoring patients, who developed bleeding.
Conclusion: Use of Urethrotech in spinal injury patients warranted adaptations to the technique, which required expertise, experience, and backup facilities. To ensure patient safety, Urethrotech catheter should be used in a hospital setting, and by medical personnel with experience in the management of spinal cord injury patients.
Keywords: urethral catheterisation, male, patient, urinary bladder, urethral sphincter, paraplegia, patient safety
Introduction
What is Urethrotech Catheterisation Device?
Urethrotech male urethral catheterisation comprises a flexible hydrophilic Nitinol guidewire, which protrudes 50 cm from the tip of a standard 5.3 mm diameter 3-way Foley catheter (Figure 1). The soft tip of the guidewire was lubricated with sterile water before insertion. The soft tip is designed to avoid urethral trauma and return if the wire is pushed against an obstruction or a non-negotiable false passage. When the guidewire enters the bladder, it should curl up as the catheter advances. The catheter was passed over the guidewire when it reached the tip of the penis. When the catheter enters the bladder, the balloon is inflated, and the guidewire is withdrawn and disposed.1
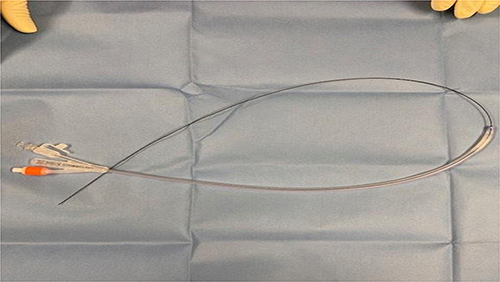 |
Figure 1 Photograph of the Urethrotech catheterisation device showing 100% silicone three-way Foley catheter 16 CH with an integrated Nitinol guidewire. |
What is Known Already?
Bugeja et al2 studied 100 consecutive male patients (mean age 67.2 years) who were routinely catheterised using the Urethrotech catheterisation device. These patients underwent cardiac surgery at a single cardiothoracic centre. Catheterisation was performed after patients were anaesthetised in the theatre. All 100 patients underwent an uneventful catheterisation during the first pass. None of the patients experienced any adverse events during the catheterisation procedure or the postoperative period. It should be noted that these patients did not have a history of difficult catheterisation; catheterisation with a standard Foley catheter was not attempted before using the Urethrotech device. Therefore, these anaesthetised patients do not represent patients with “difficult urethral catheterisation”. Dragova et al3 used a Urethrotech catheterisation device in 13 men who could not be recatheterized for the first pass with a standard Foley catheter. The nurses found the Urethrotech catheterisation device easy and successful in all 13 men and no adverse events were recorded. Fluckiger and Hubert4 used a Urethrotech catheterisation device in 21 men after a failed standard Foley catheterisation. Catheterisation failed with the Urethrotech device in 4 of the 21 men. Three of the 21 patients reported discomfort during catheterisation using the Urethrotech device.
Are there Differences in Urethral Catheterisation Between Able-Bodied Individual and Spinal Cord Injury Persons?
Urethral catheterisation may be difficult in patients with spinal cord injury due to spasm of the urethral sphincter, altered anatomy of the urethra because of previous traumatic catheterisation leading to false passages in the urethra, or previous surgery such as sphincterotomy or bladder neck resection. Moreover, these patients may lack sensation in the urethra or experience hypersensitivity. Patients with spinal cord injury above the T-6 level are at risk of developing autonomic dysreflexia. These patients may have inflamed urethral and bladder mucosa owing to bacterial colonisation and repeated episodes of urinary tract infection. Thus, the spinal cord injury patient population is quite different from that of able-bodied men with intact urethral sensation.
Gap in Knowledge
The urethral catheterisation device has not been evaluated in managing difficult urethral catheterisation in patients with spinal cord injury and neuropathic bladder. We mentioned the possible use of Urethrotech catheterisation device in a case report on urethral perforation due to catheterisation in the discussion section of the case report.5 Herein, we focus on the problems we faced in 57 cases, and the changes we made to the technique of using the Urethrotech catheterisation device to meet the needs of the individual patient. This is the first publication to discuss the limitations of the Urethrotech catheterisation device and the need to vary the technique of using the Urethrotech catheterisation device after careful assessment of the individual patient’s circumstances.
Methodology
We used a Urethrotech catheterisation device in male patients with spinal cord injuries in a regional spinal cord injury centre. We formulated an audit on the use of a Urethrotech catheterisation device in spinal cord injury patients.
The inclusion criteria were:
- Male persons with spinal cord injury
- Age above 18 years
- Routine urethral catheterisation was unsuccessful.
- Patients in whom the previous urethral catheterisation was difficult and required several attempts.
- The patient is capable of, and willing to, provide verbal consent for the use of a Urethrotech catheterisation device after detailed discussion.
The clinical audit proposal was submitted to the audit committee of the Northwest Regional Spinal Injuries Centre, Southport, United Kingdom. We applied to the New Interventional Procedures, Techniques and Advancing Practice Committee of the Southport and Ormskirk Hospital NHS Trust for approval to use the Urethrotech catheterisation device. Both committees approved the proposal for a clinical audit. The Urethrotech catheterisationn device was used within the Northwest Regional Spinal Injuries Centre, District General Hospital, Southport, Mersey and West Lancashire Teaching Hospitals NHS Trust, United Kingdom, for consecutive patients over a 19-month period.
The Urethrotech catheterisation device was shown to the patients, and the authors discussed how the catheter with the guidewire was inserted into the bladder, the potential benefit of using this device and the shortcomings, including the risk of bleeding, pain, and urinary tract infection. Following the discussion, patients provided verbal informed consent for the use of the Urethrotech catheterisation device. No patient declined to the use of the Urethrotech catheterisation device. Verbal informed consent for the procedure was acceptable to and approved by the audit committee.
Catheterisation was performed by a designated doctor who had undergone training in the use of the Urethrotech catheterisation device. One tube of Instillagel gel (6 mL) was administered intra-urethrally before inserting the guidewire. Amikacin 500 mg was administered to all patients before the use of the Urethrotech catheterisation device. Amikacin was selected because there was an outbreak of gentamicin-resistant Klebsiella infection in the spinal unit. Our policy was to administer a single dose of antibiotic in patients in whom urethral catheterisation was difficult. Nifedipine 5 mg was administered to any patient who developed symptoms of autonomic dysreflexia, eg sweating or headache. Pennine Healthcare (300 City Gate, London Road. Derby DE24 8WY, United Kingdom) provided fifteen catheters free of cost to enable us to start the audit. Subsequently, Southport and Ormskirk Hospital NHS Trust and later, Mersey and West Lancashire Teaching Hospitals NHS Trust purchased the Urethrotech catheterisation device through the NHS Supply Chain. The current price of an Urethrotech Catheterisation device is £252.66.
The procedure was evaluated by documenting whether (i) the Urethrotech catheterisation device could be inserted into the urinary bladder or not; (ii) if it was not possible to insert the Urethrotech catheterisation device, what was done; (iii) complications if any; (iv) variations to the standard technique of using the Urethrotech catheterisation device.
Results
The Urethrotech catheterisation device was used in fifty-seven cases in the spinal cord injuries centre. Urethrotech catheters could be inserted in 51 patients. None of the patients developed sepsis or urinary tract infections following catheterisation using a Urethrotech catheter. Four patients required Nifedipine 5 mg sublingually to control autonomic dysreflexia.
In one patient, with a history of periurethral abscess and false passage, the guidewire could not be introduced into the urinary bladder; a coude Foley catheter was inserted eventually after several attempts. Soon afterwards, this patient underwent suprapubic cystostomy as a planned procedure. In two patients, the guidewire was inserted into the bladder, but the size 16 CH catheter could not be advanced over the guidewire. An emergency suprapubic cystostomy was performed in one patient. In the other case, urethral stricture was dilated; a size 12 CH silicone Foley catheter was inserted. In three patients in whom routine urethral catheterisation was unsuccessful, catheterisation was done using a Urethrotech device. The guidewire curled back into the urethra because of a severe spasm of the urethral sphincter and could not be inserted into the urinary bladder. Catheterisation with a Tiemann tip catheter was successful after administration of diazepam and stretching of the anal sphincter, which caused reflex relaxation of the urethral sphincter.
We encountered the following clinical problems while using the Urethotech catheterisation device.
In two patients, the guidewire curled back and entered the drainage channel of the Urethrotech three-way Foley catheter. In the first patient, we did not know what had happened. When we attempted to withdraw the guidewire, there was resistance. The balloon of Urethrotech catheter was deflated, and the catheter was withdrawn. We noticed that the guidewire had entered the main lumen of the catheter. Slight bleeding from the urethra was also observed. Subsequently, we inserted a new Urethrotech catheterisation device. Figures 2 and 3 depict what had happened: the tip of the guidewire could be seen entering the main drainage channel of the three-way Foley catheter. In the second case, we introduced a guidewire and advanced the catheter. Surprisingly, we observed a guidewire within the lumen of the catheter drainage channel. The catheter was removed. After withdrawing the catheter and guidewire, which had been doubled back into the main drainage channel of the three-way Foley catheter, a new Urethrotech catheterisation device was inserted.
 |
Figure 2 Photograph of the Urethrotech catheterisation device showing the tip of the guidewire entering the main drainage channel of the three-way Foley catheter. |
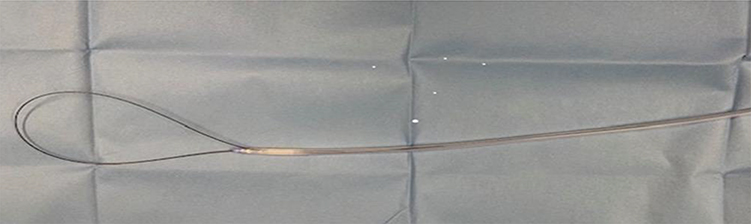 |
Figure 3 A photograph of the Urethrotech catheterisation device showing the guidewire, which had doubled back and entered the main drainage channel of the three-way Foley catheter. |
In three patients, the guidewire doubled back and reemerged from the urethral meatus. Instillagel was instilled into the urethra. The anal sphincter was stretched to cause reflex relaxation of the urethral sphincter. The guidewire can then be inserted through the urethral sphincter. The following case illustrates the value of using a Urethrotech catheterisation device along with intramuscular diazepam and stretching of anal sphincter to achieve urethral catheterisation without causing trauma in patients with spasm of the urethral sphincter.
A 59-year-old male person had sustained a cervical spinal cord injury (C-5, ASIA-D) while playing football. He was a very anxious person. Routine catheterisation was very difficult and resulted in urethral bleeding. Therefore, the Urethrotech device was used. When the guidewire was inserted into the urethra, it did not pass through the sphincter because of severe spasm; the guidewire doubled back and re-emerged from the urethral meatus. Instillagel was inserted into the urethra. Five milligrams of diazepam were given intramuscularly. Subsequently, a nurse introduced a finger into the rectum and stretched the anal sphincter. The guidewire was inserted into the urethra, followed by a 16 CH Urethrotech catheter. There was no bleeding from the urethral meatus, the urine was clear, and there was no bypassing of urine.
A spinal cord injury patient with a history of difficult catheterisation required a change of catheter after six weeks. The bladder was filled with sterile saline before the removal of the old catheter. A Urethrotech catheterisation device was then inserted. Filling the bladder with saline reduces the risk of the guidewire doubling back into the urethra, which is likely to happen in the case of an empty and collapsed bladder.
In a 59-year-old male with tetraplegia with grossly altered anatomy of the urethra due to previous surgery and false passages, and a history of very difficult urethral catheterisation, required changing of the urethral catheter. A guidewire was inserted into the bladder on the side of the existing catheter. Then, the old catheter was removed. The Urethrotech catheter was advanced over the guidewire and successfully inserted into the bladder.
Bleeding occurred following catheterisation with a Urethrotech catheter in four patients who were on anticoagulants; these patients required close monitoring for 24–48 hours. A patient, who was getting Enoxaparin for prophylaxis of venous thromboembolism, passed blood clots per urethra after he had undergone catheterisation with a Urethrotech catheterisation device. Enoxaparin was omitted for 24 hours; bleeding per urethra subsided.
In a patient with tetraplegia who developed haematuria, routine urethral catheterisation was unsuccessful. A Urethrotech catheterisation device was successfully inserted. The catheter drained blood-stained urine, but irrigation was not possible through the size 16 CH catheter. The Urethrotech catheter was removed; flexible cystoscopy was done; a size 20 CH three-way Foley catheter was inserted; continuous bladder irrigation was done.
Three patients with incomplete spinal cord injury who underwent catheterisation using a Urethrotech urethral catheterisation device experienced severe pain when the guidewire was inserted into the bladder. One patient required systemic analgesic. Despite the use of Instillagel, one patient experienced severe, intolerable pain in the lower abdomen and was unhappy with the urethral catheterisation device.
A patient with T-9 complete paraplegia developed a severe abdominal spasm following insertion of a Urethrotech catheter. An urgent ultrasound scan of the urinary bladder confirmed positioning of the catheter within the bladder and ruled out perforation, misplacement of the catheter tip in the ureter, or a Foley balloon in the prostatic urethra.
Discussion
The Urethrotech catheterisation device is useful to overcome difficult urethral catheterisation. However, major clinical issues may be encountered while using the Urethrotech catheterisation device in spinal cord injury patients. These clinical problems are discussed in detail below.
Bleeding
Some patients with spinal cord injuries, especially those with indwelling urethral catheters, are likely to have a chronically inflamed bladder and urethral mucosa. The guidewire, as it coils inside the urinary bladder, or as it traverses a tight urethral sphincter, may cause bleeding from the inflamed mucosa, particularly in patients receiving anticoagulants, either for prophylaxis of venous thromboembolism or for coexisting cardiovascular diseases. Patients may pass blood-stained urine or blood clots from the urethra coming around the catheter following catheterisation with a Urethrotech catheterisation device. If the bleeding is significant, the anticoagulant may have to be omitted for 24–48 hours until the bleeding subsides. Doctors should discuss this potential complication with the patients and carers before using the Urethrotech urethral catheterisation device.
Pain or Discomfort During Catheterisation
Patients with spinal cord injuries or incomplete lesions may also experience hypersensitivity. When the full-length guidewire is introduced or as guidewire coils inside the bladder, these patients may experience excruciating pain in the urinary bladder. The severity of pain felt by these patients when the Urethrotech catheterisation device was used, exceeded the pain or discomfort experienced by such patients during catheterisation with a standard Foley catheter. The instillation of a local anaesthetic drug, 2% lidocaine, and administration of an analgesic by intramuscular or oral route may help to reduce the pain.
Blockage of the Catheter with Blood Clots
Urethrotech catheterisation devices may be used in patients with haematuria in whom urethral catheterisation is difficult. The Urethrotech catheterisation device consists of only a 16 CH catheter, which is likely to get blocked with clots. Perhaps, a size 20 CH or 22 CH Urethrotech catheter can be developed for use in patients with haematuria in whom a size 16 CH catheter is likely to be blocked with clots.
Spasm of the Urethral Sphincter
In a patient with spinal cord injury in whom routine catheterisation was unsuccessful because of severe spasm of the urethral sphincter, diazepam, 5 mg, intramuscularly should be administered before attempting urethral catheterisation with a Urethrotech device. In addition to intramuscular diazepam or as an alternative, a finger may be introduced into the rectum, and the anal sphincter may be stretched. This leads to reflex relaxation of the urethral sphincter and facilitates urethral catheterisation using the Urethrotech device. Intramuscular diazepam together with the manoeuvre of stretching of the anal sphincter helps to achieve relaxation of urethral sphincter and thereby enable successful urethral catheterisation with a Urethrotech device, without causing urethral trauma.
We developed the following techniques that helped us insert the Urethrotech catheterisation device in challenging situations.
Change of Urethral Catheter in Patients with History of Difficult Catheterisation
Patients in whom a Urethrotech device is inserted because of difficult urethral catheterisation may experience problems while changing the catheter. We found that insertion of the guidewire of a new Urethrotech catheterisation device by the side of the existing catheter ensured successful introduction of the guidewire into the bladder. After inserting the guidewire, the old catheter can be removed, and a new Urethrotech catheter is advanced over the guidewire. This technique ensured a fail-safe method of inserting a catheter into the bladder in selected patients with grossly altered anatomy of the urethra.
Patients with an Empty Bladder During Catheterisation with Urethrotech Catheterisation Device
In patients with a small or empty bladder, the guidewire, after entering the bladder, may curve and enter the internal urethral meatus and protrude into the urethra to varying extents. Based on our previous experience, we learned how to detect whether the guidewire had doubled back into the urethra. There will be resistance to insertion of the catheter over the guidewire. The procedure should be stopped even if there is minimal resistance to advancement of the catheter over the guidewire. In such a situation, the catheter and the guidewire should be withdrawn, and the clinical situation reassessed.
When a guidewire is introduced into an empty, collapsed bladder, there is no space for the guidewire to coil around. Then, the guidewire is likely to cause trauma to the bladder mucosa and later bleeding. Efforts should be made to fill the bladder with sterile saline prior to introducing the guidewire, or the patient is asked to drink fluids whenever possible to fill the bladder naturally with urine. We instil about 150–200 mL of sterile, 0.9% sodium chloride solution before removing the old catheter. However, filling the bladder with sterile saline will be impossible if the old catheter has been removed. Vigilance should be observed while introducing the guidewire and subsequently, the catheter in patients with an empty or collapsed urinary bladder. Any slight resistance to the introduction of a guidewire or catheter should alert the doctor who is performing the catheterisation.
We modified our practice and preferred to fill the bladder with sterile saline whenever possible before inserting the guidewire of the Urethrotech device. If a patient has urine retention, the bladder is already distended, and the full bladder will accommodate the guidewire. If the bladder is empty, we considered whether it is feasible to encourage the patient to drink fluid so that the bladder becomes reasonably full.
We did not observe the following adverse event, but it could potentially occur when using the Urethrotech catheterisation device.
Guidewire Inserted into the Ureteric Orifice
On odd occasions, the guidewire may enter the ureteric orifice. This is likely to occur in patients with vesicoureteral reflux in whom the ureteric orifice may be gaping and wide open. When a Foley catheter is inserted into the bladder, it may also enter the ureter following the guidewire. A small amount of urine may have been drained through the catheter. When sterile saline is flushed through the catheter, there will be resistance to the injection of saline through the catheter. Subsequently, when the fluid is aspirated, there will be no free flow of urine. These observations should ring alarm bells, and the doctor should withdraw the catheter and the guidewire.
Potential Benefit of Ultrasound Monitoring During Catheterisation
The guidewire may be introduced into the bladder under ultrasound monitoring of the urinary bladder if facilities are available. Point-of-care ultrasound (POCUS) may be a valuable tool for monitoring guidewires and catheter insertion.
Summary of Our Experience with Urethrotech Catheterisation Device in Spinal Cord Injury Patients
Difficult urethral catheterisations in male patients with spinal cord injuries and neuropathic bladders were overcome using a Urethrotech catheter in 51 of 57 cases. The Urethrotech catheterisation device is useful in managing difficult urethral catheterisation in spinal cord injury patients despite its high cost (£252.66 per device). However, the use of a Urethrotech catheterisation device requires careful assessment and planning to meet the needs of individual patients. We adopted variations in techniques, such as filling the bladder with saline prior to catheterisation when feasible, insertion of the guidewire by the side of the old catheter, use of Tiemann tip catheters, administration of antibiotics, diazepam to control spasms, nifedipine to prevent or control autonomic dysreflexia, analgesics, stretching of the anal sphincter (by another health professional) which induces reflex relaxation of the urethral sphincter, urgent imaging studies to confirm correct positioning of the catheter, omitting anticoagulants in patients who developed urethral bleeding or haematuria, and monitoring these patients for 24–48 hours. Carrying out a wide number of variations to the technique requires expertise, experience, and backup facilities. To ensure patient safety, we are weary of using the Urethrotech catheter in patients with spinal cord injuries in settings other than a spinal injury centre or an acute hospital and only by medical personnel with experience in the management of spinal cord injury patients with complex needs.
We feel that a boxed warning should be printed on the Urethrotech catheterisation device to alert the health professionals about the potential risk of trauma to the bladder, bleeding and risk of guidewire doubling back and re-entering the urethra, when the guidewire is introduced to its full length in an empty, collapsed urinary bladder.
Data Sharing Statement
All relevant data are provided in the manuscript. Details of individual patients, such as name, date of birth, and NHS number, were removed to maintain confidentiality.
Ethical Statement
The Research, Development, and Innovation Advisory Group incorporating New Interventional Procedures, Techniques, and Advancing Practice Committee of Southport and Ormskirk NHS Trust, Southport, UK, approved the use of the Urethrotech catheterisation device. This audit is registered in the 2023-24 Forward Plan under ID number 23-162 of Mersey and West Lancashire Teaching Hospitals NHS Trust. The clinical audit ‘Use of Urethrotech in difficult urethral catheterisation of male spinal cord injury patients’ was approved by the Clinical Lead of the Audit and Research Committee of the Northwest Regional Spinal Injuries Centre, and then by the Clinical Audit and Effectiveness Office of the Southport and Ormskirk Hospital NHS Trust. This study complied with the principles of the Declaration of Helsinki.
Acknowledgment
This article is dedicated to Dr Arsalan Sheikh, SAS Doctors Tutor/Lead; Ms Zoe Whiteside, Postgraduate Coordinator & SAS Administrator, Education and Training; and Ms Dawn Aspinall, Head of Medical Education, Performance Coach, and Ambassador of Hope, Mersey and West Lancashire Teaching Hospitals NHS trust, District General Hospital, Southport, Merseyside, UK, for facilitating the publication of this article.
The article processing fee was paid out of Specialty and Specialist Doctors’ Development Fund of National Health Service, England.
Disclosure
The authors declare that they have no conflict of interest.
References
1. Medtech innovation briefing. Urethrotech UCD for difficult or failed catheterisation. Overview | Urethrotech UCD for difficult or failed catheterisation | Advice | NICE. Available from: www.nice.org.uk/guidance/mib116.
2. Bugeja S, Mistry K, Yim IHW, Tamimi A, Roberts N, Mundy AR. A new urethral catheterisation device (UCD) to manage difficult urethral catheterisation. World J Urol. 2019;37(4):595–600. doi:10.1007/s00345-018-2499-9
3. Dragova M, Bamfo A, Holmes K, Attard K, Frost A, Mundy A. Managing difficult catheterisation in nurse-led catheterisation services: does guidewire-assisted urethral catheterisation make a difference? Int J Urol Nurs. 2020;1–7. doi:10.1111/ijun.12228
4. Fluckiger S, John H. New urethral catheterisation devices for safety Urethral catheterisation in difficult cases. J Clin Urol. 2019;12(83):122–128. doi:10.1177/2051415819846081
5. Subramanian V, Madhusudan Soni B, Hughes PL, Khadr RN. Delay in diagnosis of urethral perforation due to catheterisation in a person with cervical spinal cord injury. Importance of (1) imaging studies done promptly for detection and documentation of urethral trauma, (2) Urethrotech catheterisation device to minimise urethral trauma and achieve successful catheterisation: a case report. Int J Surg Case Rep. 2023;112:108976. doi:10.1016/j.ijscr.2023.108976 Epub 2023 Oct 24. PMID: 37883868; PMCID: PMC10667899.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.