")
Back to Journals » Clinical Ophthalmology » Volume 17
Usability of an Eye Drop Delivery Aid for Single-Dose Instillation: Results from a Market Research Study
Authors Lebrón Gutiérrez K , Thomas S, Martin JL , Dahlmann-Noor A
Received 19 September 2023
Accepted for publication 20 November 2023
Published 30 November 2023 Volume 2023:17 Pages 3675—3684
DOI https://doi.org/10.2147/OPTH.S435467
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Keyla Lebrón Gutiérrez,1 Sarah Thomas,1 Julia L Martin,2 Annegret Dahlmann-Noor3
1Moorfields Eye Hospital, London, UK; 2Santen SA, La Voie-creuse 14, 1202, Geneva, Switzerland; 3NIHR Moorfields Biomedical Research Centre, London, UK
Correspondence: Annegret Dahlmann-Noor, NIHR Moorfields Biomedical Research Centre, London, UK, Email [email protected]
Background: One of the challenges of treating chronic ocular diseases like vernal keratoconjunctivitis (VKC), glaucoma, and ocular surface disease is patient adherence to topical medication. To support correct eye drop instillation, a variety of delivery aids have been developed for both single-dose and conventional multi-dose containers.
Methods: To evaluate Dropaid™ Single-dose, an eye drop delivery aid designed for single-dose containers, a usability study was conducted on 30 parents and caregivers of patients with VKC. After assessing the ability to squeeze a single eye drop from the single-dose container onto the eye of a pediatric medical dummy, the delivery aid was evaluated using an 11-point Likert scale on a variety of characteristics: from “very difficult” (− 5) to “very easy” (+5).
Results: The majority of participants rated the task of opening the single-dose units (SDUs), preparing, and positioning the Dropaid™ Single-dose device as “very easy”. When providing a single eye drop from the container, 87% of participants rated the Dropaid™ Single-dose device as either “very easy” or “easy”, with a median rating score of +5.0 (interquartile range [IQR], 4.0– 5.0). For general ease of use, 84% considered the delivery aid as either “very easy” or “easy”, with a median score of +4.0 (IQR, 3.0– 5.0). Most participants (93%) rated Dropaid™ Single-dose as either “very comfortable” or “comfortable” to hold, with a median score of +5.0 (IQR, 4.0– 5.0).
Conclusion: The Dropaid™ Single-dose delivery aid demonstrated rapid learning and ease of use across all stages of application, including opening the container, eye drop administration, and handling comfort. Although designed for use with single-dose containers to help eye drop instillation in patients with VKC, Dropaid™ Single-dose may provide a wider utility across a range of other ocular diseases such as glaucoma and dry eye.
Keywords: Dropaid, eye drop instillation, usability study, vernal keratoconjunctivitis, VKC
Introduction
Eye drop medication is the mainstay of treatment for ophthalmic conditions as they are administered locally and directly at the site of action. Major challenges in treating chronic ocular diseases, such as vernal keratoconjunctivitis (VKC), glaucoma, and ocular surface disease, include patient adherence and persistence with medication.1–3
While an apparently simple task, the effective administration of eye drops may pose problems for some patients and/or their caregivers. For example, when considering patients with glaucoma, physical and dexterity challenges in self-administering drops are commonly cited,1–3 and trouble with instilling eye drops is a significant barrier to treatment adherence.1 Such instillation problems often include difficulties with aim; controlling the number of drops dispensed; holding steady while squeezing the bottle; flinching or blinking, causing the drops not to enter the eye; and issues squeezing the bottle.1
For patients to achieve an optimal therapeutic effect, while minimizing side effects, it is imperative that eye drops are instilled correctly, and adherence is maintained for the duration of the prescribed treatment plan. Some of the most important steps in proper eye drop technique include accurate targeting into the eye, ease of squeezing one drop from the container, and not touching the bottle to the eye surface.4 If eye drops are instilled improperly, there may be a lessening in therapeutic response, enhanced systemic side effects, and direct harm to the eye (ie bottle contamination or ocular trauma by touching the eye with the bottle tip). There is evidence to suggest that the healthy ocular surface harbors a stable composition of organisms that, when disrupted (such as with ocular trauma or contamination), can predispose patients to developing ocular surface infection or inflammation.5 The ocular microbiota includes all types of microorganisms, both commensal and pathogenic, living on or in the eye, which can regulate, defend, or provoke and perpetuate the development of chronic eye diseases.6 Therefore, proper eye drop instillation remains important.
Successful eye drop instillation is an acquired skill and bottle tip-related contamination and ocular trauma need to be avoided.7 For patients with ocular diseases who self-administer eye drops, studies have shown that approximately half contaminate the bottle tip when using a conventional bottle, and less than one-third are able to instill a single drop without the bottle tip touching the eye. This is despite over 92% of patients declaring they have no problems instilling eye drops.7–9 Moreover, it is generally accepted that the risk of contamination increases with a prolonged period of drop application from the same container, with the bottle tip more likely to become contaminated than the internal fluid contents.10
Although preservatives are utilized in ophthalmic multi-dose bottles to minimize bacterial contamination and maintain sterility, there is evidence of the negative effects of preservatives, such as benzalkonium chloride, on the ocular surface, especially with long-term use.11,12 To counter this, unpreserved treatment options have been developed, including unit-dose pipettes, also known as single-dose containers or single-dose units (SDUs), designed for one-off administration.12 Studies investigating usability and patient choice for SDUs, or conventional multi-dose eye drop containers, suggest that preferences may vary from patient to patient.7,8 However, in elderly patients treated for glaucoma, a comparison of SDUs and multi-dose containers highlighted a significant benefit in utilizing SDUs in terms of ease of administration and overall performance.13 For conditions commonly affecting young children, such as VKC,14,15 the responsibility for administering eye drops typically falls to the patient’s parent, guardian, or caregiver.
To ease and support the correct instillation of eye drops, a variety of delivery aids have been developed and are readily available, which have demonstrated effectiveness compared with controls.7,8 These include the Opticare® range (manufactured by Cameron Graham Limited, UK), the Autodrop® and AutoSqueeze® (manufactured by Owen Mumford Ltd., UK), and the Xal-Ease™ delivery device (Pfizer), to name a few, but availability varies worldwide. Santen has exclusively developed the Dropaid™ delivery aids for use in combination with their products, including the green single-dose Dropaid™ device and the blue multidose Dropaid™ device. Both made from polypropylene which is easily processable, biologically inert, antibacterial, non-toxic, and recyclable. These are designed for accurate positioning over the eye with easy grip control and may be particularly useful for patients with limited dexterity. The Dropaid™ Single-dose is a delivery aid for use in combination with Santen single-dose containers to help patients easily instill eye drops from the container and is the first of its kind for use in children.
The Dropaid™ delivery aids were tested internally; with no usability testing required due to prior distribution to patients, pharmacies, and ophthalmologists since 2008 without complaints – CE registration was completed in 2015. The primary objectives were to assess compression force measurements of the device with a range of different eye drop pipettes/containers – Santen products available in Europe were chosen to represent different container types and product viscosities. Results showed that the required squeezing force for all tested product/container combinations was significantly reduced and there was not any significant variability in drop release. The evaluation points show that the unit doses (pipettes/containers) were easily adjusted into the Dropaid™ device, with drops released easily without jet or foam when squeezing the handles of the device, and the distance from the tip of the container and the plane defined by the rim of the device cup far enough to prevent the tip of the container touching the patient’s eye.
To assess the usability characteristics and patient preferences of the Dropaid™ Single-dose device, a market research study was conducted with parents of patients with VKC. The study was designed to evaluate the ability of participants to squeeze a single drop from the container, assess the usability of the delivery aid for administering Verkazia® (topical ciclosporin A ophthalmic solution) proxy in single-dose containers, and gather information on ease of use.
Materials and Methods
Adult parents or caregivers of pediatric patients diagnosed with VKC that used Dropaid™ Single-dose were considered for study inclusion. Adult participants between 18–60 years of age were identified at the pediatric department of Moorfields Eye Hospital National Health Service (NHS) Foundation Trust during routine clinic visits within the recruitment period (September–October 2022). Recruitment was performed by a member of the healthcare team trained specifically to work on the study, and all participants were presented with a study information sheet and provided written informed consent before participation. The study was scheduled to take place on the same day as a routine clinic appointment (ie when the participant would already be accompanying the patient to the clinic).
Participants were asked to administer Cationorm® Pro+ emulsion eye drops (artificial tears) onto the eye of a pediatric medical dummy via the use of Dropaid™ Single-dose. Cationorm® Pro+ is a sterile, unpreserved ophthalmic eye drop emulsion provided in single-dose containers of identical size and shape as commercial Verkazia®, but without the active ciclosporin compound. The Cationorm® Pro+ design variant was used as a proxy in this study. The Cationorm® Pro+ and Dropaid™ Single-dose bottles were supplied by Santen. All participants were informed on the Instructions for Use. A summary of the how to use the device is included in the Supplementary Materials.
After completing the usability test on the medical dummy, usability characteristics of the delivery aid were evaluated by a questionnaire, which was completed by the participant immediately following the test. Each feature of the delivery aid was evaluated using an 11-point grading system ranging from −5 (“extremely difficult”) to +5 (“extremely easy”). The number of eye drops administered using Dropaid™ Single-dose, the dominant hand used, and the first eye selected for administration were also recorded by a member of the study team. Demographic information was collected for each participant including sex, age, and prior experience of administering eye drops for ocular diseases.
Statistical Analysis Plan
Descriptive statistics were calculated for independent variables: participant role, age, gender, and handedness; duration and frequency of prior use of eye drop medications; and type of eye drop containers currently used (single-dose or multi-dose containers).
Descriptive statistics were also calculated for the dependent variables: opening the container; placing the container within the Dropaid™ Single-dose device; shaking the container; placing the delivery aid cup over the medical dummy’s eye; producing a single drop of emulsion; pressure required to apply the drop with the delivery aid; targeting the drops into the medical dummy’s eye; removing the eye drop container from the delivery aid after use; general ease of use; how comfortable the delivery aid was to hold; and any difficulties associated with using Dropaid™ Single-dose.
Given the small sample size (N=30), as well as the large number of questionnaire inquiries, the study outcomes focus on substantive differences rather than statistical significance.
Results
Demographic and Participant Profile
In total, 30 participants were included in the study. The majority (83.3%, n=25) were female, the median age was 41.5 years (interquartile range [IQR], 38.0–46.8 years), and all participants (100%) were parents of a pediatric patient with VKC attending Moorfields Eye Hospital NHS Foundation Trust.
All participants reported prior experience with administering eye drops to a child: 33% (n=10) regularly administered eye drops to a child four times a day, 27% (n=8) reported administering eye drops every day, and 23% (n=7) had applied eye drops twice a day. Participants (N=29; data missing from one participant) covered a broad range of application experience, with a median duration of 24.0 months (IQR, 12.0–48.0 months) for administering eye drops to another person. Overall, 62% (n=18) of participants had applied eye drops to their child for ≥24 months, 24% (n=7) for <12 months, and 14% (n=4) for 12–24 months.
There was a relatively even distribution regarding the proportion of participants using single-dose containers to administer eye drops to their child compared with multi-dose eye drop containers – 48% (n=16) were currently using single-dose containers and 52% used multi-dose containers (n=17). The median duration of prior use of single-dose containers was 36.0 months (IQR, 14.3–48.0 months) and prior use of multi-dose containers was 30.0 months (IQR, 10.5–41.0 months); use of eye drop container type was not mutually exclusive (Table 1).
 |
Table 1 Prior Use of Ocular Medication (Eye Drops) in Months |
Dropaid™ Single-Dose Preparation
On a categorized scale of “very difficult” (−5) to “very easy” (+5), the majority of participants rated the task of opening the container, preparing, and positioning Dropaid™ Single-dose as “very easy”. The median score for ease of opening the container was +4.5 (IQR, 4.0–5.0), with 77% (n=23) of participants rating the ability to open the container with the delivery aid as “very easy”; 20% considered the container “easy” or “neutral” (Figure 1A).
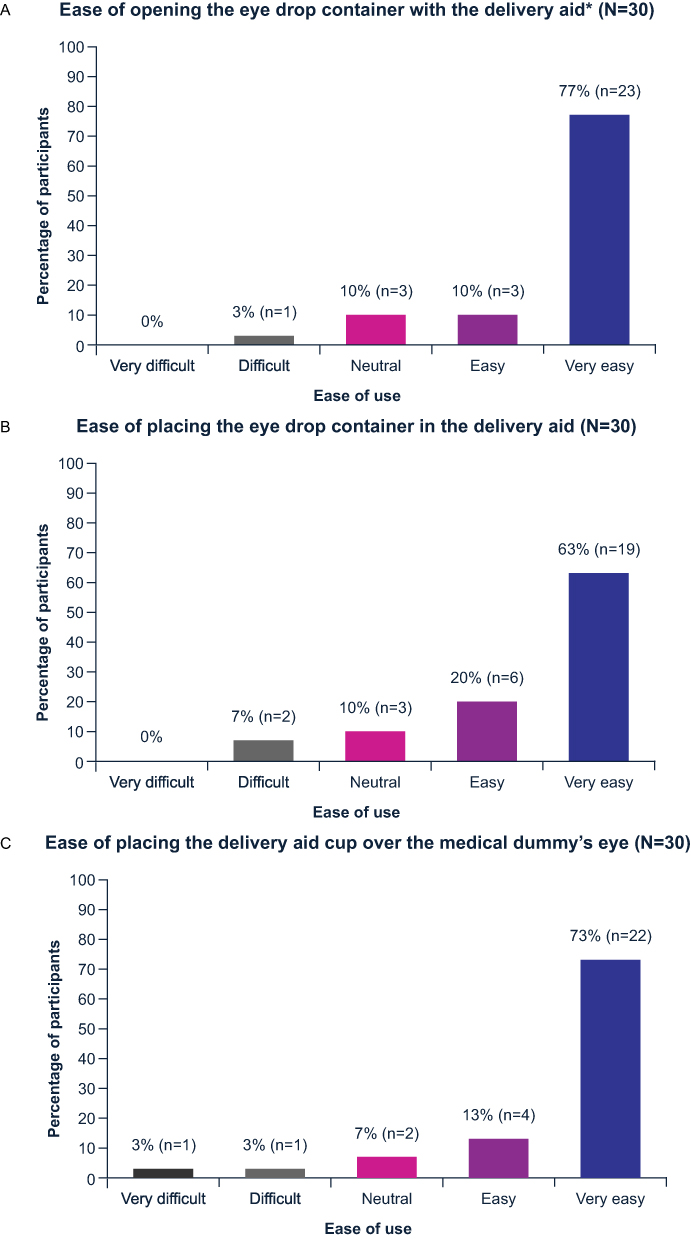 |
Figure 1 Ease of Dropaid™ Single-dose preparation. (A) Ease of opening the eye drop container with the delivery aid* (N=30). (B) Ease of placing the eye drop container in the deliver aid (N=30). (C) Ease of placing the delivery aid cup over the medical dummy’s eye (N=30). *Participants were instructed on how to use the Dropaid™ Single-dose slot to open the SDU container if required. |
Similar results were obtained for ease of placing the single-dose container into Dropaid™ Single-dose, with a median score of +4.0 (IQR, 2.0–5.0). In total, 63% (n=19) of participants rated the ease of placing the eye drop container in the delivery aid as “very easy”; 20% (n=6) rated placement as “easy”, and 10% (n=3) provided a “neutral” response (Figure 1B).
Overall, 83% of participants rated shaking the container within the delivery aid as “very easy” (70%, n=21) or “easy” (13%, n=4). The median score was +5.0 (IQR, 3.0–5.0). However, 13% of participants (n=4) rated the preparation stage as “difficult” or “very difficult” (response of −5 to −1).
The ease of placing the primed Dropaid™ Single-dose over the medical dummy’s eye was evaluated as “very easy” (73%, n=22) or “easy” (13%, n=4) by 86% of the majority. The median score was +5.0 (IQR, 3.3–5.0) (Figure 1C).
Drop Application
When utilizing Dropaid™ Single-dose to provide one drop of emulsion from the container, 77% of participants (n=23) rated the procedure as “very easy”, 10% (n=3) as “easy” and 7% (n=2) as “neutral”. The median rating score was +5.0 (IQR, 4.0–5.0), which corresponds to the “very easy” response (Figure 2A).
 |
Figure 2 Ease of drop application with Dropaid™ Single-dose. (A) Ease of squeezing a drop out of the eye drop container, within the delivery aid (N=30). (B) Squeezing force needed for dropping (N=30). (C) Ease of targeting the drop in the medical dummy’s eye (N=30). |
Results from the questionnaire indicated that the amount of pressure required to produce the drop from the eye container when within the delivery aid was rated as +3.5 (IQR, −2.0–5.0), which relates to the “large force” to “very large force” response. Half of the participants (50%, n=22) rated the eye drop dispersal as requiring a “very large force”, with only 20% (n=6) and 13% (n=4) responding as needing “little force” or “very little force”, respectively (Figure 2B). However, in follow-up, the study investigators noted that these results are contradictory to the observed ease of use. The results may be skewed due to how the question was asked, where the Likert scale of this question was from positive (“little force required”) to negative (“large force required”), unlike the other questions which were ordered from negative to positive. Therefore, the respondents may have answered in a consistent fashion assuming the same direction of the Likert scale, and thus providing “inaccurate” answers. Anecdotally, from the participants, the force required to use Dropaid™ Single-dose was little, which is reflected by the aforementioned results rating the delivery aid as either “very easy” to use (57%, n=17) or “easy” to use (27%, n=8).
Considering targeting the drop into the medical dummy’s eye, the median score was +3.0 (IQR, 1.3–5.0). In total, 47% of participants (n=14) considered the use of Dropaid™ Single-dose to target the medical dummy’s eye as “very easy” and 30% (n=9) rated it as “easy”. Conversely, 10% of participants (n=3) rated the delivery aid targeting as “very difficult” (Figure 2C).
After use, 97% of participants found that removing the used single-dose container from the delivery aid was “very easy” (67%, n=20), “easy” (17%, n=5), or provided a “neutral” response (13%, n=4). The median score for ease of container removal was +4.5 (IQR, 2.3–5.0).
General Usability of Dropaid™ Single-Dose
Participants evaluated both the general ease and comfort of use for Dropaid™ Single-dose (Figure 3 shows an example of the general usability the delivery aid). In total, 84% of participants (n=25) rated the delivery aid as either “very easy” to use (57%, n=17) or “easy” to use (27%, n=8). The associated median score was +4.0 (IQR, 3.0–5.0).
 |
Figure 3 Ease of drop application with Dropaid™ Single-dose. |
The majority of participants considered Dropaid™ Single-dose as “very comfortable” (83%, n=25) or “comfortable” (10%, n=3) to hold, with a median score of +5.0 (IQR, 4.0–5.0).
Almost three-quarters (73%, n=22) of participants reported no difficulty using Dropaid™ Single-dose. For the remaining eight participants, difficulties encountered comprised issues with dispensing the drops, ensuring the emulsion entered the eye properly (including the amount dispensed), and not understanding the delivery aid instructions. Based on free text responses, one participant suggested that delivery aid was potentially not needed for older children. The same participant also stated that more medication was “used/wasted” with Dropaid™ Single-dose compared with applying the single-dose container alone.
When asked about overall delivery aid usage, 100% of respondents (N=29; data missing from one participant) stated they would use the delivery aid as per instructions. All participants were able to perform the study without requiring practical support, and 97% did not have questions regarding Dropaid™ Single-dose, eye drop application, or container removal. In total, 53% of participants (n=16) stated they would recommend Dropaid™ Single-dose to a friend and 17% (n=5) indicated they would “maybe” recommend the delivery aid.
Additional descriptive data and images of the device can be found in the Supplementary Materials.
Discussion
This study attempted to determine the usability characteristics of Dropaid™ Single-dose for administering Verkazia® or other Santen single-dose products and evaluate the ability to squeeze a single drop from the container. Participants were experienced at instilling eye drops, with current applications to their children using a range of single-dose and multi-dose eye drop containers.
Most participants reported that preparing Dropaid™ Single-dose with the container was “very easy”, and instilling the drop into the dummy eye was either “very easy” or “easy”, with a high level of handling comfort. The majority of participants suggested they did not experience any difficulty using Dropaid™ Single-dose during the study. Where difficulties were noted, these were associated with eye drop targeting and dispensing. Most participants reported that they would recommend the delivery aid to a friend (if appropriate).
When considering the pressure required to administer eye drops from Dropaid™ Single-dose, approximately 50% of participants reported requiring a large force. The use of a large force with the delivery aid may be associated with the larger quantity of eye drops instilled during the first use compared with the second. However, the delivery aid was associated with a fast learning curve, with participants more likely to instill a single drop once they had become familiar with its use. One technique possibility implemented is recognizing that squeezing the extreme ends of the handles may help avoid using a large force.
The study was limited by the relatively small participant population (N=30), which was reflected in the lack of statistical modeling and the restricted number of eye drop instillations applied to the medical dummy. As a non-comparative study, data on treatment application and ease of use rely on the subjective responses of participants on the study day. The accuracy of data extrapolated from a Likert scale,16 which is commonly used in social science research,17 is often discussed in the scientific literature, particularly in relation to the scale intervals.18–20 Although the current study utilizes an 11-point scale (−5 to +5), the grouping of numerical responses reduces the outcomes to the equivalent of a 5-point scale (“very difficult”, “difficult”, “neutral”, “easy”, and “very easy”), with a potential impact on scale robustness.18,21,22
Delivery aids for eye drop containers are not a novel concept, especially for elderly patients experiencing either manual or visual difficulties that may compromise drop instillation. Most commercially available delivery aids are designed to accommodate multi-dose bottles for age-related conditions, such as glaucoma, to help limit squeeze-force requirements (as elderly patients often also present with dexterity issues), reduce bottle tip contamination, and lessen potential tip-related ocular trauma.7,23,24 Previous studies in both elderly patients with eye drop experience and non-elderly subjects without application experience demonstrate that eye drop delivery aids are easy to assemble and use, improve treatment delivery over conventional bottles, and are associated with a fast learning curve.7,24
Eye drop delivery aids available at Moorfields Eye Hospital include just two devices for single-dose containers.23 Dropaid™ Single-dose was initially designed for use in combination with Verkazia® for patients with VKC but enables the application of other products from Santen – as demonstrated by the use of Cationorm® Pro+ emulsion within this study. The positive findings from this market research study may have wider implications for single-dose containers with identical designs and provide the potential for expanding the utility of Dropaid™ Single-dose across a range of other products for other ocular diseases, such as glaucoma or dry eye.
Conclusion
In a usability study for administering eye drops in single-dose containers, Dropaid™ Single-dose demonstrated a favorable response from parents of pediatric patients with regards to rapid learning and ease of use across all stages: from opening the container, administration of the eye drop, comfort, and the ability to independently use the delivery aid.
Ethics Approval and Informed Consent
All study participants provided written informed consent to take part in the market research study and for their questionnaire responses to be analyzed and combined to produce a results report for sharing with the study sponsor, Santen SA. No Ethics Committee approval was required and confirmed by the Health Regulatory Authority. The study complied with the principles of the Declaration of Helsinki of 1964 as revised in 2013.
Acknowledgments
The authors acknowledge Richard Maver (Synergy Vision, UK) for medical writing and editorial assistance, based on the authors’ input and direction. This was funded by Santen SA in accordance with Good Publication Practice (GPP3) Guidelines (http://www.ismpp.org/gpp3).
Author Contributions
All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The market research study was funded by Santen SA. Publication support for third-party writing assistance for this article, provided by Synergy Vision, UK, and all associated publication costs were also funded by Santen SA. Selected results from this study have previously been presented in brief at the American Association for Pediatric Ophthalmology and Strabismus (AAPOS) congress in New York, USA (29 March–02 April 2023). The presentation of this work at AAPOS was supported by Moorfields Eye Charity.
Disclosure
A Dahlmann-Noor: Consultant/Advisor: Santen, SightGlass Vision, Théa. Honorarium recipient: CooperVision, Novartis, Santen, SightGlass Vision, Théa, Zeiss. Speaker: Santen, Zeiss. S Thomas: Consultant/Advisor: Glaucoma UK, Santen. Honorarium recipient: Santen. Speaker: Santen. JL Martin is an employee of Santen. K Lebrón Gutiérrez has no commercial or financial relationships to declare that could be construed as a potential conflict of interest.
References
1. Newman-Casey PA, Robin AL, Blachley T, et al. The most common barriers to glaucoma medication adherence: a cross-sectional survey. Ophthalmology. 2015;122(7):1308–1316. doi:10.1016/j.ophtha.2015.03.026
2. Sleath B, Robin AL, Covert D, et al. Patient-reported behavior and problems in using glaucoma medications. Ophthalmology. 2006;113(3):431–436. doi:10.1016/j.ophtha.2005.10.034
3. Stryker JE, Beck AD, Primo SA, et al. An exploratory study of factors influencing glaucoma treatment adherence. J Glaucoma. 2010;19(1):66–72. doi:10.1097/IJG.0b013e31819c4679
4. Thomas S. How to use your eye drops [website]. UK: Moorfields Eye Hospital NHS Foundation Trust; 2020. Available from: https://www.moorfields.nhs.uk/sites/default/files/How%20to%20use%20your%20eye%20drops.pdf.
5. Chang CCJ, Somohano K, Zemsky C, et al. Topical glaucoma therapy is associated with alterations of the ocular surface microbiome. Invest Ophthalmol Vis Sci. 2022;63(9):32. doi:10.1167/iovs.63.9.32
6. Borroni D, Paytuví-Gallart A, Sanseverino W, et al. Exploring the healthy eye microbiota niche in a multicenter study. Int J Mol Sci. 2022;23(18):10229. doi:10.3390/ijms231810229
7. Brand G, Hecht I, Burgansky-Eliash Z, et al. Comparison of the usability of eye drop aids and the conventional bottle. J Clin Med. 2021;10(23):5658. doi:10.3390/jcm10235658
8. Dietlein TS, Jordan JF, Lüke C, et al. Self‐application of single‐use eyedrop containers in an elderly population: comparisons with standard eyedrop bottle and with younger patients. Acta Ophthalmol. 2008;86(8):856–859. doi:10.1111/j.1755-3768.2007.01155.x
9. Stone JL, Robin AL, Novack GD, et al. An objective evaluation of eyedrop instillation in patients with glaucoma. Arch Ophthalmol. 2009;127(6):732–736. doi:10.1001/archophthalmol.2009.96
10. Teuchner B, Wagner J, Bechrakis NE, et al. Microbial contamination of glaucoma eyedrops used by patients compared with ocular medications used in the hospital. Medicine (Baltimore). 2015;94:e583. doi:10.1097/MD.0000000000000583
11. Aguayo Bonniard A, Yeung JY, Chan CC, et al. Ocular surface toxicity from glaucoma topical medications and associated preservatives such as benzalkonium chloride (BAK). Expert Opin Drug Metab Toxico. 2016;12(11):1279–1289. doi:10.1080/17425255.2016.1209481
12. Ramli N, Supramaniam G, Samsudin A, et al. Ocular surface disease in glaucoma: effect of polypharmacy and preservatives. Optom Vis Sci. 2015;92(9):e222–e226. doi:10.1097/OPX.0000000000000542
13. Parkkari M, Latvala T, Ropo A. Handling test of eye drop dispenser – comparison of unit-dose pipettes with conventional eye drop bottles. J Ocul Pharmacol Ther. 2010;26(3):273–276. doi:10.1089/jop.2009.0111
14. Kanski JJ. Disorders of the conjunctiva: vernal keratoconjunctivitis. In: Clinical Ophthalmology: A Systematic Approach.
15. Leonardi A. Management of vernal keratoconjunctivitis. Ophthalmol Ther. 2013;2(2):73–88. doi:10.1007/s40123-013-0019-y
16. Likert R. A technique for the measurement of attitudes. Arch Psychol. 1932;140:5–55.
17. Louangrath P, Sutanapong C. Validity and reliability of survey scales. Int J Soc Res Methodol. 2018;4(3):99–114. doi:10.5281/zenodo.2545038
18. Chang L. A psychometric evaluation of 4-point and 6-point Likert-type scales in relation to reliability and validity. Applied Psychol Meas. 1994;18(3):205–215. doi:10.1177/014662169401800302
19. Hasson D, Arnetz B. Validation and findings comparing VAS vs. Likert scales for psychosocial measurements. Int Electron J Health Educ. 2005;8:178–192.
20. Joshi A, Kale S, Chandel S, et al. Likert scale: explored and explained. Br J Appl Sci Technol. 2015;7(4):396–403. doi:10.9734/BJAST/2015/14975
21. Johns R. Likert items and scales [website]. UK: University of Strathclyde; 2010. Available from: https://dam.ukdataservice.ac.uk/media/262829/discover_likertfactsheet.pdf.
22. Tsang KK. The use of midpoint on Likert Scale: the implication for educational research. Hong Kong Teachers’ Centre J. 2012;11:121–130.
23. Thomas S. Eye drop compliance aids [website]. UK: Moorfields Eye Hospital NHS Foundation Trust; 2020. Available from: https://www.moorfields.nhs.uk/sites/default/files/Eye%20drop%20compliance%20aids.pdf.
24. Zhu CQ, Sadlak N, Fiorello MG, et al. A comparison of patient acceptance of 3 eye drop instillation aids. J Glaucoma. 2021;30(8):725–731. doi:10.1097/IJG.0000000000001891
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.