")
Back to Journals » Clinical Ophthalmology » Volume 16
Survey of the American Glaucoma Society Membership on Current Glaucoma Drainage Device Placement and Postoperative Corticosteroid Use
Authors Yonamine S , Ton L , Rose-Nussbaumer J, Ying GS, Ahmed IIK, Chen TC, Weiner A, Gedde SJ, Han Y
Received 15 April 2022
Accepted for publication 5 July 2022
Published 21 July 2022 Volume 2022:16 Pages 2305—2310
DOI https://doi.org/10.2147/OPTH.S369673
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Sean Yonamine,1,* Lauren Ton,2,* Jennifer Rose-Nussbaumer,3 Gui-Shuang Ying,4 Iqbal Ike K Ahmed,5 Teresa C Chen,6 Asher Weiner,7 Steven J Gedde,8 Ying Han1
1Department of Ophthalmology, University of California San Francisco, San Francisco, CA, USA; 2School of Medicine, University of California San Francisco, San Francisco, CA, USA; 3Stanford Byers Eye Institute, Palo Alto, CA, USA; 4Center for Preventive Ophthalmology and Biostatistics, Department of Ophthalmology, University of Pennsylvania, Philadelphia, PA, USA; 5Prism Eye Institute, Mississauga, Ontario, Canada; 6Massachusetts Eye and Ear Infirmary, Harvard Medical School, Boston, MA, USA; 7University at Buffalo, State University of New York, Buffalo, NY, USA; 8Bascom Palmer Eye Institute, University of Miami Miller School of Medicine, Miami, FL, USA
*These authors contributed equally to this work
Correspondence: Ying Han, Department of Ophthalmology, University of California San Francisco, San Francisco, CA, USA, Tel +1 415 514 6920, Fax +1 415 353 4250, Email [email protected]
Purpose: To assess practice patterns and opinions of glaucoma specialists regarding glaucoma drainage device tube shunt placement and post-operative anti-inflammatory medication use. We also assess the perceived need for a randomized control trial to compare them.
Patients and Methods: An online survey was distributed to a group of glaucoma specialists from the American Glaucoma Society via the American Glaucoma Society forum from April to August 2021.
Results: One hundred and twenty-eight responses were included. Ninety percent placed tubes in the anterior chamber. Sixty-one percent reported that evidence suggested the superiority of sulcus tube placement over the anterior chamber, whereas 34% reported there was not enough evidence to suggest superiority of either in preventing endothelial cell loss. Comparing these techniques for intraocular pressure control, 49% reported evidence suggested sulcus tube placement superiority whereas 46% reported there was not enough evidence. Over 40% of respondents reported that they were either unfamiliar with literature or that there was not enough evidence to support the superiority of difluprednate 0.05% over prednisolone 1% for post-operative use in preventing endothelial cell loss and for intraocular pressure control. Ninety percent and 81% of respondents respectively would benefit from randomized control trials comparing outcomes of anterior chamber vs sulcus tube placement and post-operative corticosteroid usage.
Conclusion: Most glaucoma specialists surveyed place glaucoma drainage device tube in the anterior chamber over the sulcus. A randomized control trial to determine optimal tube placement and post-operative anti-inflammatory medication use for preventing endothelial cell loss would change current glaucoma drainage device practice patterns.
Keywords: endothelial cell loss, sulcus, glaucoma drainage device
Introduction
Glaucoma is the leading cause of irreversible blindness in the world and continues to be a major public health issue.1 Glaucoma drainage device (GDD) surgery is one of the most commonly performed surgeries to treat glaucoma due to its excellent success rate and safety profile.2–5
One of the principal long-term complications of GDD surgery is progressive corneal endothelial cell loss (ECL) leading to corneal decompensation.6 Normal age-related ECL has been estimated to be approximately 0.6% per year on average.7 Studies have shown that GDD implantation with tube placement in the anterior chamber (AC) was associated with ECL of 6.4–15.2% in 1 year8–10 and 11.5–18.6% by 2 years.8,10,11
One potential mechanism for ECL after GDD surgery is direct mechanical damage from the silicone tube in the AC, the most common site of tube placement. To address this concern, the tube can be inserted into the ciliary sulcus, increasing the distance between the tube and the corneal. There are studies suggesting that sulcus tube placement may lead to a slower rate of ECL12 while providing equivalent intraocular pressure (IOP) control to AC tube placement.12–16 Despite this, most glaucoma specialists still place tubes in the AC. Sulcus tube placement is technically more challenging and may be associated with and increased risk of complications, such as intraocular bleeding and tube obstruction.
Another potential mechanism for increased ECL after GDD surgery is low grade, chronic inflammation and changes to the AC microenvironment. Better anti-inflammatory therapy may thus provide an opportunity to prevent ECL. Although topical steroids are routinely used, there may be a role for a stronger anti-inflammatory agent, such as difluprednate, in inflammation control and slowing ECL after GDD implantation. However, this has not been adequately studied.
There is little information about the current opinions of glaucoma specialists on the benefits of GDD tube placement in the AC versus the ciliary sulcus, and their opinion on postoperative corticosteroid use after GDD implantation. In this study, we conducted a survey to assess glaucoma specialists’ practice patterns and their opinions on variations of GDD placement and GDD post-operative care.
Materials and Methods
An email containing a Qualtrics electronic survey link was sent to approximately 1500 American Glaucoma Society (AGS) members subscribed to the AGS forum from April 2021 to August 2021. Members of the AGS must be glaucoma fellowship-trained ophthalmologists, current glaucoma fellows, or otherwise have a primary research interest in the study of glaucoma. The study was sent once with a reminder sent during the survey collection period. Participation was voluntary and no personal information or identifiers were collected. There was no incentive for participating in the study. Informed consent was not needed for this study because no personal identification information was collected and the data from all participants were pooled together for analysis and publication. This has been confirmed with the Institutional Review Board at University of California, San Francisco. The participants were notified that the survey results are subject to be published. The survey was created on April, 21 2021 using Qualtrics (Version April 2021), an online survey software.
Based on discussion with a focus group of glaucoma specialists, the authors of this study devised the survey questions. The survey consisted of 15 questions (Supplemental Figure 1). Physicians were asked to weigh the current level of evidence for tube placement locations and different corticosteroid usage in preventing ECL and for IOP control. They were also asked to evaluate the benefit of a randomized clinical trial (RCT) comparing post-operative ECL and IOP control in different tube placement locations and with different corticosteroid regimens, and if the results from an RCT would change their practice. Finally, survey respondents were asked to provide their location and practice characteristics.
All descriptive statistical analyses were performed using Python version 3.7 (Python Software Foundation, Fredericksburg, VA, USA). The study was approved by the Institutional Review Board of the University of California, San Francisco (Study Number: 21-33707).
Results
We received a total of 128 completed responses to the survey (Supplemental Figure 1). Respondents were primarily from the USA (n = 118) with remaining respondents from Canada (n = 6), Switzerland (n = 1), Turkey (n = 1), Israel (n = 1), and Columbia (n = 1). All had done a glaucoma fellowship with a median of 14 years in practice (interquartile range (IQR) 5, 26) and median of 15 years performing GDD (IQR 7, 25). Survey respondents performed a median of 4 GDD surgeries per month (IQR 2, 6), with 90% (IQR 50%, 95%) of tubes placed in the AC for pseudophakic patients.
Study respondents were asked to weigh the current level of evidence for AC versus sulcus for tube placement in different parameters after GDD implantation. While over half of study respondents (n = 78, 60.9%) reported that the current evidence suggests tube placement in sulcus is superior to tube placement in the AC for preventing ECL, one-third reported that there was not enough evidence to support the superiority of one tube location versus the other for preventing ECL (n = 43, 33.6%) (Table 1).
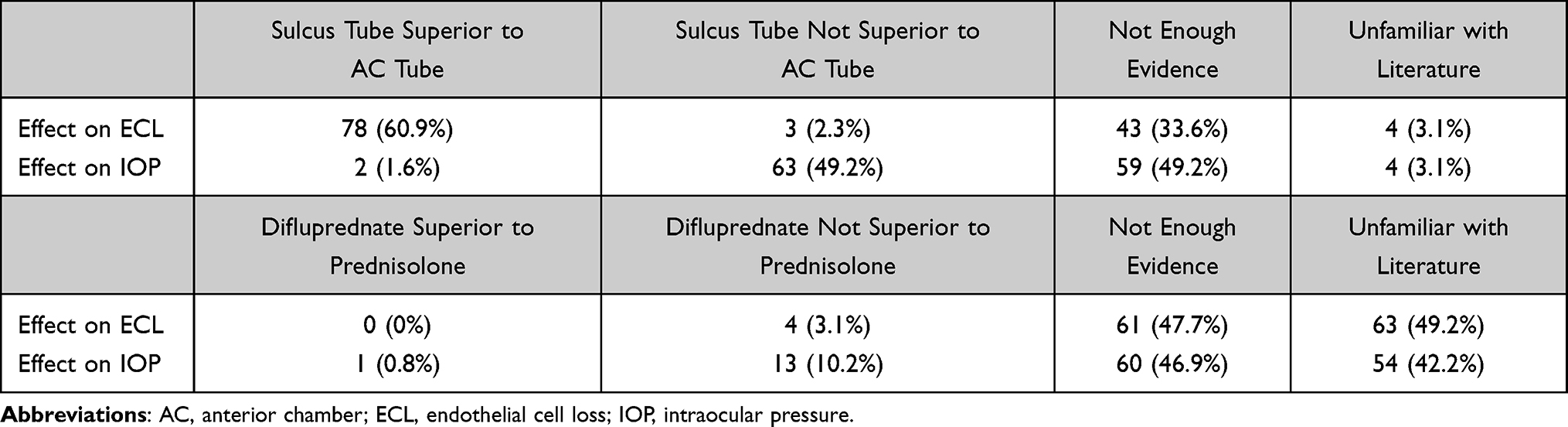 |
Table 1 Evaluation of Current Level of Evidence on the Effect of Tube Locations and Postoperative Anti-Inflammatory Treatments on ECL and IOP |
There was less consensus when asked about the current level of evidence for tube placement in controlling IOP after GDD implantation. Approximately half of respondents (n = 63, 49.2%) reported that the evidence suggests that sulcus tube placement was either equivalent or inferior to AC tube placement in controlling IOP. Almost an equal number of respondents reported there was not enough evidence to support the superiority of one tube location versus the other for IOP control (n = 59, 46.1%) (Table 1).
When asked if a RCT comparing ECL and IOP after GDD implantation with tube placement in the AC versus in the ciliary sulcus would be beneficial, 115 (89.8%) reported that it would be beneficial, and only 24 (10.2%) reported it would not be beneficial (Table 2). When asked if they would change their GDD tube placement if an RCT showed that placement in sulcus tube was superior placement in the AC in preventing ECL, the majority (n = 98, 76.5%) reported that they were likely to change their practice (Table 3).
 |
Table 2 Opinion on Whether an RCT Comparing ECL & IOP After GDD in Different Tube Locations and Postoperative Anti-Inflammatory Treatments Be Beneficial |
 |
Table 3 Assessment of Whether Practice Patterns Will Change Based on the RCT Results |
Study respondents were also asked their opinion on the current evidence for stronger postoperative corticosteroids for preventing ECL after GDD implantation. Forty-nine percent (n = 63) of respondents reported they were not familiar with the literature, while 47.7% (n = 61) reported that there was not enough evidence to support the superiority of difluprednate 0.05% over prednisolone 1% for prevention of ECL. The minority reported that current evidence suggests that difluprednate 0.05% was not superior to prednisolone in preventing ECL (n = 4, 3.1%) (Table 1).
There were similar opinions on the current evidence for stronger postoperative corticosteroids for controlling IOP after GDD implantation. Forty-six percent of respondents (n = 60) reported that there was not enough evidence to support the superiority of difluprednate 0.05% over prednisolone 1% for better IOP control, and 42.2% reported they were unfamiliar with the literature. Approximately 9% of respondents (n = 11) reported that the current evidence suggests there was either no difference in IOP control between the two corticosteroids or that prednisolone was superior to difluprednate (Table 1).
Lastly, respondents reported their opinions on the benefits of a RCT comparing the postoperative IOP control of prednisolone 1% versus difluprednate 0.05%, and its potential impact on their practice. Most respondents reported a RCT comparing the two corticosteroids would be beneficial (n = 104, 81.2%) (Table 3). The majority of respondents (n = 115, 89.8%) reported they would be at least somewhat likely to change their postoperative choice of corticosteroid after GDD if a RCT showed the superiority of difluprednate 0.05% to prednisolone for better IOP control (Table 3).
There was no significant difference in survey responses based upon years of clinical practice or years of GDD placement (10 years or less vs 11 or more years), amounts of GDD surgery (5 surgeries or less per month vs 6 surgeries or more per month), or preferred tube shunt placement (greater than 51% in the AC vs less than 50% in the AC) (all p > 0.62, Supplemental Table 1A–D).
Discussion
In this study, we surveyed glaucoma specialists’ practice patterns and opinions regarding GDD surgery. Although retrospective studies have suggested a benefit of GDD placement in the sulcus tube for endothelial cells protection, we found the majority of glaucoma specialists still place the tube in the AC in their current practice. They felt strongly that there is a need for a well-designed RCT to provide convincing evidence regarding the optimal tube locations and postoperative use of anti-inflammatory medication for GDD surgery. More importantly, they are willing to change their current practice pattern based on the RCT results.
The mechanism for the mechanical damage on endothelial cells may include: 1) direct physical contact between the silicone tube and corneal endothelium, 2) turbulence of aqueous fluid flow around the tube, 3) intermittent tube contact with endothelial cells when patients rub their eyes or blink or during different gazes, and/or 4) tube migration over time.7,17,18 One study showed that the distance of the tube tip to the corneal was negatively associated with ECL.19 It has thus been proposed that proximity to the corneal impacts endothelial cell density (ECD). ECL may be reduced or eliminated if the tube can be placed more posteriorly, such as in the vitreous cavity or ciliary sulcus behind the iris. ECL has been compared between tubes placed into the vitreous cavity versus into the AC in both retrospective and prospective comparative studies. Pars plana tube placement resulted in 0–3.5% of ECL at 1-year follow-up, which was significantly less than the 13.1% −14.1% ECL with AC tube during the same follow-up period.20,21 Recently, an interventional study of 211 eyes showed that the mean monthly ECD loss in the sulcus placement group was significantly lower than that in the AC placement group (15.3 cells/mm2 versus 29.3 cells/mm2, P < 0.001).12 There was no increased risk of tube-related postoperative complications when comparing patients who received tube placement in the sulcus (3.8%) versus the AC (4.7%). These complications included tube occlusion, persistent post-operative inflammation, and tube-related exposure/infection. In this and other studies, placement of the tube in the sulcus or vitreous cavity achieved comparable IOP lowering effect as tube placement in the AC.12–15,22
Despite these theoretical advantages and benefits demonstrated in previous clinical studies, sulcus tube placement is currently only chosen by one-third of glaucoma specialists in a published survey from December 2020 in New Zealand and Australia23 and only 10% in this current survey from the AGS. Some possible reasons for this include unfamiliarity with sulcus tube placement, technical difficulty, and concerns about potential complications including intraocular bleeding and tube occlusion with sulcus tube placement. The weight on benefit and risk of sulcus tube placement may explain the disparity between literature knowledge and practice preference. This also provides a possible explanation for about 90% of survey participants who were willing to change their practice if a well-conduct RCT provides solid evidence on tube placement superiority.
Tube placement compromises the blood-aqueous barrier and thus may change the anterior chamber microenvironment. Few studies have been performed evaluating the use of difluprednate after GDD surgery, which theoretically would provide stronger anti-inflammatory control than the commonly used prednisolone acetate. We hypothesize that with the better postoperative inflammatory control, difluprednate may not only prevent ECL but also have the added benefit of less fibrous encapsulation of the GDD, leading to better IOP control. While a recent retrospective study found that postoperative treatment with 0.05% difluprednate after AGV resulted in a similar IOP when difluprednate was used in less frequency than prednisolone 1%,24 a future RCT to evaluate the effect of difluprednate vs prednisolone acetate in GDD is still needed.
This study has several limitations inherent to survey-based research. Firstly, the survey had a low response rate of approximately 8.5%, which may have introduced selection bias. However, not all AGS members routinely access the forum. The non-responders may not have received the survey rather than having been unwilling to participate. Therefore, the reported response rate may underestimate the real rate of response. Because of the anonymous nature of the survey, we could not compare the characteristics of respondents and non-respondents. Secondly, the survey was distributed to AGS members, and the results may not be representative of the larger community of ophthalmologists. Thirdly, the survey relied on self-reported data and was subject to recall bias. Finally, the survey questionnaire used a 4-point scale with more positive response options. Although this enabled us to determine the degree of participants’ positive responses, it may potentially overestimate respondent opinions. Strengths of this survey include the fact that respondents are glaucoma experts who have extensive training and experience and who routinely perform GDD surgery.
Overall, this survey demonstrates that there is considerable interest in assessing outcomes for sulcus tube and AC tube placement as well as different postoperative steroid use, which provide strong support for RCTs assessing the aforementioned techniques for ECL prevention and IOP control amongst glaucoma experts who regularly perform GDD surgery.
Conclusion
The survey results suggest that although protection of sulcus tube on endothelial cells has been suggested by previous retrospective studies, majority of glaucoma specialists continue to preferentially place the tube in the AC in their current practice. There is a strong desire for an RCT to provide convincing evidence regarding the optimal tube placement and post-operative
anti-inflammatory medication use in preventing ECL after GDD surgery. Most critically, this survey suggests that the results of a RCT would improve glaucoma specialists current practice patterns.
Disclosure
Dr Iqbal Ike K Ahmed reports grants, personal fees from Allergan, grants, personal fees from Glaukos, grants, personal fees from Santen, grants, personal fees from Alcon, grants, personal fees from iStar, outside the submitted work. The authors report no conflicts of interest in this work.
References
1. Vajaranant TS, Wu S, Torres M, Varma R. The changing face of primary open-angle glaucoma in the United States: demographic and geographic changes from 2011–2050. Am J Ophthalmol. 2012;154(2):303–314.e3. doi:10.1016/j.ajo.2012.02.024
2. Patel S, Pasquale LR. Glaucoma drainage devices: a review of the past, present, and future. Semin Ophthalmol. 2010;25(5–6):265–270. doi:10.3109/08820538.2010.518840
3. Vinod K, Gedde SJ, Feuer WJ, et al. Practice preferences for glaucoma surgery: a survey of the American glaucoma society. J Glaucoma. 2017;26(8):687–693. doi:10.1097/IJG.0000000000000720
4. Hong CH, Arosemena A, Zurakowski D, Ayyala RS. Glaucoma drainage devices: a systematic literature review and current controversies. Surv Ophthalmol. 2005;50(1):48–60. doi:10.1016/j.survophthal.2004.10.006
5. Gedde SJ, Schiffman JC, Feuer WJ, et al. Treatment outcomes in the Tube Versus Trabeculectomy (TVT) study after five years of follow-up. Am J Ophthalmol. 2012;153(5):789–803.e2. doi:10.1016/j.ajo.2011.10.026
6. Minckler DS, Francis BA, Hodapp EA, et al. Aqueous shunts in glaucoma: a report by the American Academy of Ophthalmology. Ophthalmology. 2008;115(6):1089–1098. doi:10.1016/j.ophtha.2008.03.031
7. Janson BJ, Alward WL, Kwon YH, et al. Glaucoma-associated corneal endothelial cell damage: a review. Surv Ophthalmol. 2018;63(4):500–506. doi:10.1016/j.survophthal.2017.11.002
8. Lee EK, Yun YJ, Lee JE, Yim JH, Kim CS. Changes in corneal endothelial cells after Ahmed glaucoma valve implantation: 2-year follow-up. Am J Ophthalmol. 2009;148(3):361–367. doi:10.1016/j.ajo.2009.04.016
9. Chihara E, Umemoto M, Tanito M. Preservation of corneal endothelium after pars plana tube insertion of the Ahmed glaucoma valve. Jpn J Ophthalmol. 2012;56(2):119–127. doi:10.1007/s10384-011-0108-1
10. Kim KN, Lee SB, Lee YH, Lee JJ, Lim HB, Kim CS. Changes in corneal endothelial cell density and the cumulative risk of corneal decompensation after Ahmed glaucoma valve implantation. Br J Ophthalmol. 2016;100(7):933–938. doi:10.1136/bjophthalmol-2015-306894
11. Nassiri N, Nassiri N, Majdi-N M, et al. Corneal endothelial cell changes after Ahmed valve and Molteno glaucoma implants. Ophthalmic Surg Lasers Imaging. 2011;42(5):394–399. doi:10.3928/15428877-20110812-04
12. Zhang Q, Liu Y, Thanapaisal S, et al. The effect of tube location on corneal endothelial cells in patients with Ahmed glaucoma valve. Ophthalmology. 2021;128(2):218–226. doi:10.1016/j.ophtha.2020.06.050
13. Prata TS, Mehta A, De Moraes CGV, Tello C, Liebmann J, Ritch R. Baerveldt glaucoma implant in the ciliary sulcus: midterm follow-up. J Glaucoma. 2010;19(1):15–18. doi:10.1097/IJG.0b013e3181a2fc2d
14. Weiner A, Cohn AD, Balasubramaniam M, Weiner AJ. Glaucoma tube shunt implantation through the ciliary sulcus in pseudophakic eyes with high risk of corneal decompensation. J Glaucoma. 2010;19(6):405–411. doi:10.1097/IJG.0b013e3181bdb52d
15. Eslami Y, Mohammadi M, Fakhraie G, Zarei R, Moghimi S. Ahmed glaucoma valve implantation with tube insertion through the ciliary sulcus in pseudophakic/aphakic eyes. J Glaucoma. 2014;23(2):115–118. doi:10.1097/IJG.0b013e318265bc0b
16. Bayer A, Önol M. Clinical outcomes of Ahmed glaucoma valve in anterior chamber versus ciliary sulcus. Eye Lond. 2017;31(4):608–614. doi:10.1038/eye.2016.273
17. Topouzis F, Coleman AL, Choplin N, et al. Follow-up of the original cohort with the Ahmed glaucoma valve implant. Am J Ophthalmol. 1999;128(2):198–204. doi:10.1016/s0002-9394(99)00080-x
18. Lopilly Park HY, Jung KI, Park CK. Serial intracameral visualization of the Ahmed glaucoma valve tube by anterior segment optical coherence tomography. Eye Lond. 2012;26(9):1256–1262. doi:10.1038/eye.2012.131
19. Koo EB, Hou J, Han Y, Keenan JD, Stamper RL, Jeng BH. Effect of glaucoma tube shunt parameters on cornea endothelial cells in patients with Ahmed valve implants. Cornea. 2015;34(1):37–41. doi:10.1097/ICO.0000000000000301
20. Iwasaki K, Arimura S, Takihara Y, Takamura Y, Inatani M. Prospective cohort study of corneal endothelial cell loss after Baerveldt glaucoma implantation. PLoS One. 2018;13(7):e0201342. doi:10.1371/journal.pone.0201342
21. Tojo N, Hayashi A, Consolvo-Ueda T, Yanagisawa S. Baerveldt surgery outcomes: anterior chamber insertion versus vitreous cavity insertion. Graefes Arch Clin Exp Ophthalmol. 2018;256(11):2191–2200. doi:10.1007/s00417-018-4116-4
22. Tello C, Espana EM, Mora R, Dorairaj S, Liebmann JM, Ritch R. Baerveldt glaucoma implant insertion in the posterior chamber sulcus. Br J Ophthalmol. 2007;91(6):739–742. doi:10.1136/bjo.2006.107839
23. Lee GA, Craig JE, Liu L, Danesh-Meyer HV. Glaucoma drainage device technique in a cohort of experienced glaucoma surgeons in Australia and New Zealand. J Glaucoma. 2020;29(12):1138–1142. doi:10.1097/IJG.0000000000001662
24. Kao BW, Fong CW, Yu Y, Ying GS, Gedde SJ, Han Y. Surgical outcomes of Ahmed glaucoma valve implantation with postoperative use of prednisolone acetate versus difluprednate. Ophthalmol Glaucoma. 2022. doi:10.1016/j.ogla.2022.03.003
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.