")
Back to Journals » Nature and Science of Sleep » Volume 15
Study on the Sleep Quality Classification and Influencing Factors of Adult ICU Awake Patients Based on Latent Profile Analysis: A Cross-Sectional Survey
Authors Zhang Y , Zhang Y, Teng M, Wang B, Cheng M, Zhong S, Zhang X, Ding X, Liu C, Ma J
Received 14 July 2023
Accepted for publication 19 October 2023
Published 31 October 2023 Volume 2023:15 Pages 861—871
DOI https://doi.org/10.2147/NSS.S430635
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Yanting Zhang,* Yuan Zhang,* Manting Teng,* Bingxue Wang, Miying Cheng, Si Zhong, Xiao Zhang, Xinbo Ding,* Chang Liu,* Jing Ma*
Department of Critical Care Medicine, Zhongnan Hospital of Wuhan University, Clinical Research Center of Hubei Critical Care Medicine, Wuhan, 430071, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jing Ma, Department of Critical Care Medicine, Zhongnan Hospital of Wuhan University, Clinical Research Center of Hubei Critical Care Medicine, Wuhan, 430071, People’s Republic of China, Email [email protected]
Objective: To explore the potential category characteristics of sleep quality in conscious adult patients in the intensive care unit (ICU) and to analyze the differences in characteristics of different categories of conscious adult patients in the ICU.
Methods: From 5/4/2023 to 30/6/2023, we selected ICU patients of a Class iii Grade A hospital in Wuhan as subjects by simple random sampling. The general information questionnaire, Acute Physiology and Chronic Health Evaluation II, Numerical Rating Scale (NRS)/Critical Care Pain Observation Tool (CPOT) and Richards-Campbell Sleep Questionnaire (RCSQ) were used for investigation. To analyze the latent profile of sleep quality characteristics of adult ICU awake patients and to identify the influencing factors of the latent profile through univariate analysis and logistic regression analysis.
Results: A total of 298 awake ICU patients were investigated. There were three potential profiles of sleep quality characteristics, namely “low sleep quality” type (16.31%), “medium sleep quality” type (52.11%), and “high sleep quality” type (31.57%). Logistic regression analysis showed that age (36– 60), disease type admitted to ICU, oxygen administration method, CPOT or NRS score, postoperative or not, use of analgesic drugs or not, and use of sleep-promoting drugs or not were the factors affecting the sleep quality of adult ICU awake patients (P < 0.05).
Conclusion: The sleep quality of adult ICU awake patients has obvious classification characteristics. Health professionals can carry out individualized interventions according to the influencing factors of different potential profiles to improve the sleep quality of adult ICU awake patients.
Keywords: ICU patients, sleep quality, sleep disorders, latent profile analysis, influencing factors
Introduction
Intensive Care Unit (ICU) patients are a special group with severe, complex illnesses and widespread sleep problems. Poor sleep quality is associated with associated susceptibility to diseases resulting from impaired immune function, decreased energy levels, confusion, delayed recovery, and impaired cognitive, respiratory, heart, and endocrine functions. It has been reported that sleep disorders in critically ill patients account for more than 50%, and sleep disorders in ICU patients are closely related to mortality, infection rates, and complications.1 Critically ill patients in the ICU are exposed to disturbed daily routines, high levels of noise (eg, staff conversations and alarms) and all-night light, invasive procedures, noxious odors, extensive physical restraint, and disease-related stress both day and night.2 Studies have reported that patients in the ICU often have problems with reduced sleep quality and duration, recurrent arousals, and circadian rhythm disturbances.1,3 However, most of the relevant studies are carried out on the population, ignoring the interaction of different individual levels, resulting in the lack of pertinence of the existing research results in guiding the individualized improvement of sleep quality in adult ICU awake patients, resulting in unsatisfactory intervention effects and waste of medical resources.
At present, sleep assessment is divided into objective sleep assessment and subjective sleep assessment. Objective sleep assessment methods include Polysomnography (PSG), bispectral index, actigraphy and endogenous melatonin measurement. However, these objective sleep assessment methods are difficult to be popularized in ICU due to the high cost of instruments or materials and high technical requirements. PSG is the “gold standard” for sleep assessment. Subjective sleep assessment includes patient self-assessment questionnaire and assessment by others using questionnaire or observation,4 and the Richards Campbell Sleep Questionnaire (RCSQ), which is specifically designed for sleep assessment of awake patients in ICU, is used to evaluate sleep quality. Often relying on specific cut-off points of the scale to roughly classify subjects as “good sleep” or “poor sleep”, although practical, may fail to identify heterogeneity of the group.5 Therefore, this study used the individual-centered latent variable method to find the optimal classification model for sleep quality of adult ICU awake patients.
The traditional Latent Class Analysis (LCA) needs to convert the original score into the 0/1 category according to a critical standard, and then carry out follow-up analysis. In this process, some data information may be lost and the results may be biased. Latent Profile Analysis (LPA), as an individualized classification technique of research objects, is an extension of LCA, which can deal with observation data such as multi-point score or continuous variables to make more full and accurate use of data information.6 In this study, the RCSQ, an assessment tool for sleep quality in adult ICU awake patients, used 0–100 mm visual analogue scale. The higher the comprehensive score, the better the patient’s sleep quality, which is a continuous variable; therefore, this study intends to explore the latent classification of sleep quality in adult ICU awake patients using LPA, so as to analyze whether there is population heterogeneity in sleep quality of adult ICU awake patients and to explore the effects of demographic variables and related disease variables on different latent profiles. It is expected to provide targeted intervention measures for adult ICU awake patients with different sleep potential profiles, which is the maximum intervention now, and provide a more reasonable and scientific basis for effectively improving the sleep quality of adult ICU awake patients.
Study Design
This was an observational study.
The structure of the ICU at the study site is: a total of 16 beds, all of which are open spaces and no separate wards. Turn off the ICU space lighting at 11 o’clock every night and control the volume (instrument alarm and health professionals speaking volume). In this study, a simple random sampling method was used to select patients who were hospitalized in the general ICU of a tertiary hospital in Wuhan from April 5, 2023 to June 30, 2023, and collected data through questionnaires.
According to the results of previous studies,7 the average incidence of sleep disorders in adult ICU awake patients was calculated to be 50%, the allowable error was 6%, and the confidence was 1-α=0.95. The sample size to be investigated was calculated to be 267 cases. Considering 10% unqualified questionnaires, the sample size was 267–293.
Objects and Methods
Subjects
Inclusion criteria: ① Age ≥18 years old; ② The length of stay in ICU ≥1 night, the admission of awake patients to ICU no later than 10PM, and the extubation time of intubated patients no later than 10PM; ③ Awareness is clear. Exclusion criteria: ① long-term use of hypnotics and other hypnotics outside the hospital; ② cognitive and mental disorders; ③ with mental illness; ④ patients with delirium. All subjects gave informed consent and voluntarily participated in this study.
Survey Tools
General Information Questionnaire
Through a review of the literature, it was found that Jiang et al8 conducted a systematic evaluation of the risk factors for sleep disorder in patients awake in the ICU and found that environmental factors (equipment noise, nursing staff conversation, patient noise, light), treatment factors (night treatment, mechanical ventilation), disease factors (disease itself and drug effects, pain, and changes in comfort), and psychological factors (anxiety, visiting time, financial burden) all affected the sleep quality of ICU conscious patients. Our research team combined with literature review data and solicited the opinions of clinical and nursing experts to jointly design the general information questionnaire for adult ICU awake patients, including demographic data and disease-related data. Among them, the demographic data includes the age, gender, education level, type of medical insurance, marital status, etc., of adult ICU awake patients; disease-related information includes clinical diagnosis at the time of ICU admission, whether it is postoperative, number of tubes carried, oxygen administration, disease severity, pain score, use of analgesic drugs, and use of sleep-promoting drugs.
Acute Physiology and Chronic Health Evaluation II
Acute Physiology and Chronic Health Evaluation II (APACHE-II) is an objective system for evaluating the severity and predicting the prognosis of all kinds of critical patients, especially conscious patients in ICU. It is the most widely used and authoritative scoring method in the world. In 1981, the American Critical Illness Scoring Research group led by Knaus9 proposed the prototype of APACHE, namely APACHE-I system. After further refinement and improvement, a modified version was proposed in 1985, namely the APACHE-II system, which is currently the most widely used critical illness scoring system in China. The APACHEII scoring standard consists of three parts, namely acute physiology score (APS), age score, and chronic health status score, with a total score of 3, and the highest theoretical score is 71. In the comprehensive ICU, the score of APACHE-II is positively correlated with the severity of the disease to a certain extent, and the higher the score, the higher the risk of death,10 and the more severe the disease. In our study, the score was assessed by ICU clinicians during the first 24 hours of ICU admission.
Numerical Rating Scale for Pain
The Numerical Rating Scale (NRS) is accurate and simplicity, and it has been regarded as the gold standard for pain assessment by the American Pain Society. NRS of pain was used to represent different degrees of pain (0 = painless, 10 = severe pain), 0–3 is mild pain, 4–6 is moderate pain, and >6 is severe pain.11 It is up to the patient to choose different scores to quantify the degree of pain, with higher scores indicating greater pain intensity. NRS is often used to test pain intensity or report average pain intensity over the past 24 hours.12 The classification of NRS of pain is clear and objective, which can help patients make more accurate assessment, thereby improving the comparability of assessment between different patients. NRS of pain requires patients to have the ability of abstract scale understanding, as well as certain reading comprehension ability. Therefore, NRS of pain is more suitable for patients over 10 years old with a certain degree of education. In this study, NRS of pain scale was primarily used in patients who could communicate and express themselves autonomously.13
Critical Care Pain Observation Tool
The Critical Care Pain Observation Tool (CPOT) was originally developed from the Behavioral Pain Scale (BPS) designed by the French and later translated into English.14 From 2002 to 2003, Gelinas et al developed and improved the CPOT scale by referring to existing assessment scales and work experience.15 In 2007, Gelinas and Johnston provided the measurement quality of CPOT with a reliability of 0.80 to 0.93. The CPOT value of 3 is the critical score, with a sensitivity of 66.7% and a specificity of 83.3%, which is concise, easy to operate, and takes less time to meet the work requirements of ICU.16 The COPT scale includes four parts of behavioral indicators: facial expression, movement, muscle tone, compliance with mechanical ventilation in patients with endotracheal intubation or pronunciation in non-intubated patients. Each indicator is scored 0~2, and the total score is 0~8. A score of 0 represents painless and a score of 8 represents the most pain. In this study, the CPOT pain assessment scale was used in patients who could not communicate verbally but had somatic motor function and behavior that could be observed, such as awake patients with endotracheal intubation.
Richards-Campbell Sleep Scale
Richards-Campbell Sleep Questionnaire (RCSQ) was developed by American nursing expert Richards17 in 2000, which was mainly used to measure the sleep quality of patients in ICU. The scale was composed of 5 items, and the 0–100 mm visual analogue scoring method was used to measure the sleep status of patients from five aspects: sleep depth, difficulty in falling asleep, number of awakenings, difficulty in falling asleep and overall sleep quality. The leftmost end of the line is 100 points, which representing good sleep. The rightmost end of the line is 0 points, representing poor sleep. When measuring, the patient selected a position on the line that could represent the degree of sleep previous night, and the distance from the crossed point to the rightmost end of the line is measured using a ruler to record the patient’s score. The patient’s RCSQ sleep score was the average of five items, with higher scores indicating better sleep. This study adopted the Chinese version of RCSQ translated by Yang Hui18 et al in 2016, the content validity was 0.840, Cronbach’s α coefficient was 0.874, and the test–retest reliability was 0.912.
Data Collection Methods and Quality Control
Before completing the questionnaire, trained study group members were introduced to the purpose and significance of the survey using uniform instructional language. When the study subject cannot complete it in person due to physical limitations or language limitations, the night shift nurse will complete it in place, but it is necessary to communicate with the patient on the spot and fill in according to the actual sleep of the patient, and the questionnaire can be completed at 7am on the second day. Collect the questionnaire on the spot and check whether there are any missing items on the spot, and if so, please complete the research object in time.
Statistical Methods
The data were entered and checked by two people to ensure the accuracy of the study data. The measurement data conforming to normal distribution were described by mean ± standard deviation. Frequency and percentage were used to describe the count data or grade data. Mplus8.3 software was used to classify the sleep quality of adult ICU awake patients with different scores by exploratory latent profile analysis. Compare the difference between the expected value and the actual value by Pearson chi-square test, likelihood ratio chi-square test, Akaike information criterion (AIC), Bayesian information criterion (BIC) and sample size adjusted BIC (aBIC) to judge the model fit. Smaller values indicate better fit; bootstrap’s likelihood ratio test (BLRT) and Lo-Mendell-Rubin (LMR) are used to compare the fitting differences of each model, that is, to compare the fitting differences between K-1 class and K class models, and when the difference is statistically significant (P < 0.05), it shows that the model of K profiles is better than the model of K-1 profile, where K is the number of parameters freely estimated.19 The closer the information entropy value is to 1, the more accurate the classification.
According to the results of latent profile analysis, the best classification model for sleep quality of adult ICU awake patients was determined. SPSS 23.0 statistical software was used to analyze the differences in the distribution of different sleep types by X2 test or Fisher’s exact probability method. Wilcoxon and Kruskal–Wallis rank sum tests were used to compare the differences in general demographic data and disease-related factors of different categories of sleep quality in adult ICU awake patients. Using disordered multi-classification logistic regression, the potential category of sleep quality of adult ICU awake patients was used as the dependent variable, and the factors with significant differences in univariate analysis results were used as independent variables, and the influencing factors of different potential categories of sleep quality in adult ICU awake patients were discussed in depth, and the difference was statistically significant with P < 0.05.
Ethic
This study complied with the basic principles of the Declaration of Helsinki, and all patients signed informed consent. And this study was approved by the Ethics Committee of Zhongnan Hospital, Wuhan University ([2023023K]).
Results
General Information of the Subjects
In this study, a total of 309 questionnaires were distributed and 298 valid questionnaires were returned, and the effective questionnaire recovery rate was 96.44%. The age of the subjects was 18–87 (52.53 ± 17.39) years old, the number of tubes was 2–9 (4.07 ± 1.49), and the APACHE-II score was 2–27 (10.86 ± 4.76). Other general demographic and disease data are provided in Table 1.
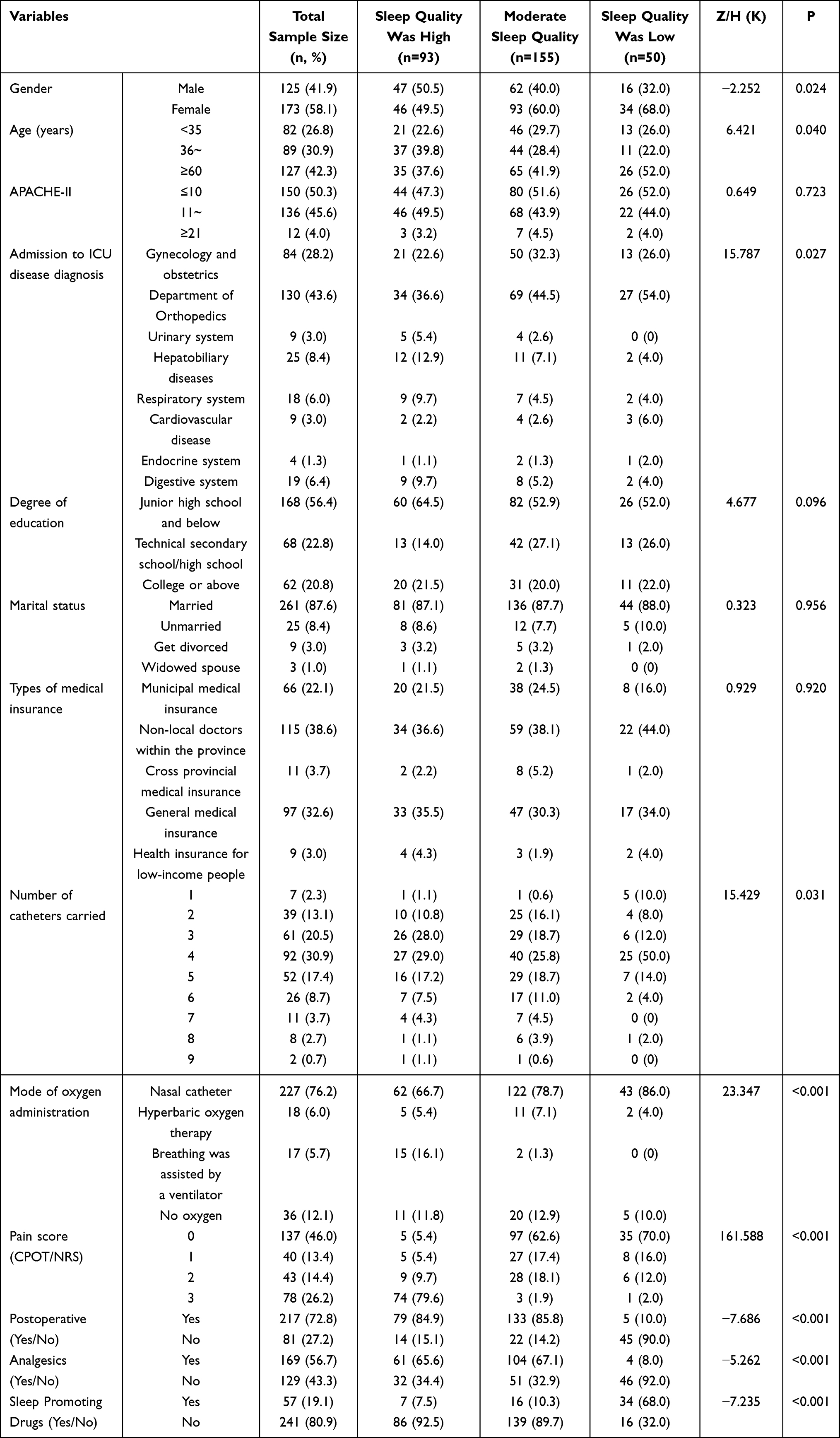 |
Table 1 General Data of Adult ICU Awake Patients and Univariate Analysis of Their Potential Categories of Sleep Quality (n=298, %) |
Latent Profile Analysis results and Naming of Sleep Quality of Adult ICU Awake Patients
The RCSQ scores of 298 adult ICU patients were sleep depth (68.070 ± 25.93), difficulty in falling asleep (68.104 ± 27.99), number of awakening frequency (58.893 ± 26.85), difficulty in falling asleep again (66.409 ± 29.02) and overall sleep quality (69.305 ± 26.66). According to the evaluation results of RCSQ sleep quality in adult ICU patients, a total of 5 latent class models were fitted in this study, and the fitting indicators of each model are shown in Table 2. As the number of model classifications increased, the values of AIC, BIC, and aBIC decreased continuously. For four categories, the P > 0.05 of LMR. The Entropy is closest to 1 when there are 5 categories, but the P result of LMR is not as good as that of 3 categories, and Yang20 found that only when the average sample size of each section reaches 50 can robust statistical analysis results be obtained. Therefore, combined with the interpretation of results and the practical significance of the study, three potential categories were selected as the optimal model in this study. Discriminant analysis was used to verify the accuracy of the optimal model of the latent profile analysis, and the results of the average posterior probability were all above 95%, indicating that the optimal model obtained by the latent profile analysis in this study was reliable and had high discriminative power.
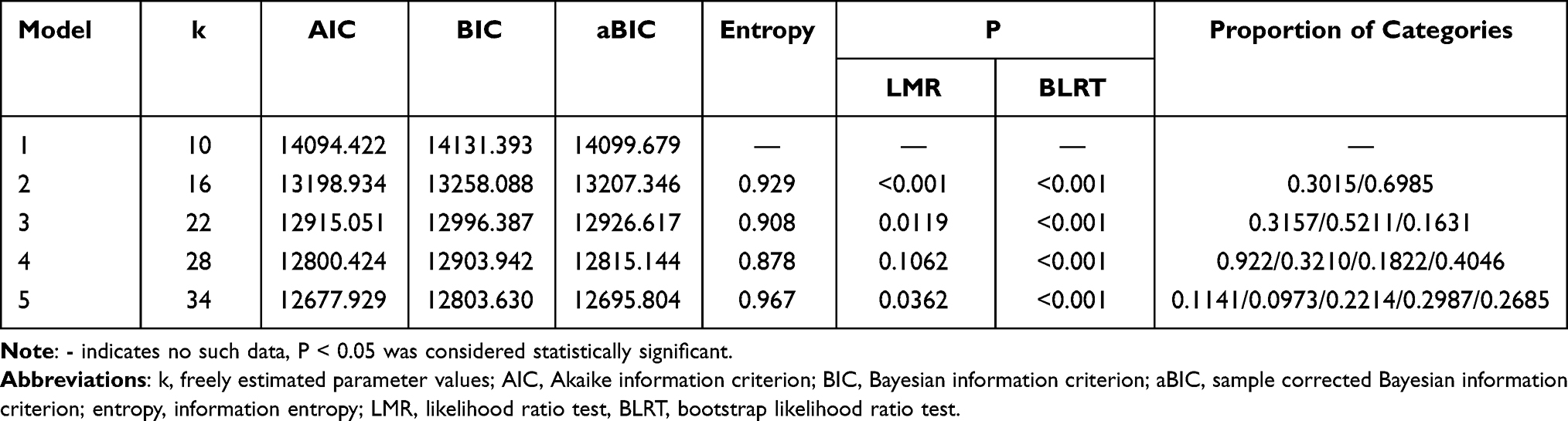 |
Table 2 Comparison of Fit Parameter Indices of Different Latent Profile Models (n = 298) |
Based on model 3, line plots of each RCSQ item score were obtained according to its feature distribution, as shown in Figure 1. According to the fluctuation of the average line chart of each item, the characteristic attributes of each category were named. The item score of C1 category was between C2 and C3, indicating that the sleep quality of this type of patients was medium, and the group was named “medium sleep quality”, accounting for 52.11% (155/298). The overall score level of C2 category was higher, indicating that the patients in this category had higher sleep quality, which was named as the “high sleep quality” group, accounting for 31.57% (93/298). The overall score level of C3 category was low, indicating that the sleep quality of these patients was low, which was named as the “poor sleep quality” group, accounting for 16.31% (50/298).
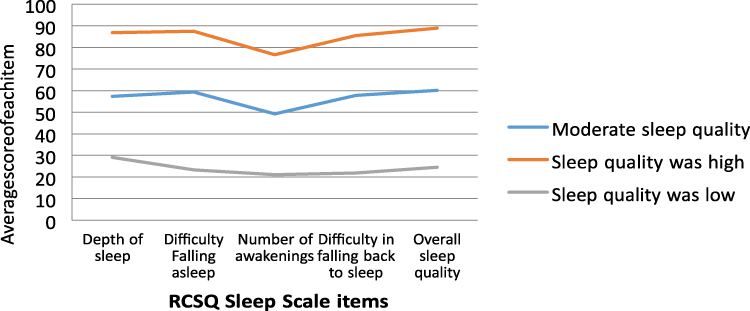 |
Figure 1 Distribution of three latent class characteristics of sleep quality in adult ICU awake patients. |
Univariate Analysis of Potential Categories of Sleep Quality in Adult ICU Awake Patients
The results of univariate analysis showed that the differences in gender, age, type of ICU admission, number of catheters carried, oxygen mode, CPOT or NRS score, postoperative period, analgesic drugs, and sleep stimulating drugs were statistically significant (P < 0.05), as shown in Table 1.
Multivariate Analysis of Potential Categories of Sleep Quality in Adult ICU Awake Patients
Taking the latent profile category of sleep quality of adult ICU awake patients as the dependent variable (“C1 class moderate sleep quality” group as the reference) and the statistically significant factors in the univariate analysis as the independent variables, the unordered multi-classification logistic regression model was constructed for multivariate analysis. Since the unordered multinomial logistic regression automatically performs the comparison of categorical data, there is no need to set dummy variables. The assignment of each variable is shown in Table 3.
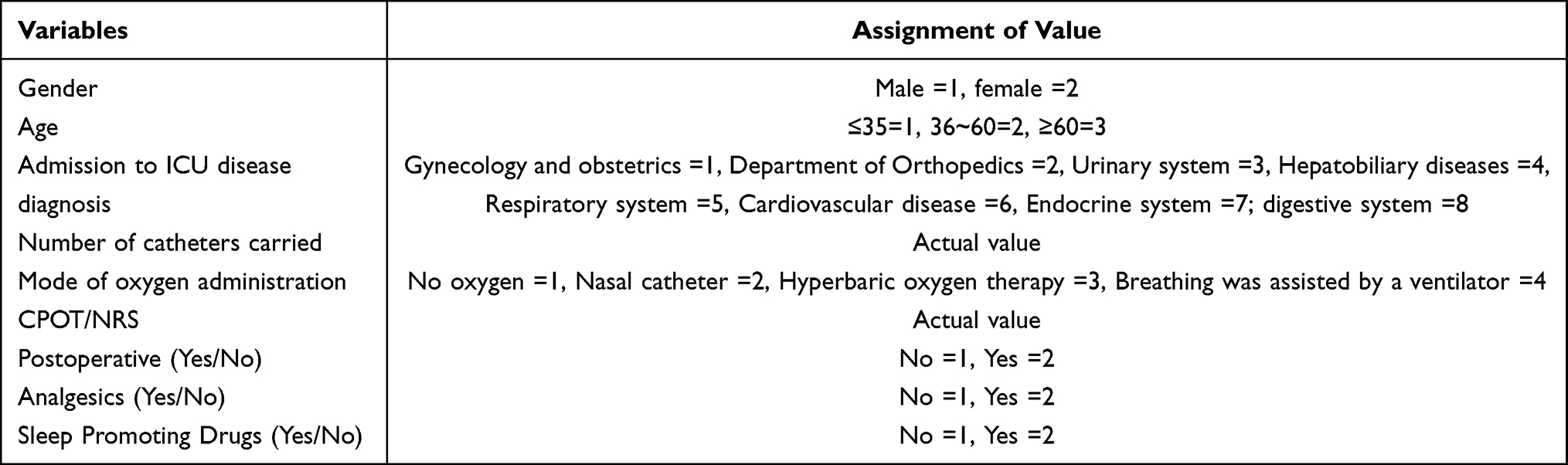 |
Table 3 Assignment Table for Unordered Multinomial Logistic Regression Analysis of Potential Category Influencing Factors of Sleep Quality in Adult ICU Awake Patients |
The results of logistic regression analysis showed that age (36–60, P = 0.042), CPOT OR NRS score (P < 0.001) were the influencing factors of high sleep quality, and the OR were (0.353, 95% CI: 0.129–0.963) and (0.130, 95% CI: 0.080–0.211), respectively. Age and pain score had a negative effect on the “high sleep quality” group, that is, the younger the age and the lower the pain score, the higher the sleep quality of the patients.
Age (36–60, P = 0.031), type of disease admitted to ICU, oxygen administration method, CPOT or NRS score, postoperative or not, use of analgesics or not, use of sleep-promoting drugs or not were the influencing factors of poor sleep quality group (P < 0.05). The lower the age, the more complex the way of oxygen inhalation, the higher the pain score, the postoperative patients, and the patients who did not use analgesics or sleep-promoting drugs had lower sleep quality, as shown in Table 4.
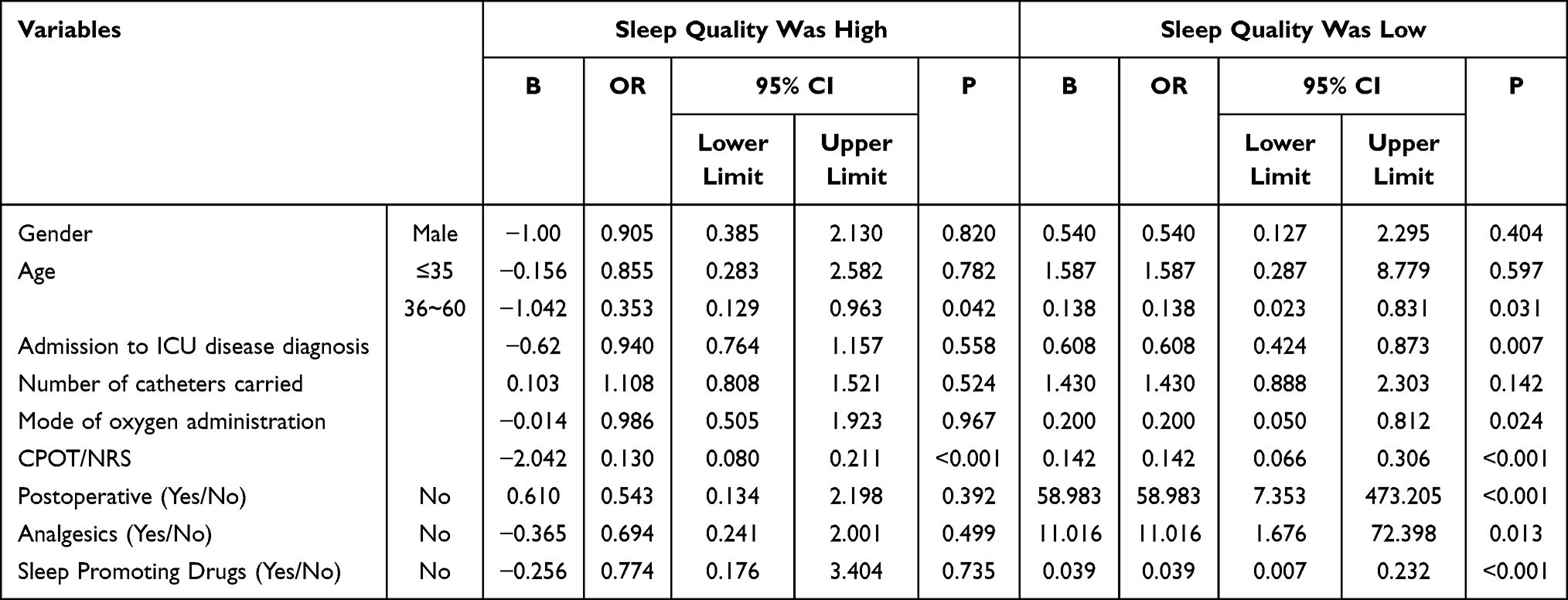 |
Table 4 Multivariate Analysis of Potential Categories of Sleep Quality in Adult ICU Awake Patients |
Discussion
The Sleep Quality of Adult ICU Awake Patients is Generally at a Moderate Level and There is Population Heterogeneity in Sleep Characteristics
In this study, the overall sleep quality score of RCSQ in adult awake patients in ICU was (69.305±26.66), which was at a medium level, and the score of difficulty in falling asleep was (68.104±27.99), and the score of difficulty in falling asleep again was (66.409±29.02), which was relatively high. It shows that sleep disorders are common in adult ICU awake patients, which is similar to the results of the study (49.05 ±18.86) of Li et al.21 Moreover, the study results of Bao22 et al showed that 42.69% of patients had moderate sleep quality, which was consistent with the results of this study (52.11%). Due to the special treatment environment of ICU, patients have psychological pressure, and their sleep problems are often ignored by the nurses.23 Therefore, health professionals should pay great attention to the sleep management of patients.
In this study, through latent profile analysis, we found that there were significant individual differences in sleep quality among adult awake patients of ICU, which were identified into three latent categories, named as “poor sleep quality”, “medium sleep quality”, and “high sleep quality”. ① The “poor sleep quality” group accounted for 16.31%, and the score of each item was below 30 score and the line chart performance was relatively flat. The main characteristics of this category of patients were shallow sleep depth, difficulty falling asleep, more awakening times, difficulty re-falling asleep and low overall sleep quality. Analysis of the reasons may be related to the unfamiliar environment of ICU. In this study, through potential cross-sectional analysis, it was found that there were significant individual differences in sleep quality in adult ICU awake patients, which were identified into three potential categories, named “low sleep quality”, “moderate sleep quality” and “high sleep quality”. (1) “Low sleep quality” type, accounting for 16.31%, the scores of each item were below 30 points and the line chart performance was relatively flat, and patients in this category were mainly characterized by shallow sleep depth, difficulty falling asleep, many awakenings, difficulty re-falling asleep and low overall sleep quality. The reasons for the analysis may be related to the unfamiliar environment of the ICU, the patient’s adaptive ability, and the disease. Therefore, for such patients, the causes and influencing factors of sleep disorders should be actively clarified, and targeted non-drug interventions should be carried out as soon as possible, such as prolonging sleep time through light therapy and mind-body exercise, reducing the number and time of wakefulness, and improving sleep quality.24 ②medium sleep quality group accounting for 52.11%. The RCSQ score of these patients was between 50 ~ 60, which was at the middle level. However, the scores of difficulty in falling asleep and re-sleeping after awakening remained high. Awake adult ICU patients with “medium sleep quality” may be the main type of sleep disorders. ③ The “high sleep quality” group accounted for 31.57%. Figure 1 shows that the scores of each item of RCSQ in this category of patients were between 75 ~ 90, which is at a high level. However, the characteristics of these patients are the same as those of the C1, C2 categories of patients, and the scores of difficulty falling asleep and re-falling asleep after awakening are still high, and sleep disturbances remain. The results of this study show that there are obvious categorical characteristics of sleep quality in adult ICU awake patients, suggesting that health professionals must recognize the differences between the nursing needs of different categories of patients and incorporate effective resources and interventions into treatment plans to improve sleep quality of adult ICU awake patients.
The Distribution Characteristics of ICU Awake Patients with Different Sleep Quality Types Were Significantly Different
Although the patient’s general profile and disease-related information are not easy to intervene, understanding the differences among patients with different sleep quality types can help health professionals identify them early. The results of univariate analysis of this study showed that there were differences in gender, age, disease type in ICU, number of catheters, oxygen administration method, CPOT or NRS score, postoperative or not, use of analgesics and use of sleep-promoting drugs among adult ICU awake patients with different sleep quality types, and the older the age, the worse the sleep quality of the patients. This is different from the studies of Chen et al4 and Li et al,21 which may be related to the fact that our study did not include the noise factor and the definition of the research object was different. The noise variable was not included because it was routine to provide earplugs during our daily nursing, and we will ask patients at bedtime if they need them and provide them in a timely manner. However, the above variables did not all enter the final logistic regression, which may be related to the small sample size of the “high sleep quality” group and the “poor sleep quality” group in our study. Future studies can expand the sample size to further verify the influence of the above factors on the categories of adult ICU awake patients.
There are Many Influencing Factors for ICU Awake Patients with “Poor Sleep Quality”, and Targeted Interventions Should Be Taken
The results of logistic regression analysis showed that age (36–60), CPOT or NRS score were the influencing factors of “high sleep quality”. Age (36–60), type of ICU admission, oxygen administration method, CPOT or NRS score, postoperative or not, use of analgesic drugs or not, use of sleep-promoting drugs were the influencing factors of “poor sleep quality” group. This is consistent with the results of previous studies.1,2 Among the influencing factors of age, only the 36–60 years old age group is the influencing factor of adult ICU awake patients, which may be because the psychology of this age group is more stressful than that of the elderly, and most of them are transferred to ICU after surgery, which has a greater impact on sleep of these patients due to objective reasons such as pain. In addition, compared with the “medium sleep quality” group, the patients who were not transferred to ICU after surgery did not use analgesics, and sleep-promoting drugs were more likely to belong to the “poor sleep quality” group. The type of disease admitted to ICU, oxygen administration method, CPOT or NRS score were important predictors of “poor sleep quality”. Therefore, health professionals should attach great importance to the sleep problems of ICU patients in clinical work, conduct correct and timely assessment, and give effective targeted and personalized interventions to improve the sleep quality of patients, such as standardized pain management, drug intervention when necessary, and timely handling of instrument alarms. However, drug intervention is costly and prone to side effects. Non-drug intervention has the advantages of less adverse reactions, low cost and strong operability, and has been recognized by health professionals and patients.25 And studies have shown that26 non-pharmacological interventions can improve patients’ sleep well.
Conclusions
This study found that the sleep quality of adult ICU awake patients was generally at a medium level. Three categories were identified by latent profile analysis, which confirmed that there was obvious group heterogeneity in the sleep quality of adult ICU awake patients. It is suggested that health professionals should take targeted intervention measures according to different types of patients’ sleep quality and different influencing factors in the process of clinical practice.
Limitations and Prospects of This Study
This study has certain limitations: this study is an observational survey and cannot be inferred the causal relationship between the sleep quality of awake ICU patients and the patient’s diagnosis. This study is the first to use latent profile analysis to classify the sleep quality of adult ICU awake patients at an individual level and name it based on the trend of latent profile analysis charts, and the appropriateness of this name needs to be further explored. In addition, this study was a single-center study. On the one hand, future studies should expand the sample of survey subjects and carry out multi-center studies, longitudinally analyze the association between sleep disorders and disease diagnosis in adult ICU patients and explore its causal relationship. On the other hand, objective assessment tools can be used to assess the sleep characteristics of adult ICU awake patients to improve the accuracy of sleep potential classification, further verify the conclusions of this study, and lay the foundation for the construction of targeted intervention programs for different classifications of sleep quality in adult patients with awake ICU.
Through the profile analysis of sleep quality of adult ICU awake patients, targeted interventions can be taken for these patients according to different types of sleep quality, so as to reduce the incidence of sleep disorders in ICU awake patients, improve their sleep quality, and further reduce the incidence of delirium in ICU patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Clinical Nursing Research Program of Zhongnan Hospital of Wuhan University in 2022 (LCHLYJ202210).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang CY, Shang M, Feng LZ., et al. Correlation between APACHE III score and sleep quality in ICU patients. J Int Med Res. 2019;47(8):3670–3680. doi:10.1177/0300060519856745
2. Stewart JA, Green C, Stewart J, et al. Factors influencing quality of sleep among non-mechanically ventilated patients in the intensive care unit. Aust Crit Care. 2017;30(2):85–90. doi:10.1016/j.aucc.2016.02.002
3. Alsulami G, Rice AM, Kidd L. Prospective repeated assessment of self-reported sleep quality and sleep disruptive factors in the intensive care unit: acceptability of daily assessment of sleep quality. BMJ Open. 2019;9(6):e029957. doi:10.1136/bmjopen-2019-029957
4. Chen LX, Ji DH, Pei JH, et al. Research progress of sleep assessment in ICU awake patients. Chin Nurs Manage. 2015;15(12):1522–1525.
5. Walrath C, Petras H, Mandell DS, et al. Gender differences in patterns of risk factors among children receiving mental health services:Latent class analyses. J Behav Health Serv Res. 2004;31(3):297–311.
6. Bin Y, zhang JT, Yu CF, et al. Identification of psychological and behavioral problems in college students: based on latent profile analysis. Psychol Dev Educ. 2015;31(3):350–359.
7. Pisanim A, Friese RS, Gehlbach BK, et al. Sleep in the intensive care unit. Am J Respir Crit Care Med. 2015;191(7):731–738. doi:10.1164/rccm.201411-2099CI
8. Jiang LJ, Han LL, Yang LP, et al. Systematic review of risk factors for sleep disorders in awake ICU patients. Chin J Evid Based Med. 2019;19(7):803–810.
9. Knaus WA, Zimmerman JE, Wagner DP, et al. APACHE—acute physiology and chronic health evaluation: a physiologically based classification system. Crit Care Med. 1981;9(8):591–597. doi:10.1097/00003246-198108000-00008
10. Jiang XC. Clinical application and significance of critical illness severity score. Chin J Emerg Med. 2000;12(4):195–197.
11. Wang SH. Clinical Nursing Evaluation Scale and Its Application. Changsha: Hunan Science and Technology Press; 2011:150–151.
12. Dworkjn RH, Turk DC, Famr JT, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005;1(13):9–19. doi:10.1016/j.pain.2004.09.012
13. Zhang YK, Wang YW, Wang S, et al. Summary of the best evidence for pain management in adult ICU conscious patients. Chin J Nurs. 2021;28(11):40–45. doi:10.16460/j.isn1008-9969.2021.11.040
14. Geélinas C, Johnston C. Pain assessment in the critically ill ventilated adult: validation of the critical-care pain observation tool and physiologic indicators. Clin J Pain. 2007;23(6):497–505. doi:10.1097/AJP.0b013e31806a23fb
15. Shannon K, Bucknall T. Pain assessment in critical care: what have we learnt from research. Intensive Crit Care Nurs. 2009;19(3):154–162. doi:10.1016/S0964-3397(03)00027-2
16. Wang F, Xu ZH, Huang QH, et al. Research progress of pain observation tools for critical patients. Chin J Mod Nurs. 2013;19(11):1349–1350. doi:10.3760/cma.j.issn.1674-2907.2013.11.041
17. Richards KC, O’SulliVaIl PS, Phjllips RL. Measurement of sleep in critically ill patients. J Nurs Meas. 2000;8(2):13l–144. doi:10.1891/1061-3749.8.2.131
18. Yang H, Sun DD, Li ZZ, et al. Reliability and validity of the Chinese version of Richards-Campbell sleep questionnaire in awake patients in ICU. Chin Nurs Manage. 2017;17(5):601–604. doi:10.3969/j.issn.1672-1756.2017.05.008
19. Wang MC, Bi XY. Latent Variable Modeling and Mplus Application: An Advanced Chapter. Chongqing: Chongqing University Press; 2018:13–15.
20. Yang CC. Evaluating latent class analysis models in qualitative phenotype identification. Comput Stat Data Anal. 2006;50(4):1090–1104. doi:10.1016/j.csda.2004.11.004
21. Li JJ, Pan WY, Wang XR, et al. Current status and influencing factors of sleep quality in ICU awake patients. Qilu J Nurs. 2020;26(1):1–4. in Chinese. doi:10.3969/j.issn.1006-7256.2020.01.001
22. Bao J. Sleep quality and its influencing factors in ICU awake patients. World J Sleep Med. 2018;5(11):1348–1350.
23. Nesbitt L, Goode D. Nurses perceptions of sleep in the intensive care unit environment: a literature review. Intens Crit Care Nurs. 2014;30(4):231235. doi:10.1016/j.iccn.2013.12.005
24. Gong MJ, Tan SJ, Sun YQ, et al. Meta-analysis of exercise intervention on sleep structure in adults with sleep disorders. J Capital Instit Physi Educ. 2021;33(3):276–284. in Chinese. doi:10.14036/j.cnki.cn11-4513.2021.03.006
25. Lan Y, Wu X, Tan HJ, et al. Auricular acupuncture with seed or pellet attachments for primary insomnia: a systematic review and meta-analysis. BMC Comple Altem Med. 2015;15(1):103. doi:10.1186/s12906-015-0606-7
26. Hauri PJ. Can we mix behavioral therapy with hypnotics when treating insomniacs? Sleep. 1997;20(12):1111–1118. doi:10.1093/sleep/20.12.1111
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.