")
Back to Journals » Nature and Science of Sleep » Volume 15
Sleep and Pain in Veterans with Chronic Pain: Effects of Psychological Pain Treatment and Temporal Associations
Authors Wilson M , Skeiky L, Muck RA , Miller MA, Hansen DA , Williams RM , Jensen MP , Van Dongen HPA
Received 18 July 2023
Accepted for publication 26 November 2023
Published 19 December 2023 Volume 2023:15 Pages 1061—1077
DOI https://doi.org/10.2147/NSS.S418532
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Marian Wilson,1,2,* Lillian Skeiky,2,3,* Rachael A Muck,2,3 Megan A Miller,4 Devon A Hansen,2,3 Rhonda M Williams,4,5 Mark P Jensen,5 Hans PA Van Dongen2,3
1College of Nursing, Washington State University, Spokane, WA, USA; 2Sleep and Performance Research Center, Washington State University, Spokane, WA, USA; 3Department of Translational Medicine and Physiology, Washington State University, Spokane, WA, USA; 4Rehabilitation Care Service, VA Puget Sound Health Care System, Seattle, WA, USA; 5Department of Rehabilitation Medicine, University of Washington, Seattle, WA, USA
*These authors contributed equally to this work
Correspondence: Marian Wilson, College of Nursing, Washington State University, 103 E. Spokane Falls Blvd, Spokane, WA, 99202, USA, Tel +1 509 324 7443, Email [email protected]
Introduction: Chronic pain is highly prevalent in US military Veterans. Non-opioid and non-pharmacologic treatments are recommended when clinically appropriate, but research on the mechanisms underlying benefits of these treatments is lacking. Here, we examined the role of sleep in the effects of three non-pharmacologic pain treatments in Veterans. Specifically, we investigated whether treatment effects on sleep predicted treatment effects on pain occurring later, or vice versa.
Methods: Veterans enrolled in a randomized controlled trial were invited to participate in this supplementary sleep study. A total of 174 Veterans were randomized to one of three 8-session, in-person, group-based pain treatments: hypnosis, mindfulness meditation, or education control. Measurements included self-reported sleep disturbance, pain intensity, and pain catastrophizing; sleep duration was assessed with actigraphy. Sleep and pain measurements were obtained at baseline, posttreatment, and 3-month posttreatment follow-up.
Results: At baseline, average pain intensity was moderate (mean ± SD: 5.7 ± 1.7 on the 0– 10 Numeric Rating Scale), pain catastrophizing was just below the clinically relevant threshold (mean ± SD: 28.6 ± 12.2 on the Pain Catastrophizing Scale), and subjective sleep disturbance exceeded the US population average (mean ± SD: 58.5 ± 8.1 on the Patient Reported Outcomes Measurement Information System Sleep Disturbance – Short Form). By contrast, objective sleep duration was consistent with the recommended daily sleep amount of 7– 8 h for adults (mean ± SD: 8.3 ± 1.4 h). Across treatment conditions, pain intensity, pain catastrophizing, and subjective sleep disturbance were significantly less at posttreatment and 3-month follow-up than at baseline (p < 0.001). Actigraphic sleep duration did not differ significantly as a function of time. There was a high degree of covariation among the measures of pain intensity, pain catastrophizing, and sleep disturbance (p < 0.05). However, self-reported sleep disturbance was not significantly correlated with actigraphic sleep duration (|r| <= 0.13, p > 0.05). Sleep and pain variables observed at prior assessments predicted these same variables at subsequent assessments. There was no significant evidence that changes in pain preceded changes in sleep or that changes in sleep preceded changes in pain (all p > 0.05).
Discussion: For this study’s Veterans, treatment-related changes in sleep and pain appeared to occur in parallel. The concomitant changes in sleep and pain suggest that therapies improving pain in Veterans may yield attendant benefits for the treatment of sleep, and possibly vice versa.
Keywords: chronic pain, complementary and integrative treatments, sleep, Veterans
Introduction
Chronic pain is highly prevalent in US military Veterans, at rates more than triple that of the general US adult population.1,2 Severe pain that limits life and work activities affects 9% of Veterans.1 Guidelines for evidence-based medication prescribing and safe opioid use from the US Veterans Health Administration call for the integration of non-pharmacological modalities for pain treatment.3 Use of non-opioid and non-pharmacologic treatments should be maximized as first-line options for chronic pain when clinically appropriate.4 Yet, research is lacking regarding which complementary and integrative treatments may be indicated for specific pain syndromes and what mechanisms support beneficial effects.
Complicating pain treatment, particularly among Veterans, are common comorbidities such as sleep dysregulation, mood disorders, substance use disorders, and Post Traumatic Stress Disorder (PTSD),5 all of which can potentially amplify pain symptoms and vice versa. PTSD occurs in half of all US Veterans with chronic pain6 and is disruptive to sleep, with frequent co-morbid problems of insomnia, nightmares, sleep-related breathing disorders, and parasomnia.7 The co-occurrence of pain with PTSD can also contribute to greater opioid use.8 Determining how non-pharmacological therapies affect this cluster of symptoms, particularly sleep, within a Veteran population may offer new insights for treatment.
It is commonly believed that there is a bidirectional relationship between pain and sleep,9,10 although understanding of the biological underpinnings of this relationship remains limited. Historically, it has been assumed that sleep disturbances are a direct result of chronic pain, and, therefore, treatment of chronic pain should resolve or improve sleep symptoms.11 However, studies have also found direct effects on pain when sleep is altered or fragmented.12,13 For example, experimentally induced sleep deprivation has been found to increase next-day pain.13,14 Moreover, one longitudinal study found that early changes in sleep were a stronger predictor of changes in pain than vice versa and that early self-reported sleep improvements predicted pain improvements over the course of a year.15
Theories explaining pain/sleep mechanisms include mediation by neurotransmitters (eg, dopamine, serotonin) or endogenous opioids, or by negative affect11 or reward16 pathways. Sleep deprivation has also been found to reduce pain thresholds17,18 and alter levels of interleukin-6,19,20 reflecting a potential inflammatory response to sleep loss.21,22 Given the consistent findings that individuals with both chronic pain and sleep disturbance generally experience more distress including greater pain severity, longer pain duration, and more pain-related disability,11 greater understanding of how pain affects sleep and vice versa remains an important goal.
It has been suggested that offering pharmacological and non-pharmacological approaches that can treat concurrent chronic pain and sleep disturbance is a logical next step.23 The demand for non-pharmacological treatments is heightened due to risks of commonly prescribed medications for pain and sleep (eg, opioids and benzodiazepines) that are compounded when taken together.13 Identifying effective non-pharmacological treatments for the frequently co-mingling symptoms of pain and sleep disturbance – and investigating whether treatment-related reductions in pain are a result of treatment-related improvements in sleep, or rather sleep improves as a result of reduced pain, or both – could lead to progress in both pain and sleep outcomes.
The current study is a supplementary study paired with a randomized clinical trial (RCT; Clinical Trials NCT02653664) investigating the efficacy of psychologically based non-pharmacological treatments for chronic pain in US Veterans with diverse chronic pain conditions.24 Each of the three study treatment conditions in the RCT included 8 in-person group sessions, delivered by allied health professionals on staff at a large Veterans Health Administration (VA) medical system in the Northwest. The RCT investigated whether training in self-hypnosis and mindfulness meditation resulted in significantly greater pre- to post-treatment decreases in average pain intensity when compared to receiving 8 sessions of an education control intervention. Protocol details have been previously published along with justifications for testing the chosen psychological treatments for effects on pain.25
For the present supplementary study, we sought to investigate the potential role of sleep in treatment-related improvements in pain. Given the potentially bidirectional relationship between pain and sleep,9,10 our research hypothesis was that changes in pain across the study would be accompanied by changes in sleep. We did not posit a priori any specific direction of the temporal relationship between changes in pain and changes in sleep. We pursued our investigation using a cross-lagged design, where the temporal relationship between observed effects (ie, changes in sleep preceding changes in pain, or vice versa) could shed light on the direction of the effect.
We recruited participants at the time of enrollment into the parent RCT. Supplementary study participants were asked to wear a wrist actigraph during the study and to complete additional self-report measures related to sleep. The specific aims of the supplementary study were to explore the reciprocal relationships between sleep and pain measures over time, focusing on changes from pretreatment baseline to posttreatment (at the end of the 8-week treatment period) to follow-up (3 months after the end of the treatment period). We aimed to (1) analyze and compare the effects of the three treatment conditions on sleep and (2) determine whether sleep measures obtained through wrist actigraphy and by self-report predicted changes in pain occurring later, or vice versa, or whether changes in sleep and pain occurred in parallel.
Material and Methods
Participants
Study participants were US Armed Forces Veterans receiving health care services through a large VA medical system comprising two VA medical centers in the Northwest US. Participants were recruited into the parent RCT via clinical provider referrals, mailed invitations based on medical record screenings, and self-referral. The supplementary study was approved for funding in the third year of the parent RCT. Study staff approached all who subsequently enrolled in the parent RCT to participate in the supplementary study. Those who were interested in joining the supplementary study were asked to complete an additional informed consent. Of the 213 individuals approached, 184 (86%) enrolled in the supplementary study, and of these, 174 (95%) were randomized to treatment. The present investigation is based on the N = 174 Veterans who were randomized to treatment.
Participants were eligible if they had enrolled in the parent RCT after meeting the following criteria: Veteran status (defined as prior service in the US Armed Forces and eligible to receive health care services through the Veterans Health Administration); 18 years of age or older; self-reported presence of chronic physical pain; average pain intensity rating of greater than or equal to 3 on a 0–10 Numeric Rating Scale (NRS) of pain intensity in the last week;26 worst pain intensity rating of greater than or equal to 5 on the 0–10 NRS of pain intensity in the last week; duration of chronic pain 3 months or more; experiencing pain at least 75% of the time in the past three months; and able to read, speak, and understand English.
Participants were ineligible for the parent RCT and, therefore, this supplementary study if they met any of the following criteria: severe cognitive impairment defined as two or more errors on the Six-Item Cognitive Screener;27 current or history of diagnosis of primary psychotic or major thought disorder as listed in participant’s medical record or self-reported within the past five years; hospitalization for psychiatric reasons other than suicidal ideation, homicidal ideation, and/or PTSD self-reported or noted in chart, within the past 5 years; psychiatric or behavioral conditions in which symptoms were unstable or severe as listed in participant’s medical record or self-reported within the past 6 months; any behavioral issues noted in the medical record that would indicate the participant may be inappropriate in a group setting; presenting symptoms at time of screening that would interfere with participation, specifically active suicidal ideation with intent to harm self or active delusional or psychotic thinking; difficulties or limitations communicating over the telephone; any planned life events that would interfere with participating in the key elements of the study; and reported average daily use of greater than 120 mg morphine equivalent dose. No additional eligibility criteria were required for the supplementary study.
Participants were financially compensated for their time, earning up to $450 for assessments that were part of the primary study and an additional $150 if actigraphy devices were returned at all three data collection time points ($50 per time point). The supplementary study was approved by the Institutional Review Boards of the University of Washington, the VA Puget Sound Health Care System, and Washington State University. The investigation was carried out in accordance with the latest version of the Declaration of Helsinki.
Study Design
Veterans recruited into the supplementary study had been randomly assigned one of three treatments, each comprised of eight 90-minute sessions delivered in person in a group format over an 8–12-week period: training in self-hypnosis (n = 61), training in mindfulness meditation (n = 56), or education control (n = 57). These treatments were based on those used in other trials by the investigators,28 and details are provided in the published protocol.25 Participants were asked to continue their usual pain and other medical treatments during the trial. Interventions were delivered by a variety of health professionals on staff at the VA medical center (ie, psychologists, nurses, occupational therapists) who received two days of training and delivered all three treatment conditions to groups of 3–12 participants. Treatment fidelity was maintained with twice monthly supervision by research investigators and monitored using adherence rating forms tailored for each condition. Average fidelity adherence ratings were 97% across the clinicians and conditions.
The hypnosis condition involved training in self-hypnosis to mitigate pain under the premise that people can be trained to enter a state of focused attention that makes them more open to suggestions for making changes in perceptions, sensations, thoughts, and behaviors.29 Each hypnosis session included a scripted hypnosis activity comprising an induction, clinical suggestions, posthypnotic suggestions, and a posthypnosis alerting process, followed by discussion focused on encouraging home practice. In-session hypnotic inductions were 15–30 minutes in duration. All of the clinical suggestions included in the hypnotic sessions targeted some combination of increased comfort, increases in adaptive thoughts about or the meaning of pain, or improvements in comorbid symptoms thought to impact pain (eg, improved mood and optimism, relaxation, and sleep quality). Eight pre-recorded audio recordings were provided to the hypnosis condition participants, based on the hypnosis scripts that were used by the study clinicians during each of the eight-group sessions.
The mindfulness meditation condition sought to teach the regulation of attention decoupled from emotion, hypothesized to be a central mechanism across forms of mindfulness meditation,30 in conjunction with pain acceptance, under the premise that this underlies reductions in pain. The mindfulness meditation treatment used was based on manuals and techniques developed by members of the primary study investigative team.31,32 Participants in this condition were instructed on a combination of Shamatha meditation, which involves quieting the mind and maintaining focus on a specific object, as well as Vipassana, an open monitoring form of mindfulness meditation that acknowledges the mind’s sensory, emotional, or cognitive events while avoiding judgment.33 Each of the mindfulness meditation sessions included an in-session scripted practice, which lasted from 3 to 45 minutes, as well as a guided inquiry that explored participants’ experiences with the practice and encouraged patient, gentle persistence in daily practice. The pre-recorded audio recordings provided for home practice included all of the meditation activities that were facilitated in the group sessions.
The education control condition served as an active control treatment, matched to the hypnosis and mindfulness meditation treatments on time, attention, and modality. The education control condition involved a combination of facilitated discussion and didactics to increase participants’ knowledge about chronic pain and efficacy in pain self-management. Sessions included didactic instruction and facilitated discussion about topics such as the biopsychosocial model, sleep hygiene, and mood. Audio recordings provided for home practice were 15–25 minutes in duration and included a review of information provided in the group sessions plus affirming messages for participating.
Procedure
Procedures for the supplementary study were integrated and synchronized with the procedures in the parent RCT. In addition to the study procedures for the parent RCT, participants in the supplementary study wore a wrist actigraph, completed a sleep diary for 7 days, and completed several additional self-report measures during each of three study assessment periods: pretreatment baseline, posttreatment after the 8 sessions, and 3-month follow-up. All assessments were conducted via structured phone interviews by trained staff members who were unaware of treatment allocation.25
Participants were blind to the study hypotheses and were told that each of the three conditions is a type of “pain self-management” intervention that previous individuals with pain found to be helpful. All research staff conducting recruitment and assessments were blind to the randomization assignment database, maintaining concealment of treatment allocation. All research staff conducting the outcome assessments were blind to treatment condition throughout the follow-up period. Study investigators were not blind to allocation but had minimal direct interaction with subjects. The biostatistician and data managers involved in data analysis for the parent RCT and supplementary study were blind to the intervention codes.
The sleep and pain data obtained at the three assessments for each of the three treatment conditions are the focus of the present paper.
Measures
Demographic Data
Prior to random assignment to the treatment conditions, all participants were asked to provide information regarding their age, self-identified gender, self-identified racialized group, self-identified ethnicity, marital status, income, education level, employment status, and deployment history (number and months of deployments). Descriptive information of the study sample was provided previously in a paper focusing on baseline variables and variables mediating the baseline sleep–pain relationship.34 For the purpose of the present investigation, we report age, self-identified gender, self-identified racialized group, self-identified ethnicity, and pain type. Pain type was assessed and categorized as neuropathic, non-neuropathic, mixed/undetermined via the PainDETECT measure35 and Self-Report Leeds Assessment of Neuropathic Symptoms and Signs (S-LANSS).36
Sleep-Related Measures
Subjective Sleep Disturbance
At each of the three time points, the 8-item Patient Reported Outcomes Measurement Information System Sleep Disturbance – Short Form (PROMIS-SD) was used to measure sleep disturbance.37 The PROMIS-SD assesses different aspects of sleep quality and daily impact of sleep over the past 7 days. As with most PROMIS measures, the raw scores are transformed into standardized T scores. The PROMIS-SD has been shown to be reliable and valid in adult populations with chronic health conditions.37 Higher T scores indicate more sleep disturbance.
Actigraphic sleep duration. At each of the three time points, participants were asked to wear an actigraph (Respironics Actiwatch 2, Philips Respironics, Bend, OR) on the wrist of their non-dominant arm continuously for 7 consecutive days, 24 hours a day. The device measured rest/activity patterns across 1-minute intervals, which can be used to compute the durations of sleep periods (Actiware 6.0.4 software, Philips Respironics, Bend, OR). During this one-week period, they were also asked to complete a brief questionnaire each morning and evening and fill out a sleep log to provide estimates of time to bed, time to sleep, time awake and time out of bed. Guided by the participants’ sleep log data, sleep durations were quantified based on the software’s default algorithm, which has been validated against polysomnography.38 The actigraphically derived average daily sleep duration, calculated as the aggregated sleep duration divided by the total actigraphic recording time for each assessment, was used as an objective measure of sleep.
Pain-Related Measures
Pain Intensity
At each of the three time points (baseline, posttreatment, and follow-up), the 0–10 Numeric Rating Scale (NRS) of pain intensity was used to assess average pain intensity as is recommended in clinical trials of pain treatments.26 Participants were asked to rate their average pain intensity during the past 24 hours on a 0–10 Likert scale (0 = “No pain” and 10 = “Pain as severe as it could be”). 0–10 NRS data were collected up to 4 times within one week at each time point in telephone calls separated by at least 24 hours and then an average was calculated.
Pain Catastrophizing
At each of the three time points, the 13-item Pain Catastrophizing Scale (PCS) was used to measure catastrophic thinking related to pain.39 The PCS is a commonly used measure of pain catastrophizing with considerable support for its validity and reliability.39 Respondents indicate the frequency with which they have each of 13 catastrophizing thoughts listed in the measure on a 5-point Likert scale (0 = “Not at all”, 4 = “All the time”). Higher scores indicate a greater frequency of pain-related catastrophic thoughts. At baseline, Cronbach’s α for our sample was 0.93, indicating excellent reliability.
Statistical Analysis
Statistical analyses were performed using SAS 9.4 software. To describe the sample, descriptive statistics of demographics and baseline measurements were computed. Baseline differences between the three treatment conditions were evaluated with Fisher’s exact test for categorical variables and one-way analysis of variance (ANOVA) for continuous variables. Attrition at the posttreatment and 3-month follow-up assessments was also evaluated using Fisher’s exact test and one-way ANOVA.
To investigate the effects of treatment condition on each of the sleep and pain outcome measures, mixed-effects ANOVA was used, with fixed effects for treatment condition and time point and their interaction, and a random effect on the intercept. Planned contrasts were included for pairwise comparisons among time points, and to compare each of the active treatment conditions (ie, hypnosis and mindfulness meditation) to the education control condition at the posttreatment and 3-month follow-up assessments. A power calculation performed in advance of the supplementary study indicated that a sample size of at least 117 Veterans would be expected to yield adequate statistical power (80% or more at an overall type I error rate of 0.05) to detect differences in change from baseline to posttreatment between the active treatment conditions and the education control condition.
In order to examine whether subjective and objective sleep measures predicted later changes in pain variables, or vice versa, from baseline to posttreatment to 3-month follow-up, cross-lagged regression analyses of paired sleep and pain measurements were conducted,40 controlling for treatment condition at the posttreatment and 3-month follow-up assessments. Here, lagged reciprocal effects between paired sleep and pain measurements were of primary interest, and tested for significance with planned contrasts. Differences in self-report measurements tend to be stable and cluster among measures;41,42 therefore, the cross-lagged regression analyses were implemented to also account for autoregressive carry-over effects and for concurrent reciprocal effects at the posttreatment and 3-month follow-up assessments. Goodness-of-fit was assessed relative to equivalent models without reciprocal terms and tested for significance using likelihood ratio tests. The cross-lagged regression analyses were repeated for each treatment condition separately.
Results
Demographic Characteristics of the Study Sample
The descriptive information of the N = 174 study participants is presented in Table 1 and was representative of the parent study sample. Participants’ ages were 53.0 ± 13.7 years (mean ± SD). Seventy-one percent were men, and the majority (62%) self-identified as being White (62%) and non-Hispanic (89%). Participants experienced a mix of pain types, most commonly probable neuropathic (42%). There was no significant difference in age between the treatment conditions (F2,171 = 2.40, p = 0.094); participants assigned to the hypnosis condition were slightly younger (50.1 ± 13.1 y) compared to the mindfulness meditation condition (55.5 ± 13.8 y) and the education control condition (53.7 ± 13.8 y). Fisher’s exact test revealed no significant differences between the three conditions in terms of self-identified gender (p = 0.49), pain types (p = 0.53), or self-identified race (p = 0.36), but there was a significant difference for ethnicity (5 self-identified as Hispanic in the hypnosis condition, 10 in the mindfulness condition, and 2 in the education control condition, p = 0.043). The median number of treatment sessions attended was 7 (out of 8).
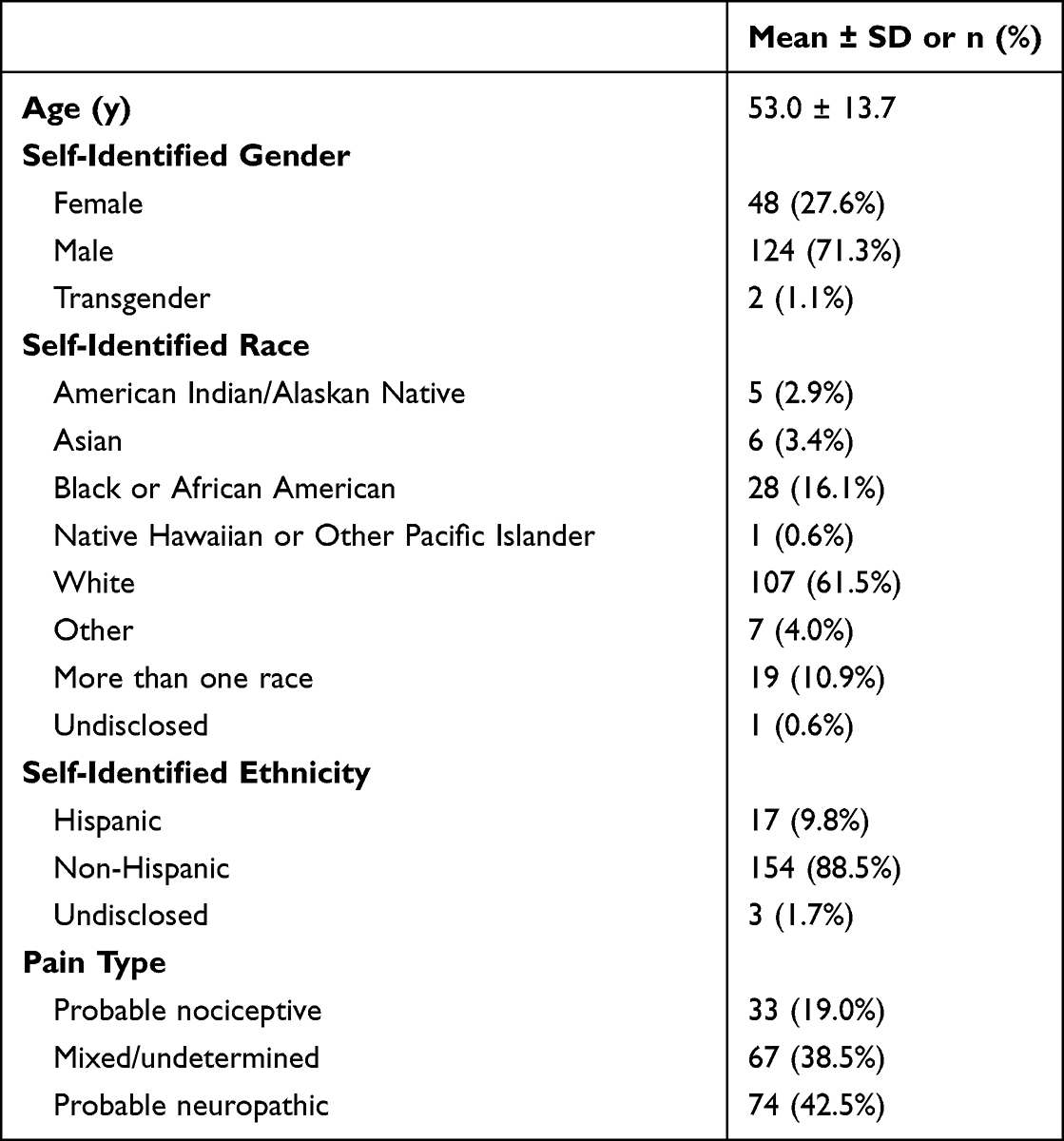 |
Table 1 Demographics of the Baseline Sample of This Investigation (N = 174) |
Baseline Sleep and Pain
Baseline scores on the PROMIS-SD were 58.5 ± 8.1 (mean ± SD), indicating greater subjective sleep disturbance than the US general population average by 0.85 standard deviation units. There was no statistically significant difference in baseline subjective sleep disturbance between treatment conditions (F2,171 = 0.05, p = 0.95). Baseline actigraphy data to quantify objective sleep duration were available for 139 participants, 80% of those who enrolled in the supplementary study. Participants wore their actigraphs for nearly a full week (6.9 ± 0.8 days). Baseline actigraphic sleep duration was 8.3 ± 1.4 h (mean ± SD), in line with the recommended 7–8 hours of daily sleep for adults.43 There was a trend for a difference in baseline objective sleep duration between treatment conditions (F2,136 = 2.85, p = 0.061), with the education control condition obtaining on average 0.6 h more sleep per day than the other two conditions (p < 0.05 in planned contrasts for pairwise comparisons).
Baseline average pain intensity scores on the 0–10 NRS were 5.7 ± 1.7 (mean ± SD), indicating moderate pain severity. There was no statistically significant difference in baseline pain intensity between treatment conditions (F2,171 = 1.63, p = 0.20). Baseline pain catastrophizing scores on the PCS were 28.6 ± 12.2 (mean ± SD), which at the mean is just below the clinically relevant threshold of 30.44 There was no statistically significant difference in baseline pain catastrophizing between treatment conditions (F2,171 = 0.51, p = 0.60).
Posttreatment and 3-Month Follow-Up Samples
The time interval between the baseline and posttreatment assessments was 78.3 ± 11.7 days (mean ± SD based on the actigraphy records). The time interval between the posttreatment and 3-month follow-up assessments was 93.0 ± 11.8 days, and the time interval from baseline to 3-month follow-up was 170.8 ± 16.5 days (ie, 24.4 weeks on average).
A portion of the overall sample was lost to attrition at the posttreatment and 3-month follow-up assessments. At posttreatment, complete survey data were available for 158 (91%) of the enrolled 174 individuals, with actigraphy data available for 109 (63%). At the 3-month follow-up, complete survey data were available for 138 (79%) of enrolled 174 individuals, with actigraphy data available for 88 (51%). Participants wore their actigraphs for nearly a full week both posttreatment (6.8 ± 1.0 days) and at 3-month follow-up (6.8 ± 0.7 days).
Attrition was higher among individuals self-identifying as Hispanic (29%) compared to those self-identifying as non-Hispanic (7%) at the posttreatment assessment (Fisher’s exact test, p = 0.012); and non-significantly among individuals identifying as Hispanic (35%) compared to those identifying as non-Hispanic (19%) at the 3-month follow-up (Fisher’s exact test, p = 0.12). Attrition was not significantly related to treatment condition at either time point (Fisher’s exact test, posttreatment p = 0.12, follow-up p = 0.50).
Of those withdrawing from the supplemental sleep study, 33% (19) withdrew from the parent RCT. The notably higher rates of attrition for actigraphy, as compared to survey data, were due to the additional burden of the 1-week periods of continuous actigraph wearing, poor participant adherence in returning the actigraphs after each data collection period, loss of communication with participants, and technical issues with a few of the actigraphy devices.
Differences in sleep and pain measures at baseline for participants who were lost to attrition at the posttreatment assessment were not statistically significant for subjective sleep disturbance (F1,172 = 1.48, p = 0.23), objective sleep duration (F1,140 = 0.92, p = 0.34), pain intensity (F1,172 = 0.05, p = 0.83), and pain catastrophizing (F1,172 = 0.59, p = 0.44). Likewise, differences in baseline sleep and pain measures for participants who were lost to attrition at the 3-month follow-up assessment were not statistically significant for subjective sleep disturbance (F1,172 = 2.47, p = 0.12), objective sleep duration (F1,137 = 0.07, p = 0.79), pain intensity (F1,172 = 0.18, p = 0.67), and pain catastrophizing (F1,172 = 0.36, p = 0.55). As such, missing data at the posttreatment and 3-month follow-up assessments could be reasonably assumed to be missing at random (ie, not systematically related to the measurements) and all available data were therefore used for analyses, with data loss unlikely to bias the results.
Effects of Treatment Conditions Over Time
Figure 1 shows the sleep and pain data at each time point, both collapsed across treatment conditions (left panels) and stratified by treatment condition (right panels). Means and standard deviations for the data below are provided in Table 2. Although self-reported sleep disturbance and pain intensity effects were reported in the primary RCT as treatment outcomes,24 we repeated the analyses here to confirm the results in this supplementary study sample. Additional analyses on objective sleep and self-reported pain catastrophizing were not previously reported.
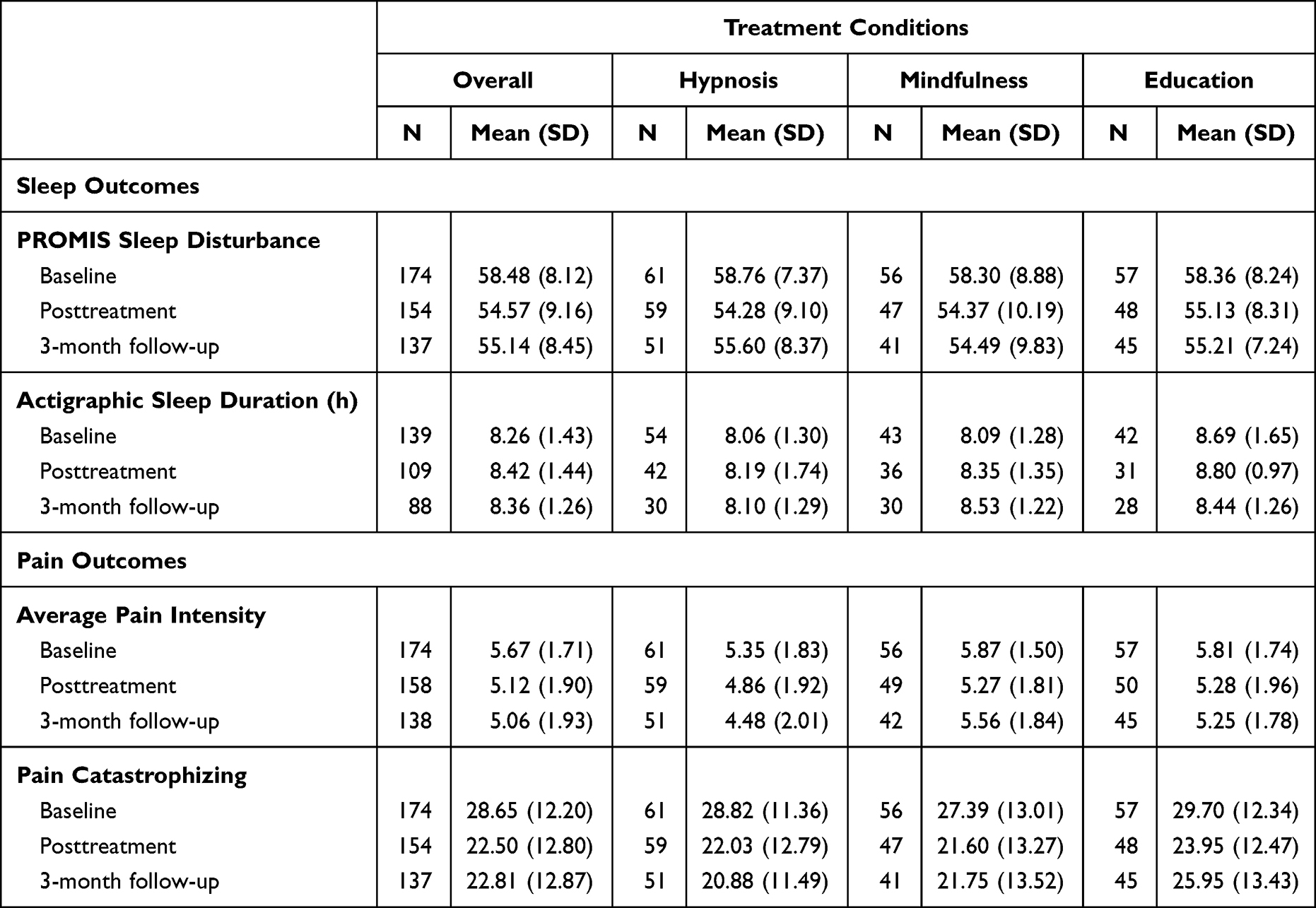 |
Table 2 Means and Standard Deviations for the Sleep and Pain Data |
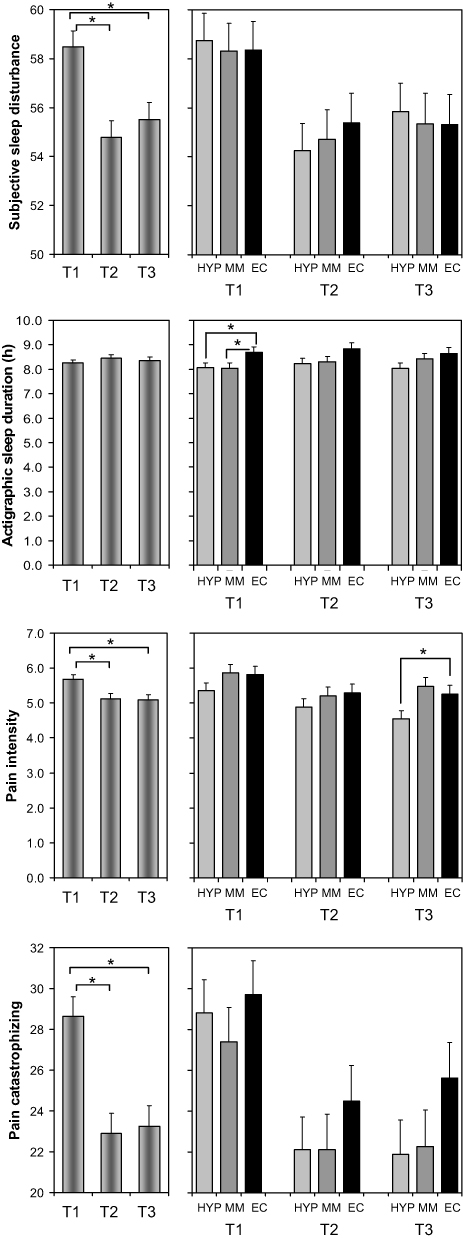 |
Figure 1 Means (and SE) of sleep and pain measures across the three time points. Left: aggregated over treatment conditions. Right: stratified by the three treatments. Brackets indicate significant planned contrasts for pairwise comparisons between time points (left panels) and for pairwise comparisons between treatments at a given time point (right panels). *p < 0.05. Abbreviations: T1, pretreatment baseline assessment; T2, posttreatment assessment; T3, 3-month follow-up assessment; HYP, hypnosis condition; MM, mindfulness meditation condition; EC, education control condition. |
For subjective sleep disturbance, there was again a significant effect of time (F2,285 = 22.39, p < 0.001), but no significant effect of treatment condition (F2,285 = 0.01, p = 0.98) or treatment condition by time interaction (F4,285 = 0.43, p = 0.79). Subjective sleep disturbance decreased from baseline to posttreatment (F1,285 = 39.97, p < 0.001) and remained below baseline at 3-month follow-up (F1,285 = 1.37, p = 0.24). Planned contrasts showed no significant differences between the active treatment conditions (hypnosis and mindful meditation) and the education control condition posttreatment or at 3-month follow-up.
For objective sleep duration measured with actigraphy, there was no significant effect of time (F2,185 = 1.24, p = 0.29) and no significant treatment condition by time interaction (F4,185 = 0.40, p = 0.81), but there was a significant effect of treatment condition (F2,185 = 3.24, p = 0.041). Objective sleep duration was greater in the educational control condition than in the other two conditions throughout the study. However, no pairwise comparisons with the control condition at the posttreatment and 3-month follow-up assessments were significant.
Consistent with the findings from the primary study in the entire sample,24 for average pain intensity, there was a significant effect of time (F2,290 = 20.26, p < 0.001), but no significant effect for treatment condition (F2,290 = 2.22, p = 0.11) or a treatment condition by time interaction (F4,290 = 1.44, p = 0.22). Average pain intensity decreased from baseline to posttreatment (F1,290 = 29.49, p < 0.001) and remained below baseline at 3-month follow-up (F1,290 = 0.10, p = 0.75). Consistent with the results of the full sample in the primary study, the results for this supplementary study indicate a statistically significant difference in average pain intensity between the hypnosis condition and the education control condition at the 3-month follow-up assessment (F1,290 = 4.24, p = 0.040), with the hypnosis condition showing lower pain intensity. No other pairwise comparisons with the control condition at the posttreatment and 3-month follow-up assessments were statistically significant in the supplementary study sample.
Likewise, for pain catastrophizing, there was a significant effect of time (F2,285 = 43.43, p < 0.001), but no significant effect of treatment condition (F2,285 = 0.89, p = 0.41) or treatment condition by time interaction (F4,285 = 0.77, p = 0.55). Pain catastrophizing decreased from baseline to posttreatment (F1,285 = 70.15, p < 0.001) and remained at a decreased level from posttreatment to 3-month follow-up (F1,285 = 0.24, p = 0.62). Planned contrasts showed no significant differences between the tested treatment conditions (hypnosis and mindful meditation) and the education control condition posttreatment or at 3-month follow-up, consistent with similar analyses conducted for the primary study sample.24
As shown in Table 3, there were statistically significant correlations among the sleep and pain measures in this study. In particular, the three self-report measures (assessing pain intensity, pain catastrophizing, and sleep disturbance) showed substantial covariation between and within time points, with greater sleep disturbance corresponding to greater pain intensity and greater pain catastrophizing, and vice versa. However, correlations between these self-report measures and actigraphic sleep duration were consistently weak and, with one exception, non-significant.
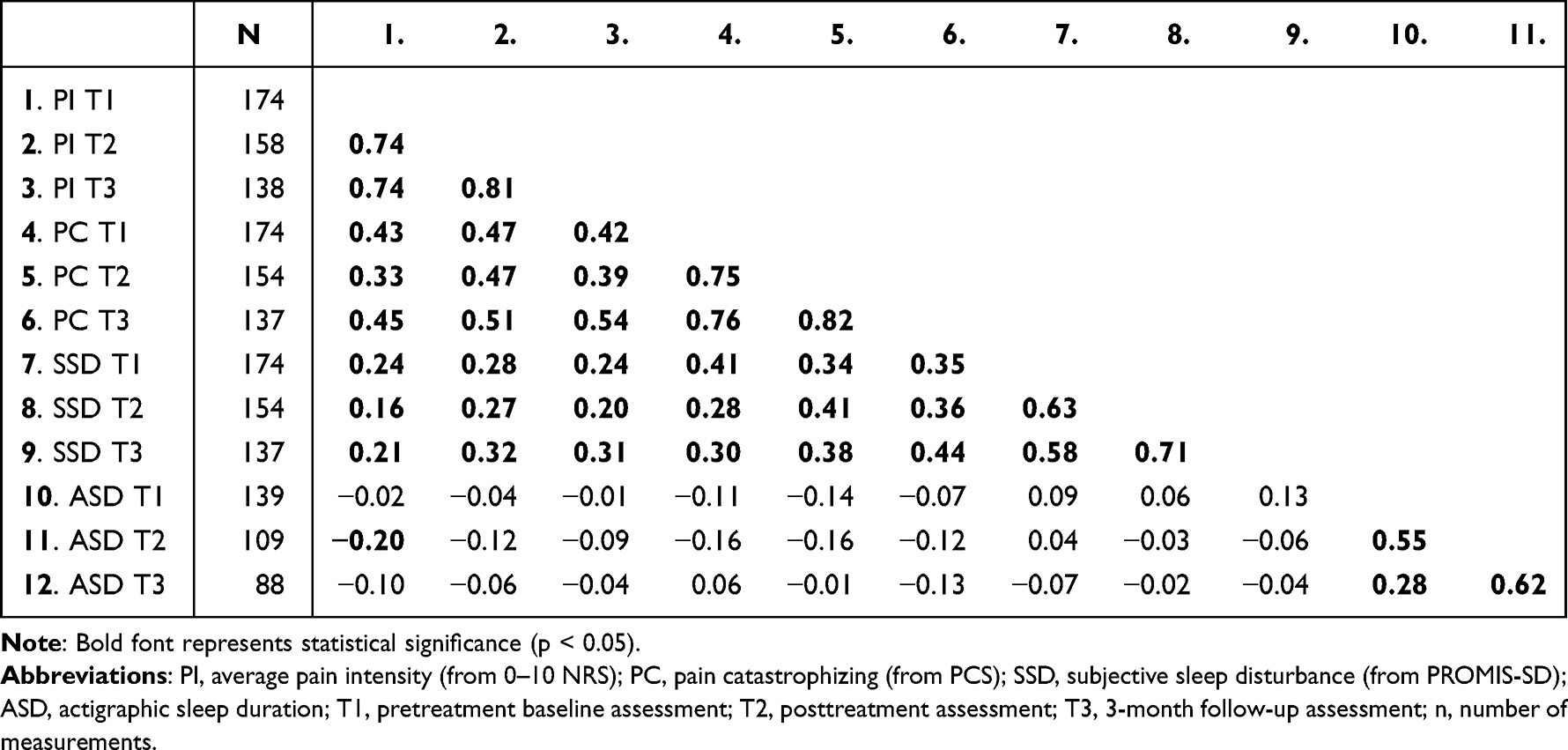 |
Table 3 Pearson Correlation Coefficients for the Pain and Sleep Measures at Baseline, Posttreatment, and 3-Month Follow-Up |
Cross-Lagged Regression Analyses
Figure 2 (top) presents the results of the cross-lagged regression analysis for pain intensity (0–10 NRS) and subjective sleep disturbance (PROMIS-SD) across the three time points. Goodness-of-fit of the cross-lagged regression model was statistically significant (χ28 = 37.6, p < 0.001). Pain intensity at prior assessments was significantly predictive of pain intensity at subsequent assessments; likewise, subjective sleep disturbance at prior assessments was significantly predictive of subjective sleep disturbance at subsequent assessments (horizontal arrows). The concurrent reciprocal relationships between pain intensity and subjective sleep disturbance at the posttreatment and 3-month follow-up assessments (vertical arrows) were statistically significant (p < 0.05) or showed a trend (0.05 ≤ p < 0.10). However, the cross-lagged reciprocal relationships (diagonal arrows) were not statistically significant. When the analysis was repeated for each treatment condition separately, the cross-lagged reciprocal relationships were again not statistically significant. Thus, rather than a causal, temporal relationship whereby subjective sleep disturbance predicted later changes in pain intensity or vice versa, our results suggest that changes in these measures occurred in parallel in the study sample.
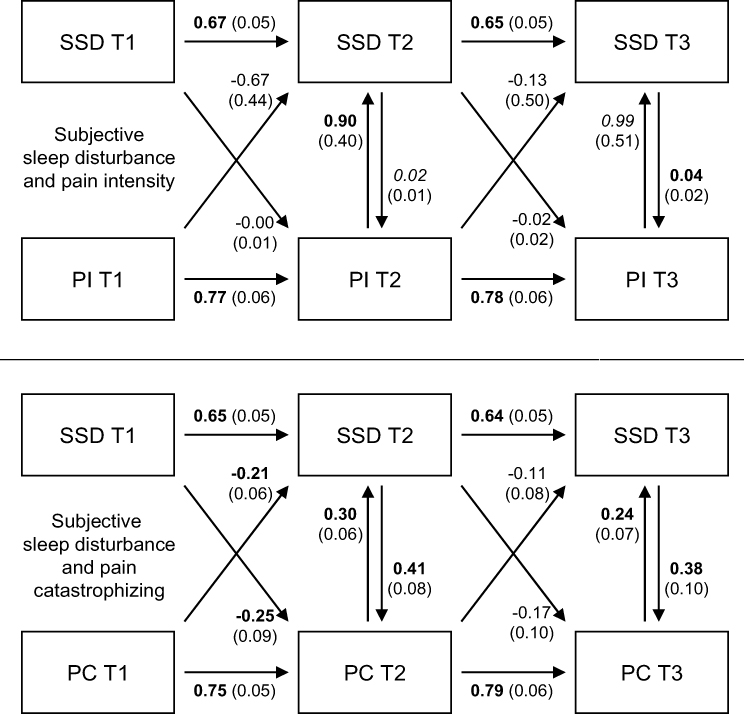 |
Figure 2 Cross-lagged regression analysis for measures of pain and subjective sleep disturbance. Top: pain intensity (PI. from 0–10 NRS) and subjective sleep disturbance (SSD, from PROMIS-SD). Bottom: pain catastrophizing (PC, from PCS) and SSD. Numbers shown are regression coefficients (with standard errors). Bold font represents statistical significance (p < 0.05), italicized represents a trend (0.05 ≤ p < 0.10). Abbreviations: T1, pretreatment baseline assessment; T2, posttreatment assessment; T3, 3-month follow-up assessment. |
Figure 2 (bottom) presents the results of the cross-lagged regression analysis for pain catastrophizing (PCS) and subjective sleep disturbance across the three time points. Goodness-of-fit of the cross-lagged regression model was statistically significant (χ28 = 73.3, p < 0.001). Like subjective sleep disturbance, pain catastrophizing at prior assessments was significantly predictive of pain catastrophizing at subsequent assessments (horizontal arrows). The concurrent reciprocal relationships between pain catastrophizing and subjective sleep disturbance at the posttreatment and 3-month follow-up assessments were all statistically significant. Importantly, the cross-lagged reciprocal relationships at the posttreatment assessment (but not the 3-month follow-up assessment) were statistically significant as well.
When the cross-lagged regression analysis was repeated for the mindfulness meditation and education control conditions separately, none of the cross-lagged reciprocal relationships were statistically significant. However, for the hypnosis condition, all of the cross-lagged reciprocal relationships were significant. As shown in Figure 3, the corresponding regression coefficients were negative. As Table 3 revealed that there were no negative correlations between cross-lagged measurements pairs for pain catastrophizing and subjective sleep disturbance, these inverse cross-lagged reciprocal relationships (diagonal arrows) may be interpreted as tempering the overwhelmingly strong positive concurrent reciprocal relationships (vertical arrows) and autoregressive carry-over effects (horizontal arrows) – possibly a manifestation of regression to the mean. As with pain intensity, therefore, our results for pain catastrophizing and subjective sleep disturbance suggest that changes in these measures occurred mostly in parallel.
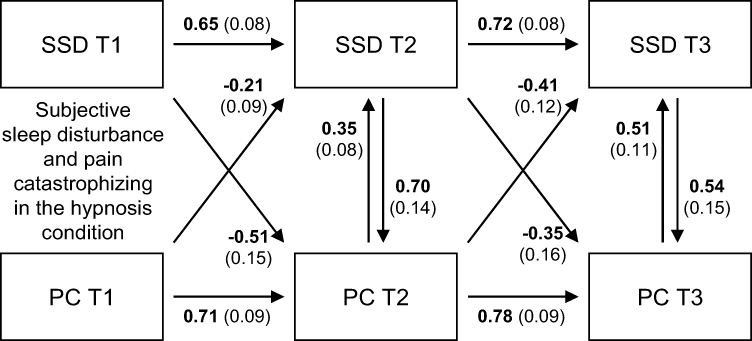 |
Figure 3 Cross-lagged regression analysis for pain catastrophizing and subjective sleep disturbance in the hypnosis condition only. Numbers shown are regression coefficients (with standard errors). Bold font represents statistical significance (p < 0.05). Abbreviations: PC, pain catastrophizing (from PCS); SSD, subjective sleep disturbance (from PROMIS-SD); T1, pretreatment baseline assessment; T2, posttreatment assessment; T3, 3-month follow-up assessment. |
Figure 4 (top) presents the results of the cross-lagged regression analysis for pain intensity (0–10 NRS) and actigraphic sleep duration across the three time points. Goodness-of-fit of the cross-lagged regression model was statistically significant (χ28 = 186.1, p < 0.001). Like pain intensity, actigraphic sleep duration at prior assessments was significantly predictive of actigraphic sleep duration at subsequent assessments, albeit to a lesser degree. The concurrent reciprocal relationships between pain intensity and actigraphic sleep duration were not statistically significant, and the same applied for the cross-lagged reciprocal relationships. Our results suggest that changes in pain intensity and objectively measured sleep duration occurred in parallel.
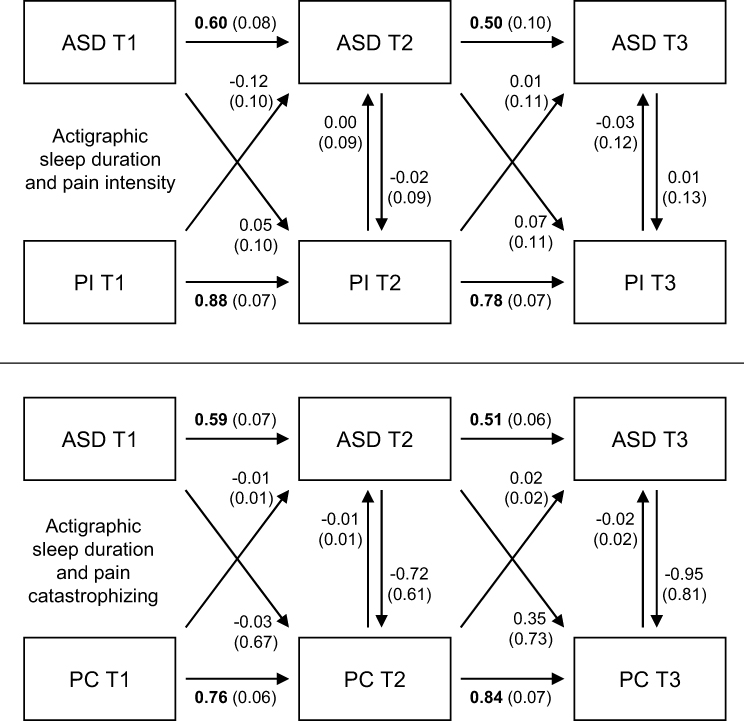 |
Figure 4 Cross-lagged regression analysis for measures of pain and actigraphic sleep duration. Top: pain intensity (PI, from 0–10 NRS) and actigraphic sleep duration (ASD). Bottom: pain catastrophizing (PC, from PCS) and ASD. Numbers shown are regression coefficients (with standard errors). Bold font represents statistical significance (p < 0.05). Abbreviations: T1, pretreatment baseline assessment; T2, posttreatment assessment; T3, 3-month follow-up assessment. |
Finally, Figure 4 (bottom) presents the results of the cross-lagged regression analysis for pain catastrophizing (PCS) and actigraphic sleep duration across the three time points. Goodness-of-fit of the cross-lagged regression model was statistically significant (χ28 = 362.7; p < 0.001). The concurrent reciprocal relationships between pain catastrophizing and actigraphic sleep duration were not statistically significant, and neither were the cross-lagged reciprocal relationships. Again, these results suggest that changes in pain catastrophizing and objectively measured sleep duration occurred in parallel.
Discussion
This supplementary study was part of a larger study of US Armed Forces Veterans with chronic pain who were randomized to one of three pain treatments: training in self-hypnosis, training in mindfulness meditation, or education control intervention. In the supplementary study, additional data were collected using self-report instruments measuring subjective sleep disturbance, pain intensity, and pain catastrophizing, as well as actigraphic assessments of objective sleep duration. These sleep and pain measurements were obtained at baseline, after the 8–12-week treatment period, and during 3-month follow-up. At baseline, average pain intensity scores indicated moderate pain severity;26 pain catastrophizing scores were just below the clinically relevant threshold;44 and sleep disturbance was greater than the US population average.45 However, actigraphic sleep duration was consistent with the recommended 7–8 hours of daily sleep for adults.43 In all three treatment conditions, pain intensity, pain catastrophizing, and subjective sleep disturbance decreased from baseline to posttreatment, and remained at a decreased (ie, improved) level at 3-month follow-up. However, objective sleep duration did not change significantly over time. Furthermore, subjective sleep and pain measures, but not objective sleep duration, were strongly associated at and between the three time points. Observations at prior assessments predicted observations for the same outcome variables at subsequent assessments. Results from cross-lagged regression analyses indicated that changes in sleep and pain occurred in parallel.
Despite the smaller sample of the supplementary study, findings with regard to pain intensity and subjective sleep disturbance were similar to those reported in the primary RCT.24 Here, we added the variables of pain catastrophizing and objective sleep duration. As in the primary RCT, the improvements over time from pre- to posttreatment were not significantly different between the two active treatment conditions (hypnosis and mindfulness meditation) compared to the education control condition. The observed improvements were sustained at the 3-month assessment, and at this time point, significant differences between treatment conditions emerged; hypnosis yielded a greater reduction in pain intensity than the education control condition. These findings align with previously reported benefits of hypnosis on pain intensity,46,47 pain interference,47 and pain catastrophizing.48 However, the findings of this sleep study differed from the primary RCT in that for the latter, significant improvements were noted in the mindfulness meditation condition relative to the education control condition at 3-month follow-up. The smaller sample of the supplementary study could explain this difference.
Unexpectedly, objective sleep duration was greater in the educational control condition than in the other two conditions. However, this condition difference was already present at baseline, and thus likely reflects idiosyncratic variability among individuals assigned to the different conditions. Objective sleep duration was relatively unchanged over time despite improvements over time in subjective sleep disturbance. This likely reflects a ceiling effect on objective sleep duration – in the absence of significant sleep insufficiency, increases in sleep duration are limited by the circadian drive for wakefulness from the endogenous biological clock.49
The divergence between objective and subjective measures of sleep in this study suggests that in our sample of Veterans, reduced sleep quality rather than reduced sleep quantity was the predominant effect of pain on sleep. Prior research suggests that sleep disturbances may present a barrier to treatment engagement and therefore contribute to attrition rates in Veteran studies of web-based cognitive-behavioral therapy.50 Further research could examine whether subjective poor sleep quality contributed to the inability of this sample of Veterans to maximize the potential benefits of the treatments provided.
Also of note, while this study restricted eligibility to Veterans who had not been hospitalized for PTSD within five years, our previous investigation found more than half of the participants scored above the clinically relevant threshold for PTSD as measured by the PTSD Checklist 5 (PCL-5).34,51 PTSD was also significantly correlated with subjective sleep disturbance.34 The interplay between sleep, pain, and PTSD among Veterans is an area worthy of further attention. Similarly, other mental health conditions that we did not investigate in this study are known to impact sleep and pain and may have influenced study outcomes. Baseline levels of depression and anxiety have been previously reported as higher on average than those of healthy normal US populations for participants in this supplementary sleep study sample.34
The study design provided an opportunity to examine whether changes in sleep preceded changes in pain measures, or vice versa, or whether sleep and pain changed in parallel, among Veterans with chronic pain. The correlations in Table 3 imply that the observations for the self-report measures were highly stable within individuals across the three time points. This was seen for actigraphic sleep duration as well, but to a lesser extent. In the cross-lagged regression analyses, a high level of consistency in measurements over time within individuals was also observed. Although pain intensity and subjective sleep disturbance at prior assessments were significantly predictive of pain intensity and subjective sleep disturbance at subsequent assessments, the cross-lagged reciprocal relationships were not statistically significant for any of the treatment conditions. It appears that in the participants of this supplementary study, changes in sleep and pain over time were distinct phenomena occurring in parallel.
It is possible these findings reflect limitations of the time intervals between measurements and examining group data versus individual outcomes; high between-subjects variability could hamper the ability to detect causal patterns. However, it is also possible that the findings reflect true bidirectionality of the relationship between pain and sleep, as previously suggested by others.9,10,52 Studies have shown that sleep disturbance increases next-day pain,12–14 and thus it stands to reason that improvements in sleep could result in improvements in pain. Similarly, it is well known that pain interferes with sleep,10–12,53 and thus improvements in pain could result in improvements in sleep. Further, the two pain treatments in this study may have independently improved sleep as well. Training in self-hypnosis and mindfulness meditation have each been used effectively to improve sleep,54–57 albeit those therapies focused on sleep disturbances specifically; it is not clear whether the interventions have a more generic influence on next-night sleep regardless of the treatment content. Nonetheless, the hypnosis and mindfulness treatments for chronic pain employed in this study could have produced changes in sleep and pain that were truly simultaneous, either through parallel mechanisms or through a single mechanism with multiple concurrent effects.
Limitations of the study include the loss of actigraphy data exceeding the overall attrition rates of the supplementary study. This data loss reduced the sample size for the actigraphy measurements to below the pre-assessed threshold for adequate statistical power and may have limited our ability to detect associations between sleep and pain in the cross-lagged regression analyses. Additionally, our ability to investigate temporal relationships between sleep and pain was constrained by the time intervals between the baseline, posttreatment, and 3-month follow-up assessments. Specifically, it is possible that changes in sleep precede changes in pain, or vice versa, at shorter time scales, and this would have gone unnoticed in our study design.
The ability to detect whether improvements in sleep predict improvements in pain may also have been limited by the fact that the baseline pain intensity was moderate, pain catastrophizing was just below the clinically relevant threshold, sleep disturbance was less than one standard deviation higher than the mean of the general population, and sleep duration was in line with the recommended level for healthy adults. While the observed levels of pain and sleep disturbance are not insignificant, outcomes may have been different if individuals with more clinically significant chronic pain or sleep disturbance had been enrolled. Results may not generalize to populations with more severe degrees of pain or greater levels of pain catastrophizing.
Conclusions
Assessing the role of sleep within the context of novel non-pharmacological pain treatments is necessary to understand therapeutic mechanisms and, potentially, to reveal underlying causal relationships. It remains unclear whether treatment-related reductions in pain are a result of improvements in sleep disturbance, whether sleep disturbance improves as a result of reduced pain, or both. Our findings corroborated previously reported benefits of training in self-hypnosis and mindfulness meditation on both pain and pain-related sleep problems, but did not show that changes in sleep preceded changes in pain or vice versa in the study sample. That is, for the Veterans participating in this study, changes in sleep disturbance and pain appeared to occur in parallel. These parallel changes in sleep disturbance and pain suggest that, just like treatments improving pain may yield benefits for sleep, treatments improving sleep may yield benefits for pain in populations experiencing chronic pain.
Data Sharing Statement
Requests for access to limited, fully deidentified data will be considered on a case-by-case basis; please contact the corresponding author. Access is limited because open access to data was not included as part of informed consent.
Acknowledgments
The authors would like to thank all the Veterans who participated in this research project.
Funding
The study was supported by the National Institutes of Health grant 1R01AT008336-01 (MPJ, RMW) and supplement 3R01AT008336-03S1 (MPJ, MW). Analyses were supported in part by CDMRP grant W81XWH-20-1-0442 (HPAVD) and DURIP grant N00014-22-1-2368 (DAH).
Disclosure
Hans Van Dongen reports personal fees from Jazz Pharmaceuticals, Eisai; grants from Federal Express Corporation, Google, Trackthatsleep, and non-financial support from SleepScore Labs, outside the submitted work. The authors report no other conflicts of interest in this work. The views expressed in this article are those of the authors and do not reflect the official policy or position of their affiliating institutions or the US Department of Veterans Affairs.
References
1. Nahin RL. Severe pain in veterans: the effect of age and sex, and comparisons with the general population. J Pain. 2017;18(3):247–254. doi:10.1016/j.jpain.2016.10.021
2. Zelaya CE, Dahlhamer JM, Lucas JW, Connor EM. Chronic pain and high-impact chronic pain among U.S. adults, 2019. NCHS Data Brief. 2020;390:1–8.
3. U.S. Department of Veterans Affairs. VHA pain management. Available from: https://www.va.gov/painmanagement/.
4. Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC clinical practice guideline for prescribing opioids for pain – United States, 2022. MMWR Recomm Rep. 2022;71(3):1–95. doi:10.15585/mmwr.rr7103a1
5. Mysliwiec V, JL M, CS U, et al. The management of chronic insomnia disorder and obstructive sleep apnea: synopsis of the 2019 U.S. Department of Veterans Affairs and U.S. Department of Defense clinical practice guidelines. Ann Intern Med. 2020;172(5):325–336. doi:10.7326/M19-3575
6. Fishbain DA, Pulikal A, Lewis JE, Gao J. Chronic pain types differ in their reported prevalence of post -traumatic stress disorder (PTSD) and there is consistent evidence that chronic pain is associated with PTSD: an evidence-based structured systematic review. Pain Med. 2017;18(4):711–735. doi:10.1093/pm/pnw065
7. Khazaie H, Ghadami MR, Masoudi M. Sleep disturbances in veterans with chronic war-induced PTSD. J Inj Violence Res. 2016;8(2):99–107. doi:10.5249/jivr.v8i2.808
8. Kind S, Otis JD. The interaction between chronic pain and PTSD. Curr Pain Headache Rep. 2019;23(12):91. doi:10.1007/s11916-019-0828-3
9. Moldofsky H. Sleep and pain. Sleep Med Rev. 2001;5(5):385–396. doi:10.1053/smrv.2001.0179
10. Roehrs T, Roth T. Sleep and pain: interaction of two vital functions. Semin Neurol. 2005;25(1):106–116. doi:10.1055/s-2005-867079
11. Husak AJ, Bair MJ. Chronic pain and sleep disturbances: a pragmatic review of their relationships, comorbidities, and treatments. Pain Med. 2020;21(6):1142–1152. doi:10.1093/pm/pnz343
12. Lautenbacher S, Kundermann B, Krieg JC. Sleep deprivation and pain perception. Sleep Med Rev. 2006;10(5):357–369. doi:10.1016/j.smrv.2005.08.001
13. Koffel E, McCurry SM, Smith MT, Vitiello MV. Improving pain and sleep in middle-aged and older adults: the promise of behavioral sleep interventions. Pain. 2019;160(3):529–534. doi:10.1097/j.pain.0000000000001423
14. Roehrs T, Hyde M, Blaisdell B, Greenwald M, Roth T. Sleep loss and REM sleep loss are hyperalgesic. Sleep. 2006;29(2):145–151. doi:10.1093/sleep/29.2.145
15. Koffel E, Kroenke K, Bair MJ, Leverty D, Polusny MA, Krebs EE. The bidirectional relationship between sleep complaints and pain: analysis of data from a randomized trial. Health Psychol. 2016;35(1):41–49. doi:10.1037/hea0000245
16. Reid MJ, Climent-Sanz C, Finan PH. The sleep-reward-pain pathway model: an integrative review. Curr Sleep Med Rep. 2022;8:97–104. doi:10.1007/s40675-022-00232-7
17. Onen SH, Alloui A, Gross A, Eschallier A, Dubray C. The effects of total sleep deprivation, selective sleep interruption and sleep recovery on pain tolerance thresholds in healthy subjects. J Sleep Res. 2001;10(1):35–42. doi:10.1046/j.1365-2869.2001.00240.x
18. Kundermann B, Krieg JC, Schreiber W, Lautenbacher S. The effect of sleep deprivation on pain. Pain Res Manag. 2004;9(1):25–32. doi:10.1155/2004/949187
19. Shearer WT, Reuben JM, Mullington JM, et al. Soluble TNF-α receptor 1 and IL-6 plasma levels in humans subjected to the sleep deprivation model of spaceflight. J Allergy Clin Immunol. 2001;107(1):165–170. doi:10.1067/mai.2001.112270
20. Liu PY, Irwin MR, Krueger JM, Gaddameedhi S, Van Dongen HPA. Night shift schedule alters endogenous regulation of circulating cytokines. Neurobiol Sleep Circadian Rhythms. 2021;10:100063. doi:10.1016/j.nbscr.2021.100063
21. Irwin MR, Olmstead R, Carroll JE. Sleep disturbance, sleep duration, and inflammation: a systematic review and meta-analysis of cohort studies and experimental sleep deprivation. Biol Psychiatry. 2016;80(1):40–52. doi:10.1016/j.biopsych.2015.05.014
22. Besedovsky L, Lange T, Haack M. The sleep-immune crosstalk in health and disease. Physiol Rev. 2019;99(3):1325–1380. doi:10.1152/physrev.00010.2018
23. Tang NK, Lereya ST, Boulton H, Miller MA, Wolke D, Cappuccio FP. Nonpharmacological treatments of insomnia for long-term painful conditions: a systematic review and meta-analysis of patient-reported outcomes in randomized controlled trials. Sleep. 2015;38(11):1751–1764. doi:10.5665/sleep.5158
24. Williams RM, Day MA, Ehde DM, et al. Effects of hypnosis vs mindfulness meditation vs education on chronic pain intensity and secondary outcomes in Veterans: a randomized clinical trial. Pain. 2022;163(10):1905–1918. doi:10.1097/j.pain.0000000000002586
25. Williams RM, Ehde DM, Day M, et al. The chronic pain skills study: protocol for a randomized controlled trial comparing hypnosis, mindfulness, and pain education in Veterans. Contemp Clin Trials. 2020;90:105935. doi:10.1016/j.cct.2020.105935
26. Dworkin RH, Turk DC, Farrar JT, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005;113(1–2):9–19. doi:10.1016/j.pain.2004.09.012
27. Callahan CM, Unverzagt FW, Hui SL, Perkins AJ, Hendrie HC. Six-item screener to identify cognitive impairment among potential subjects for clinical research. Med Care. 2002;40(9):771–781. doi:10.1097/00005650-200209000-00007
28. Jensen MP. Treatments That Work: Hypnosis for Chronic Pain Management: Therapist Guide. New York: Oxford University Press; 2011.
29. McEachrane-Gross FP, Liebschutz JM, Berlowitz D. Use of selected complementary and alternative medicine (CAM) treatments in veterans with cancer or chronic pain: a cross-sectional survey. BMC Complement Altern Med. 2006;6:34. doi:10.1186/1472-6882-6-34
30. Davidson RJ, Goleman DJ. The role of attention in meditation and hypnosis: a psychobiological perspective on transformations of consciousness. Int J Clin Exp Hyp. 1977;25(4):291–308. doi:10.1080/00207147708415986
31. Day MA, Thorn BE, Ward LC, et al. Mindfulness-based cognitive therapy for the treatment of headache pain: a pilot study. Clin J Pain. 2014;30(2):152–161. doi:10.1097/AJP.0b013e318287a1dc
32. Day MA, Ehde DM, Burns J, et al. A randomized trial to examine the mechanisms of cognitive, behavioral and mindfulness-based psychosocial treatments for chronic pain: study protocol. Contemp Clin Trials. 2020;93:106000. doi:10.1016/j.cct.2020.106000
33. Zeidan F, Grant JA, Brown CA, McHaffie JG, Coghill RC. Mindfulness meditation-related pain relief: evidence for unique brain mechanisms in the regulation of pain. Neurosci Lett. 2012;520(2):165–173. doi:10.1016/j.neulet.2012.03.082
34. Wilson M, Skeiky L, Muck RA, et al. Pain catastrophizing mediates the relationship between pain intensity and sleep disturbances in U.S. veterans with chronic pain. Military Med. 2022:usac065. doi:10.1093/milmed/usac065.
35. Freynhagen R, Baron R, Gockel U, Tölle TR. painDETECT: a new screening questionnaire to identify neuropathic components in patients with back pain. Curr Med Res Opin. 2006;22(10):1911–1920. doi:10.1185/030079906X132488
36. Bennett MI, Smith BH, Torrance N, Potter J. The S-LANSS score for identifying pain of predominantly neuropathic origin: validation for use in clinical and postal research. J Pain. 2005;6(3):149–158. doi:10.1016/j.jpain.2004.11.007
37. Yu L, Buysse DJ, Germain A, et al. Development of short forms from the PROMIS™ sleep disturbance and sleep-related impairment item banks. Behav Sleep Med. 2011;10(1):6–24. doi:10.1080/15402002.2012.636266
38. Kushida CA, Chang A, Gadkary C, Guilleminault C, Carrillo O, Dement WC. Comparison of actigraphic, polysomnographic, and subjective assessment of sleep parameters in sleep-disordered patients. Sleep Med. 2001;2(5):389–396. doi:10.1016/s1389-9457(00)00098-8
39. Sullivan MJL, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. 1995;7(4):524–532. doi:10.1037/1040-3590.7.4.524
40. Zyphur MJ, Allison PD, Tay L, et al. From data to causes I: building a general cross-lagged panel model (GCLM). Organ Res Methods. 2020;23(4):651–687. doi:10.1177/1094428119847278
41. Van Dongen HPA, Baynard MD, Maislin G, Dinges DF. Systematic interindividual differences in neurobehavioral impairment from sleep loss: evidence of trait-like differential vulnerability. Sleep. 2004;27(3):423–433.
42. Fillingim RB. Individual differences in pain: understanding the mosaic that makes pain personal. Pain. 2017;158(Suppl 1):S11–S18. doi:10.1097/j.pain.0000000000000775
43. Watson NF, Badr MS, Belenky G, et al. Recommended amount of sleep for a healthy adult: a joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society. Sleep. 2015;38(6):843–844. doi:10.5665/sleep.4716
44. Sullivan MJL. The Pain Catastrophizing Scale User Manual. Montreal, Quebec: School of Physical and Occupational Therapy, McGill University; 1995.
45. Buysse DJ, Yu L, Moul DE, et al. Development and validation of patient-reported outcome measures for sleep disturbance and sleep-related impairments. Sleep. 2010;33(6):781–792. doi:10.1093/sleep/33.6.781
46. Tan G, Rintala DH, Jensen MP, Fukui T, Smith D, Williams W. A randomized controlled trial of hypnosis compared with biofeedback for adults with chronic low back pain. Eur J Pain. 2015;19(2):271–280. doi:10.1002/ejp.545
47. McKernan LC, Finn MTM, Crofford LJ, Kelly AG, Patterson DR, Jensen MP. Delivery of a group hypnosis protocol for managing chronic pain in outpatient integrative medicine. Int J Clin Exp Hypn. 2022;70(3):227–250. doi:10.1080/00207144.2022.2096455
48. Rizzo RRN, Medeiros FC, Pires LG, et al. Hypnosis enhances the effects of pain education in patients with chronic nonspecific low back pain: a randomized controlled trial. J Pain. 2018;19(10):1103.e1–1103.e9. doi:10.1016/j.jpain.2018.03.013
49. Borbély AA. A two process model of sleep regulation. Hum Neurobiol. 1982;1(3):195–204.
50. Buckheit KA, Nolan J, Possemato K, et al. Insomnia predicts treatment engagement and symptom change: a secondary analysis of a web-based CBT intervention for veterans with PTSD symptoms and hazardous alcohol use. Transl Behav Med. 2022;12(1):ibab118. doi:10.1093/tbm/ibab118
51. Bovin MJ, Black SK, Rodriguez P, et al. Development and validation of a measure of PTSD-related psychosocial functional impairment: the inventory of psychosocial functioning. Psychol Serv. 2018;15(2):216–229. doi:10.1037/ser0000220
52. Li MT, Robinson CL, Ruan QZ, et al. The influence of sleep disturbance on chronic pain. Curr Pain Headache Rep. 2022;26(10):795–804. doi:10.1007/s11916-022-01074-2
53. Turk DC, Fillingim RB, Ohrbach R, et al. Assessment of psychosocial and functional impact of chronic pain. J Pain. 2016;17(9 Suppl):T21–T49. doi:10.1016/j.jpain.2016.02.006
54. Ong JC, Ulmer CS, Manber R. Improving sleep with mindfulness and acceptance: a metacognitive model of insomnia. Behav Res Ther. 2012;50(11):651–660. doi:10.1016/j.brat.2012.08.001
55. Becker PM. Hypnosis in the management of sleep disorders. Sleep Med Clin. 2015;10(1):85–92. doi:10.1016/j.jsmc.2014.11.003
56. Ong JC, Moore C. What do we really know about mindfulness and sleep health? Curr Opin Psychol. 2020;34:18–22. doi:10.1016/j.copsyc.2019.08.020
57. Wofford N, Snyder M, Corlett CE, Elkins GR. Systematic review of hypnotherapy for sleep and sleep disturbance. Int J Clin Exp Hypn. 2023;71(3):176–215. doi:10.1080/00207144.2023.2226177
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.