")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 19
Severe Acute Exacerbations of Chronic Obstructive Pulmonary Disease: Are There Significant Differences Between Hospitalized and Emergency Department Patients?
Authors Saint-Pierre MD
Received 7 November 2023
Accepted for publication 10 January 2024
Published 16 January 2024 Volume 2024:19 Pages 133—138
DOI https://doi.org/10.2147/COPD.S447477
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jill Ohar
Mathieu D Saint-Pierre1– 3
1University of Ottawa, Faculty of Medicine, Ottawa, ON, Canada; 2Institut du Savoir Montfort, Ottawa, ON, Canada; 3Montfort Hospital, Division of Respirology, Ottawa, ON, Canada
Correspondence: Mathieu D Saint-Pierre, Montfort Hospital, 713 Montreal Road, Ottawa, ON, K1K 0T2, Canada, Email [email protected]
Rationale: Current guidelines define a severe acute exacerbation of chronic obstructive pulmonary disease (AECOPD) as an increase in symptoms requiring hospital admission or emergency department (ED) visit. Little is known about whether or not subjects requiring hospitalization and those needing only ED care have similar patient profiles and if their clinical outcomes appear comparable.
Objective: The main goals of this study were to compare the demographic and clinical characteristics of patients treated for an AECOPD with an inpatient admission versus an ED visit and to review if hospital resource utilization was different between the 2 groups after discharge.
Methods: Subjects treated in 2022 at Montfort Hospital for an AECOPD were reviewed. Patient demographic information was collected in addition to spirometry results and blood eosinophil counts on file. Supplemental oxygen use and medication lists were also recorded. Patients with an initial hospital admission were compared to those requiring only ED care with univariate and multivariate analyses. We also assessed if subjects were again treated for an AECOPD up to 6 months post initial discharge, and if so, the type of hospital visits (hospitalization or ED).
Measurements and Main Results: A total of 135 individuals necessitated hospitalization and 79 received ED care for the treatment of an AECOPD. On univariate analysis, patients requiring an inpatient stay appeared older and were more likely to have spirometry results on file. A greater proportion of hospitalized individuals were on supplemental oxygen and prescribed at least one long-acting inhaled medication. These studied variables remained significant after multivariate logistic regression analysis. Subjects with an initial inpatient admission were also more likely to require hospitalization upon repeat presentation for a severe AECOPD.
Conclusion: Given the important differences observed in both patient characteristics and hospital resource utilization, this study supports considering an AECOPD requiring inpatient admission versus an ED visit as distinct categories of events.
Keywords: chronic obstructive pulmonary disease, guidelines, severe acute exacerbation, hospitalization, emergency department
Introduction
Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) represents an important cause of both hospitalizations and emergency department (ED) visits.1 In fact, AECOPD is the most prevalent cause of inpatient admission in Canada aside from childbirth, with recent data showing an upward trend in hospitalizations since 2010.2,3 National spending for AECOPD requiring hospital care is at least 4 billion Canadian dollars per year.4 Both the Global Initiative for Chronic Obstructive Lung Disease (GOLD) report and the Canadian Thoracic Society (CTS) guidelines define the severity of an AECOPD based on healthcare resource utilization, with a severe event considered as an increase in COPD symptoms beyond day-to-day variability and requiring hospital admission or ED visit. A moderate AECOPD is characterized as an episode treated in an outpatient setting with oral corticosteroids (OCS) and/or antibiotic, while a mild AECOPD necessitates only short-acting bronchodilator use.5–7
Despite this apparent global consensus regarding the definition of a severe AECOPD, little is known about whether or not subjects requiring an inpatient admission and those only needing ED care have similar patient profiles and if their clinical outcomes appear comparable. Therefore, the primary objectives of this study were to assess in a real-world setting the demographic and clinical characteristics of patients treated for an AECOPD with hospitalization versus an ED visit and to review if hospital resource utilization was different between the 2 groups up to 6 months after the initial discharge.
Materials and Methods
After local research ethics board (REB) approval (Montfort Hospital file #22-23-02-052), all individuals treated in 2022 for an AECOPD at Montfort Hospital (Ottawa, Ontario, Canada) were reviewed. Patient consent was not required by the REB as this was a retrospective study; data was anonymized and kept strictly confidential. All ethical principles set out in the Declaration of Helsinki were followed. Montfort Hospital is an academic teaching hospital affiliated with the University of Ottawa that provides acute care to approximately 1.5 million people. Patients receiving usual inpatient care are admitted under Family Medicine or General Internal Medicine physicians, while those requiring intensive care are managed by board-certified intensivists. Subjects assessed in the ED are treated by emergency medicine specialists. Patients are often co-managed by trainees such as medical students and residents.
Lists for both inpatient and ED visits were provided by the hospital archives department based on having a discharge diagnosis (clinician-based) of AECOPD. Patients with other reported pulmonary disorders were excluded from this review. Subjects with a primary diagnosis of pneumonia, influenza, or coronavirus disease 2019 were also removed.
Patient demographic information collected included age, gender, cigarette smoking history, and the presence of a primary care provider (PCP). Patient mortality in the hospital was recorded. Spirometry results and all blood eosinophil counts (BEC) on the hospital’s electronic medical records (EMR) system were reviewed. Home supplemental oxygen use was also charted, in addition to long-acting inhaled medications at the time of hospital presentation. Lastly, we reviewed if subjects were again treated at Montfort Hospital for an AECOPD after 1 month and after 6 months post-discharge, and if so, the type of hospital visits (hospitalization or ED).
Univariate analysis was first completed to compare the clinical characteristics and prescribed therapies of subjects requiring an initial hospital admission versus only ED care. Student’s t-test was used for continuous variables and Pearson’s chi-squared test for categorical variables. Continuous results were presented as means with range and categorical results as total numbers and percentages. Multivariate logistic regression analysis was subsequently performed. Readmissions for AECOPD (and hospital visit type) were also compared using a t-test and chi-squared method. A statistically significant relationship was defined as p < 0.05. All statistical analyses were completed using IBM SPSS Statistics version 29 (Armonk, New York).
Results
A total of 135 individuals were hospitalized at Montfort Hospital in 2022 for an AECOPD (mean length of stay of 8 days), with 16 requiring admission to the intensive care unit. Eight subjects died in the hospital. Seventy-nine patients were treated in the ED without hospitalization.
On univariate analysis, patients requiring an inpatient stay for the treatment of an AECOPD appeared on average older (71 versus 67 years old, p < 0.01), were more likely to have prior spirometry on file (50% versus 30%, p < 0.01), and had lower mean % predicted forced expiratory volume in the first second (FEV1) (46% versus 57%, p = 0.03). Patients treated with only an ED visit less often had a PCP on file (73% versus 84%, p = 0.07). A greater proportion of hospitalized individuals were on home supplemental oxygen (27% versus 9%, p < 0.01) and prescribed at least one long-acting inhaled medication at the time of initial presentation (92% versus 71%, p < 0.01). 55% were already on triple therapy (long-acting muscarinic antagonist, long-acting beta-agonist, and inhaled corticosteroid) compared to 38% for patients treated in the ED (p = 0.02). Mean cigarette smoking history was similar between both groups (50 versus 54 pack-years for hospitalized and ED patients, p = 0.56). No significant relationship was found with gender, current smoking status, or mean peak BEC on file (Table 1).
 |
Table 1 Univariate Analysis of Patient Characteristics and Prescribed Therapies for Subjects Presenting with a Severe Acute Exacerbation of Chronic Obstructive Pulmonary Disease |
Older age, the presence of prior spirometry on file, and the use of supplemental oxygen at home remained predictive of hospitalization for AECOPD after multivariate logistic regression analysis. Patients on no long-acting inhaled medication at the time of presentation were more likely to only require ED care (Table 2). The limited proportion (43%) of patients with available % predicted FEV1 results unfortunately precluded the inclusion of this variable in the multivariate model.
 |
Table 2 Multivariate Logistic Regression Analysis of Patient Characteristics and Prescribed Therapies for Subjects Presenting with a Severe Acute Exacerbation of Chronic Obstructive Pulmonary Disease |
There were overall 37 hospital visits for an AECOPD after 1 month and 113 after 6 months post-discharge. Patients with an initial inpatient admission were more likely to require hospitalization upon repeat presentation for AECOPD compared to those with an initial ED visit (65% versus 27% of severe AECOPD after 1 month, p = 0.03, and 75% versus 43% of severe AECOPD after 6 months, p = 0.01) (Table 3).
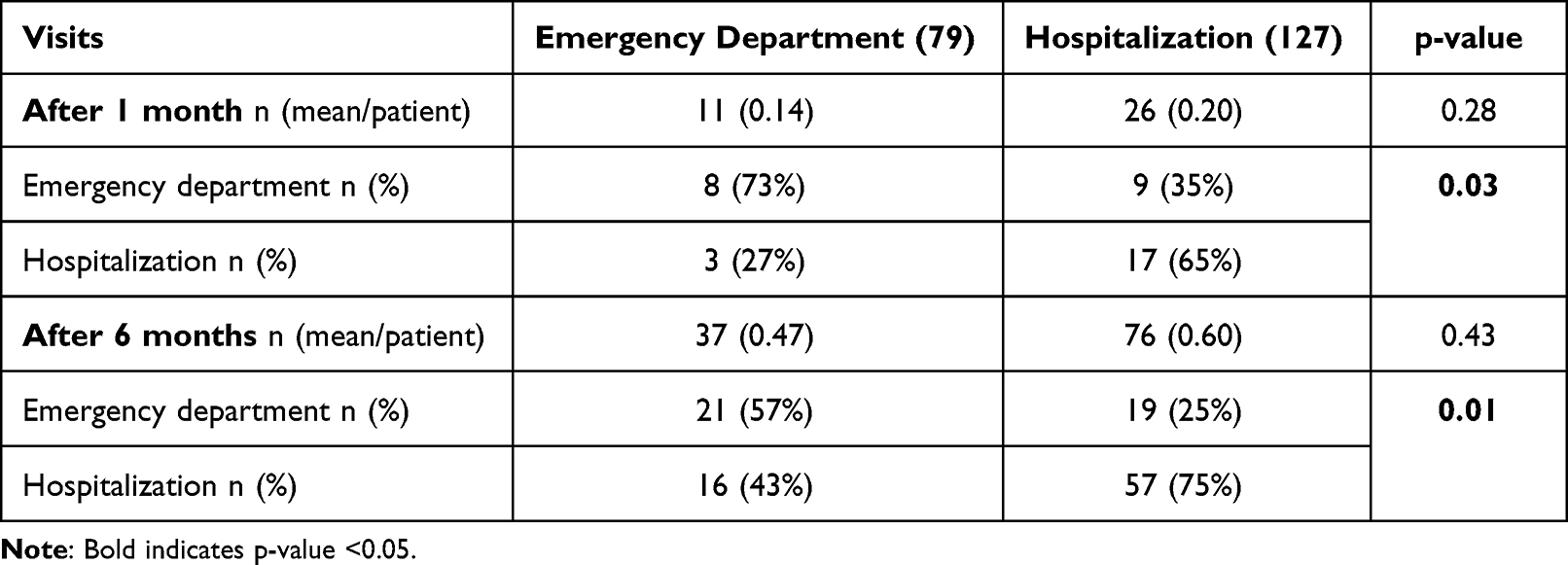 |
Table 3 Visits for a Severe Acute Exacerbation of Chronic Obstructive Pulmonary Disease After 1 and 6 Months Post-Discharge |
Discussion
The GOLD and CTS COPD statements are used to guide clinical treatment decisions. Currently, patients are considered to be at higher risk of future AECOPD if they have had 2 or more moderate or at least 1 severe AECOPD in the prior year.5,7 Therefore, any hospital presentation for COPD would lead to the recommendation of a potentially more intensive treatment strategy. Severe AECOPD has been described to cause worsening patient symptoms and quality of life, accelerated decline of lung function, increased risk of future AECOPD, and can lead to death.8–14 It would however appear important to determine if and how these outcomes may differ in patients necessitating an inpatient admission versus only ED care.
In most healthcare models, patients can self-present to the ED. An AECOPD treated in this setting could have often been addressed in an outpatient clinic, and therefore labeled as either a mild or moderate event. Although outside the scope of this hospital-based review, it appears reasonable to suspect that patients discharged from the ED with a course of OCS and/or an antibiotic for an AECOPD likely have similar clinical outcomes compared to subjects treated the same way in an office setting. An AECOPD requiring hospitalization is also associated with a much greater financial cost.15
There is also marked variability regarding access to medical care in Canada and between different countries.16,17 Approximately 15% of the population of Ottawa does not have a PCP, and these affected individuals are often forced to go to the ED for any severity of complaint.18 Indeed, it was identified that 27% of patients treated at the Montfort Hospital ED did not have a PCP on file. The lack of a PCP has previously been identified as a risk factor for ED presentation during an AECOPD.19 In this context, subjects may also be more likely to present to the ED with a first presentation of their disease. This may in part explain why more ED-treated patients were not on long-acting inhaled therapy (29%).
Given the shortcomings of grading the severity of an AECOPD based on healthcare resource utilization, there have been efforts to revise these criteria. Recently published trials that assessed the potential benefits of single-inhaler triple therapy medications have defined a severe AECOPD as an event resulting in hospital admission or death, removing a typical ED visit from this category.20–22 Furthermore, the Rome proposal attempted to integrate objectively measurable variables to help classify events as mild, moderate, or severe. This international panel of experts suggested that a severe AECOPD requires blood gas values indicating acidotic hypercapnic respiratory failure.23
This study has certain limitations. We must consider that some patients may have been misdiagnosed by physicians as having COPD instead of another condition. It is possible that other clinical factors not included in this review may lead to a higher probability of inpatient admission for an AECOPD, such as patient functional status and comorbidities. Individuals may have had pulmonary function testing done in another healthcare center, with results not available on the hospital EMR platform. The minority of patients had % predicted FEV1 values on file at Montfort Hospital, which prevented its inclusion in the multivariate analysis. Certain patients could have also been treated for a severe AECOPD in another institution after their initial visit to Montfort Hospital, and therefore not accounted for when reviewing subsequent hospital visits.
Conclusions
Patients hospitalized for an AECOPD appeared to have more advanced disease compared to those treated in the ED. Furthermore, the initial visit type was predictive of hospital resource utilization for the treatment of a subsequent AECOPD. The study results highlight the need to better define what should be labeled as a severe AECOPD. It would seem more appropriate to consider an AECOPD requiring hospitalization versus only ED care as distinct categories of events.
Abbreviations
AECOPD, acute exacerbation of chronic obstructive pulmonary disease; BEC, blood eosinophil counts; CTS, Canadian Thoracic Society; ED, emergency department; EMR, electronic medical records; FEV1, forced expiratory volume in the first second; GOLD, Global Initiative for Chronic Obstructive Lung Disease; OCS, oral corticosteroids; PCP, primary care provider; REB, research ethics board.
Funding
Montfort Hospital.
Disclosure
No conflicts exist for the author.
References
1. Gershon AS, Guan J, Victor JC, Goldstein R, To T. Quantifying health services use for chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2013;187(6):596–601. doi:10.1164/rccm.201211-2044OC
2. Canadian Institute for Health Information. Hospital stays in Canada report; 2020.
3. Amegadzie JE, Lee TY, Sadatsafavi M, Lynd LD, Sin DD, Johnson KM. Trends in hospital admissions for chronic obstructive pulmonary disease over 16 years in Canada. Can Med Ass J. 2023;195(35):E1172–E1179.
4. Canadian Lung Association. Pre-budget consultations house of commons; 2011.
5. Global initiative for chronic obstructive lung disease 2023 report. Available from: https://goldcopd.org/2023-gold-report-2/.
6. Bourbeau J, Bhutani M, Hernandez P, et al. Canadian thoracic society clinical practice guideline on pharmacotherapy in patients with COPD – 2019 update of evidence. Can J Respir Crit Care Sleep Med. 2019;3:210–232. doi:10.1080/24745332.2019.1668652
7. Bourbeau J, Bhutani M, Hernandez P, et al. 2023 Canadian thoracic society guideline on pharmacotherapy in patients with stable COPD. Can J Respir Crit Care Sleep Med. 2023;7:173–191. doi:10.1080/24745332.2023.2231451
8. Wedzicha JA, Brill SE, Allinson JP, Donaldson GC. Mechanisms and impact of the frequent exacerbator phenotype in chronic obstructive pulmonary disease. BMC Med. 2013;11(1):181. doi:10.1186/1741-7015-11-181
9. Wilkinson TMA, Donaldson GC, Hurst JR, Seemungal TAR, Wedzicha JA. Early therapy improves outcomes of exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2004;169(12):1298–1303. doi:10.1164/rccm.200310-1443OC
10. Dransfield MT, Kunisaki KM, Strand MJ, et al. Acute exacerbations and lung function loss in smokers with and without chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2017;195(3):324–330. doi:10.1164/rccm.201605-1014OC
11. Watz H, Tetzlaff K, Magnussen H, et al. Spirometric changes during exacerbations of COPD: a post hoc analysis of the WISDOM trial. Respir Res. 2018;19(1):251. doi:10.1186/s12931-018-0944-3
12. Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. New Engl J Med. 2010;363(12):1128–1138. doi:10.1056/NEJMoa0909883
13. Soler-Cataluña JJ, Martínez-García MÁ, Román Sánchez P, Salcedo E, Navarro M, Ochando R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925–931. doi:10.1136/thx.2005.040527
14. Ho TW, Tsai YJ, Ruan SY, Huang CT, Lai F, Yu CJ. In-hospital and one-year mortality and their predictors in patients hospitalized for first-ever chronic obstructive pulmonary disease exacerbations: a nationwide population-based study. PLoS One. 2014;9(12):e114866. doi:10.1371/journal.pone.0114866
15. Mittmann N, Kuramoto L, Seung S, Haddon J, Bradley-Kennedy C, FitzGerald J. The cost of moderate and severe COPD exacerbations to the Canadian healthcare system. Respir Med. 2008;102(3):413–421. doi:10.1016/j.rmed.2007.10.010
16. Hasegawa K, Tsugawa Y, Tsai CL, Brown DF, Camargo J. Frequent utilization of the emergency department for acute exacerbation of chronic obstructive pulmonary disease. Respir Res. 2014;15(1):40. doi:10.1186/1465-9921-15-40
17. Rowe BH, Cydulka RK, Tsai CL, Clark S, Sinclair D, Camargo J. Comparison of Canadian versus United States emergency department visits for chronic obstructive pulmonary disease exacerbation. Canad Resp J. 2008;15(6):295–301. doi:10.1155/2008/696482
18. Payne E. Up to 150,000 Ottawa residents don’t have access to primary care: Ottawa public health. Ottawa Citizen. 2023;2023:1.
19. Tsai CL, Griswold SK, Clark S, Camargo CA. Factors associated with frequency of emergency department visits for chronic obstructive pulmonary disease exacerbation. J Gen Intern Med. 2007;22(6):799–804. doi:10.1007/s11606-007-0191-7
20. Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. New Engl J Med. 2018;378(18):1671–1680. doi:10.1056/NEJMoa1713901
21. Papi A, Vestbo J, Fabbri L, et al. Extrafine inhaled triple therapy versus dual bronchodilator therapy in chronic obstructive pulmonary disease (TRIBUTE): a double-blind, parallel group, randomised controlled trial. Lancet. 2018;391(10125):1076–1084. doi:10.1016/S0140-6736(18)30206-X
22. Rabe KF, Martinez FJ, Ferguson GT, et al. Triple inhaled therapy at two glucocorticoid doses in moderate-to-very-severe COPD. N Engl J Med. 2020;383(1):35–48. doi:10.1056/NEJMoa1916046
23. Celli BR, Fabbri LM, Aaron SD, et al. An updated definition and severity classification of chronic obstructive pulmonary disease exacerbations. Am J Respir Crit Care Med. 2021;204(11):1251–1258. doi:10.1164/rccm.202108-1819PP
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.