")
Back to Journals » Clinical Ophthalmology » Volume 16
Rub and Rinse Contact Lenses Before Wearing as a Protective Regimen Against Contact Lens-Related Eye Infections
Authors Juhong J, Mordmuang A , Jewboonchu J, Rattanathamma P, Narkkul U , Karnjana K , Udomwech L
Received 5 January 2022
Accepted for publication 21 February 2022
Published 1 March 2022 Volume 2022:16 Pages 567—577
DOI https://doi.org/10.2147/OPTH.S357099
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Jakkrit Juhong,1,2 Auemphon Mordmuang,1 Juntamanee Jewboonchu,1 Phisut Rattanathamma,3 Udomsak Narkkul,1 Kulwadee Karnjana,1 Lunla Udomwech1,2
1School of Medicine, Walailak University, Nakhon Si Thammarat, 80160, Thailand; 2Department of Ophthalmology, Walailak University Hospital, Walailak University, Nakhon Si Thammarat, 80160, Thailand; 3Department of Otolaryngology, Walailak University Hospital, Walailak University, Nakhon Si Thammarat, 80160, Thailand
Correspondence: Lunla Udomwech, School of Medicine, Walailak University, 222 Thaiburi, Tha Sala, Nakhon Si Thammarat, 80160, Thailand, Tel +66 7567 2875, Fax +66 7567 2807, Email [email protected]
Purpose: Data on contact lens (CL) users in Thailand are limited, and previous reports have mainly focused on young populations. This study aims to determine demographic data, hygienic behaviour, and complications related to the usage of CLs in the general population.
Methods: This was a cross-sectional survey conducted from November 2020 to March 2021 using an anonymous questionnaire. Information on the demographic traits of the participants, characteristics of CL use, and CL care behaviours was collected. The responses were summarised and presented as a total behaviour score. Regression analysis was performed to evaluate the potential risk factors for a history of CL-related eye infections.
Results: A total of 134 CL wearers were recruited. Of all the participants, 83.58% were female and 16.42% were male. The average age was 31.14± 10.69 years old. The total behaviour score showed that 62.69% of the population had good CL behaviour, while 37.31% exhibited poor CL behaviour. More than 50% of participants practised appropriate CL handling. Common unfavourable behaviours (> 50%) reported were not using CL care solution to clean the storage case, not rubbing and rinsing the lens before storage, exposure to water during wear, use of makeup around the ocular area, and missing annual eye exams. Other less common but important instances of mishandling included using tap water to clean the lenses, topping off old CL solution, and exceeding the recommended planned-replacement period. However, no behaviours were significantly associated with a history of CL-related eye infections. Rubbing and rinsing CLs before wearing them was found to be a protective factor against a history of eye infections.
Conclusion: Rubbing and rinsing CLs before wearing should be mentioned as an additional recommendation for the user.
Keywords: behaviour, contact lens care, rubbing and rinsing, contact lens-related infection, mishandling contact lens
Introduction
Contact lenses (CLs) are thin lenses placed directly on the eye’s surface, mainly for correcting refractive errors, cosmetic purposes, and as a therapeutic modality for some corneal pathologies.1 The number of CL wearers continues to rise globally, both in developed and developing countries.2 CLs provide a safe and effective way to correct vision. On the other hand, CL wearers may risk eye infections if their lenses are not correctly used, cleansed, disinfected, and stored.3 There are an estimated 125 million CL wearers around the world, with 6% of them experiencing complications each year.4 These problems can range from blepharitis, meibomian gland dysfunction, conjunctivitis, to sight-threatening ulcerative keratitis and endophthalmitis.5
A study of compliance behaviours for CL-related eye infections in the United States reported that 99% of CL wearers engaged in at least one compliance behaviour regarding CL hygiene, and 33% reported having experienced a previous CL-related eye complication requiring a doctor’s visit. The most common poor CL behaviours were CL overuse and sleeping with one’s lenses on.6 Among university students in Thailand, poor CL behaviours were related to purchasing lenses from the internet, wearing them for over one year, and long wear duration (>12 hours).7 A number of studies provide information on the prevalence of usage, knowledge, and risky behaviours of CL care, especially in young populations.7–9 However, there are limited studies about the relationship between the behaviour and compliance of CL users in the general population in Thailand. This study aims to establish the demographic data, compliance, and history of complications related to the usage of CLs in Thailand, and to identify risky behaviours related to a history of eye infections. The results offer practical knowledge and underscore the importance of adherence to good CL routine care, which might be further integrated into public health prevention policies to prevent undesirable events for CL wearers in the future.
Methods
A cross-sectional survey was conducted from November 2020 to March 2021, with all eligible participants recruited consecutively. A recruitment notice was placed at Walailak University Hospital’s Contact Lens Clinic, various institutions in Thailand, and online. Participants who were interested gave internet-based informed consent and completed an online questionnaire using the Google Form platform. All the tenets of the Declaration of Helsinki were adhered to, and the research team was granted permission from Walailak University’s Institutional Review Board before the first participant was enrolled (WUEC-20-321-01). Inclusion criteria mandated that the participants have worn their CLs on average at least once weekly in the past month. There was no age limit for this study; however, participants who were younger than 18 needed to give their own consent, as well as obtain permission from their parents or guardians before taking part. Exclusion criteria included those who could not give informed consent. The questionnaire was adapted from the American Academy of Ophthalmology and a European study for CL-related microbial keratitis10,11 with permission and consisted of 4 parts. The first part involved demographic information (eg age, gender, education level, objective CL use, and experience wearing CLs). The second part entailed the CL type and details of CL use (eg type of lens materials, type of CL, frequency of wear, cleaning solution, consultation for CL care, and place of purchase). The third and fourth parts consisted of 35 items that asked about the participants’ wear and care behaviours. Answers to the questions in the third and fourth parts were summarised to determine the total behaviour scores. Participants who received a score of ≥ 80% were described as having good behaviour. All the questions in each part are available in the Appendix. Both descriptive and inferential statistics were applied to the survey data. Demographic data were analysed using descriptive analysis, mean ± standard deviation (SD), median, frequency, and percentage as appropriate. Logistic regression analysis was performed to identify any association of the independent categorical variables, including participant demographic data, characteristics of CL use, wear and care behaviour, and total behaviour scores with a history of CL-related eye infections. The factors that showed univariate P value less than 0.2 and the variables that have been reported as a significant factor in previous studies were selected for determination of adjusted odds ratio (AOR) using multivariate method. Analyses were carried out using IBM SPSS Statistics for Windows, version 23.0 (SPSS, Chicago, IL). P values less than 0.05 were considered statistically significant.
Results
Demographics and Characteristics of CL Use in the Participants
A total of 134 CL wearers were recruited for this study. Of all the participants, 112 (83.58%) were female and 22 (16.42%) were male. The average age was 31.14±10.69 years old (median: 31.00, range: 15–74 years). A summary of the participants’ demographic data is shown in Table 1. The education level of the population demonstrated that 20.90% had less than college degree, and 79.1% had received college degree education or higher. The main objective of using CLs was mostly to correct refractive errors (94.02%), less than 4.48% for cosmetics, and 1.50% for the treatment of corneal disease. Most of the participants (approximately 70%) had experience wearing CLs for more than a year, 33.58% had worn CLs for 1 to 5 years, and 36.57% had worn CLs for 6 to 10 years. The use of rigid gas-permeable (RGP) CLs and soft CLs were 5.22% and 94.78%, respectively. Soft CLs consisted of 61.42% of CLs for refractive correction, and 38.58% were cosmetic, coloured CLs. All soft CL wearers used either disposable or reusable CLs on a daily basis, or planned replacements. The most popular replacement plan interval was monthly, utilised by 82.10% of the participants. The daily, weekly, and biweekly replacement plans were minorities. A proportion of 54.48% wore CLs daily. Multipurpose solutions were the most popular method for disinfecting reusable CLs (86.57%), and only 1.49% used a hydrogen peroxide system. Normal saline was used solely as a means to clean the lenses by 11.94% of the population. Regarding patient evaluation and education, most participants received CL handling instructions from opticians in optical shops. However, more than 25% sought information by themselves without any recommendations from eye care professionals. The data are shown in Table 2.
 |
Table 1 Participants’ Demographic Data |
 |
Table 2 Types and Details of CLs Used |
Wear and Care Behaviours
The questions used to determine the participants’ wear and care behaviours are presented in Table 3. The behaviours of CL wearing and hygiene practices were evaluated and scored to classify the participants as having either good or poor behaviour; 84 (62.69%) participants had good behaviour, while 50 (37.31%) had poor behaviour. More than 60% used CLs properly, such as wearing CLs for less than 8 hours a day, always checking the packaging and expiration date, correcting the sides of CLs before putting them in, washing one’s hands with soap before lens handling, and putting CLs in and removing them starting from the same eye. However, part of the population harboured inappropriate behaviours that could contaminate the lens or disinfecting system, such as not washing one’s hands with soap before putting CLs in and taking them out (2.24% and 11.19%, respectively), using a lens that had been dropped (41.04%), sleeping with CLs in (36.57%), sharing CLs with others (1.50%), exceeding the replacement plan (49.25%), applying eye makeup (55.97%), and missing annual eye examinations (76.87%). An evaluation of participants’ CL care behaviour found that more than 50% of them showed good hygiene in handling CLs. Most of them performed the rub and rinse regimen after using their CLs and even before wearing them. Most used an appropriate CL care solution and soaked their CLs in the solution for at least 6 hours. However, some participants had risky behaviours, such as using tap water (8.96%) or normal saline solution (27.61%) to clean the lenses. Apart from CL handling, the storage case was cleaned with a CL cleaning solution (39.55%); fresh CL solution was always used each time (90.30%), and the case was replaced at least every 3 months (95.52%). As for the CL solution, the caps were always closed after use (64.18%), the CLs were renewed within 3 months (91.04%), and participants did not top off the old cleaning solution (72.39%).
 | 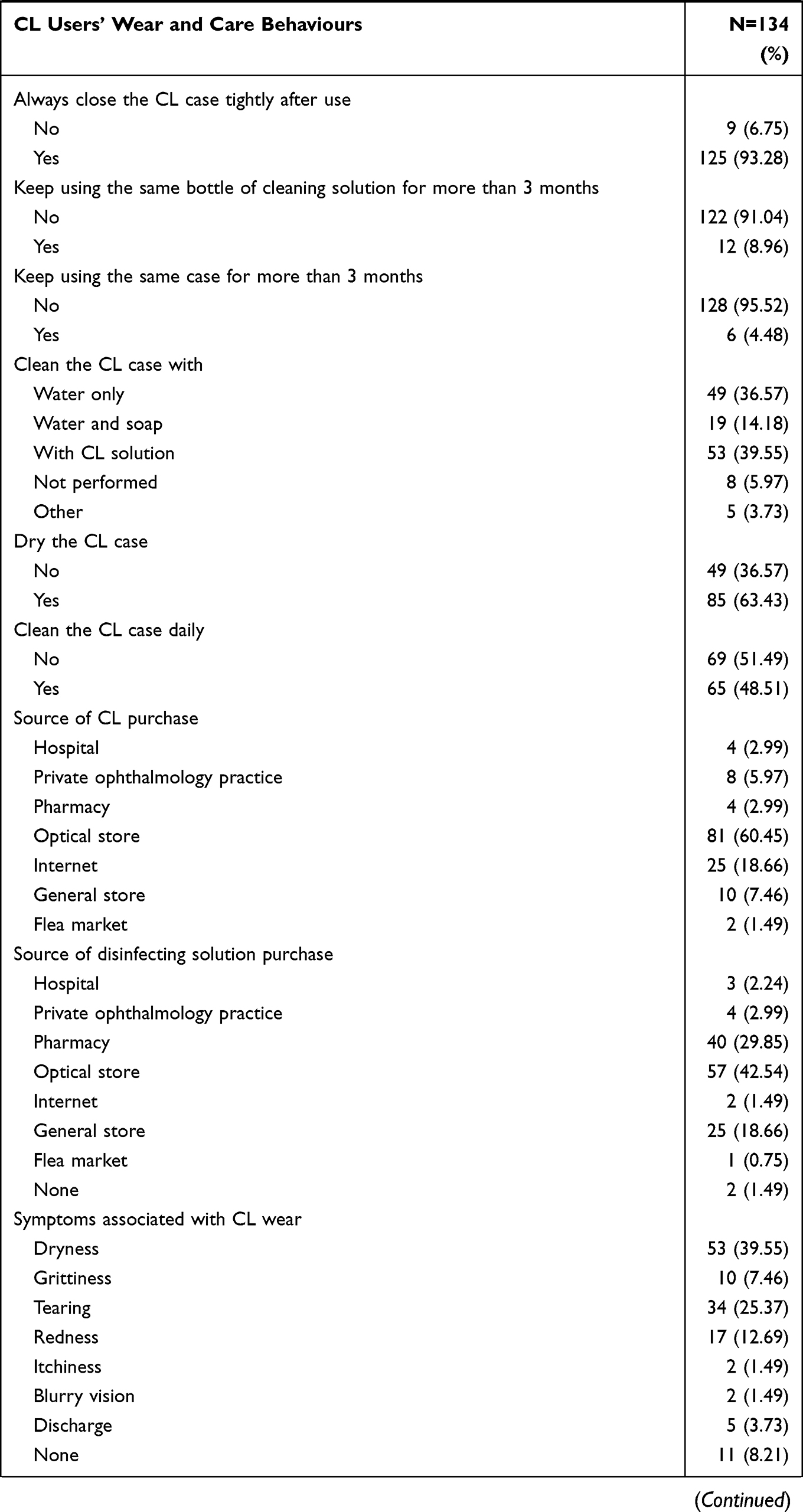 |  |
Table 3 CL Users’ Wear and Care Behaviours |
Risk Factors and CL Wearer Characteristics Associated with a History of CL-Related Ocular Infections
Univariate analysis was performed to determine the significance of the association between the participants’ demographics, wear and care behaviours, and a history of CL-related eye infections. The data are displayed in Table 4. The demographic information of CL wearers regarding gender, age, and education level did not show a significant association with a history of eye infections. The number of participants with a history of infections was nearly similar among those who wore CLs for more than 8 hours and ≤ 8 hours, without any significance. From univariate analysis, rubbing and rinsing CLs before putting them in was found to be significantly associated with less of a history of eye infections (P=0.010). Factors with P values less than 0.2 were further selected for multivariate analysis, those included education level, soaking CLs in CL cleaning solution at least 6 hours per day, rubbing and rinsing CLs before putting in, and total score of wear and care behaviours. Additionally, risky behaviours such as sleeping with one’s CLs on, showering during CL wear, applying eye makeup, exceeding the recommended planned replacement period, and soaking CLs with cleaning solution for less than 6 hours presented no statistical association with infections. The participants’ total behaviour scores were evaluated; participants with either good or poor behaviour showed no significant difference regarding a history of eye infections, with 18 out of 84 (21.42%) and 11 out of 50 (22.00%) cases per group, respectively.
 |
Table 4 Association Between Demographic Data, Wear and Care Behaviours, and History of CL-Related Ocular Infections |
Discussion
Poor CL compliance could result in CL-related complications that can range from mild to sight-threatening conditions. Age, gender, and education have influencing factors on CL compliance.12–15 Age has been reported as a factor for CL-related complications. A recent study from a tertiary hospital in China found corneal infection or inflammation to be associated with young age.5 Similar findings were discovered in a population in the United States, suggesting that younger CL wearers are less compliant with CL hygiene in replacing lenses and cases at intervals longer than recommended.16 Another report from a North American population revealed that CL-related complications were most prevalent in individuals between 15 and 25 years old.17 In Thailand, where this study took place, most reports focus on young populations, indicating improper CL hygiene, such as lens overuse, not replacing fresh cleaning solution in storage cases, swimming while wearing CLs, using tap water to clean the lenses, and not performing hand washing before lens handling.18 To determine the difference between the behaviour of the young and adult groups, we performed research in diverse settings to better represent general CL users in Thailand, resulting in a wide population age range from 15 to 74. Nonetheless, age was not found to be a risk factor for a history of eye infections.
In agreement with previous studies, CL wearers were predominantly female.12,19 Although findings from Saudi Arabia and India imply that the most common reason in females for choosing CLs is cosmetic purposes,20,21 the majority of females in the present study wore CLs to correct refractive errors. Females were previously found to be less likely to follow the replacement schedule;22 however, this outcome was not established in our study. Additionally, no significant association between sex and history of ocular infections was detected. The type of CL and behaviour were investigated to understand users’ preferences, which could suggest proper CL care and hygiene practices. The majority of CLs in the present study were monthly soft CLs, leaving RGP CLs for a minority of approximately 5%. The popularity of soft CLs was mentioned in 2020 market research from Contact Lens Spectrum, where soft lenses account for nearly 90% of lens fits in the market, with silicone hydrogels predominating. Reusable lenses were more commonly used and prescribed than daily disposable lenses.23 As long as the prescribing trend still favours reusable CLs, the risk for microbial accumulation and eye infections should always be considered. In addition, the hydrophilic properties of soft CL materials, such as hydroxyethyl methacrylate and silicone, have been recognized as the most susceptible to bacterial adhesion and may resist disinfectants, such as biofilm formation by Staphylococcus aureus and Pseudomonas aeruginosa.24 Reusable lenses require care using disinfecting solutions, daily cleaning regimens, and storage cases, in which contamination can lead to serious microbial infections in the eyes.
Focusing on CL wear and care behaviour, although most participants reported good CL care behaviour (62.69%), a large proportion of the population was confused about the steps of the CL care regimen. Most eye care professionals recommend washing, rubbing, and rinsing CLs with CL care solution immediately after taking them off and before submerging them in disinfecting solution. Most participants performed some kind of CL cleaning (rub, rinse, or rub and rinse the CLs with cleaning solution) before putting the CLs in. Paradoxically, fewer people performed such routines after taking off the CLs, and less than half of participants performed both rubbing and rinsing their CLs. This reflects the awareness of CL wearers of the CL cleaning and disinfecting process, despite inadequate knowledge. Interestingly, the practice of cleaning CLs before wearing them is the only behaviour demonstrated as a protective factor against eye infections. The actual impact of this regimen needs more clarification through research in microbiology, aiming to specifically answer this question. Should the action provide true benefit against eye infections, implementation should be encouraged. Most of the participants used CL cleaning solution and normal saline solution to clean their CLs; however, there were 12 participants and 1 participant who used tap water and saliva to clean their lenses, respectively. Using tap water led to more risk for eye infections and microbial keratitis caused by bacterial species and Acanthamoeba spp., since microorganisms from environmental contaminants may adhere to the surface of CLs.25 Another risk was noted: Half of the participants overused the recommended planned replacement period. Exceeding the lens’s planned-replacement schedule was reported to be associated with a large number of eye complications.26
Poor behaviours may be influenced by a lack of patient education and an understanding of possible complications. Since the distribution of CLs in Thailand is not regulated, it is unnecessary to consult a professional for CL fitting; thus, people receive no professional advice at the beginning. Forty percent of the studied population did not have their CLs prescribed by an eye care professional. Roughly a quarter bought their CLs from unreliable sources such as from the internet, general stores, and flea markets. Most participants did not have their eyes checked annually, but this number still reflected a healthier estimate than that of university students from a previous study in Thailand.7 Annual eye examinations can detect complications such as dry eye, conjunctivitis, and corneal neovascularisation early, and provide opportunities for ophthalmologists or optometrists to re-evaluate and emphasise good CL hygiene. Thus, CL wearers should be encouraged to check their eyes on a regular basis.
Conclusion
The observed undesirable habits, such as topping off old cleaning solution, inadequate or lack of hand washing, using lenses that have been dropped, failing to clean the CL case daily, exposure to potentially contaminated water, and overusing CLs, although were not found to be statistically associated with a history of eye infections, should still be discouraged. A finding of protective effect from cleaning CLs by rubbing and rinsing before wearing them should be mentioned as an additional recommendation for the user.
Abbreviations
AOR, adjusted odds ratio; CI, Confidence interval; CL, Contact lenses; e.g., For example; IRB, Institutional review board; N, Number; OR, odd ratio; RPG, Rigid gas permeable; SD, Standard deviation.
Acknowledgments
The authors are grateful to thank the Research Center of Excellence in Innovation of Essential Oil and Research Institute for Health Science, and the Research Center in Tropical Pathobiology, Walailak University, for their kind support and laboratory facilities.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Walailak University, Grant Number WU-IRG-63-081, 2020.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lee SY, Kim YH, Johnson D, Mondino BJ, Weissman BA. Contact lens complications in an urgent-care population: the University of California, Los Angeles, contact lens study. Eye Contact Lens. 2012;38(1):49–52. doi:10.1097/ICL.0b013e31823ff20e
2. Key JE. Development of contact lenses and their worldwide use. Eye Contact Lens. 2007;33(6 Pt 2):
3. Dart JK, Radford CF, Minassian D, Verma S, Stapleton F. Risk factors for microbial keratitis with contemporary contact lenses: a case-control study. Ophthalmology. 2008;115(10):
4. Stamler JF. The complications of contact lens wear. Curr Opin Ophthalmol. 1998;9(4):66–71. doi:10.1097/00055735-199808000-00012
5. Li W, Sun X, Wang Z, Zhang Y. A survey of contact lens-related complications in a tertiary hospital in China. Cont Lens Anterior Eye. 2018;41(2):201–204. doi:10.1016/j.clae.2017.10.007
6. Cope JR, Collier SA, Rao MM, et al. Contact lens wearer demographics and risk behaviors for contact lens-related eye infections–United States, 2014. MMWR Morb Mortal Wkly Rep. 2015;64(32):865–870. doi:10.15585/mmwr.mm6432a2
7. Supiyaphun C, Jongkhajornpong P. Contact lens use patterns, behavior and knowledge among university students in Thailand. Clin Ophthalmol. 2021;15:1249–1258. doi:10.2147/OPTH.S304735
8. Bhandari M, Hung PR. Habits of contact lens wearers toward lens care in Malaysia. Med J Malaysia. 2012;67(3):274–277.
9. Khoza N, Moodley T, Sokhulu S, et al. Knowledge, attitudes and practices of contact lens use in a South African adolescent population. Afr Health Sci. 2020;20(2):768–774. doi:10.4314/ahs.v20i2.29
10. Sauer A, Abry F, Berrod JP, et al. [Study and prevention of contact lens-related microbial keratitis with a standardized questionnaire]. J Fr Ophtalmol. 2010;33(10):701–709. French. doi:10.1016/j.jfo.2010.09.022
11. Sauer A, Bourcier T. Microbial keratitis as a foreseeable complication of cosmetic contact lenses: a prospective study. Acta Ophthalmol. 2011;89(5):e439–442. doi:10.1111/j.1755-3768.2011.02120.x
12. Wagner H, Richdale K, Mitchell GL, et al. Age, behavior, environment, and health factors in the soft contact lens risk survey. Optom Vis Sci. 2014;91(3):252–261. doi:10.1097/OPX.0000000000000164
13. Carnt N, Keay L, Willcox M, Evans V, Stapleton F. Higher risk taking propensity of contact lens wearers is associated with less compliance. Cont Lens Anterior Eye. 2011;34(5):202–206. doi:10.1016/j.clae.2010.10.004
14. Bui TH, Cavanagh HD, Robertson DM. Patient compliance during contact lens wear: perceptions, awareness, and behavior. Eye Contact Lens. 2010;36(6):334–339. doi:10.1097/ICL.0b013e3181f579f7
15. Lim CH, Carnt NA, Farook M, et al. Risk factors for contact lens-related microbial keratitis in Singapore. Eye (Lond). 2016;30(3):447–455. doi:10.1038/eye.2015.250
16. Chalmers RL, Wagner H, Mitchell GL, et al. Age and other risk factors for corneal infiltrative and inflammatory events in young soft contact lens wearers from the Contact Lens Assessment in Youth (CLAY) study. Invest Ophthalmol Vis Sci. 2011;52(9):6690–6696. doi:10.1167/iovs.10-7018
17. Lam DY, Kinoshita BT, Jansen ME, et al. Contact lens assessment in youth: methods and baseline findings. Optom Vis Sci. 2011;88(6):708–715. doi:10.1097/OPX.0b013e3182142396
18. Leeamornsiri S, Titawattanakul Y. Comparative knowledge and behavior of contact lens care between medical and non-medical students. J Med Assoc Thai. 2015;98(Suppl 3):S16–23.
19. Mohd-Ali B, Azmi N. Wearing pattern and awareness about contact lens wear in secondary school students in Kuala Lumpur. Clin Optom (Auckl). 2021;13:155–160. doi:10.2147/OPTO.S277786
20. Bamahfouz AY, Nafady-Hego H, Jouhargy S, et al. Awareness of contact lens care among college students in Saudi Arabia. Int J Sci Study. 2016;4(1):90–96.
21. Noushad B, Saoji Y, Bhakat P, Thomas J. Contact lens compliance among a group of young, university-based lens users in South India. Australas Med J. 2012;5(3):168–174. doi:10.4066/AMJ.2012.104
22. Gyawali R, Nestha Mohamed F, Bist J, Kandel H, Marasini S, Khadka J. Compliance and hygiene behaviour among soft contact lens wearers in the Maldives. Clin Exp Optom. 2014;97(1):43–47. doi:10.1111/cxo.12069
23. Morgan P, Woods C, Tranoudis I, et al. International contact lens prescribing in 2019. Contact Lens Spectrum. 2020;35:26–32.
24. Mordmuang A, Udomwech L, Karnjana K. Influence of contact lens materials and cleaning procedures on bacterial adhesion and biofilm formation. Clin Ophthalmol. 2021;15:2391–2402. doi:10.2147/OPTH.S310862
25. Taher EE, Méabed EMH, Abdallah I, Abdel Wahed WY. Acanthamoeba keratitis in noncompliant soft contact lenses users: genotyping and risk factors, a study from Cairo, Egypt. J Infect Public Health. 2018;11(3):377–383. doi:10.1016/j.jiph.2017.09.013
26. Dumbleton KA, Woods CA, Jones LW, Fonn D. The relationship between compliance with lens replacement and contact lens-related problems in silicone hydrogel wearers. Cont Lens Anterior Eye. 2011;34(5):216–222. doi:10.1016/j.clae.2011.03.001
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.