")
Back to Journals » Clinical Interventions in Aging » Volume 19
Risk Factors and Short-Term Outcomes of Postoperative Pulmonary Complications in Elderly Patients After Cardiopulmonary Bypass
Authors Liu J, Li X, Xie W, Wang Y, Xu Z, Bai YX, Zhou Q, Wu Q
Received 10 September 2023
Accepted for publication 28 December 2023
Published 6 January 2024 Volume 2024:19 Pages 31—39
DOI https://doi.org/10.2147/CIA.S439601
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Maddalena Illario
Jie Liu,* Xia Li,* Wanli Xie, Yanting Wang, Zhenzhen Xu, Yun-Xiao Bai, Quanjun Zhou, Qingping Wu
Department of Anesthesiology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qingping Wu; Quanjun Zhou, Email [email protected]; [email protected]
Objective: The risk factors of postoperative pulmonary complications (PPCs) have been extensively investigated in non-cardiac surgery and non-elderly adult patients undergoing cardiac surgery. However, data on elderly patients after cardiopulmonary bypass (CPB) is limited. This study aimed to evaluate the risk factors and short-term outcomes for PPCs in elderly patients undergoing CPB procedures.
Patients and Methods: Data from 660 patients who underwent CPB over a six-year period at a tertiary care hospital were collected. The primary outcome encompassed the incidence of PPCs, including re-intubation, postoperative mechanical ventilation exceeding 48 hours, pulmonary infection, pleural effusion requiring thoracic drainage, and acute respiratory distress syndrome. Missing data were managed using multiple imputation. Univariate analysis and the multiple logistic regression method were utilized to ascertain independent risk factors for PPCs.
Results: Among the 660 patients, PPCs were observed in 375 individuals (56.82%). Multiple logistic regression identified serum albumin levels < 40 g/L, type of surgery, CPB duration > 150 minutes, blood transfusion, and intra-aortic balloon pump use before extubation as independent risk factors for PPCs. Patients experiencing PPCs had prolonged mechanical ventilation, extended hospitalization and ICU stays, elevated postoperative mortality, and higher tracheotomy rates compared to those without PPCs.
Conclusion: Elderly patients following CPB displayed a substantially high incidence of PPCs, significantly impacting their prognosis. Additionally, this study identified five prominent risk factors associated with PPCs in this population. These findings enable clinicians to better recognize patients who may benefit from perioperative prevention strategies based on these risk factors.
Keywords: postoperative pulmonary complications, elderly patients, cardiopulmonary bypass, cardiac surgery
Introduction
Postoperative pulmonary complications (PPCs) frequently occur subsequent to cardiac surgery, substantially increasing mortality rates, prolonging stays in the intensive care unit (ICU), extending mechanical ventilation durations, and contributing to elevated healthcare expenditures.1–4 Cardiopulmonary bypass (CPB) assumes a critical role in cases of cardiac arrest by diverting the patient’s blood from the cardiopulmonary system externally to establish a new circulation.5 CPB induces distinctive physiological consequences. Owing to the systemic inflammatory response and ischemia-reperfusion injury, patients become more susceptible to reduced lung function and a heightened incidence of PPCs.
Annually, over 300 million surgical procedures are conducted globally, with this number steadily increasing.6,7 As the global population ages, there is a burgeoning trend of elderly patients undergoing open-heart surgery.8 Although age is no longer a barrier for surgical candidacy, elderly patients remain susceptible due to various comorbidities.9 Besides, despite recognition as a high-risk group,10–12 limited research has delved into the risk factors and clinical outcomes of PPCs in elderly patients undergoing CPB. Identification of significant perioperative factors influencing PPCs in this subgroup will assist clinicians in selecting suitable surgical candidates and improving perioperative care.
Material and Methods
Study Design and Population
We conducted a retrospective analysis involving elderly patients who underwent elective cardiac surgery with CPB at Wuhan Union Hospital between January 2014 and December 2019. The elderly population is defined as individuals aged 65 years and above.13 Patients who died within 48 hours after surgery or underwent a second thoracotomy were excluded. This study adhered to the principles outlined in the Declaration of Helsinki and received approval from the Ethics Committee of Wuhan Union Hospital (No.2021–0621). Due to the retrospective and anonymized nature of the data, patients’ informed consent requirement was waived by the Ethics Committee.
Data Collection
Demographic data and clinical characteristics of patients were obtained through the electronic medical record system. Demographic information encompassed age, gender, body mass index (BMI), drinking history, smoking history, forced expiratory volume in one second/forced vital capacity (FEV1/FVC) ratio, left ventricular ejection fraction (LVEF), and European System for Cardiac Operative Risk Evaluation (EuroScore). Documented comorbidities included hypertension, diabetes, coronary artery disease, myocardial infarction, cerebrovascular disease, pulmonary hypertension, as well as atrial fibrillation. Preoperative medication history covered positive inotropic drug use and antibiotic use. Laboratory tests comprised hemoglobin levels, platelet count, lymphocyte count, neutrophil count, monocyte count, serum albumin, aspartate transaminase, alanine transaminase, serum creatinine, urea nitrogen, along with estimated glomerular filtration rate (eGFR). Intraoperative and postoperative variables included surgical incision, type of surgery, CPB time, aortic cross-clamp time, duration of surgery, duration of anesthesia, blood transfusion, use of intra-aortic balloon pump (IABP) before extubation, together with postoperative complications. Anemia was defined as a hemoglobin level below 130 g/L in the males or below 120 g/L in the females.
Outcome
The primary endpoint of the study was the incidence of PPCs during hospitalization. PPCs specifically refer to re-intubation, postoperative mechanical ventilation lasting more than 48 hours, pulmonary infection, pleural effusion requiring thoracic drainage, and acute respiratory distress syndrome (ARDS). Pulmonary infection was featured by the administration of antibiotic therapy and symptoms such as purulent sputum, alterations in chest radiographs, fever, or an abnormal white blood cell count.14
Data Analysis
Continuous variables with a normal distribution were presented as mean ± standard deviation (SD), while those with a skewed distribution were provided as median and interquartile range (IQR). Categorical variables were presented using frequencies and percentages. Continuous variables were analyzed using the t-test or Mann–Whitney test, and categorical variables were assessed using the chi-square test or Fisher exact test.
Multiple imputation was employed to address missing data, with a deletion rate of under 15%. Univariate analysis and multivariate logistic regression methods were used on the interpolated data to investigate the independent risk factors for PPCs. To facilitate clinical interpretation, continuous variables were converted into binary variables based on clinical expertise or the Youden’s index of the receiver operating characteristic curve. Statistical significance was set at a two-tailed P-value of <0.05. All data analyses were performed using R software version 4.1.1.
Results
Clinical Characteristics
Among the 668 evaluated patients, three died within 48 hours post-surgery, and five were excluded due to secondary thoracotomy. Consequently, our study included data from 660 patients for analysis. Data deletion primarily involved test parameters, with a total of 14 missing indicators (Figure 1). The most conspicuous missing indicator was the FEV1/FVC ratio, with a 14.5% absence rate, while the remaining absent indicators were approximately 10% or less. As shown in Table 1, 375 (56.82%) patients developed PPCs. The median patient age was 68 years, with 57.27% males. The proportion of patients with smoking and drinking history was 29.70% and 23.48%, respectively. Median values for lung function (FEV1/FVC ratio) and heart function (LVEF) were 72.52% and 61%, respectively. The median EuroScore among the entire elderly population was 4 (3, 5). Common comorbidities included coronary artery disease (50.91%), hypertension (45.61%), and diabetes (15.61%). Most patients underwent valve surgery (54.85%), followed by combined coronary artery bypass grafting (CABG) and valve surgery (25.91%).
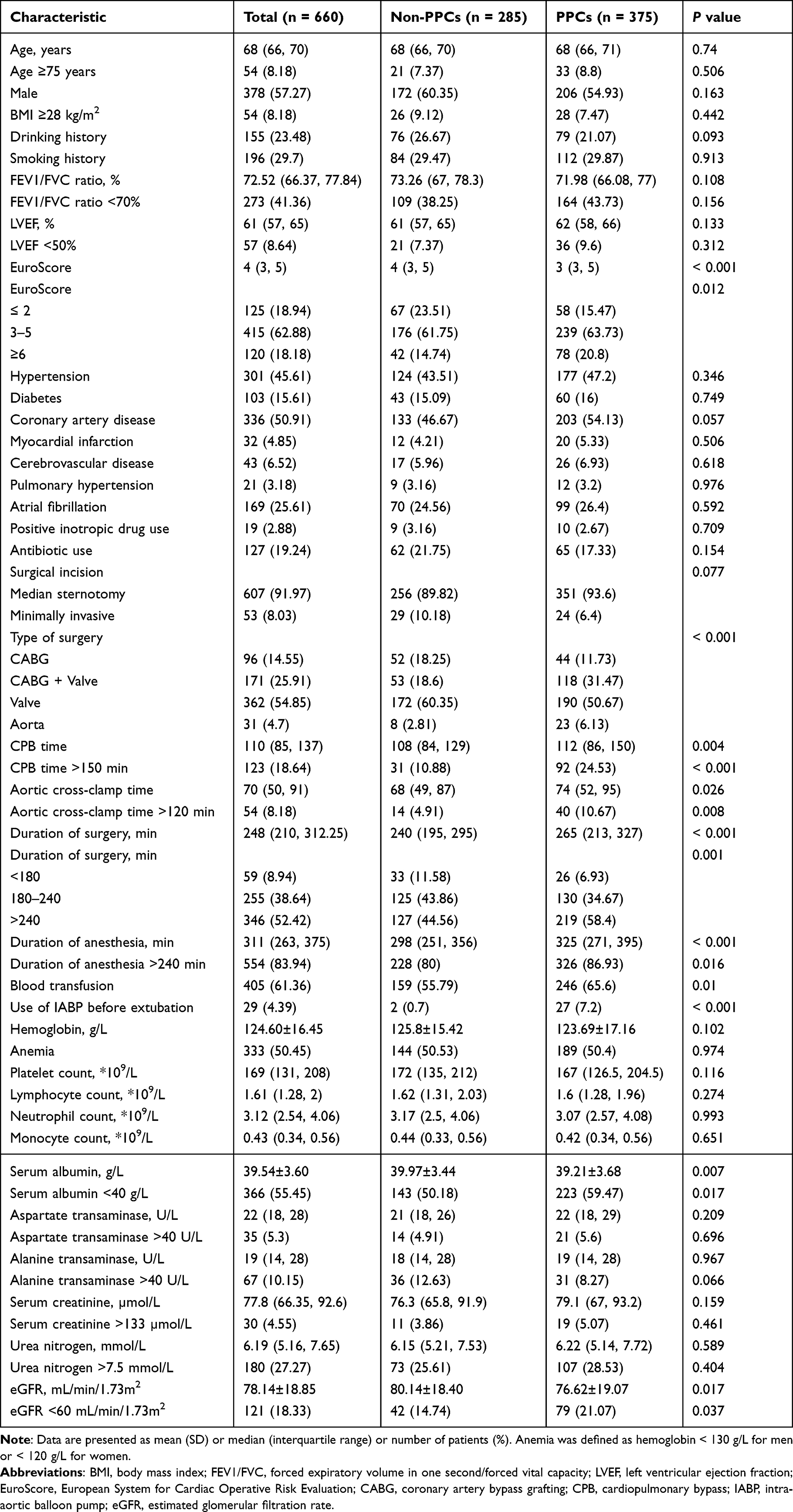 |
Table 1 The Characteristics of Patients |
 |
Figure 1 Specific distribution of missing variables. (A) Proportion of missing variables. The missing rate varied from 0.6% to 14.5%; (B) Quantification of missing values across different combinations of variables. Red squares indicate missing data. Abbreviations: BMI, body mass index; FEV1/FVC, forced expiratory volume in one second/forced vital capacity; eGFR, estimated glomerular filtration rate. |
Variables Associated with PPCs
Notably, trends in the association of continuous variables and their conversion to categorical variables with postoperative pulmonary complications were consistent. Univariate analysis revealed statistically significant differences in serum albumin, eGFR, CPB time, aortic cross-clamp time, duration of surgery, duration of anesthesia, type of surgery, blood transfusion, and use of IABP before extubation (Table 1). We incorporated statistically significant categorical variables into the multivariate regression model to facilitate clinical interpretation. In the multivariate model, it was found that the serum albumin level <40 g/L (adjusted odds ratio [OR], 1.43; 95% confidence interval [CI], 1.03–1.98; P = 0.032), combined CABG and valve surgery (adjusted OR, 2; 95% CI, 1.14–3.51; P = 0.016), aorta-related surgery (adjusted OR, 2.6; 95% CI, 1.01–6.7; P = 0.047), CPB time >150 min (adjusted OR, 1.93; 95% CI, 1.01–3.66; P = 0.046), blood transfusion (adjusted OR, 1.44; 95% CI, 1.03–2.01; P = 0.033), and the use of IABP before extubation (adjusted OR, 7.36; 95% CI, 1.69–32.07; P = 0.008) were independently associated with PPCs (Table 2).
 |
Table 2 Multivariable Logistic Regression for Predictors of PPCs |
Distribution of PPCs
The specific percentages of PPCs are illustrated in Figure 2. Among the various pulmonary complications, pulmonary infection was the most prevalent (28.79%), followed by pleural effusion requiring thoracic drainage (26.36%) and postoperative mechanical ventilation exceeding 48 hours (22.88%). Conversely, ARDS and reintubation were less frequent. Within patients with PPCs, the majority (57.33%) experienced a single pulmonary complication, while 13.87% had three or more PPCs.
 |
Figure 2 Distribution of PPCs in the Study. (A) Proportion of various PPCs: The incidences of individual pulmonary complications, ranked from highest to lowest, were pulmonary infection, pleural effusion requiring thoracic drainage, postoperative mechanical ventilation lasting more than 48 hours, ARDS, and re-intubation. (B) Incidence of multiple PPCs in patients. Most patients experienced a single pulmonary complication, with fewer individuals exhibiting various categories of pulmonary complications. Abbreviations: PPCs, postoperative pulmonary complications; ARDS, acute respiratory distress syndrome. |
Clinical Impact of PPCs
Both hospitalization and postoperative hospitalization durations were significantly longer in patients with PPCs than those without PPCs (33 vs 27, P <0.001; 18 vs 15, P <0.001). Moreover, patients experiencing PPCs had significantly prolonged postoperative ICU stays and mechanical ventilation (5 vs 3, P <0.001; 42 vs 24, P <0.001). Of the 25 recorded deaths, 22 occurred in the PPCs group (22 vs 3, P = 0.001). Furthermore, the tracheotomy rate was significantly higher in patients within the PPCs group (8.53% vs 0.35%, P <0.001). Detailed short-term outcomes for patients with PPCs are presented in Table 3.
 |
Table 3 Comparison of Short-Term Outcomes in Patients with and without PPCs |
Discussion
Our study confirmed that preoperative low serum albumin levels, type of surgery, prolonged CPB duration, blood transfusion, and IABP utilization were independent predictors for elderly patients after CPB. With the increased life expectancy, there is a growing prevalence of cardiac surgery under CPB among older individuals. Considering the elderly population after CPB is at high risk for PPCs, recognizing these risk factors is crucial for optimizing perioperative management.
The incidence of PPCs varies widely, ranging from 2% to 59%, depending on patient characteristics, PPCs definition, and surgical procedures.15 In our study, we observed that 56.82% of elderly patients with CPB experienced PPCs, indicating a substantial incidence and enabling the effective identification of specific risk factors. Multivariate analysis revealed that serum albumin levels less than 40g/L, combined CABG and valve surgery, aorta-related surgery, CPB time exceeding 150 min, blood transfusion, and IABP before extubation were associated with an elevated risk of PPCs post-CPB. Consistent with previous research, our findings indicated a significant increase in mortality, ICU stay, and postoperative hospitalization periods for patients with PPCs. Previous studies have reported some risk factors for PPCs after CPB, mainly including age, prolonged CPB time, and preoperative pulmonary hypertension.10,16 Our study highlighted different risk factors that fully reflected the distinctiveness of the elderly group and emphasized the necessity of conducting this research. We detailed the incidence of PPCs in older patients undergoing CPB and endeavored to elucidate the potential risk factors and short-term outcomes of PPCs.
Serum albumin, produced and secreted by hepatocytes, serves as an indicator of the body’s nutritional status. Furthermore, it functions as a negative acute-phase protein, downregulated during inflammatory states, thereby reflecting both the nutritional status and the inflammatory response and subsequently impacting the patient’s postoperative prognosis.17 With progressive age, serum albumin concentration diminishes at a consistent rate each year.18,19 In cardiac surgery, hypoalbuminemia is frequently observed due to surgical loss and significant hemodilution.20 Within our study cohort, 55.45% of patients exhibited albumin concentrations below 40 g/L. Notably, in a prior investigation focusing on off-pump CABG, a preoperative albumin level <40 g/L was independently associated with acute kidney injury.21 While several studies in cardiac surgery have explored the relationship between postoperative hypoalbuminemia and adverse outcomes, the consideration of preoperative hypoalbuminemia has been limited.22,23 Our emphasis on preoperative albumin levels aimed to identify the optimal opportunity for preventing PPCs. Since low albumin is a modifiable risk factor, optimizing the nutritional status of patients may have a potential in reducing the incidence of PPCs.
CPB-induced local inflammation, systemic inflammatory response syndrome, pulmonary ischemia/reperfusion injury, ventilation arrest, as well as circulating endotoxin collectively increase susceptibility to lung injury.24 As anticipated, our study revealed that patients undergoing more than 150 minutes of CPB time significantly increased the risk of PPCs.
Furthermore, blood transfusion predisposes individuals to pulmonary dysfunction, potentially leading to complications such as transfusion-related acute lung injury and transfusion-associated circulatory overload.25 Studies in cardiac surgery have associated transfusions with adverse outcomes, including mortality, renal failure, pneumonia, and readmission.26–28 In a multicenter study involving adult cardiac surgery patients, each additional unit of blood product transfusion was linked to a 7% increased risk of stroke, renal failure, and major infections (deep sternal wound infection, sepsis, and pneumonia).29 Similarly, our study identified a significant positive correlation between blood transfusion and PPCs. IABP, widely used as a mechanical circulatory assist device, often signals compromised cardiac function in patients. The use of IABP has been subject to some controversy due to its association with higher complication rates.30 A meta-analysis on the prognosis of preoperative IABP implantation in patients undergoing CABG surgery suggested a reduction in the risk of postoperative complications in this specific population.31 However, the population in the study was predominantly those with impaired cardiac function, so early support with extracorporeal circulation might positively impact prognosis. Contrarily, our study concluded that using IABP before extubation significantly escalated the risk of PPCs. This observation might be attributed to the absence of patients with preoperative IABP use in our study, where only a small proportion (8.64%) displayed poor preoperative cardiac function (LVEF <50%). Patients requiring intraoperative or postoperative IABP exhibited more critical cardiac conditions and were more likely to develop PPCs.
Our study had several limitations. Firstly, similar to other retrospective studies, inherent selection bias might exist. Secondly, the retrospective nature limited our ability to collect certain parameters, such as frailty and intraoperative mechanical ventilation, which could potentially serve as risk factors for PPCs. Finally, our study was conducted at a single center, potentially limiting its generalizability. Larger prospective trials are necessary to comprehensively validate these findings.
Conclusions
In conclusion, this study identified five simple elements contributing to the risk of PPCs in elderly patients undergoing CPB. PPCs were prevalent in patients after CPB and associated with prolonged mechanical ventilation, extended hospital and ICU stays, higher mortality, and tracheotomy rates. Recognizing and treating the above risk factors may reduce the incidence of PPCs and ultimately improve the prognosis of elderly patients after CPB.
Acknowledgments
All authors sincerely thank all the participants who contributed to this study and the reviewers for their valuable suggestions.
Funding
This study was supported by the National Key Research and Development Program of China (Grant No. 2018YFC2001903) and the National Natural Science Foundation of China (Grant No. 81873952) and the National Natural Science Foundation of China (Grant No. 81901948).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mathis MR, Duggal NM, Likosky DS, et al. Intraoperative mechanical ventilation and postoperative pulmonary complications after cardiac surgery. Anesthesiology. 2019;131(5):1046–1062. doi:10.1097/ALN.0000000000002909
2. Costa Leme A, Hajjar LA, Volpe MS, et al. Effect of intensive vs moderate alveolar recruitment strategies added to lung-protective ventilation on postoperative pulmonary complications: a randomized clinical trial. JAMA. 2017;317(14):1422–1432. doi:10.1001/jama.2017.2297
3. He S, Chen B, Li W, et al. Ventilator-associated pneumonia after cardiac surgery: a meta-analysis and systematic review. J Thorac Cardiovasc Surg. 2014;148(6):3148–3155.e3141–3145. doi:10.1016/j.jtcvs.2014.07.107
4. Tanner TG, Colvin MO. Pulmonary complications of cardiac surgery. Lung. 2020;198(6):889–896. doi:10.1007/s00408-020-00405-7
5. Sarkar M, Prabhu V. Basics of cardiopulmonary bypass. Indian J Anaesth. 2017;61(9):760–767. doi:10.4103/ija.IJA_379_17
6. Meara JG, Leather AJ, Hagander L, et al. Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Int J Obstet Anesth. 2016;25:75–78. doi:10.1016/j.ijoa.2015.09.006
7. Dobson GP. Trauma of major surgery: a global problem that is not going away. Int J Surg. 2020;81:47–54. doi:10.1016/j.ijsu.2020.07.017
8. Atladottir HO, Modrau IS, Jakobsen CJ, Torp-Pedersen CT, Gissel MS, Nielsen DV. Impact of perioperative course during cardiac surgery on outcomes in patients 80 years and older. J Thorac Cardiovasc Surg. 2021;162(5):1568–1577. doi:10.1016/j.jtcvs.2020.03.005
9. Gill TM, Vander Wyk B, Leo-Summers L, Murphy TE, Becher RD. Population-based estimates of 1-year mortality after major surgery among community-living older US adults. JAMA Surg. 2022;157(12):e225155. doi:10.1001/jamasurg.2022.5155
10. Ji Q, Mei Y, Wang X, Feng J, Cai J, Ding W. Risk factors for pulmonary complications following cardiac surgery with cardiopulmonary bypass. Int J Med Sci. 2013;10(11):1578–1583. doi:10.7150/ijms.6904
11. Häder A, Köse-Vogel N, Schulz L, et al. Respiratory infections in the aging lung: implications for diagnosis, therapy, and prevention. Aging Dis. 2023;14(4):1091–1104. doi:10.14336/AD.2023.0329
12. Schneider JL, Rowe JH, Garcia-de-Alba C, Kim CF, Sharpe AH, Haigis MC. The aging lung: physiology, disease, and immunity. Cell. 2021;184(8):1990–2019. doi:10.1016/j.cell.2021.03.005
13. Chen X, Giles J, Yao Y, et al. The path to healthy ageing in China: a Peking University-Lancet Commission. Lancet. 2022;400(10367):1967–2006. doi:10.1016/S0140-6736(22)01546-X
14. Jammer I, Wickboldt N, Sander M, et al. Standards for definitions and use of outcome measures for clinical effectiveness research in perioperative medicine: European Perioperative Clinical Outcome (EPCO) definitions: a statement from the ESA-ESICM joint taskforce on perioperative outcome measures. Eur J Anaesthesiol. 2015;32(2):88–105. doi:10.1097/EJA.0000000000000118
15. O’Gara B, Talmor D. Perioperative lung protective ventilation. BMJ. 2018;362:k3030 doi:10.1136/bmj.k3030.
16. Naveed A, Azam H, Murtaza HG, Ahmad RA, Baig MAR. Incidence and risk factors of pulmonary complications after cardiopulmonary bypass. Pak J Med Sci. 2017;33(4):993–996. doi:10.12669/pjms.334.12846
17. Bohl DD, Shen MR, Kayupov E, Della Valle CJ. Hypoalbuminemia independently predicts surgical site infection, pneumonia, length of stay, and readmission after total joint arthroplasty. J Arthroplasty. 2016;31(1):15–21. doi:10.1016/j.arth.2015.08.028
18. Cabrerizo S, Cuadras D, Gomez-Busto F, Artaza-Artabe I, Marín-Ciancas F, Malafarina V. Serum albumin and health in older people: review and meta analysis. Maturitas. 2015;81(1):17–27. doi:10.1016/j.maturitas.2015.02.009
19. Weaving G, Batstone GF, Jones RG. Age and sex variation in serum albumin concentration: an observational study. Ann Clin Biochem. 2016;53(Pt 1):106–111. doi:10.1177/0004563215593561
20. Xiang F, Huang F, Huang J, et al. Expert consensus on the use of human serum albumin in adult cardiac surgery. Chin Med J. 2023;136(10):1135–1143. doi:10.1097/CM9.0000000000002709
21. Lee EH, Baek SH, Chin JH, et al. Preoperative hypoalbuminemia is a major risk factor for acute kidney injury following off-pump coronary artery bypass surgery. Intensive Care Med. 2012;38(9):1478–1486. doi:10.1007/s00134-012-2599-8
22. Berbel-Franco D, Lopez-Delgado JC, Putzu A, et al. The influence of postoperative albumin levels on the outcome of cardiac surgery. J Cardiothorac Surg. 2020;15(1):78. doi:10.1186/s13019-020-01133-y
23. van Beek DEC, van der Horst ICC, de Geus AF, Mariani MA, Scheeren TWL. Albumin, a marker for post-operative myocardial damage in cardiac surgery. J Crit Care. 2018;47:55–60. doi:10.1016/j.jcrc.2018.06.009
24. Nteliopoulos G, Nikolakopoulou Z, Chow BHN, Corless R, Nguyen B, Dimarakis I. Lung injury following cardiopulmonary bypass: a clinical update. Expert Rev Cardiovasc Ther. 2022;20(11):871–880. doi:10.1080/14779072.2022.2149492
25. Vlaar AP, Juffermans NP. Transfusion-related acute lung injury: a clinical review. Lancet. 2013;382(9896):984–994. doi:10.1016/S0140-6736(12)62197-7
26. Unal D, Senayli Y, Polat R, et al. Peri-operative blood transfusion in elective major surgery: incidence, indications and outcome - an observational multicentre study. Blood Transfus. 2020;18(4):261–279. doi:10.2450/2020.0011-20
27. LaPar DJ, Hawkins RB, McMurry TL, et al. Preoperative anemia versus blood transfusion: which is the culprit for worse outcomes in cardiac surgery? J Thorac Cardiovasc Surg. 2018;156(1):66–74.e62. doi:10.1016/j.jtcvs.2018.03.109
28. Mazzeffi MA, Holmes SD, Taylor B, et al. Red blood cell transfusion and postoperative infection in patients having coronary artery bypass grafting surgery: an analysis of the society of thoracic surgeons adult cardiac surgery database. Anesth Analg. 2022;135(3):558–566. doi:10.1213/ANE.0000000000005920
29. Massimiano PS, Rongione AJ. Number and type of blood products are negatively associated with outcomes after cardiac surgery. Ann Thorac Surg. 2022;113(3):748–756. doi:10.1016/j.athoracsur.2021.06.061
30. Freund A, Desch S, Thiele H. Intra-aortic balloon counterpulsation - Does it work? Prog Cardiovasc Dis. 2020;63(5):623–629. doi:10.1016/j.pcad.2020.07.001
31. Zangrillo A, Pappalardo F, Dossi R, et al. Preoperative intra-aortic balloon pump to reduce mortality in coronary artery bypass graft: a meta-analysis of randomized controlled trials. Crit Care. 2015;19(1):10. doi:10.1186/s13054-014-0728-1
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.