")
Back to Journals » Orthopedic Research and Reviews » Volume 15
Reverse Total Shoulder Arthroplasty in Alkaptonuric Shoulder: Case Presentation, Review of Literature, and Technical Considerations
Authors Dawod MS , Alswerki MN , Darabah AJ , Satari AO, Alrwashdeh AO , Alaqarbeh ZN, Alisi MS
Received 21 December 2022
Accepted for publication 6 April 2023
Published 15 April 2023 Volume 2023:15 Pages 69—77
DOI https://doi.org/10.2147/ORR.S402214
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Moh’d S Dawod,1 Mohammad N Alswerki,2 Asem J Darabah,1 Anas O Satari,1 Asaad O Alrwashdeh,3 Zaid N Alaqarbeh,3 Mohammed S Alisi2,4,5
1Mutah University, Faculty of Medicine, Al-karak, Jordan; 2Jordan University Hospital, Amman, Jordan; 3Al-Karak Hospital, Al-karak, Jordan; 4Faculty of Medicine, Islamic University of Gaza, Gaza, Palestine; 5Ministry of Health, Gaza, Palestine
Correspondence: Mohammad N Alswerki, Jordan University Hospital, Queen Rania Al-Abdullah Street – Aljubeiha / P.O. Box 13046, Amman, 11942, Jordan, Email [email protected]
Importance: Alkaptonuric shoulder arthropathy is a challenging clinical entity in arthroplasty. In this report, we describe an atypical presentation, technical considerations, a literature review, and some recommendations of significant benefits to shoulder surgeons.
Objective: The author’s objective in this report is to illustrate the deleterious metabolic effects of ochronosis on cartilage and the development of early arthritis.
Design: This is a case report study, done in May 2021.
Setting: Middle East, Jordan.
Introduction: Alkaptonuria is a metabolic disease of amino acid metabolism that can affect multiple organ systems, including the musculoskeletal system. The musculoskeletal system manifestations usually involve the spine, knee, and, uncommonly, the shoulder. Tissue ochronosis caused by alkaptonuria can cause significant damage to the joint and surrounding soft tissue envelope. In this case, we presented a patient who has end-stage glenohumeral arthritis and rotator cuff arthropathy secondary to ochronosis.
Case Presentation: In this case report, we present a 42-year-old male patient who presented to the clinic with severe right shoulder pain and limitations of the range of motion, especially with abduction. The patient underwent radiographic assessment, which showed a rotator cuff arthropathy combined with advanced degenerative changes of the right glenohumeral joint. The patient underwent reverse total shoulder arthroplasty. After the surgery and on follow-up later on for a period of one year and after a period of physiotherapy and rehabilitation, the patient showed remarkable improvement in the pain and range of motion.
Conclusion: Alkaptonuria can have a detrimental effect on the articular cartilage and the surrounding soft tissue envelope, which might manifest clinically as early degenerative arthritis changes in a young adult patient. Shoulder involvement is extremely rare and can manifest with substantial injury to the glenohumeral joint; whenever such extensive damage is present, shoulder arthroplasty is the best treatment.
Keywords: alkaptonuria, shoulder arthritis, glenohumeral arthritis, shoulder arthroplasty, reverse total shoulder arthroplasty
Introduction
Alkaptonuria is a metabolic disease with an autosomal recessive mode of inheritance.1 The disease is rare, with a prevalence of 1:250,000–1,000,000 worldwide.2 It is attributed to homogentisic acid oxidase deficiency and leads to failures in processing the amino acids phenylalanine and tyrosine.3 Eventually, this leads to the buildup of homogentisic acid and its subsequent polymerization with body collagen fibers. Most cases typically present with homogentisic aciduria, arthritis, and ochronosis.4 Homogentisic aciduria is caused by the partial renal clearance of homogentisic acid, which results in a dark urine color following its oxidation.5,6 Ochronosis is an inevitable complication of alkaptonuria.7 It is defined as the deposition of homogentisic acid in connective tissue, such as articular tissue.8 Mainly, this deposition affects weight-bearing joints (the spine followed by the knee).9,10 The shoulder joint is considered a rare joint to be affected by ochronosis.11 Currently, the treatment plan for alkaptonuria is symptomatic, and the definite treatment for arthropathy is joint replacement.12,13
Clinical features of alkaptonuria can start in early childhood with the blackish discoloration of urine; other systemic involvement then ensues. Around the age of forty, tissue ochronosis, kidney and prostate stones, and tendon ruptures develop.14 These changes are caused by a single gene defect and cause malfunctioning or inactive homogentisate 1.2-dioxygenase (HGD), which is one of the main enzymes in tyrosine metabolism and is needed to break down homogentisic acid (HGA).15 When HGA cannot be converted into maleylacetoacetic acid and thus cannot be excreted, it causes elevated levels and the accumulation of HGA in the body.16
Management of degenerative arthritis secondary to alkaptonuria is pretty much the same as management of arthritis secondary to other etiologies.17 Conservative management in the form of analgesics and physical therapy is usually the first management modality. However, with the unrelenting metabolic process of accumulation of homogentisic acid, rapid arthritic changes ensue.18,19
In the medical literature, there were many cases of alkaptonuric arthropathy that affected more than one joint (eg, hip, knee), but there were not many about the shoulder and how the case was treated. The use of shoulder arthroscopy was described in the literature for the diagnosis and treatment of ochronotic tissue debridement.20–22 However, total joint replacement is currently the gold standard and the definitive treatment option for ochronosis-induced advanced arthritis.23 In cases with shoulder involvement and secondary damage to the stabilizing rotator cuff muscles, reverse total shoulder arthroplasty is a valid and reliable option, as shown in the case report by Butterfield et al, with excellent results seen in follow-up at four months.24
Case Presentation
History and Physical Examination
A 43-year-old male patient, a right-handed manual worker, presented to our arthroplasty clinic at Al-Karak hospital, Jordan, with a one-year history of right shoulder pain. The patient has no previous shoulder injuries. NSAIDs only partially alleviated the pain, which was aggravated by activity. His family history for alkaptonuria was positive because his sister had the disease. Physical examination revealed a limited range of motion in the right shoulder with abduction weakness. The patient had signs of alkaptonuria, such as black urine and black pigmentation in the mouth, eyes, and ear pinnae. His urine had been black since he was five years old, he reported.
However, unfortunately, the patient neither tested for nor was informed that he had alkaptonuria previously despite having some suggestive symptoms. Therefore, the patient was diagnosed intraoperatively with the striking features of extensive ochronosis. Laboratory findings were unremarkable except for a mild elevation of the inflammatory markers (ESR and CRP). A summary of the lab values is found in Table 1.
 |
Table 1 The Patient Laboratory Profile Was as Following |
Imaging Studies
As of preoperative assessment, patient underwent radiographic assessment of the affected shoulder. The preoperative image shown in Figure 1.
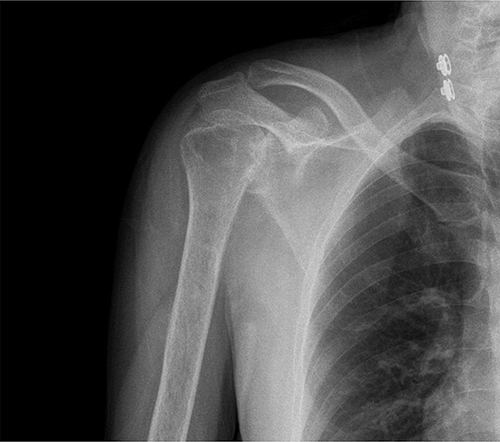 |
Figure 1 Preoperative right shoulder X-ray of the patient showing severe arthritic changes, superior migration, and subchondral bone cyst, finding suggestive of advanced osteoarthritic changes and rotator cuff arthropathy of the right glenohumeral joint. |
Since there were signs of rotator cuff arthropathy, the patient had a right shoulder MRI without contrast (Figure 2), which showed severe osteoarthritic changes of the right glenohumeral joint, including narrowing of the joint space, osteophytes, abnormal signal intensity of visualized bone consistent with bone marrow edema, and multiple subchondral cysts. Also, thickening with altered signal intensity of the supraspinatus tendon is compatible with tendinopathy, a feature of degenerative secondary rotator cuff arthropathy.
 |
Figure 2 Preoperative right shoulder MRI with prominent osteophytes of the glenoid, increased signal at the supraspinatus tendon, and prominent bone marrow edema, and subchondral cyst. |
Management
Based on the MRI results, which pointed to rotator cuff arthropathy, the patient was selected to undergo a reverse total shoulder arthroplasty.
In addition to the standard surgical procedure for reverse arthroplasty, a remarkable intraoperative finding of soft tissue ochronosis is observed in Figure 3. A diffuse black discoloration of the proximal humerus, glenoid labrum, and rotator cuff degenerative tendons. There were no intraoperative or postoperative complications during or following the surgery.
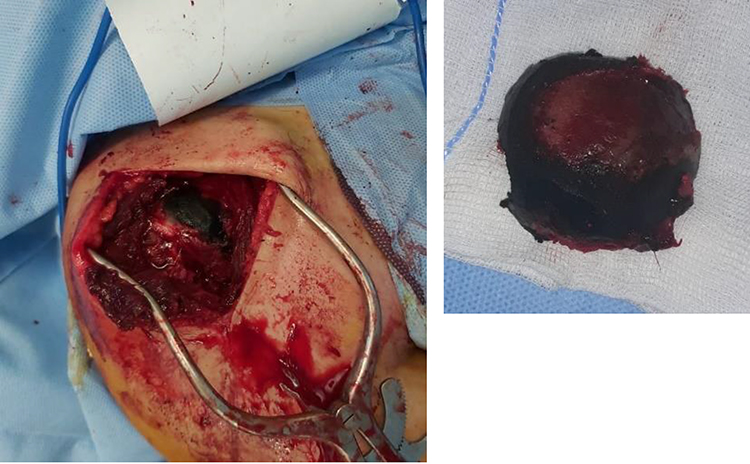 |
Figure 3 Intraoperative findings of severe black discoloration of the soft tissue (ochronosis), a striking feature of Alkaptonuria. (A) Soft tissue ochronosis. (B) Humerus head cut with severe blackish discoloration. |
A postoperative X-ray showed well-positioned and aligned components in Figure 4. The patient’s postoperative course was unremarkable with clean dressing and gradual return of shoulder range of motion. The patient was started on physiotherapy on the first postoperative day. The physiotherapy was gentle range-of-motion exercises; the abduction range-of-motion exercises have improved from the preoperative status. Patient was put in arm sling for a period of 2 weeks postoperatively.
 |
Figure 4 Postoperative radiography of the reverse procedure, with the humerus stem, head, and components well fixed and in a good position and orientation. |
Technical Considerations
Aside from the standard deltopectoral approach steps used in shoulder surgery, there were a few technical difficulties encountered intraoperatively. The intraoperative course was challenging in this case and different from other surgeries done for rotator cuff arthropathy.
Firstly, the soft tissue discoloration (ochronosis) that was affecting the proximal humerus, the labrum, the rotator cuff tendons, and surrounding tissues was obscuring the field and making proper identification of the anatomical structures very difficult. Secondly, the inflammatory process induced by alkaptonuria and evidenced by adhesions added to the technical difficulties with poor demarcation of the soft tissue planes. Thirdly, an increased blood loss was noticed compared to the standard reverse procedure, which is clearly due to poor delineation between anatomical structures, the presence of inflammatory adhesions, and increased vascularity given the underlying inflammatory process.
The author’s recommendations when dealing with such cases include the following tips.
- The use of an extensible approach is very advisable for better identification and delineation of the anatomical planes and structures.
- A good intraoperative hemostasis is crucial in these cases to prevent excessive intraoperative bleeding from the underlying inflammation and adhesions.
- In anticipation of excessive bleeding, preparation of blood products may be necessary as well.
- Gentle soft tissue handling is mandatory to avoid injury to previously inflamed and irritated tissues and minimize the risk of infection and adhesions.
- After thorough irrigation at the end of surgery, meticulous closure is crucial to prevent postoperative wound complications.
Rehabilitation Protocol and Follow-Up
Rehabilitation was started as soon as the first week after the surgery. Rehabilitation is done by trained physiotherapists in our hospital. Our postoperative rehabilitation protocol was conducted over two phases. The first phase, which started postoperatively and lasted for 6 weeks, was to have passive and patient-assisted range of motion to encourage shoulder range of motion and avoid stiffness. During phase one, the patient was kept in an arm sling. The second phase was from 6 weeks to a 5–6-month period, which focused on periscapular and deltoid strengthening. At this phase, the arm sling was discontinued.
The first follow-up visit was two weeks after the surgery. During this visit, the wound was healed and cleaned. Periodically, the patient was followed up for one year. After 2 months of surgery, the patient returned to his manual working activity of carpentry, and has painless stable range of motion. At the final follow-up visit, the Oxford shoulder score (OSS),25 which is a 12-item Patient-Reported Outcome (PRO) measurement specifically designed and developed for assessing outcomes of shoulder surgery, was improved from 47 preoperatively to 12 postoperatively, an indication of remarkable functional improvement.
Discussion
Musculoskeletal involvement in alkaptonuria can be detrimental and lead to early arthritic changes. These changes can cause permanent damage to the articular surface and surrounding soft tissue envelope and necessitate joint replacement.
A review of the literature on alkaptonuria over the last fifty years using the PubMed search engine reveals five hundred and sixteen case reports, only eight of which involve the shoulder joint. Castagna et al, Gupta et al, and Schouten et al reported cases of ochronotic arthropathy with many joints involved, including the shoulder, which have been managed arthroscopically.11,20,21 Afonso et al and Dorleijn et al reported cases of shoulder ochronotic arthropathy preceded by knee involvement; in the latter, the diagnosis of alkaptonuria was established via a biopsy taken by knee arthroscopy.26,27 Merolla et al reported a case of ochronotic arthropathy of the shoulder associated with autoimmune diseases in his first-degree relatives, but no cases of alkaptonuria were identified in the family.28 Also, Nas et al reported a case of shoulder arthropathy with spine involvement.29 In the latest case report, the shoulder was the first and only joint affected by ochronosis associated with a rotator cuff injury.24 Similarly, in this case, only the right shoulder joint was severely affected by a rotator cuff tear, with secondary degenerative arthritis and rotator cuff arthropathy, and no other joints were involved.
The current treatment options for alkaptonuria are limited, and there is no treatment that can prevent the occurrence of complications such as ochronosis. Vitamin C has been proposed as its anti-oxidant properties might be able to stop the oxidation of homogentisic acid (HGA) into harmful metabolites, but later on, found to not affect levels of HGA in urine.30 In addition, low tyrosine and phenylalanine diet has also been proposed as these two amino acids are degraded into HGA but the effects of going on the diet were not studied on the long term.31 Additionally, nitisinone was proposed since it is a potent inhibitor of the enzyme 4-hydroxyphenylpyruvate dioxygenase which produces HGA, but it can increase serum tyrosine levels which may lead to corneal irritation.32
In addition to the treatment modalities aforementioned. The standard conservative management for degenerative arthritis can be utilized. This included the use of analgesics and physical therapy. However, due to renal involvement of alkaptonuria, physicians are advised to avoid and limit the use of nonsteroidal anti-inflammatory drugs (NSAIDs).
However, the treatment of alkaptonuric arthropathy can be clinically challenging in many aspects. Firstly, given the underlying ongoing metabolic derangement and accumulation of toxic metabolites in the cartilage and joints, this will lead to accelerated joint wear compared to the wear caused by the degenerative senile arthritis. Secondly, response to usual conservative treatment modalities can be expected to be suboptimal in these patients due to the extensive articular damage and inflammatory arthritis. Thirdly, due to the fact that these patients usually present in early or mid-adulthood, they usually have higher expectations compared to their low-demand geriatric counterparts undergoing joint replacement. Fourthly, surgery in these patients can be complicated by tissue ochronosis, poor anatomical demarcations, and increased blood loss; this hostile biology at the surgery site may infer unique surgical challenges to the surgeon. Finally, other system involvement by alkaptonuria, like the cardiovascular and renal systems, can increase the overall patient risk of perioperative complications.
There are some surgical considerations when performing arthroplasty on an alkaptonuric joint. Given the poor bone quality of the involved joints, there were some concerns regarding the longevity of the implants used in these patients. However, in a case series of 11 arthroplasties (both upper and lower limbs) for end-stage ochronotic arthritis reported by Spencer et al, prosthetic joint survival was comparable to that found in patients with degenerative osteoarthritis.33 In another series done by Al-Ajlouni et al involving four hips and four knees followed for 2–10 years, none of these patients at follow-up had prosthesis-related complications.34 Another surgical concern was increased perioperative complications (including infection, periprosthetic fracture, and wear) compared to non-alkaptonuric patients. However, in a follow-up study done by Pachore et al on 12 hip arthroplasties on patients who were followed for up to 24 years, all involved patients had excellent outcomes, and there were no increased complications noticed.35 The same findings of no increased complications were reported by Al-Ajlouni et al as well.34
It is not uncommon for alkaptonuria to be diagnosed intraoperatively during arthroplasty surgery. As in our case, the diagnosis is usually made after visualization of the extensive blackish discoloration of the cartilage and surrounding tissues. Shaikh et al reported the intraoperative diagnosis of a 70-year-old female patient during hip arthroplasty.36 Elafarm et al reported a similar intraoperative diagnosis during knee arthroplasty for a 50-year-old man.37 In another example, Gencer et al reported an intraoperative diagnosis of alkaptonuria during knee arthroscopy; the patient later underwent a successful knee arthroplasty due to the severe arthritis caused by ochronosis of the cartilage, menisci, and bone surfaces.38
Although alkaptonuria is a rare disease, it is found to be more prevalent in Jordan, which is the highest country in the Middle East regarding alkaptonuria prevalence.3 The exact prevalence of alkaptonuria is still unknown, but it is estimated to be high due to high rates of consanguinity, which reach up to 63%.39 One study reported that there were nine cases of alkaptonuria in a single family; a separate study reported that there were forty cases in a single south Jordanian village.40,41 More studies are still needed to identify emergent cases and determine the exact prevalence and distribution of the disease.
Conclusion
Alkaptonuria is a metabolic disease affecting amino acid metabolism. Axial skeleton involvement is a common theme; shoulder involvement, however, is unusual. Alkaptonuria can result in end-stage arthritis, which necessitates joint replacement, as in our case. Management of alkaptonuric arthropathy can be challenging, and there are important surgical considerations to be made. The authors clinical message from this report is that alkaptonuric shoulder arthropathy is a manageable disease, and total joint arthroplasty offers good pain relief, an improved functional range of motion, and an improved patient reported outcome. Given the variability and severity of the symptoms of alkaptonuria, it is not uncommon to diagnose patients lately with end-stage arthropathy intraoperatively. The orthopedic surgeon needs to be vigilant in such cases and inquire about family history and the possibility of metabolic disease when encountering a young patient with advanced shoulder arthrosis.
Availability of Supporting Data
The data used to support the findings of this report are included within the article.
Ethical Approval and Consent to Participate
The patient included in this study voluntarily agreed to the inclusion of materials in this work by signing a written consent form. The informed consent explained the premise of this report, the state of his anonymity within the report, and the confidentiality of his personal information. An appropriate institutional review board was obtained for this report by the Mutah University Research Office.
Consent for Publication
Written informed consent was obtained from the patient for publication.
Funding
This report did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no conflict of interest.
References
1. Gallagher JA, Ranganath LR, Zatkova A. Alkaptonuria ☆. Ref Modul Life Sci. 2017. doi:10.1016/B978-0-12-809633-8.06029-5
2. Khalil R, Ali D, Mwafi N, et al. Variant analysis of alkaptonuria families with significant founder effect in Jordan. Biomed Res Int. 2021;2021:1–8. doi:10.1155/2021/1515641
3. Mistry JB, Bukhari M, Taylor AM. Alkaptonuria. Rare Dis. 2013;1(1):e27475. doi:10.4161/RDIS.27475
4. Syam G, Nair DS, Yadav S, Varghese J, Jamsheed T. Ochronotic surprise during total knee replacement! A case report. J Orthop Case Reports. 2021;11(10):49–52. doi:10.13107/jocr.2021.v11.i10.2464
5. Ferreira AM, Santos FL, Costa AM, et al. Knee osteoarthrosis secondary to ochronosis - clinical case. Rev Bras Ortop. 2014;49(6):675–680. doi:10.1016/j.rboe.2013.11.001
6. Kural C, Cetinus EM, Kural A, Ugras AA, Kaya I. Knee ochronotic arthropathy and arthroscopic findings. Acta Orthop Traumatol Turc. 2009;43(1):67–71. doi:10.3944/AOTT.2009.067
7. Lurie DP, Musil G. Knee arthropathy in ochronosis: diagnosis by arthroscopy with ultrastructural features. J Rheumatol. 1984;11(1):101–103.
8. Ramsperger R, Lubinus P, Lubinus HH. Alkaptonuria and ochronotic arthropathy. Arthroscopic and intraoperative findings in implantation of a knee joint surface replacing prosthesis. Chirurg. 1994;65(11):1061–1065.
9. Aquaron R. Alkaptonuria: a very rare metabolic disorder. Indian J Biochem Biophys. 2013;50(5):339–344.
10. Drakoulakis E, Varvitsiotis D, Psarea G, Feroussis J. Ochronotic arthropathy: diagnosis and management: a critical review. Am J Orthop. 2012;41(2):80–83.
11. Gupta PK, Acharya A, Sabat D, Mourya A. Arthroscopic diagnosis and treatment of shoulder ochronotic arthropathy – a case report. J Clin Orthop Trauma. 2017;8(1):S80. doi:10.1016/J.JCOT.2016.11.009
12. Kerimoglu S, Onder C, Aynaci O, Malkoc CH. Hip arthroplasty for ochronosis. Saudi Med J. 2005;26(11):1812–1814.
13. Cetinus E, Cever I, Kural C, Erturk H, Akyildiz M. Ochronotic arthritis: case reports and review of the literature. Rheumatol Int. 2005;25(6):465–468. doi:10.1007/s00296-004-0538-x
14. Jiang L, Cao L, Fang J, Yu X, Dai X, Miao X. Ochronotic arthritis and ochronotic Achilles tendon rupture in alkaptonuria: a 6 years follow-up case report in China. Medicine. 2019;98(34):e16837. doi:10.1097/MD.0000000000016837
15. Sharabi AF, Goudar RB. Alkaptonuria; 2022. Available from. https://www.ncbi.nlm.nih.gov/books/NBK560571/.
16. Heoedus ZL, Nayak U. Homogentisic acid and structurally related compounds as intermediates in plasma soluble melanin formation and in tissue toxicities. Arch Int Physiol Biochim Biophys. 1994;102(3):175–181. doi:10.3109/13813459409007534
17. Raaijmaakers M, Steenbrugge F, Dierickx C. Ochronosis, arthroscopy of a black knee: a case report and review of the literature. Knee Surgery, Sport Traumatol Arthrosc. 2008;16(2):182–184. doi:10.1007/s00167-007-0413-x
18. Martin JP, Batkoff B. Homogentisic acid autoxidation and oxygen radical generation: implications for the etiology of alkaptonuric arthritis. Free Radic Biol Med. 1987;3(4):241–250. doi:10.1016/S0891-5849(87)80031-X
19. Braconi D, Millucci L, Bernardini G, Santucci A. Oxidative stress and mechanisms of ochronosis in alkaptonuria. Free Radic Biol Med. 2015;88:70–80. doi:10.1016/j.freeradbiomed.2015.02.021
20. Castagna A, Giombini A, Vinanti G, Massazza G, Pigozzi F. Arthroscopic treatment of shoulder ochronotic arthropathy: a case report and review of literature. Knee Surg Sports Traumatol Arthrosc. 2006;14(2):176–181. doi:10.1007/S00167-005-0657-2
21. Schouten TTJ, Oldenburg RA, van Kampen PM, Huijsmans PE. Arthroscopic soft-tissue interposition arthroplasty of the glenohumeral joint for ochronotic arthropathy: a case report. J Orthop Sci. 2020;25(4):734–738. doi:10.1016/j.jos.2017.12.008
22. Thacker M, Garude S, Puri A. Ochronotic arthropathy: arthroscopic findings in the shoulder and the knee. Arthroscopy. 2003;19(8):e99–e102. doi:10.1016/s0749-8063(03)00744-8
23. Patel VG. Total knee arthroplasty in ochronosis. Arthroplast Today. 2015;1(3):77. doi:10.1016/J.ARTD.2015.03.003
24. Butterfield BP, Garver TH. Reverse total shoulder arthroplasty for treatment of ochronotic arthropathy. J Surg Case Reports. 2022;2022(4):Apr. doi:10.1093/JSCR/RJAC190
25. The oxford shoulder score. Available from: https://innovation.ox.ac.uk/outcome-measures/oxford-shoulder-score-oss/.
26. Afonso CT, Pinto S, Freitas M, Pedrosa D, Ruano A. Total shoulder reverse arthroplasty in alkaptonuria: an effective option to treat a complication of a rare disease. J Orthop Case Reports. 2022;12(1):31. doi:10.13107/JOCR.2022.V12.I01.2604
27. Dorleijn D, van Noort A, Janus G. Short-term results of total shoulder arthroplasty for ochronotic arthritis. J Surg Case Reports. 2019;2019(7). doi:10.1093/JSCR/RJZ219
28. Merolla G, Dave AC, Pegreffi F, Belletti L, Porcellini G. Shoulder arthroplasty in alkaptonuric arthropathy: a clinical case report and literature review. Musculoskelet Surg. 2012;96:93–99. doi:10.1007/s12306-012-0184-5
29. Nas K, Gür A, Akdeniz S, Çevik R, Harman M, Saraç AJ. Ochronosis: a case of severe ochronotic arthropathy. Clin Rheumatol. 2002;21(2):170–172. doi:10.1007/S10067-002-8277-4
30. Albatayneh EM, Al-Sbou MS, Mahgoub SS, Mwafi NR, Alnawaiseh NA. Serum oxidative-antioxidative status in patients with alkaptonuria. J Clin Med Res. 2019;11(5):337. doi:10.14740/JOCMR3801
31. Davison AS, Norman BP, Smith EA, et al. Serum amino acid profiling in patients with alkaptonuria before and after treatment with nitisinone. JIMD Rep. 2018;41:109. doi:10.1007/8904_2018_109
32. Introne WJ, Perry MB, Troendle J, et al. A 3-year randomized therapeutic trial of nitisinone in alkaptonuria. Mol Genet Metab. 2011;103(4):307. doi:10.1016/J.YMGME.2011.04.016
33. Spencer J, Gibbons CM, Sharp R, et al. Acta Orthopaedica Scandinavica Arthroplasty for ochronotic arthritisNo failure of 11 replacements in 3 patients followed 6-12 years Arthroplasty for ochronotic arthritis No failure of 11 replacements in 3 patients followed 6-12 years. Acta Orthop Scand. 2004;75(3):355–358. doi:10.1080/00016470410001321
34. Al-Ajlouni JM, Alisi MS, Yasin MS, et al. Long-term outcomes of the knee and hip arthroplasties in patients with alkaptonuria. Arthroplast Today. 2020;6(4):689–693. doi:10.1016/J.ARTD.2020.07.037
35. Pachore JA, Shah VI, Upadhyay S, Shah K, Sheth A, Kshatriya A. Primary Hip arthroplasty for the treatment of alkaptonuric Hip arthritis: 3- to 24-year follow-ups. Arthroplasty. 2019;1(1):1–9. doi:10.1186/S42836-019-0010-8/FIGURES/7
36. Shaikh A, Desai M, Kantanavar R, Shah S. Intraoperative diagnosis of a rare case of arthropathy – a case report and review of literature. J Orthop Case Reports. 2020;10(8):58. doi:10.13107/JOCR.2020.V10.I08.1860
37. Elafram R, Ben Ammou A, Ben Romdhane M, Sghaier M. Alkaptunuria; a case report. Int J Surg Case Rep. 2022;100:107682. doi:10.1016/J.IJSCR.2022.107682
38. Batuhan Gencer CÇ. Diagnosing an ochronotic arthropathy during knee arthroscopy: management of a Rare Case. Available from: http://www.jmhsci.org/wp-content/uploads/2021/07/BJMHS450324.pdf.
39. Tadmouri GO, Nair P, Obeid T, Al Ali MT, Al Khaja N, Hamamy HA. Consanguinity and reproductive health among Arabs. Reprod Health. 2009;6(1):1–9. doi:10.1186/1742-4755-6-17/TABLES/1
40. Al-Sbou M, Mwafi N, Lubad MA. Identification of forty cases with alkaptonuria in one village in Jordan. Rheumatol Int. 2012;32(12):3737–3740. doi:10.1007/S00296-011-2219-X
41. Al-Sbou M, Mwafi N. Nine cases of Alkaptonuria in one family in southern Jordan. Rheumatol Int. 2012;32(3):621–625. doi:10.1007/S00296-010-1701-1
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.