")
Back to Journals » Patient Preference and Adherence » Volume 15
Rehabilitation Goals and Effects of Goal Achievement on Outcome Following an Adapted Physical Activity-Based Rehabilitation Intervention
Authors Preede L , Soberg HL, Dalen H, Nyquist A, Jahnsen R , Saebu M, Bautz-Holter E, Røe C
Received 20 March 2021
Accepted for publication 23 June 2021
Published 9 July 2021 Volume 2021:15 Pages 1545—1555
DOI https://doi.org/10.2147/PPA.S311966
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Line Preede,1– 3 Helene L Soberg,1,4 Håkon Dalen,2 Astrid Nyquist,2 Reidun Jahnsen,2,3 Martin Saebu,2 Erik Bautz-Holter,1,3 Cecilie Røe1,3
1Department of Physical Medicine and Rehabilitation, Oslo University Hospital, Oslo, Norway; 2Beitostølen Healthsports Centre, Beitostølen, Norway; 3Faculty of Medicine, University of Oslo, Oslo, Norway; 4Faculty of Health Sciences, Oslo Metropolitan University, Oslo, Norway
Correspondence: Line Preede Haneholmveien 216, Sandefjord, 3231, Norway
Tel +47 930 56 136
Email [email protected]
Purpose: To explore the goal-setting process carried out at a rehabilitation facility providing adapted physical activity, by 1) identifying goals set by individuals with chronic disabilities, 2) comparing these goals to the negotiated goals set in collaboration with the rehabilitation team and 3) assessing goal achievement and its association with self-reported functioning after 12 months.
Methods: A prospective observational study where adults (18– 67 years) admitted to Beitostølen Healthsports Centre (n=151) reported mental and physical functioning measured by the Medical Outcomes Study 12-item Short-Form Health Survey (SF-12) administered at baseline (eight weeks before rehabilitation), admission, discharge and follow-up 12 months after rehabilitation. The participants provided their individual goals for rehabilitation in the admission questionnaire. Individual goals were compared to negotiated goals set by the participants and the rehabilitation team together as part of the goal-setting process at the facility. The goals were linked to The International Classification of Functioning, Disability and Health (ICF) for comparison. Goal achievement was assessed on a 10-point numeric rating scale (NRS) in the discharge questionnaire. The association between SF-12 physical and mental functioning at long-term follow-up and goal achievement was explored.
Results: The 293 individual goals and the 407 negotiated goals were most frequently linked to the ICF-component Body Functions. When comparing negotiated to individual goals, negotiated goals were more frequently linked to activities and participation. Goals to wide to be linked to the ICF were less frequent. For 76% of the participants, content of individual goals was captured in negotiated goals. Goal achievement with NRS scores ≥ 9 points was reported by 66% of the included participants. Goal achievement was a significant predictor for long-term mental functioning (p=0.04).
Conclusion: Collaboration between participants and health professionals resulted in more specific goals directed towards the activities and participation component. Goal achievement predicted long-term mental functioning following rehabilitation.
Keywords: adapted physical activity, disability, rehabilitation, participation, goal-setting, international classification of functioning, disability and health
Introduction
The present study explores the goal-setting process in a rehabilitation setting focusing on adapted physical activity (APA) and participation. The identification of a person’s goals and wishes is believed to be a key element and crucial for the success of rehabilitation interventions.1–3 Goals should reflect the perspective of the persons living with the disability. Goal-setting needs to be conducted in close collaboration between the individual and the health professionals as a basis for individually tailored rehabilitation interventions.4–6 Advantages of patient involvement in goal-setting are increased patient motivation, patient satisfaction and greater achievement of goals.2,7–10
Insufficient implementation of personally valuable goals is known to be a reason for dissatisfaction with rehabilitation, and capturing the patients’ concerns and perspectives is essential for goal achievement.6,11 When setting goals for a treatment period, health professionals have to capture the content of the patients’ individual goals while also guiding the process and setting meaningful goals for both the patients and the health professionals. Ensuring a shared understanding is important for effective goal-setting and treatment, and it requires a common vocabulary as well as communicative processes between the patient and the multidisciplinary team.12,13
The International Classification of Functioning, Disability and Health (ICF) describes functioning associated with different health conditions.14 The ICF has a biopsychosocial perspective that captures various components and facilitates the collection of data on chronic health conditions.15 For goal-setting, the ICF has been used to give structure to the goals by linking the content to components in the ICF, ensuring comparability and reproducibility of goals and goal-setting processes.6,16,17 Mapping goals to ICF identifies specific targets for intervention and establishes a common language within the multidisciplinary team.16,18
Regarding patients’ and health providers’ reported goals, previous studies have indicated that health providers tend to set goals focusing on body function, while patients tend to have a more participation-centered focus.19 Researchers have proposed that professionals set body function-goals because they are easily measured and evaluated, allowing patients to follow their progress.12,20 Rice et al21 found that in out-patient stroke rehabilitation, patients were significantly more satisfied with their body function-based goals compared to their activity and participation-based goals, concluding that these goals may be more realistically achieved during rehabilitation.21 Even though body function-goals are easy to measure and achieve and patients may be satisfied with such goals, when patients are involved in goal-setting they tend to set goals related to activities and participation.22,23
There is conflicting evidence regarding the effect of goal-setting on outcome,24,25 and there is a lack of studies investigating populations with chronic disabilities. Both Müller et al26 and Kus et al27 found significant associations between goal achievement in rehabilitation and overall functioning, while Lohmann et al22 did not find an association between these factors. The three above studies investigated patients in acute and post-acute phases after injury and standardized outcome measures of functioning were not applied. Coffey et al28 found that stronger goal pursuit and goal adjustment tendencies upon admission predicted lower disability and a better quality of life six months after discharge.28 They applied standardized outcome measures, but the population was in the post-acute phase after injury.
Physical activity is an important active ingredient offered to improve different aspects of health for people with disabilities.29 APA refers to physical activities that are adapted to the specific needs of each individual with a disability.30 The practical framework created by APA is used in several rehabilitation programs focusing on physical activity.
During the last decades rehabilitation research have had an increasing focus on participation and goal-setting in rehabilitation. Research have presented different aspects of goal-setting as it is carried out in clinical rehabilitation practice.31–35 Still, to our knowledge no studies have investigated goal-setting practices in rehabilitation interventions focusing on physical activity as the main ingredient.
Thus, the aims of the current study were 1) to identify goals set by individuals with chronic disabilities attending a rehabilitation program involving adapted physical activity, 2) to compare these goals to the negotiated goals set in collaboration with the rehabilitation team and 3) to assess goal achievement and its association with self-reported functioning after 12 months.
Materials and Methods
Design
The study was a prospective observational study in which data were collected through written questionnaires administered at baseline (eight weeks before rehabilitation), admission, discharge and follow-up (four weeks and 12 months after rehabilitation). The paper is a secondary analysis of the data collected and published in a randomized controlled trial.36 The study was conducted in accordance with the Declaration of Helsinki.
Setting
The study was conducted at Beitostølen Healthsports Centre (BHC), a rehabilitation institution located in the mountains of Norway that specializes in inpatient rehabilitation for children and adults with chronic disabilities. This rehabilitative care is part of specialist care and funded by the government. The rehabilitation program at BHC is based on APA. The main scope of the program is to support individual goal achievement in order to increase activity and participation. The rehabilitation is group oriented with individual goal-based schedules. Health professionals at BHC are working multidisciplinary in rehabilitation teams. They are familiar with the ICF, and goal-setting and schedule planning is carried out using the ICF framework.
Participants
Participants with chronic disabilities, as defined by the World Health Organization,37 who were aged 18 to 73 years and admitted to a four-week rehabilitation program at BHC between September 2010 and December 2012 were assessed for eligibility. The exclusion criteria were insufficient knowledge of Norwegian to fill out the questionnaires and severe cognitive disorders. Participants who participated in the rehabilitation program and signed the written informed consent form were included. The study was approved on the 27th of December in 2008 by the Regional Medical Committee for Research Ethics in Norway (S-08837c 2008/21144). See Figure 1 for details on the participant inclusion process.
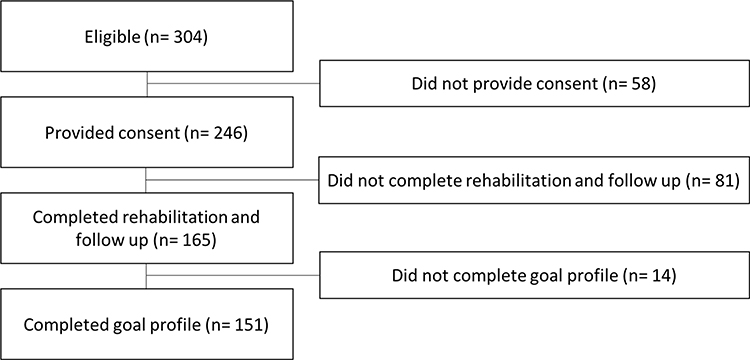 |
Figure 1 Flow chart of the participant inclusion process. |
Assessments
The questionnaires administered to the participants at baseline and the 12-month follow-up were used for the analyses in this paper. Baseline measures were gathered at home 8 weeks before rehabilitation and not at admission to ensure comparability with the follow-up measures, also gathered in the patient’s home environment.
Self-reported physical and mental functioning were measured by the Medical Outcomes Study 12-item Short-Form Health Survey (SF-12, license number QM 027126).38,39 The SF-12 consists of 12 items and yields a Physical Component Summary score (PCS) and Mental Component Summary score (MCS). The PCS and MCS norm-based scores for the SF-12 were calculated.40
Goal-Setting
Participants provided short-term goals for the rehabilitation stay in two different ways.
In the questionnaire administered to the participants at admission, they were asked to write down two goals for the rehabilitation stay (hereafter termed individual goals). The goals were listed by the participants alone, before entering the rehabilitation facility and meeting the rehabilitation team.
Goals were also gathered from the observed goal-setting practice at BHC, where the participants set one to four goals for the rehabilitation stay in collaboration with the rehabilitation team (hereafter termed negotiated goals). The goals were negotiated in a meeting where the person attending rehabilitation sat down together with one or more health professionals from the rehabilitation team and discussed desired goals and possibilities ending with the final negotiated goals for the stay.
Goal Achievement
At discharge, the participants rated their level of achievement of the two individual goals on a 10-point numeric rating scale (NRS), ranging from “no achievement” (1) to “full achievement” (10) for each goal. The mean value of the two scores was calculated for use in the analyses. NRS are widely used to rate pain intensity,41,42 and have also been validated for use in research regarding other subjective health concerns,43–47 allowing parametric statistical approaches.
Linking Goals to the ICF
Goals were linked to the ICF according to the established linking rules by Cieza et al.48,49 The linking was performed in the following manner: a) Two researchers with good knowledge of the ICF separately extracted meaningful concepts (one or more) from the goals. b) Each meaningful concept was linked to a second-level ICF category within the four ICF components Body Functions (b), Body Structures (s), Activities and Participation (d) and Environmental factors (e).14 This was also performed by two researchers separately. c) When the researchers disagreed, a third researcher selected the final ICF category to reach a consensus. For example, the goal “improve walking skills” with the meaningful concept “walking”, was linked to the ICF-category “d450 walking”.
Meaningful concepts that could not be linked to ICF-components were given descriptor codes, as described in the linking rules, including “personal factors” (pf) and “health condition” (hc). The descriptor codes also included concepts that were not sufficiently specific to be linked to the second level of the ICF and were termed “not definable” (nd). If these concepts were related to physical health, they were termed “not definable physical health” (ndph). The same process was followed for concepts regarding mental health (ndmh) and quality of life (ndqol).
Capturing Individual Goals
A participant’s individual goals were compared to negotiated goals by comparing the ICF categories (including the specific descriptors) linked from the goals. The individual goals of the participant were classified as captured if at least one of the ICF categories was retained in the negotiated goals.
Statistical Methods
All data were analyzed using SPSS, version 25. A significance level of p<0.05 was adopted. The association between goal achievement and long-term mental and physical functioning (PCS and MCS) was calculated by multiple regression analyses adjusting for age, gender and baseline PCS and MCS.
Results
Participants
Characteristics of the included participants are displayed in Table 1. The age, sex and disability distributions did not differ significantly between the groups of participants with a complete goal profile and those not completing rehabilitation, follow-up, or goal profile (p=0.09, p=0.29, p=0.85).
 |
Table 1 Characteristics of the Included Participants |
Neurological conditions, including cerebral palsy, multiple sclerosis and inherited motor neuron disorders, were the most frequent health conditions associated with disability (48%, Table 1). The reported musculoskeletal problems included rheumatic diseases. Cerebrovascular diseases, spinal cord injuries and visual impairments were among the other reported health conditions associated with disability. The median duration of the health condition associated with disability was 15.0 years (IQR 20.0).
The participants had a mean baseline PCS of 37.7 and MCS of 49.9. Their baseline PCS was clearly lower compared with a Norwegian reference population without disabilities (PCS 50.3 (SD 8.8), MCS 50.6 (SD 9.9).38
Individual Goals
Of the 151 participants, 142 set two individual goals, and nine set only one individual goal. In total, 293 individual goals were set.
Linking the 293 goals resulted in 374 meaningful concepts that were linked to the second level of the ICF, resulting in 408 codes. Of these codes, 337 (83%) fit into a second-level ICF category, while 71 (17%) were assigned a descriptor code. Of the 408 codes, 183 (45%) were linked to the Body functions component, 153 (37%) were linked to Activities and Participation and one (<1%) was linked to Environmental factors. The most frequently used ICF category among the individual goals was “d570 Looking after one’s health”, which was used in 54 of the 408 codes (13%). For more details, see Figure 2 and Table S1.
 |
Figure 2 Distribution of the ICF-components for the 408 ICF-codes linked from the 293 individual goals and the 490 ICF-codes linked from the 407 negotiated goals. |
Negotiated Goals
Of the 151 participants, 16 set four negotiated goals, 81 set three, 46 set two and eight participants set only one negotiated goal. In total, 407 negotiated goals were set.
Linking the 407 goals resulted in 459 meaningful concepts that were linked to the second level of the ICF, resulting in 490 codes. Of these codes, 439 (90%) fit into a second-level ICF category, while 51 (10%) were assigned a descriptor code. Of the 490 codes, 227 (46%) were linked to the Body functions component, 205 (42%) were linked to Activities and Participation and seven (2%) were linked to Environmental factors. The most frequently used ICF category among the negotiated goals was “d155 Acquiring skills”, which was used in 80 of the 490 codes (16%). For more details, see Figure 2 and Table S1.
Capturing Individual Goals
A total of 76% of the participants had negotiated goals that captured their individual goals, meaning that at least one of the ICF categories was retained in the negotiated goals. For 24% of the participants, none of the ICF categories in the individual goals were captured in the negotiated goals.
Achievement of Individual Goals
Of the 151 participants with a goal profile, 66% (n=98) listed a mean goal achievement of ≥9 points on the NRS scale. Only four participants listed a goal achievement of ≤5 points. Four participants did not answer the questions about goal achievement at discharge (Figure 3).
 |
Figure 3 Distribution of the participants (n=151) mean reported goal achievement at discharge. |
Regression models revealed that goal achievement was a significant predictor of the improvement in mental functioning (MCS) one year after rehabilitation. Goal achievement was not a predictor of the improvement in physical functioning (PCS) (Table 2).
 |
Table 2 Linear Regression Models of Goal Achievement as a Predictor for Long-Term Physical and Mental Functioning |
Discussion
The results show that even though both the participants’ individual goals and the negotiated goals were most frequently linked to the Body Functions ICF-component, the negotiated goals were more frequently linked to the Activities and Participation ICF-component. The negotiated goals were also more frequently sufficiently specific to be linked to a second-level ICF category. This result differs from previous researchers’ findings that showed that patients tend to set goals linked to the Activity and Participation ICF-component.19,22,23 A possible explanation to this is that the previous studies included participants attending acute or post-acute rehabilitation care, while the participants in the present study were in a chronic phase of disability and rehabilitation. It is known that patients’ focus shift from acute to chronic phases of disability. BHC is a rehabilitation facility focusing on increasing physical activity, which in goal-setting, might lead to a “body functions-oriented” focus on improving strength and endurance rather than a focus on being able to return to a “normal life”. The latter might be the focus in post-acute rehabilitation programs and might generate goals directed more towards activity and participation.
Siegert and Taylor13 have emphasized the fact that the context in which goal-setting takes place is important. When patients leave a stroke unit focused on activities of daily living, the content of their goals are likely to shift, with an emphasis on social functioning and reintegration in the community and the aspects patients are working towards in their home environment.13 Although the present study investigates rehabilitation for individuals in a chronic phase of disability, it still involves this inpatient context focusing on increasing physical activity. When setting goals to reflect the desires during the inpatient rehabilitation period, the physical activity focus might lead to the high frequency of body functions-oriented goals.
The fact that body function-goals were most frequently used can also be a result of the strong connection between goal-setting and active ingredients in rehabilitation. Previous research states that many of the goals set by therapists can be interpreted as treatment interventions, suggesting that therapists’ goals are actually stepping stones to an end point that may be representative of a goal at the activity and participation level.12
More of the goals set by the individuals alone (17%) than negotiated goals (10%) had descriptor codes representing concepts that could not be coded to a specific category in the ICF. When the goals were linked to the ICF, we found that many of the units regarding physical health and exercise in general could not be linked to a specific ICF category because they were too vague, for example “improving physical health”. They were given the descriptor code ndph as described in the linking rules.49 Lohmann et al investigated goals set by patients in early post-acute rehabilitation and reported similar results.22 They found that 120 of 546 goals (22%) could not be coded into second-level ICF categories mainly because they were overly broad regarding improvement in a general health condition or autonomy. They argued that because of this, an important task for the rehabilitation team is to specify the goals by breaking them down into smaller and more specific components while still ensuring that they correspond to the initial goal of the patient.22 Muller et al performed research in patients in the acute phase in hospitals and found that patients tend to express their views and goals in very general phrases.26 They also concluded that it is the health professionals who must clarify the general goals in a more detailed way and deconstruct them into components that can be addressed by therapy.26,27,50 Locke and Latham’s goal-setting theory states that specific, high (challenging) goals lead to a higher level of task performance than do easy goals or vague, abstract goals, such as the exhortation to “do one’s best”.51 Knowing this and that the rehabilitation team at BHC is trained in goal-setting, we expected the descriptor code ndph to decrease from the process of setting individual goals to that of setting negotiated goals with the rehabilitation team, which did not occur. The descriptor code ndph remained equally frequent in both the individual goals and the negotiated goals (9% of all the codes). Nevertheless, the number of other descriptor codes representing other concepts that could not be linked, such as hc (health condition), nd (not definable) or pf (personal factor), was less prevalent in the negotiated goals than in the individual goals (8% versus 1%), indicating that skilled health professionals in the rehabilitation team are better at specifying goals, as suggested by previous research. This is also the case for the ICF category most frequently used in the individual goals, “d570 Looking after one’s health”. Relatively vague meaningful concepts regarding having good health, such as “getting into shape”, were linked to this category. The category decreased in prevalence through the negotiating process (from 13% of the codes from the individual goals to 9% of the codes from the negotiated goals), indicating that the health professionals are skilled in specifying these types of goals.
The health professionals at BHC are familiar with the ICF, and goal-setting and schedule planning are carried out using the ICF framework. This may explain why the negotiated goals are more easily linked to the ICF. There is no standardized language connected to the ICF that is used when setting goals at BHC, but every active ingredient chosen after goal-setting is connected to a desired improvement or ability that can be linked to an ICF category. Integrating the ICF in the clinical goal-setting practice has been discussed as a way of standardizing goal-setting processes, making them comparable, and making it easier to involve goal-setting in outcome evaluations.16,23 Standardizing how patients and clinicians develop goals by using the ICF might promote collaboration between the two parties and encourage more clinicians to adopt collaborative goal-setting in their practice, as it serves as an implementation framework.52 However, previous studies have stressed that standardized language such as the ICF should not limit the content of goal-setting, particularly the specificity of the goals.23
The ICF category most frequently used in the negotiated goals was “d155 Acquiring skills”. Meaningful concepts about getting to know and learning to manage new activities were linked to this category. One of the main focuses of rehabilitation at BHC is activity competence; to gain knowledge of and learn to manage activities that can be transferred to the participant’s local environment.5 The focus on activity rather than impairment and body function has always been one of the cornerstones of the rehabilitation facility. Learning to manage an activity properly is an equally or even more important skill than improving muscle power or endurance when the endpoint is being active and participating in a community setting after the rehabilitation program. The high frequency of this ICF category in the negotiated goals reflects BHC’s focus. Another main focus of BHC is adaptation of assistive devices for activity. Hence, one might wonder why components in the ICF-category environmental factors were almost absent in both the individual and negotiated goals. Adaptation of devices and using devices to be active are not goals, but examples of active ingredients needed to reach the main goal which, in this case, is the activity. If the goal was to learn how to ride a bike, adapting the bike is not the goal, but an ingredient needed, a stepping stone towards reaching the goal. However, making adaptation of equipment inherent to the activity goals more explicitly in the negotiated goal setting process, might uncover failed goal attainment due to unsuccessful adaptation of the equipment.
Three-quarters of the participants experienced at least one of the ICF categories or descriptor codes from their individual goals being captured in the negotiated goals, meaning that as many as one-quarter of the participants experienced their initial goals not being captured at all. Some of the goals may not have been captured because the categories changed as they were specified in the negotiating process. In this process the rehabilitation team added useful information about what they believed was possible to achieve with the participant’s foundation, what the facility can offer, how seasons and weather might interfere and more. Through the goal-setting meeting the individual goals were negotiated to meet the possibilities offered by the rehabilitation and the individually tailored rehabilitation was fitted to meet the demands stated by the participant’s goals. This reasoning may also apply to goals that could not be realistically achieved during the four-week rehabilitation program. The team working at BHC encourages individuals to work towards every challenging goal that is possible to achieve, but goals that were clearly impossible to achieve within the time frame of the program, were modified through the negotiating process. As previously mentioned, challenging goals lead to high task performance, but goals that are too challenging might compromise an individual’s focus regarding his or her ability to complete the steps to achieve the goal.51
To the best of our knowledge, this is the first study investigating the association between goal achievement and outcome of rehabilitation in a mixed diagnostic study population with chronic disabilities using standardized outcome measures (SF-12). The results indicate that goal achievement is associated with long-term improvement in mental functioning one year after rehabilitation. This association was not found for physical functioning, even though there was improvement. The goals reflect that the rehabilitation context at BHC is focused on physical activity. Interestingly, it was mental functioning rather than physical functioning that was affected by achieving these goals. According to self-determination theory, the satisfaction of needs for autonomy, competence, and relatedness is a universal requirement for psychological well-being.53 Goal achievement is a factor commonly leading to the satisfaction of needs; hence, achieving goals should lead to psychological well-being. A previous study carried out on individuals at BHC found that satisfaction of psychological needs at the end of the program was positively linked to SF-12 mental functioning during the program.54 The results on long-term improvements in physical and mental functioning following rehabilitation in this population were previously published by the same research group.55 The study indicated that low levels of fatigue and high self-efficacy contributed to improvement in functioning, however, many of the factors predicting the improvement remained unknown. The present study indicates that goal achievement can be included as a predictor of long-term improvement in mental functioning.
Strengths and Limitations
The strengths of this study include the comparison of individual goals with negotiated goals set with the rehabilitation team, and the evaluation of goal achievement as a predictor of outcome using standardized outcome measures.
This study has a methodological weakness in regard to measuring goal achievement. In the questionnaire on goal achievement that was administered at discharge, the participants were not asked to specify which goals they considered achieved. Another weakness is that a validated cut-off value was not used in the measurement of goal achievement on an NRS from 1–10. There is a lack of validated simple tools to measure goal achievement. Goal attainment scaling (GAS) with adjustments for the degree of goal achievement in which partial completion and additional achievement are recognized, is a possible instrument for goal-setting.25 These factors captured by GAS were, however, not part of the clinical goal assessment for adults at BHC which this study observed and explored “as is”. Using GAS in the present study would demand more resources as GAS is complex and requires trained personnel. The NRS was chosen to measure goal achievement because it is quick, convenient, and easy to understand, allowing parametric statistical approaches. To validate the NRS with GAS, might have strengthened the results presented. In addition, goal-setting processes are complex, and assessing these processes may require supplementary qualitative approaches.
The study did not address the participant’s cognition except from the exclusion criterion “severe cognitive disorders”. Addressing cognition might giver further insight into characteristics associated with goal-setting as it is well known that cognitive impairments influences goal setting.56
Data collection occurred several years before this paper was published. Still, the rehabilitation carried out at the facility including the goal-setting procedures, have not changed and the present results are highly relevant.
The participants undergoing rehabilitation at BHC might not be representative of the general Norwegian population with disabilities, especially regarding their interest in physical activity. Individuals are referred to BHC because they wish to engage in the rehabilitation offered at BHC, and most of them are well aware of the intensive physical program. This might weaken the external validity of the results in this study. On the other hand, the inclusion and exclusion criteria were not strict, and most of the individuals at BHC were eligible for enrolment in this study, which strengthens the validity of the study.
The theory of APA does not focus on diagnoses, but on possibilities of participation in the environment, with the result that most APA-based rehabilitations are catered for people with a mixed diagnostic background. This is reflected in the present study’s patient population that has a wide heterogeneity in diagnoses associated with disability. Still, it is the common focus, and not the heterogeneity which makes this intervention comparable to other interventions based on APA along with a wide variety of interventions focusing on participation.
Conclusions
Adults with chronic disabilities participating in a rehabilitation program focusing on APA most frequently set individual goals with meaningful concepts that could be linked to the ICF-component Body functions. Goal negotiation with the rehabilitation team increased the frequency of goals linked to Activities and Participation and more specific goals. Goal achievement was a predictor for long-term improvement in mental functioning following the rehabilitation program. The study provides knowledge on the components of goal-setting that can be used to develop rehabilitation interventions in the future. Clinical practice should implement validated goal-setting processes, and goal achievement should be included as a predictor of successful rehabilitation interventions.
Acknowledgments
We would like to thank Oddlaug Hovi Gullaksen and Bjørg Anita Gustavsen Riste for their valuable support, help with data collection and the administration of the study and Dorte Louise Sagen for helping out in the linking process. This work was supported by the Sophies Minde Foundation.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Gardner T, Refshauge K, McAuley J, Hübscher M, Goodall S, Smith L. Combined education and patient-led goal setting intervention reduced chronic low back pain disability and intensity at 12 months: a randomised controlled trial. Br J Sports Med. 2019;53(22):1424–1431. doi:10.1136/bjsports-2018-100080
2. Levack WM, Weatherall M, Hay-Smith EJ, Dean SG, McPherson K, Siegert RJ. Goal setting and strategies to enhance goal pursuit for adults with acquired disability participating in rehabilitation. Cochrane Database Syst Rev. 2015;(7):Cd009727. doi:10.1002/14651858.CD009727.pub2
3. Wade DT. Goal setting in rehabilitation: an overview of what, why and how. Clin Rehabil. 2009;23(4):291–295. doi:10.1177/0269215509103551
4. Kersten P, Ellis-Hill C, McPherson KM, Harrington R. Beyond the RCT - understanding the relationship between interventions, individuals and outcome - the example of neurological rehabilitation. Disabil Rehabil. 2010;32(12):1028–1034. doi:10.3109/09638281003775568
5. Imms C, Granlund M, Wilson PH, Steenbergen B, Rosenbaum PL, Gordon AM. Participation, both a means and an end: a conceptual analysis of processes and outcomes in childhood disability. Dev Med Child Neurol. 2017;59(1):16–25. doi:10.1111/dmcn.13237
6. Dekker J, de Groot V, Ter Steeg AM, et al. Setting meaningful goals in rehabilitation: rationale and practical tool. Clin Rehabil. 2020;34(1):3–12. doi:10.1177/0269215519876299
7. McAndrew E, McDermott S, Vitzakovitch S, Warunek M, Holm MB. Therapist and patient perceptions of the occupational therapy goal-setting process. Phys Occup Ther Geriatr. 2009;17(1):55–63. doi:10.1080/J148v17n01_05
8. Holliday RC, Cano S, Freeman JA, Playford ED. Should patients participate in clinical decision making? An optimised balance block design controlled study of goal setting in a rehabilitation unit. J Neurol Neurosurg Psychiatry. 2007;78(6):576–580. doi:10.1136/jnnp.2006.102509
9. Levack WMM, Dean SG, Siegert RJ, McPherson KM. Purposes and mechanisms of goal planning in rehabilitation: the need for a critical distinction. Disabil Rehabil. 2016;23(4):379. doi:10.1002/oti.1440
10. Turner-Stokes L, Rose H, Ashford S, Singer B. Patient engagement and satisfaction with goal planning: impact on outcome from rehabilitation. Int J Ther Rehabil. 2015;22(5):210–216. doi:10.12968/ijtr.2015.22.5.210
11. Dager TN, Kjeken I, Berdal G, et al. Rehabilitation for patients with rheumatic diseases: patient experiences of a structured goal planning and tailored follow-up programme. SAGE Open Med. 2017;5:2050312117739786. doi:10.1177/2050312117739786
12. Leach E, Cornwell P, Fleming J, Haines T. Patient centered goal-setting in a subacute rehabilitation setting. Disabil Rehabil. 2010;32(2):159–172. doi:10.3109/09638280903036605
13. Siegert RJ, Taylor WJ. Theoretical aspects of goal-setting and motivation in rehabilitation. Disabil Rehabil. 2004;26(1):1–8. doi:10.1080/09638280410001644932
14. World Health Organization. International Classification of Functioning, Disability and Health: ICF. World Health Organization; 2001.
15. World Health Organization. Towards a Common Language for Functioning, Disability and Health: ICF. World Health Organisation; 2002.
16. Nguyen L, Cross A, Rosenbaum P, Gorter JW. Use of the international classification of functioning, disability and health to support goal-setting practices in pediatric rehabilitation: a rapid review of the literature. Disabil Rehabil. 2019;1–11. doi:10.1080/09638288.2019.1643419
17. Angeli JM, Schwab SM, Huijs L, Sheehan A, Harpster K. ICF-inspired goal-setting in developmental rehabilitation: an innovative framework for pediatric therapists. Physiother Theory Pract. 2019;1–10. doi:10.1080/09593985.2019.1692392
18. Eftekhar P, Mochizuki G, Dutta T, Richardson D, Brooks D. Goal attainment scaling in individuals with upper limb spasticity post stroke. Occup Ther Int. 2016;23(4):379–389. doi:10.1002/oti.1440
19. Soberg HL, Finset A, Roise O, Bautz-Holter E. Identification and comparison of rehabilitation goals after multiple injuries: an ICF analysis of the patients’, physiotherapists’ and other allied professionals’ reported goals. J Rehabil Med. 2008;40(5):340–346. doi:10.2340/16501977-0174
20. Glazier SR, Schuman J, Keltz E, Vally A, Glazier RH. Taking the next steps in goal ascertainment: a prospective study of patient, team, and family perspectives using a comprehensive standardized menu in a geriatric assessment and treatment unit. J Am Geriatr Soc. 2004;52(2):284–289. doi:10.1111/j.1532-5415.2004.52072.x
21. Rice DB, McIntyre A, Mirkowski M, et al. Patient-centered goal setting in a hospital-based outpatient stroke rehabilitation center. PMR. 2017;9(9):856–865. doi:10.1016/j.pmrj.2016.12.004
22. Lohmann S, Decker J, Muller M, Strobl R, The GE. ICF forms a useful framework for classifying individual patient goals in post-acute rehabilitation. J Rehabil Med. 2011;43(2):151–155. doi:10.2340/16501977-0657
23. Haas B, Playford ED, Ahmad AQ, Yildiran T, Gibbon AJ, Freeman JA. Rehabilitation goals of people with spinal cord injuries can be classified against the international classification of functioning, disability and health core set for spinal cord injuries. Spinal Cord. 2016;54(4):324–328. doi:10.1038/sc.2015.155
24. Levack WM, Taylor K, Siegert RJ, Dean SG, McPherson KM, Weatherall M. Is goal planning in rehabilitation effective? A systematic review. Clin Rehabil. 2006;20(9):739–755. doi:10.1177/0269215506070791
25. Hurn J, Kneebone I, Cropley M. Goal setting as an outcome measure: a systematic review. Clin Rehabil. 2006;20(9):756–772. doi:10.1177/0269215506070793
26. Muller M, Strobl R, Grill E. Goals of patients with rehabilitation needs in acute hospitals: goal achivement is an indicator for improved functioning. J Rehabil Med. 2011;43(2):145–150. doi:10.2340/16501977-0652
27. Kus S, Muller M, Strobl R, Grill E. Patient goals in post-acute geriatric rehabilitation--goal attainment is an indicator for improved functioning. J Rehabil Med. 2011;43(2):156–161. doi:10.2340/16501977-0636
28. Coffey L, Gallagher P, Desmond D. Goal pursuit and goal adjustment as predictors of disability and quality of life among individuals with a lower limb amputation: a Prospective Study. Arch Phys Med Rehabil. 2014;95(2):244–252. doi:10.1016/j.apmr.2013.08.011
29. Anderson LS, Heyne LA. Physical activity for children and adults with disabilities: an issue of “amplified” importance. Disabil Health J. 2010;3(2):71–73. doi:10.1016/j.dhjo.2009.11.004
30. Hutzler Y, Sherrill C. Defining adapted physical activity: international perspectives. Adapt Phys Activ Q. 2007;24(1):1–20. doi:10.1123/apaq.24.1.1
31. Scobbie L, McLean D, Dixon D, Duncan E, Wyke S. Implementing a framework for goal setting in community based stroke rehabilitation: a process evaluation. BMC Health Serv Res. 2013;13(1):190. doi:10.1186/1472-6963-13-190
32. Holliday RC, Ballinger C, Playford ED. Goal setting in neurological rehabilitation: patients’ perspectives. Disabil Rehabil. 2007;29(5):389–394. doi:10.1080/09638280600841117
33. Levack WM, Dean SG, Siegert RJ, McPherson KM. Navigating patient-centered goal setting in inpatient stroke rehabilitation: how clinicians control the process to meet perceived professional responsibilities. Patient Educ Couns. 2011;85(2):206–213. doi:10.1016/j.pec.2011.01.011
34. Cameron LJ, Somerville LM, Naismith CE, Watterson D, Maric V, Lannin NA. A qualitative investigation into the patient-centered goal-setting practices of allied health clinicians working in rehabilitation. Clin Rehabil. 2018;32(6):827–840. doi:10.1177/0269215517752488
35. Draaistra H, Singh MD, Ireland S, Harper T. Patients’ perceptions of their roles in goal setting in a spinal cord injury regional rehabilitation program. Can J Neurosci Nurs. 2012;34(3):22–30.
36. Roe C, Preede L, Dalen H, et al. Does adapted physical activity-based rehabilitation improve mental and physical functioning? A randomized trial. Eur J Phys Rehabil Med. 2016.
37. World Health Organization. World report on disability. Available from: http://whqlibdoc.who.int/publications/2011/9789240685215_eng.pdf?ua=1.
38. Gandek B, Ware JE, Aaronson NK, et al. Cross-validation of item selection and scoring for the SF-12 health survey in nine countries: results from the IQOLA project. International quality of life assessment. J Clin Epidemiol. 1998;51(11):1171–1178. doi:10.1016/S0895-4356(98)00109-7
39. Ware J
40. Ware JE, Kosinski M, Turner-Bowker DM, Gandek B. How to Score Version 2 of the SF-12(R) Health Survey. QualityMetric Incorporated; 2002.
41. Williamson A, Hoggart B. Pain: a review of three commonly used pain rating scales. J Clin Nurs. 2005;14(7):798–804. doi:10.1111/j.1365-2702.2005.01121.x
42. Childs JD, Piva SR, Fritz JM. Responsiveness of the numeric pain rating scale in patients with low back pain. Spine (Phila Pa 1976). 2005;30(11):1331–1334. doi:10.1097/01.brs.0000164099.92112.29
43. Gladman D, Nash P, Goto H, et al. Fatigue numeric rating scale validity, discrimination and responder definition in patients with psoriatic arthritis. RMD Open. 2020;6(1):e000928. doi:10.1136/rmdopen-2019-000928
44. Farrar JT, Troxel AB, Stott C, Duncombe P, Jensen MP. Validity, reliability, and clinical importance of change in a 0–10 numeric rating scale measure of spasticity: a post hoc analysis of a randomized, double-blind, placebo-controlled trial. Clin Ther. 2008;30(5):974–985. doi:10.1016/j.clinthera.2008.05.011
45. Gift AG, Narsavage G. Validity of the numeric rating scale as a measure of dyspnea. Am J Crit Care. 1998;7(3):200–204. doi:10.4037/ajcc1998.7.3.200
46. Surti B, Spiegel B, Ippoliti A, et al. Assessing health status in inflammatory bowel disease using a novel single-item numeric rating scale. Dig Dis Sci. 2013;58(5):1313–1321. doi:10.1007/s10620-012-2500-1
47. Lampropoulou S, Nowicky AV. Evaluation of the numeric rating scale for perception of effort during isometric elbow flexion exercise. Eur J Appl Physiol. 2012;112(3):1167–1175. doi:10.1007/s00421-011-2074-1
48. Cieza A, Brockow T, Ewert T, et al. Linking health-status measurements to the international classification of functioning, disability and health. J Rehabil Med. 2002;34(5):205–210. doi:10.1080/165019702760279189
49. Cieza A, Geyh S, Chatterji S, Kostanjsek N, Ustun B, Stucki G. ICF linking rules: an update based on lessons learned. J Rehabil Med. 2005;37(4):212–218. doi:10.1080/16501970510040263
50. Wressle E, Oberg B, Henriksson C. The rehabilitation process for the geriatric stroke patient--an Exploratory Study of goal setting and interventions. Disabil Rehabil. 1999;21(2):80–87. doi:10.1080/096382899298016
51. Locke EA, Latham GP. New directions in goal-setting theory. Curr Dir Psychol Sci. 2006;15(5):265–268. doi:10.1111/j.1467-8721.2006.00449.x
52. Constand MK, MacDermid JC. Applications of the international classification of functioning, disability and health in goal-setting practices in healthcare. Disabil Rehabil. 2014;36(15):1305–1314. doi:10.3109/09638288.2013.845256
53. Church AT, Katigbak M, Locke K, et al. Need satisfaction and well-being. J Cross Cult Psychol. 2013;44(4):507–534. doi:10.1177/0022022112466590
54. Sæbu M. Physical Activity and Motivation in Young Adults with a Physical Disability. [PhD thesis]. Norwegian School of Sport Sciences; 2011.
55. Preede L, Saebu M, Perrin PB, et al. One-year trajectories of mental and physical functioning during and after rehabilitation among individuals with disabilities. Health Qual Life Outcomes. 2015;13(1):135. doi:10.1186/s12955-015-0328-z
56. Rosewilliam S, Roskell CA, Pandyan AD. A systematic review and synthesis of the quantitative and qualitative evidence behind patient-centred goal setting in stroke rehabilitation. Clin Rehabil. 2011;25(6):501–514. doi:10.1177/0269215510394467
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.