")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 19
Real-World Disease Burden and Healthcare Resource Utilization Among Patients with COPD and Asthma Using Triple Therapy (FF/UMEC/VI) in the United States
Authors Igboekwe E, Verma S, Paczkowski R
Received 12 July 2023
Accepted for publication 19 December 2023
Published 25 January 2024 Volume 2024:19 Pages 281—296
DOI https://doi.org/10.2147/COPD.S423993
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Emmeline Igboekwe,1 Sumit Verma,2 Rosirene Paczkowski3
1US Medical Affairs, R&D Global Medical, GSK, Durham, NC, USA; 2STATinMED, LLC, Dallas, TX, USA; 3Value Evidence and Outcomes, R&D Global Medical, GSK, Collegeville, PA, USA
Correspondence: Rosirene Paczkowski, GSK, Upper Providence UP4410, 1250 South Collegeville Road, Collegeville, PA 19426, USA, Tel +1 904.832.7934, Email [email protected]
Purpose: Chronic obstructive pulmonary disease (COPD) and asthma are associated with chronic inflammation of the respiratory tract; despite some overlap of symptoms, they are considered separate disorders. Triple therapy is recommended for patients with COPD and asthma whose symptoms remain uncontrolled despite dual therapy. There are limited real-world studies evaluating outcomes among patients with COPD and asthma who are receiving inhaled triple therapy. This United States (US)-based real-world study aimed to evaluate clinical and economic outcomes among patients with COPD and asthma receiving single-inhaler triple therapy (fluticasone furoate/umeclidinium/vilanterol [FF/UMEC/VI]).
Patients and Methods: Retrospective pre-post study using claims data from the Optum Clinformatics® database. Patients with COPD and asthma were indexed on the first date of FF/UMEC/VI prescription (1 October 2017– 31 March 2019). Each patient acted as their own control. Patients were required to have continuous health plan enrollment for 12 months prior to (pre-treatment) and following (post-treatment) index. Exacerbations, all-cause and COPD-related healthcare resource utilization, and costs were compared before and after FF/UMEC/VI initiation.
Results: Overall, 2743 patients were included (mean age: 71 years; 64% female). Cardiovascular disease was the most prevalent comorbidity during both the pre- and post-treatment periods (90% for both periods). There was a lower proportion of patients with ≥ 1 COPD exacerbation or ≥ 1 asthma exacerbation post-treatment versus pre-treatment (51% vs 57%, p< 0.0001, and 22% vs 32%, p< 0.0001, respectively). Fewer patients had ≥ 1 all-cause office visit post-treatment versus pre-treatment (99.3% vs 99.7%, p=0.0329); more patients had ≥ 1 COPD-related office visit post-treatment versus pre-treatment (89.6% vs 87.5%, p=0.0035). Total all-cause healthcare costs were significantly higher post-treatment versus pre-treatment ($72,809 vs $63,734, p< 0.0001). The driver of increased costs appeared to be primarily non-COPD-related (COPD-related costs: post-treatment $27,779 vs pre-treatment $25,081, p=0.0062).
Conclusion: FF/UMEC/VI reduced exacerbations among patients with COPD and asthma in a real-world setting in the US.
Plain Language Summary: Chronic obstructive pulmonary disease (COPD) and asthma are different respiratory conditions that have similar symptoms. Patients can be diagnosed with both conditions at the same time. A flare-up of COPD or asthma symptoms can lead to a lung attack, which can result in hospitalization and a considerable decline in patient health as well as being associated with high healthcare resource use and costs.
An inhaler with three different medicines (fluticasone furoate, umeclidinium, and vilanterol; shortened to FF/UMEC/VI) can be prescribed for patients with COPD or asthma. This study was done to assess how FF/UMEC/VI (taken using a single inhaler) affected lung attacks as well as healthcare resource use and costs among patients who have been diagnosed with both COPD and asthma.
This study found that fewer patients experienced a lung attack in the first 12 months after starting FF/UMEC/VI compared with the 12 months before starting FF/UMEC/VI. A lower proportion of patients had ≥ 1 medical office visit, ≥ 1 hospital admission, or ≥ 1 emergency room visit after starting FF/UMEC/VI compared with before FF/UMEC/VI. Many patients in this study had other medical conditions such as heart and kidney disease as well as their asthma and COPD. Although total healthcare costs were higher for patients after they had started FF/UMEC/VI compared with before, this appeared to be mainly due to patients’ other medical conditions, besides from COPD.
FF/UMEC/VI may be able to reduce future symptom flare-ups and lung attacks in patients who have been diagnosed with both COPD and asthma.
Keywords: asthma, chronic obstructive pulmonary disease, exacerbation, HCRU, real-world, triple therapy
Introduction
Chronic obstructive pulmonary disease (COPD) is one of the leading causes of mortality in the United States (US),1 and is associated with a substantial economic burden.2 Exacerbations of COPD, defined as an acute worsening of respiratory symptoms, can result in prolonged illness and hospitalization.3 Following a severe exacerbation, patients are likely to experience a significant decrease in quality of life and an increase in healthcare resource utilization (HCRU) and costs.4 Hospitalization due to severe exacerbation is also associated with poor long-term prognosis and higher mortality risk.5 Preventing exacerbations among patients with COPD using appropriate treatment is therefore crucial.
Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommendations state that for patients with a history of ≥2 moderate exacerbations or ≥1 severe exacerbations (leading to hospitalization) in the last year and elevated blood eosinophil counts (≥300 cells/µL), triple therapy (long-acting β2-agonist [LABA] + long-acting muscarinic antagonist [LAMA] + inhaled corticosteroid [ICS]) should be considered as initial maintenance therapy.6 For patients who experience recurrent exacerbations whilst receiving mono or dual bronchodilator therapy an escalation to triple therapy is recommended. The GOLD strategy suggests that if there is any indication for ICS, triple therapy should be the preferred treatment choice (dual therapy with an ICS is no longer recommended for patients with COPD).6
Historically, triple therapy required the use of multiple devices. Fluticasone furoate/umeclidinium/vilanterol (FF/UMEC/VI) is a single-inhaler triple therapy (SITT), approved by the US Food and Drug Administration in September 2017 for the long-term maintenance of COPD.7 FF/UMEC/VI has been shown to reduce exacerbations and improve lung function and health status compared with dual therapy.8 In addition, the cost-effectiveness of FF/UMEC/VI versus dual therapy and multiple-inhaler triple therapy (MITT) among patients with COPD has previously been demonstrated.9–13
Patients with COPD who are receiving triple inhaled therapy were often symptomatic prior to initiation of triple therapy and may be vulnerable to further pulmonary complications.6 Additionally, patients with COPD frequently experience concurrent comorbid diseases, such as cardiovascular disease, metabolic syndrome, osteoporosis, depression, anxiety, lung cancer, and asthma, which can contribute significantly to morbidity and mortality.6,14 Asthma is considered a risk factor for the development of COPD. Adults with asthma have a 12.5 times higher risk of acquiring COPD over time compared with those without asthma.15 A 2018 international review examining the epidemiology of COPD and asthma overlap, estimated that among patients with a COPD diagnosis, between 4.2% and 66.0% of patients also display features commonly associated with asthma, and among patients with an asthma diagnosis, between 11.1% and 61.0% of patients also display features commonly associated with COPD.16 Patients displaying features of both COPD and asthma have been shown to have a greater symptom burden, more frequent exacerbations, a more rapid decline in lung function, higher mortality, and higher HCRU compared with patients with COPD or asthma alone.17–19 Although both COPD and asthma are associated with chronic inflammation of the respiratory tract, and display some overlap of symptoms, they are now considered separate disorders.6 GOLD recommendations suggest that if concurrent COPD and asthma diagnoses are suspected, pharmacotherapy should primarily follow asthma guidelines.6 Global Initiative for Asthma (GINA) recommendations state that triple therapy should be considered for patients if their asthma remains uncontrolled with medium or high dose ICS + LABA.20 In September 2020, FF/UMEC/VI was approved for the maintenance treatment of asthma in patients aged ≥18 years; FF/UMEC/VI is the only SITT to be approved for both COPD and asthma.7
There is a lack of real-world evidence studies evaluating exacerbations and HCRU among patients with COPD and asthma who are receiving FF/UMEC/VI therapy. This US-based real-world study was designed to understand the exacerbation reduction potential of FF/UMEC/VI (taken using a single inhaler) in relation to HCRU and related costs among patients with COPD and asthma.
Materials and Methods
Study Design and Objectives
This was a retrospective pre-post cohort study using claims data from the Optum Clinformatics® database, which contains data on patient prescription drug history, medical history, and HCRU. The population covered by the database is predominantly in the South and North Central (Midwest) census regions of the US, although there are members in all 50 states. Pharmacy claims data are a profile of all outpatient prescription pharmacy services provided and covered by the health plan. Medical claims or encounter data are collected from all available health care sites (inpatient hospital, outpatient hospital, emergency department, physician’s office, surgery center, etc.) for virtually all types of provided services, including specialty, preventive, and office-based treatments. Medical claims data include multiple diagnosis codes recorded with International Classification of Diseases (ICD) 9th/10th revision diagnoses codes.
Data were obtained for the period from 1 October 2016 to 31 March 2020 (study period); 1 October 2017 to 31 March 2019 was defined as the identification period (Figure 1). The index date was the date of the first claim for FF/UMEC/VI. The 12-month period immediately prior to index was defined as the pre-treatment period and the 12-month period immediately following index was defined as the post-treatment period.
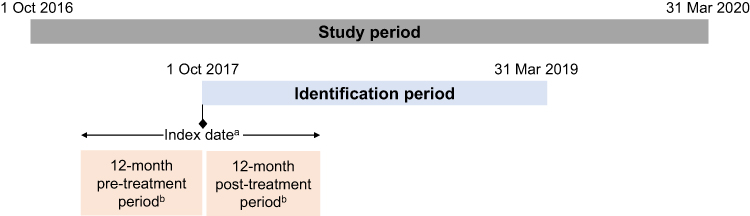 |
Figure 1 Study design. Abbreviations: COPD, chronic obstructive pulmonary disease; FF/UMEC/VI, fluticasone furoate/umeclidinium/vilanterol. Notes: aFirst prescription for FF/UMEC/VI during the identification period; bContinuous health plan enrollment. Patients were required to have ≥2 COPD medical claims and ≥2 asthma medical claims during the study period. |
The primary objective of this study was to compare the rate of any, moderate, and severe COPD exacerbations before and after the initiation of FF/UMEC/VI for patients with COPD and asthma. The secondary objectives were to compare all-cause and COPD-related HCRU and costs among patients with COPD and asthma receiving FF/UMEC/VI before and after treatment initiation, and to compare the rate of any, moderate, and severe asthma exacerbations before and after initiation of FF/UMEC/VI for patients with COPD and asthma.
Study Population
Patients with concurrent COPD and asthma diagnoses, who initiated triple therapy with FF/UMEC/VI were identified. Eligible patients were required to have ≥2 pharmacy or administration claims for FF/UMEC/VI during the identification period; have ≥2 diagnosis claims for COPD (ICD-10-clinical modification [CM]: J41–J44) anytime during the study period on different dates; have ≥2 diagnosis claims for asthma (ICD-10-CM: J45) anytime during the study period on different dates; be ≥40 years of age at index; and have continuous health plan enrollment with medical and pharmacy benefits for ≥12 months prior to index and for ≥12 months following index. Patients were excluded if they had ≥1 diagnosis claim for cystic fibrosis (ICD-10-CM: E84) or lung cancer (ICD-10-CM: C34.x) during the 12-month pre-treatment period, or if they had ≥1 prescription claim for any triple-therapy, including FF/UMEC/VI or MITT, prior to index.
Data Analysis
In this pre-post study, each patient acted as their own control. A description of the sociodemographic and clinical characteristics examined as of the index date/during the baseline period is shown in Supplementary Table 1. Dichotomous variables are reported using frequencies and percentages; continuous variables are reported using mean and standard deviation (SD). P-values comparing pre- and post-treatment initiation were calculated using paired t-tests for continuous variables and McNemar tests for dichotomous or categorical variables. For variables that deviated from the normal distribution assumption, generalized linear models, using a generalized estimating equation, were used to account for repeated measures as follows: for healthcare costs, a gamma distribution was used; for the number of exacerbations, a negative binomial distribution was used; and for the proportion of patients with exacerbations, a binomial distribution and logit link was used.
Multivariable Modeling
To model the proportion of patients with exacerbations in the pre-treatment period versus the post-treatment period, a generalized linear model with binomial distribution and logit link using general estimating equations was used. For each model, the odds ratios (ORs) for comparison of pre- and post-treatment proportions was calculated, including 95% confidence intervals (CIs), and p-values. Models for the proportion of patients with exacerbations and the number of exacerbations per patient were adjusted for the following variables: age on index date; COPD severity score on index date; sex; payer type; baseline medication use; the proportion of patients with baseline exacerbations/number of baseline exacerbations.
Results
Overall, 2743 patients were included in the final study sample (Figure 2). Patient demographics at baseline are reported in Table 1. The mean (SD) age was 71 (9.7) years and there were more female patients (n=1759; 64%) than male patients. Geographic regions represented in the US included the South (56%), the West (19%), and the Midwest (16%). In total, 86% of patients were Medicare enrollees and 14% of patients were commercially insured.
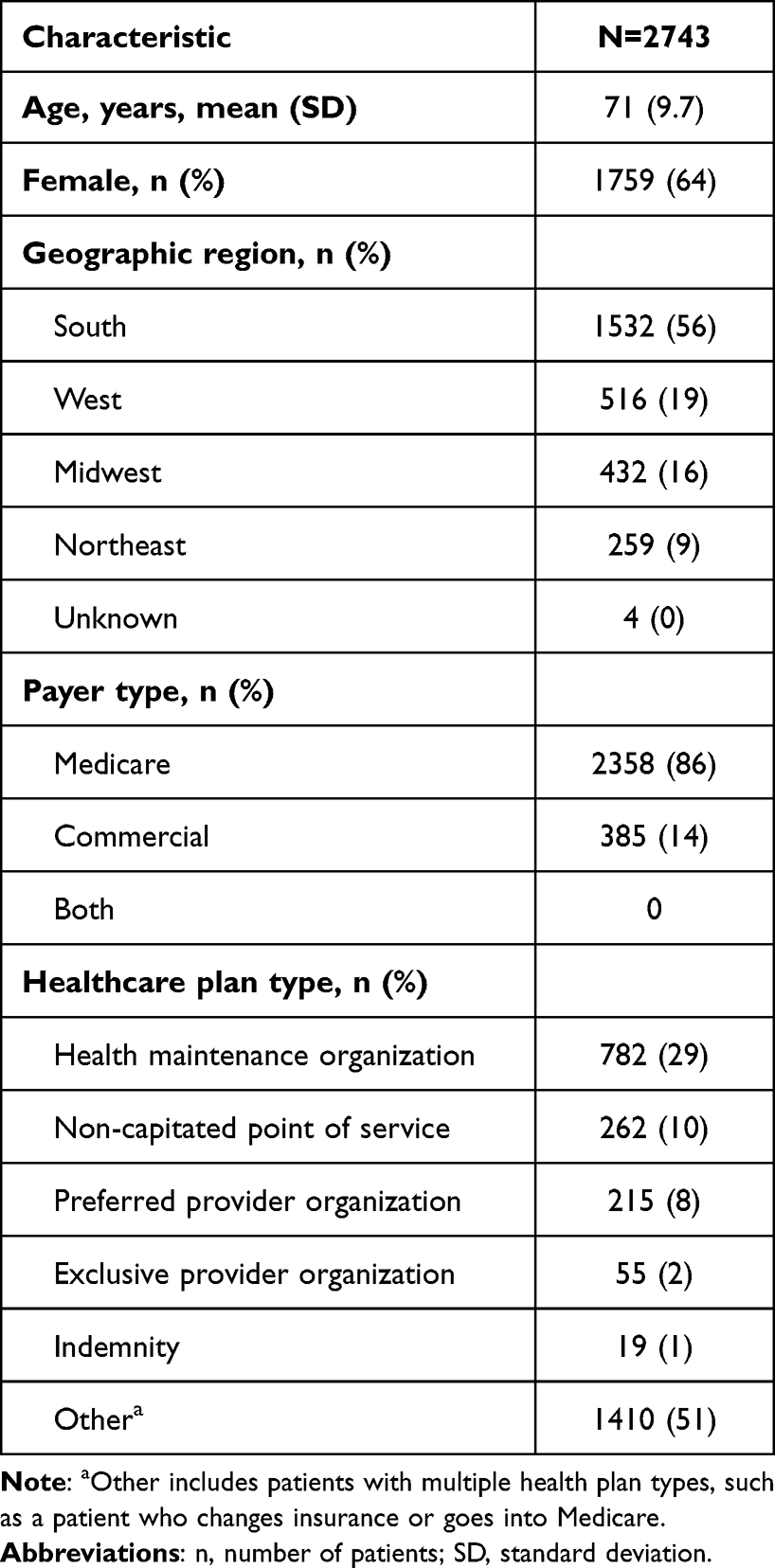 |
Table 1 Patient Demographics at Baseline |
 |
Figure 2 Patient attrition. Abbreviations: COPD, chronic obstructive pulmonary disease; FF/UMEC/VI, fluticasone furoate/umeclidinium/vilanterol; ICD-(CM), International Classification of Diseases-(Clinical Modification). Notes: aThe first medication claim date was classified as the index date; bICD-9-CM: 491, 492, or 496; ICD-10-CM: J41–J44; cICD-9-CM: 493; ICD-10-CM: J45; dICD-9-CM: 277.0x; ICD-10-CM: E84; eICD-9-CM: 162.x; ICD-10-CM: C34.x. |
Clinical Characteristics: Pre-Treatment versus Post-Treatment
The mean Charlson Comorbidity Index score was higher post-treatment compared with pre-treatment (4.53 vs 4.23, p<0.0001; Table 2). Cardiovascular disease was the most prevalent comorbidity during both the pre- and post-treatment periods (90% for both periods). During the post-treatment period, there was a significantly lower proportion of patients with pneumonia compared with the pre-treatment period (20% vs 23%, p=0.0032). Conversely, there was a significantly higher proportion of patients with chronic renal failure, depression, gastroesophageal reflux disease (GERD), and pulmonary vascular diseases during the post-treatment period compared with the pre-treatment period.
 |
Table 2 Clinical Characteristics and Exacerbation Outcomes Post-FF/UMEC/VI Treatment versus Pre-Treatment |
During the post-treatment period, there was a significant reduction in COPD severity score compared with the pre-treatment period (30.2 vs 32.7, p<0.0001). There was also a significant reduction in the number of claims for spirometry tests, oral corticosteroids, short-acting bronchodilators, and long-acting bronchodilators during the post-treatment period compared with the pre-treatment period (Table 2). There was a significant increase in the proportion of patients with evidence of oxygen therapy and emphysema during the post-treatment period compared with the pre-treatment period.
Treatment Characteristics
The mean (SD) duration that each patient was on the index therapy was 118.2 (110.0) days in the 12-month post-index period. Mean (SD) proportion of days covered (PDC) was 0.4 (0.3) during the 6-month post-index period and 0.3 (0.3) during the 12-month post-index period. Overall, 18% of patients were adherent (PDC ≥80%) during the first 6 months following index; during the 12-month post-treatment period, 11% of patients were adherent (PDC ≥80%) to the index therapy.
During the post-treatment period, there was a significant reduction in the use of short-acting β2-agonist (SABA) and SABA + short-acting muscarinic antagonist (SAMA) combination rescue therapies (Table 2).
COPD Exacerbations: Pre-Treatment versus Post-Treatment
There was a lower proportion of patients with ≥1 COPD exacerbation (moderate and/or severe) during the post-treatment period compared with the pre-treatment period (51% vs 57%, p<0.0001; Table 2). The proportion of patients with ≥1 moderate COPD exacerbation and ≥1 severe COPD exacerbation were both significantly lower during the post-treatment period versus the pre-treatment period.
Patients were 2.6 times more likely to have an exacerbation in the pre-treatment period versus the post-treatment period (OR: 2.63 [95% CI 2.21 to 3.13, p<0.0001]) (Table 3). With an increase in age, patients were less likely to have an exacerbation in the post-treatment period versus the pre-treatment period (OR: 0.98 [95% CI 0.97 to 0.99, p<0.0001]). Patients who were commercially insured were 0.27 times less likely to have an exacerbation post-treatment versus pre-treatment compared with Medicare enrolled patients (OR: 0.73 [95% CI 0.56 to 0.95, p=0.0170]). For every one unit increase in COPD severity score, patients were 0.05 times more likely to have an exacerbation post-treatment versus pre-treatment (OR: 1.05 [95% CI 1.04 to 1.06, p<0.0001]).
 |
Table 3 Proportion of Patients with COPD or Asthma Exacerbations – Multivariable Modeling |
Incidence of overall COPD exacerbations was 20% higher during the pre-treatment period versus the post-treatment period (incident rate [IR] 1.20 [95% CI 1.18 to 1.23, p<0.0001]) (Table 4). For each unit increase in patient age, there was a 1% decrease in the IR of exacerbation during the post-treatment period. For each unit increase in COPD severity score, there was a 2% increase in the IR of exacerbation during the post-treatment period.
 |
Table 4 Number of COPD or Asthma Exacerbations per Patient – Multivariable Modelinga |
Incidence of moderate COPD exacerbations was 27% higher during the pre-treatment period versus the post-treatment period (IR: 1.27 [95% CI 1.23 to 1.31, p<0.0001]) (Table 4). For each unit increase in age, there was a 2% decrease in the IR of moderate exacerbation post-treatment. For each unit increase in COPD severity score, there was a 2% increase in the IR of moderate exacerbation post-treatment.
Incidence of severe COPD exacerbations was 48% higher during the pre-treatment period versus the post-treatment period (IR: 1.48 [95% CI 1.35 to 1.62, p<0.0001]) (Table 4). For each unit increase in COPD severity score, there was a 2% increase in the IR of severe exacerbation post-treatment.
There was a 20% decrease in the IR for overall COPD exacerbations during the post-treatment period for commercially insured patients versus Medicare enrolled patients (IR: 0.80 [95% CI 0.68 to 0.95, p=0.0106]). The use of SABA or fixed-dose SABA + SAMA dual therapy during the pre-treatment period significantly increased the IR of overall COPD exacerbations during the post-treatment period by 23% (IR for SABA: 1.23 [95% CI 1.07 to 1.40], p=0.0032; IR for SABA + SAMA: 1.23 [95% CI 1.07 to 1.40], p=0.0035, respectively).
Asthma Exacerbations: Pre-Treatment versus Post-Treatment
There was a lower proportion of patients with ≥1 asthma exacerbation during the post-treatment period compared with the pre-treatment period (22% vs 32%, p<0.0001; Table 2).
Patients were 2.6 times more likely to have an exacerbation in the pre-treatment period versus the post-treatment period (OR: 2.61 [95% CI 2.15 to 3.17, p<0.0001]) (Table 3). With an increase in age, patients were less likely to have an exacerbation in the post-treatment period versus the pre-treatment period (OR: 0.98 [95% CI 0.97 to 0.99, p<0.0003]). For every one unit increase in COPD severity score, patients were 0.01 times more likely to have an exacerbation post-treatment versus pre-treatment (OR 1.01 [95% CI 1.00 to 1.02], p=0.0140). Patients who used ICS during the pre-treatment period were 0.27 times more likely to have an exacerbation in the post-treatment period versus patients with no ICS use pre-treatment (OR 1.27 [95% CI 1.01 to 1.60], p=0.0374).
Incidence of asthma exacerbations was 49% higher during the pre-treatment versus the post-treatment period (IR: 1.49 [95% CI 1.39 to 1.59, p<0.0001]) (Table 4). For each unit increase in patient age, there was a 2% decrease in the IR of exacerbation during the post-treatment period. For each unit increase in COPD severity score, there was a 1% increase in the IR of exacerbation during the post-treatment period.
HCRU and Costs: Pre-Treatment versus Post-Treatment
There were fewer patients with ≥1 all-cause office visit during the post-treatment period compared with the pre-treatment period (99.3% vs 99.7%; Table 5). Although there were numerically fewer patients with ≥1 inpatient admission and ≥1 emergency room visit during the post-treatment period versus the pre-treatment period, this did not reach statistical significance. There was a significant reduction in the proportion of patients with ≥1 COPD-related pharmacy claims during the post-treatment period versus pre-treatment (90.7% vs 96.2%, p<0.0001; Table 5). Conversely, there was a significant increase in the proportion of patients with ≥1 COPD-related outpatient visit, COPD-related office visit, and other outpatient visit during the post-treatment period compared with the pre-treatment period.
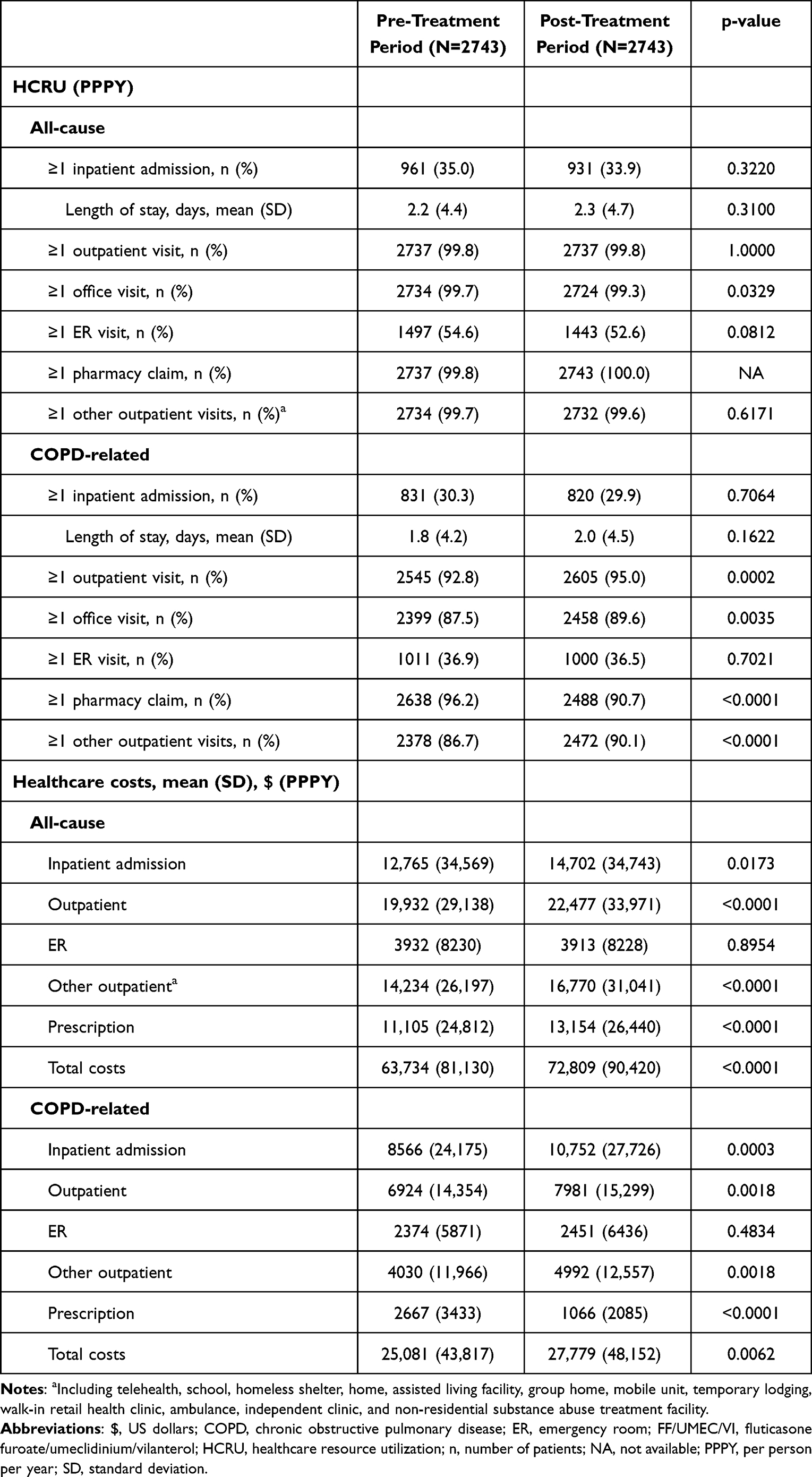 |
Table 5 HCRU and Healthcare Costs Post-FF/UMEC/VI Treatment versus Pre-Treatment |
Total all-cause healthcare costs were significantly higher during the post-treatment period versus the pre-treatment period ($72,809 vs $63,734, p<0.0001; Table 5). All-cause inpatient admission costs, outpatient costs, and prescription costs were higher post-treatment compared with pre-treatment (Table 5).
Similar results were seen for COPD-related costs (Table 5). Total COPD-related costs were significantly higher during the post-treatment period versus the pre-treatment period ($27,779 vs $25,081, p=0.0062). COPD-related prescription costs were significantly lower post-treatment versus pre-treatment ($1066 vs $2667, p<0.0001).
Discussion
The findings of this retrospective study provide important insights into the real-world clinical and economic burden and outcomes of patients with COPD and asthma using FF/UMEC/VI triple therapy in the US.
The proportion of patients with COPD exacerbations (including total, moderate, and severe) was significantly reduced during the 12-month period following the first FF/UMEC/VI prescription date. As demonstrated by the multivariate results, patients had higher odds for COPD-related exacerbation events prior to treatment with FF/UMEC/VI compared with after the first FF/UMEC/VI prescription. The observed reductions in exacerbations following FF/UMEC/VI are supportive of prior clinical data in which patients with COPD receiving FF/UMEC/VI via a single device demonstrated a lower rate of moderate or severe exacerbations compared with patients receiving dual therapy (FF/VI or UMEC/VI).8
To date, there have been a lack of real-world studies evaluating exacerbations and HCRU among patients with concurrent COPD and asthma. In this study, significantly fewer patients had ≥1 asthma exacerbation in the 12 months following FF/UMEC/VI initiation versus the 12 months prior to FF/UMEC/VI initiation, and patients had higher odds for asthma exacerbations prior to treatment with FF/UMEC/VI compared with after the first FF/UMEC/VI prescription.
The GOLD strategy document6 suggests that for patients with COPD and asthma, pharmacotherapy should primarily follow asthma guidelines (GINA).20 For these patients, the use of ICS is mandatory to lower the risk of future exacerbations.20 FF/UMEC/VI provides ICS and maximal bronchodilation (LABA + LAMA).7 ICS-containing regimens have previously been shown to be associated with an increased risk of pneumonia in patients with COPD.21 However, in the current study there was a significantly lower proportion of patients with pneumonia during the post-treatment period versus the pre-treatment period (20% vs 23%, p=0.0032). Although there was a significant increase in Charlson Comorbidity Index score post-treatment versus pre-treatment, we observed a significant decrease in COPD severity score, along with significant reductions in the number of claims for both short-acting and long-acting bronchodilators. The reduced number of claims for oral corticosteroids and SABA during the post-treatment period is indicative of improved symptom control and/or lung function following FF/UMEC/VI initiation. The results observed in this study are supportive of the use of triple therapy as per the GOLD and GINA guidelines.6,20
Importantly, improvements in exacerbation rates were seen even at the levels of adherence observed during this study. During the 12-month post-treatment period of the current study, 11% of patients were adherent (PDC ≥80%) to the index therapy. Adherence to COPD therapy is critical for achieving optimal clinical outcomes;22 however, observed adherence rates to inhaled therapies among patients with COPD are generally low. Non-adherence rates to COPD therapies between 22% and 93% were reported across 37 studies in a recent systematic review.23 The current GOLD strategy document includes recommendation that single inhalers may be more convenient and effective than multiple inhalers,6 and prior studies have demonstrated that patients receiving single-inhaler triple therapy have significantly better adherence and persistence compared with patients receiving triple therapy via multiple inhalers.24,25
While there were significant reductions in office visits for all-cause HCRU, and in pharmacy claims for COPD-related HCRU, during the 12-month period following the first FF/UMEC/VI prescription, the proportion of patients with ≥1 COPD-related outpatient visit or office visit increased during the same period. As patients were escalated to triple therapy, indicative of disease progression and/or an increase in symptoms, or the patient receiving an asthma diagnosis, which resulted in addition of an ICS, a rise in COPD-related HCRU may be expected. Patients may also have been referred to a specialist. Further to this, when a patient is prescribed a new medication, it is likely that their healthcare provider would like to monitor them to assess how they are responding to the therapy, which would result in further visits. Therefore, this increase in HCRU may not necessarily be due to worsening disease, but could be due to closer/more regular monitoring of patients. The observed decrease in exacerbations but increase in HCRU could also be due to the vulnerability of the patient population receiving FF/UMEC/VI (ie, moderate-to-severe COPD and high prevalence of cardiovascular disease, pulmonary complications, and other comorbidities).
All-cause and COPD-related healthcare costs increased during the 12-month period following the first FF/UMEC/VI prescription date, consistent with the increased HCRU observed during this time. As COPD is a progressive disease, it is possible that FF/UMEC/VI could lead to cost avoidance among patients with COPD and asthma (via reduction in the rate of moderate and severe exacerbations). Prior exacerbation is among the most prominent predictors of future COPD exacerbation,26,27 which is a key driver of the economic burden of the disease.2 It should be noted that the driver of all-cause healthcare cost appeared to be non-COPD-related, indicating that comorbidities, such as cardiovascular disease, chronic renal failure, and diabetes, are likely the cause of the significant increase in healthcare costs among this patient population. In the pre-treatment period, non-COPD-related costs were approximately $38,700 versus approximately $25,100 for COPD-related costs. Post-treatment, non-COPD-related costs were approximately $45,000 versus approximately $27,800 for COPD-related costs. The increase in COPD-related costs was much smaller than the increase in all-cause costs, likely due to improved clinical outcomes for COPD. Patients who were identified as needing further treatment for their COPD (ie, an escalation to triple therapy) may have also been identified for needing further care for other comorbid conditions, leading to an increase in all-cause healthcare costs. Significantly more patients had record of other comorbidities such as chronic renal failure, pulmonary vascular disease, and GERD during the post-treatment period compared with the pre-treatment period, which may have contributed to the increase in all-cause costs. Of note, specific asthma-related HCRU and costs were not captured in this study; however, this would be useful to examine in future studies. Also, although the cost-effectiveness of FF/UMEC/VI among patients with COPD has previously been demonstrated,9–13 given the more recent approval for FF/UMEC/VI in asthma, there are currently no relevant studies examining the cost-effectiveness of FF/UMEC/VI among patients with asthma. Future studies investigating the cost-benefit ratio of FF/UMEC/VI among patients with asthma and among patients with both COPD and asthma would be of value.
Limitations of this study include those often associated with database studies, including potential incorrect coding of diagnosis codes and missing information. Also, a pharmacy claim for a medication does not necessarily mean that the medication was taken by the patient as prescribed. In addition, the pre-post study design does not account for time-varying confounding factors, which could potentially change during the study period as the patients are acting as their own controls. The study design did not account for the fact that patients’ COPD would likely become more severe over time. Indicators of disease severity, eg, results from clinical/laboratory tests conducted by physicians to monitor patients’ COPD and/or asthma, were not available within the claims data. Finally, patients switching to alternate medication during the study period was not captured in the analysis.
Conclusion
The current study demonstrated that FF/UMEC/VI is able to reduce exacerbations among patients with COPD and asthma in a real-world setting. Significantly fewer patients experienced ≥1 exacerbation (COPD or asthma) in the 12 months following first FF/UMEC/VI prescription versus the 12 months prior to FF/UMEC/VI initiation. Although fewer patients had ≥1 all-cause office visit and ≥1 COPD-related pharmacy claim following FF/UMEC/VI initiation compared with before FF/UMEC/VI initiation, there were significantly more patients with ≥1 COPD-related office visit following FF/UMEC/VI initiation. All-cause and COPD-related healthcare costs were both significantly higher during the 12 months following FF/UMEC/VI initiation compared with the 12 months prior to initiation. The patients with COPD in this study have a high disease burden and high medical costs, resulting from their asthma, as well as other debilitating comorbidities, such as cardiovascular disease, chronic renal failure, GERD, and diabetes. These non-COPD conditions appear to be the driver of the increased healthcare costs observed following FF/UMEC/VI initiation, rather than the management of COPD exacerbations. Future studies examining the cost-benefit ratio of FF/UMEC/VI specifically among patients with both COPD and asthma would be of value. In addition, further real-world analysis is required to better understand current COPD management among patients with asthma and how it may be improved to reduce the ongoing economic burden and improve clinical outcomes.
Abbreviations
$, US dollars; CCI, Charlson Comorbidity Index; CI, confidence interval; COPD, chronic obstructive pulmonary disease; ER, emergency room; FDC, fixed-dose combination; FF/UMEC/VI, fluticasone furoate/umeclidinium/vilanterol; GERD, gastroesophageal reflux disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; HCRU, healthcare resource utilization; ICD-(CM), International Classification of Diseases-(Clinical Modification); ICS, inhaled corticosteroid; IR, incident rate; LABA, long-acting β2-agonist; LABD, long-acting bronchodilator; LAMA, long-acting muscarinic antagonist; MITT, multiple-inhaler triple therapy; NA, not available; NDC, National Drug Code; OR, odds ratio; PDC, proportion of days covered; PPPY, per person per year; SABA, short-acting β2-agonist; SAMA, short-acting muscarinic antagonist; SD, standard deviation; US, United States.
Data Sharing Statement
The data analyzed in this manuscript are contained in a database owned by Optum Clinformatics®, and therefore are not publicly available. Access to the data may be available on license from Optum (https://www.optum.com/business/life-sciences.html).
Ethics Approval and Informed Consent
As this was an analysis of claims data, institutional review board (IRB) approval was not required. Per Title 45 of CFR, Part 46 (www.hhs.gov/ohrp/humansubjects/guidance/45cfr46.html#46.101), the administrative claims data analysis of our study was exempt from the IRB review as it was a retrospective analysis of existing data (hence no patient intervention or interaction), and no patient-identifiable information was included in the claims dataset.
Acknowledgments
The Authors would like to thank Dr Matthew Mintz for his involvement in reviewing and providing feedback on the first draft of the manuscript. Editorial support (in the form of writing assistance, including preparation of the draft manuscript under the direction and guidance of the authors, collating and incorporating authors’ comments for each draft, assembling tables and figures, grammatical editing, and referencing) was provided by Rebecca Cunningham of Apollo, OPEN Health Communications, and was funded by GSK.
Author Contributions
All authors made a significant contribution to the work reported, whether that was in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the manuscript; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by GSK (study number 214321). GSK-affiliated authors were involved in study conception and design, data analysis, data interpretation, and the decision to submit the article for publication. GSK funded the article processing charges and open access fee.
Disclosure
SV was an employee of STATinMED at the time of the study; STATinMED received funds from GSK to conduct the study but not for manuscript development. RP and EI are employees of and/or hold stocks/shares in GSK.
References
1. Centers for Disease Control and Prevention Deaths: leading causes for 2019; 2021. Available from: https://www.cdc.gov/nchs/nvss/leading-causes-of-death.htm#publications.
2. Iheanacho I, Zhang S, King D, Rizzo M, Ismaila AS. Economic burden of chronic obstructive pulmonary disease (COPD): a systematic literature review. Int J Chron Obstruct Pulmon Dis. 2020;15:439–460. doi:10.2147/COPD.S234942
3. Lareau S, Moseson E, Slatore CG. Exacerbation of COPD. Am J Respir Crit Care Med. 2018;198(11):P21–P22. doi:10.1164/rccm.19811P21
4. Halpin DM, Miravitlles M, Metzdorf N, Celli B. Impact and prevention of severe exacerbations of COPD: a review of the evidence. Int J Chron Obstruct Pulmon Dis. 2017;12:2891–2908. doi:10.2147/COPD.S139470
5. Hoogendoorn M, Hoogenveen RT, Rutten-van Mölken MP, Vestbo J, Feenstra TL. Case fatality of COPD exacerbations: a meta-analysis and statistical modelling approach. Eur Respir J. 2011;37(3):508–515. doi:10.1183/09031936.00043710
6. Global Initiative for Chronic Obstructive Lung Disease Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: 2023 report; 2023. Available from: https://goldcopd.org/2023-gold-report-2/.
7. Trelegy Ellipta. North Carolina: GlaxoSmithKline; 2020.
8. Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378(18):1671–1680. doi:10.1056/NEJMoa1713901
9. Ismaila AS, Risebrough N, Schroeder M, et al. Cost-effectiveness of once-daily single-inhaler triple therapy in COPD: the IMPACT trial. Int J Chron Obstruct Pulmon Dis. 2019;14:2681–2695. doi:10.2147/COPD.S216072
10. Schroeder M, Benjamin N, Atienza L, et al. Cost-effectiveness analysis of a once-daily single-inhaler triple therapy for patients with chronic obstructive pulmonary disease (COPD) using the FULFIL trial: a Spanish perspective. Int J Chron Obstruct Pulmon Dis. 2020;15:1621–1632. doi:10.2147/COPD.S240556
11. Schroeder M, Shah D, Risebrough N, et al. Cost-effectiveness analysis of a single-inhaler triple therapy for patients with advanced chronic obstructive pulmonary disease (COPD) using the FULFIL trial: a UK perspective. Respir Med X. 2019;1:100008. doi:10.1016/j.yrmex.2019.100008
12. Fenwick E, Martin A, Schroeder M, et al. Cost-effectiveness analysis of a single-inhaler triple therapy for COPD in the UK. ERJ Open Res. 2021;7(1):00480–2020. doi:10.1183/23120541.00480-2020
13. Halpin DMG, Kendall R, Shukla S, et al. Cost-effectiveness of single- versus multiple-inhaler triple therapy in a UK COPD population: the INTREPID trial. Int J Chron Obstruct Pulmon Dis. 2022;17:2745–2755. doi:10.2147/COPD.S370577
14. Negewo NA, Gibson PG, McDonald VM. COPD and its comorbidities: impact, measurement and mechanisms. Respirology. 2015;20(8):1160–1171. doi:10.1111/resp.12642
15. Silva GE, Sherrill DL, Guerra S, Barbee RA. Asthma as a risk factor for COPD in a longitudinal study. Chest. 2004;126(1):59–65. doi:10.1378/chest.126.1.59
16. Uchida A, Sakaue K, Inoue H. Epidemiology of asthma-chronic obstructive pulmonary disease overlap (ACO). Allergol Int. 2018;67(2):165–171. doi:10.1016/j.alit.2018.02.002
17. Barrecheguren M, Pinto L, Mostafavi-Pour-Manshadi SM, et al. Identification and definition of asthma-COPD overlap: the CanCOLD study. Respirology. 2020;25(8):836–849. doi:10.1111/resp.13780
18. Andersén H, Lampela P, Nevanlinna A, Säynäjäkangas O, Keistinen T. High hospital burden in overlap syndrome of asthma and COPD. Clin Respir J. 2013;7(4):342–346. doi:10.1111/crj.12013
19. Kendzerska T, Sadatsafavi M, Aaron SD, et al. Concurrent physician-diagnosed asthma and chronic obstructive pulmonary disease: a population study of prevalence, incidence and mortality. PLoS One. 2017;12(3):e0173830. doi:10.1371/journal.pone.0173830
20. Global Initiative for Asthma Global strategy for asthma management and prevention; 2022. Available from: https://ginasthma.org/wp-content/uploads/2022/07/GINA-Main-Report-2022-FINAL-22-07-01-WMS.pdf.
21. Nici L, Mammen MJ, Charbek E, et al. Pharmacologic management of chronic obstructive pulmonary disease. An official American Thoracic Society clinical practice guideline. Am J Respir Crit Care Med. 2020;201(9):e56–e69. doi:10.1164/rccm.202003-0625ST
22. Vestbo J, Anderson JA, Calverley PM, et al. Adherence to inhaled therapy, mortality and hospital admission in COPD. Thorax. 2009;64(11):939–943. doi:10.1136/thx.2009.113662
23. Bhattarai B, Walpola R, Mey A, Anoopkumar-Dukie S, Khan S. Barriers and strategies for improving medication adherence among people living with COPD: a systematic review. Respir Care. 2020;65(11):1738–1750. doi:10.4187/respcare.07355
24. Mannino D, Bogart M, Wu B, et al. Adherence and persistence to once-daily single-inhaler versus multiple-inhaler triple therapy among patients with chronic obstructive pulmonary disease in the USA: a real-world study. Respir Med. 2022;197:106807. doi:10.1016/j.rmed.2022.106807
25. Halpin DMG, Rothnie KJ, Banks V, et al. Comparative adherence and persistence of single- and multiple-inhaler triple therapies among patients with chronic obstructive pulmonary disease in an English real-world primary care setting. Int J Chron Obstruct Pulmon Dis. 2022;17:2417–2429. doi:10.2147/COPD.S370540
26. Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. doi:10.1056/NEJMoa0909883
27. Rothnie KJ, Müllerová H, Smeeth L, Quint JK. Natural history of chronic obstructive pulmonary disease exacerbations in a general practice-based population with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198(4):464–471. doi:10.1164/rccm.201710-2029OC
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.