")
Back to Journals » Patient Preference and Adherence » Volume 18
Preferences for Physical Examination Service in Community Health Service Center in China: A Discrete Choice Experiment
Authors Sun H, Li F, Xu Y, Qi Q, Du Y
Received 13 October 2023
Accepted for publication 22 December 2023
Published 6 January 2024 Volume 2024:18 Pages 39—51
DOI https://doi.org/10.2147/PPA.S440896
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Huajun Sun,1 Fangshi Li,1 Yaxuan Xu,2 Qi Qi,3 Yue Du1
1School of Public Health, Tianjin Medical University, Tianjin, People’s Republic of China; 2School of Nursing, Tianjin Medical University, Tianjin, People’s Republic of China; 3School of Optometry, Tianjin Medical University, Tianjin, People’s Republic of China
Correspondence: Yue Du, School of Public Health, Tianjin Medical University, 22# Qixiangtai Road, Heping District, Tianjin, 300070, People’s Republic of China, Tel +86 18920015698, Fax +86 02283336597, Email [email protected]
Objective: Physical examination services play a crucial role in the early detection of diseases, improving the effectiveness of treatment. However, the current physical examination services provided by community health service centers are limited. The objective of this study was to investigate the aspects of physical examination services that are most valued by residents.
Methods: Identify and develop attributes and levels through literature research and expert group interviews. A discrete choice experiment was designed. The main effects design gives rise to 16 choice sets. The 16 choice sets were grouped into 2 blocks, and respondents were randomly assigned to one of the blocks. In each choice set, respondents were asked to choose from two alternatives with an opt-out option. In 2023, the discrete choice experiment was administered in several community health service centers within a China population sample. A mixed logit and a latent class analysis were conducted.
Results: Participants (n = 399) preferred to receive health advice service. The services provided by the basic team with clinical experts are preferred over those provided solely by the basic team. The results indicated a preference for a participant to be serviced by face-to-face or telephone compared with WeChat. Low cost is also preferred. As participants grow older, their preference for face-to-face or telephone-based services increased. As participants’ service demand increase, participants more preferred to receive interpretation of physical examination report and follow-up of important abnormal results, participants more preferred to be serviced by basic team with clinical experts or basic team with health manager etc.
Conclusion: We should improve the construction of the service team, optimize the service mode, expand the scope of examination services, reduce the cost of examination services, and meet the needs of residents for physical examination services. More attention should be paid to the needs of elderly and rural residents.
Keywords: discrete choice experiment, physical examination, community health service, preference
Introduction
Since 2009, China has implemented the National Basic Public Health Service Project, which places primary medical institutions such as community health service centers at the forefront of managing the health of key population.1 However, the services provided by community health service centers in China lack variety and require improvement.2,3 Physical examination is one of the main contents of health management for key population. In Tianjin, people aged 60 and above, as well as those aged 35 and above with hypertension or diabetes, are eligible for free physical examinations at the community health service center. Regular examination can prevent the onset of diseases4 and ultimately improve their overall quality of life.5
Physical examinations can be divided into three service stages: pre-examination services, examination services, and post-examination services. Examination services usually include body check-up, blood routine, urine routine, electrocardiogram, ultrasound, etc. Follow-up services of physical examination typically include the interpretation of physical examination reports, follow-up on important abnormal results, and review of important abnormal findings. However, a Chinese study shows that only about 40% residents undergo regular examinations.6 Common factors that interfere with residents’ physical examination perception and planning include health self-assessment, economic reasons, occupational status, education, exercise status and time.7 Moreover, the provision of physical examination services itself can heighten the health awareness of participants.
Physical examinations and follow-up on important abnormal results play an integral role in secondary prevention, they can also achieve early and correct detection and diagnosis of diseases, and improve the effectiveness of treatment. Following up on the important abnormal results ensures that their health problems are handled in a timely and standardized manner. Review of important abnormal results can help understand the changes in the health status of the individuals, making the diagnosis more clear. Referral services can enable individuals with abnormal physical examination results to receive faster and more accurate diagnosis and treatment. The effectiveness of physical examination services is usually measured by their diagnostic accuracy among key populations. However, previous studies on the health management of key population are primarily focused on the analysis of service utilization rates and satisfaction rates,8,9 with few reports on the detection of abnormal results during physical examinations.
The attitudes of residents towards physical examination services vary widely, and residents’ perceptions can significantly affect the implementation of physical examination services. For example, time constraints have been identified as a barrier in delivering various public health services consistently.10 Hu Q et al find that waiting time is a critical factor influencing patient preferences, and longer waiting time can easily trigger negative emotions among patients.11 There fore, it is imperative to optimize the medical examination process, minimize waiting time, and mitigate negative emotions among residents. By investigating and addressing residents’ preferences for physical examination services, the services can be improved and residents’ needs be better satisfied, which, in turn, can facilitate the smooth implementation of health examination services and improve overall service effectiveness and satisfaction levels.
Discrete choice experiments (DCEs) are widely used in health economics fields, serving various purposes such as measuring health service demand preferences.12–14 For example, Lieberz D et al examined the physical performance measures of elderly people and used discrete choice experiment to determine their preferences for relevant nursing modes.15 The discrete choice experiment was also used to evaluate the preference of sharing electronic health records and genetic information.16 At present, while there is a growing body of research focusing on health plans and using discrete choice experiments to determine residents’ preference for the service contents provided for health plans.16 There is a gap in the literature regarding the follow-up service of physical examination using discrete choice experiments.
This study uses the discrete choice experiment method to analyze residents’ preferences for physical examination services and identify the factors that influence their utilization. The aim is to provide insights for optimizing the physical examination services in community health service centers.
Methods
Identification and Development of Attributes and Levels
Relevant attributes and levels were retrieved from the literature review and interviews with an expert group. Relevant publications from databases such as Web of Science, PubMed, and CNKI were searched, using keywords such as “physical examination” “physical screening” “health examination” “post physical examination service” and “follow-up service”. Research specifically on post-physical examination services is limited, so literature on preventive care was also included. The expert group consists of experts in health examinations, health management, public health and other areas. Twelve attributes were identified from the literature, and 3 attributes were identified from expert group discussions, with 2 attribute being duplicate. A total of 13 attributes were identified. The list of 13 attributes and their levels is presented in Supplementary Table 1. The expert group votes to select the attributes they consider to be the most important, and the top 6 attributes with the highest number of votes are chosen ultimately. The selection of the attributes was informed by principal services, additional services, service team, service mode, wait time and cost. An list of attributes and levels was presented to and reviewed by experts at Tianjin Basic Public Health Service Quality Control Center and experts at Tianjin Medical University. The list of 6 attributes and their levels is presented in Table 1.
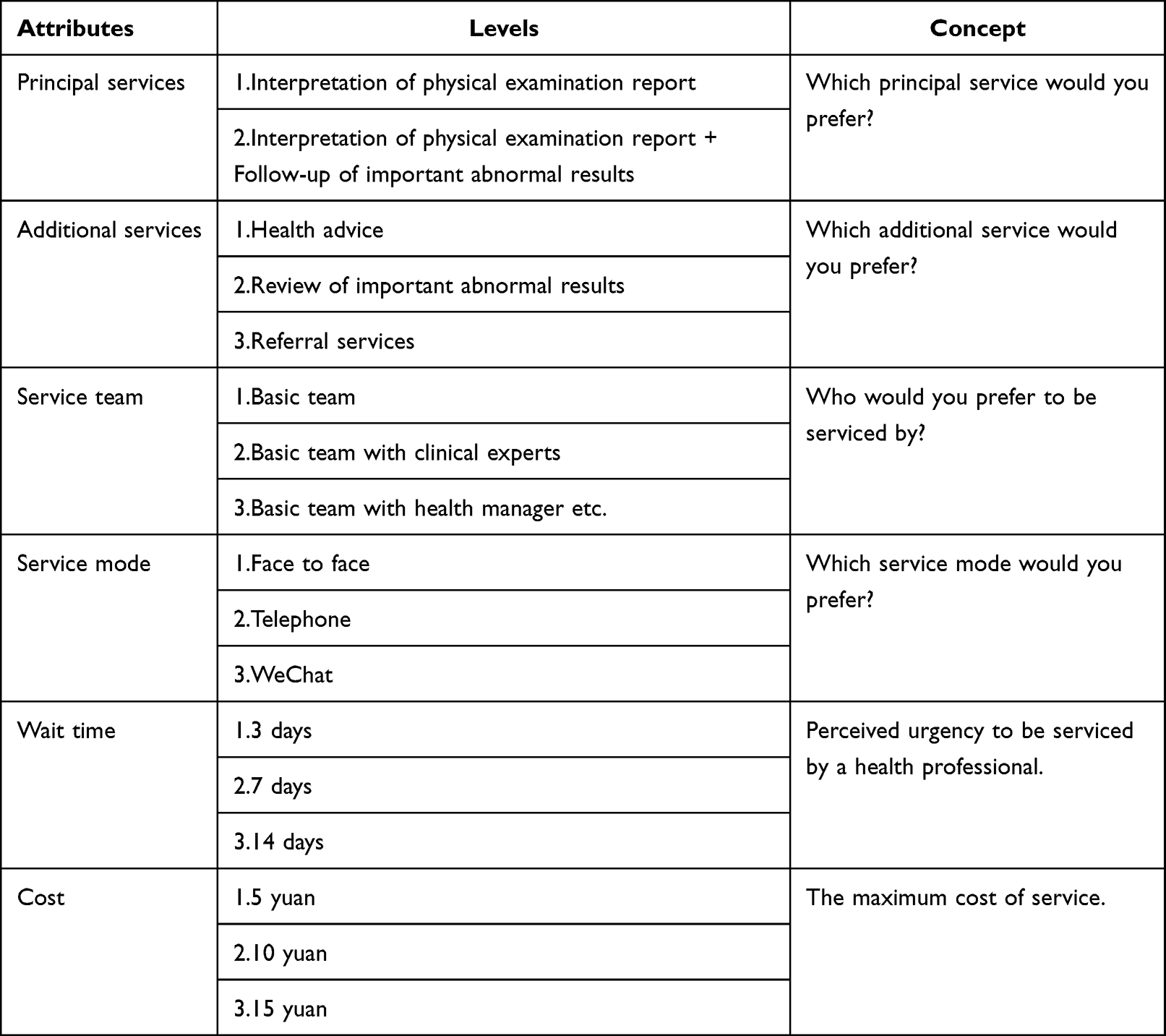 |
Table 1 Finalized Attributes and Levels |
The interpretation of physical examination report is one of the mandatory services that community health service centers are required to provide in Tianjin. Follow-up of important abnormal results is a recently planned service that will soon be made mandatory for community health service centers. To make the discrete choice experiment more instructive in improving Tianjin’s physical examination services policy, these two service contents have been set as the main content. Although health advice, review of important abnormal results and referral services are important components of physical examination services, their implementation varies in Tianjin. Regrettably, not all people undergoing physical examinations at community health service centers are able to access these services, so we classify them as additional services. The level of each services in the principal service and additional service are differentiated based on whether they provide relevant services.
Development of Choice Experiment
The main effects design gives rise to 16 choice sets and the design had a D-efficiency of 81.1%. Stata version 16 was used to generate the design. The 16 choice sets were grouped into 2 blocks of 8 choice sets, and respondents were randomly assigned to one of the blocks. The opt-out option was provided after the forced choice between the 2 alternatives to identify those who would rather not participate in a service program all together. A repeated choice set with the first choice set was added to each block, so as to test whether the respondents chose the same option. Questionnaires with inconsistent answers will be excluded. Each block contains nine choice sets.
Cognitive Interview and Pilot Study
After the development of choice experiment, cognitive interviews were used to test respondents’ comprehension of DCE attributes.17,18 Cognitive interviews are commonly used in developing DCE in health.19–21 The interviews followed a predetermined schedule and evaluated participant’s comprehension based on various components, including comprehension of the attribute items, the use of that information in decision-making, and the articulation of their responses.22 Upon completing all choice sets, participants were also asked whether there were any additional attributes that might affect their choices.
Participants for the cognitive interviews were recruited from community health service centers in Tianjin, China. Eight participants, aged 35 years or older, who had undergone at least one physical examination within the past 5 years, were interviewed. Difficulties encountered during the experiments were attributed to the respondent’s low educational levels of and lack of autonomy. As a result, adjustments were made throughout the interview process. More graphical content has been added to the questionnaire to enhance the clarity. The example of questionnaire in Supplementary Box 1 and Supplementary Figure 1. After adding graphics, all participants reported being able to understand all the attributes and levels of the discrete choice experiment. Their descriptions suggest that there is a shared understanding of the content among different participants. Furthermore, all cognitive interview participants reported that they did not consider other attributes to be important in their decision-making process and found the presented attributes to be sufficiently comprehensive. Therefore, no changes to the attributes and levels are necessary based on their feedback.
A pilot study was conducted with a general population sample (n = 144) to ensure that the experiment performed as intended. Statistical analysis was conducted using mixed logit (MIXL) model. Because results were consistent with expectations, no changes were made to the DCE.
Recruitment and Data Collection
The study was utilized a face-to-face survey conducted by trained and qualified investigators. These investigators guided participant through the questionnaire, explained relevant questions, and recorded their answers. Participants were eligible for the study if they aged 35 or older who resided in Tianjin and had undergone at least one physical examination in the past 5 years. The inclusion criteria for the survey participants are essentially aligned with the target population for physical examination services provided by the community health service center. The survey was conducted in several community health service centers in Tianjin, China. The survey location is consistent with the location where the service is conducted. Ethical approval for the study was obtained from Tianjin Fourth Central Hospital (Ethical NO. SZXLL-2023-021). The study adhered to the Declaration of Helsinki. Informed consent was obtained from all participants.
Analysis
Descriptive statistics were used to describe the demographic characteristics of the sample. MIXL and latent class (lclogit) models were used to analyze the choice experiment responses. Willingness-to-pay measures were also calculated. The analysis was conducted using Stata version 16.
Mixed Logit
The MIXL model relates the probability of choosing an alternative within a choice set to the attribute levels used to describe each option and also allows for the specification of one or more parameters as randomly distributed.23 In addition, the MIXL includes a random error term that adjusts for variations in an individual’s preferences. The MIXL model estimates a set of mean preference weights and a set of standard deviations of effects across the sample. Interpretation of mean preference weights is made in relation to a base level. The standard deviations indicate variability in the mean preference weights; larger (smaller) values indicate greater (smaller) variability.24
By establishing interaction terms between DCE attributes and demographic characteristics of the participants, the participants’ choice of service set was taken as dependent variable, interaction terms and service attribute level were taken into logit model as independent variable, to explore the preference heterogeneity of different demographic groups. The first step is to interact with individual social demographics and various attributes separately and screen out meaningful interaction items among them. The second step is to incorporate all significant interactions between social demographics and various attributes into the model for reanalysis, as shown in Table 4. Wait time and cost did not interact with social demographics.
 |
Table 2 Demographic Characteristics |
 |
Table 3 Mixed Logit Results. (Main Effect) |
 |
Table 4 Mixed Logit Results. (Main Effect and Interaction Effect) |
In both the MIXL and latent class (lclogit) models, all attributes except cost and waiting time were dummy coded (categorical), with one level (the base level) being omitted. Cost and waiting time were specified as continuous variables to facilitate estimation of willingness to pay.
Cost Equivalence Measures
On the basis of the MIXL estimates, 2 cost equivalence measures using the cost and wait time attributes (and associated confidence intervals) were calculated using the “wtp” command: (1) willingness to pay (WTP) using the cost attribute and (2) WTW using the waiting time attribute. Waiting time and cost were entered in the model as continuous, and the linear specification was tested. Interpretation of estimates for each attribute level is made in comparison with the base case.
Lclogit Model
In addition to the MIXL model, lclogit models can further explore preference heterogeneity. The model assumes that classes of respondents exist within the sample, and the preference weights within each class are identical but are also systematically different from preference weights in other classes.24 Within each class, preference weights are estimated using a conditional logit model.24 A user-written Stata module,25 lclogit, was used to conduct this analysis. Demographics of each class were tabulated using by class: tabulate in Stata after model estimation.
The optimal number of lclogit models was chosen by Bayesian information criterion, conditional Akaike information criterion, the percentage of the number of minimum class, model fit and the rationality of the results. A 3-class model was selected to explore class membership. Some class membership variables were selected and included in the lclogit model: gender (male vs female), home of residence (urban vs rural), frequency of physical examination (every year vs not every year), age, education, family income, health state, service demand. Age, education, family income, health state and service demand are continuous variables. Education is calculated by converting the highest academic qualification into years of education. Health status and service needs were self-rated on a scale of 1 to 5, with higher scores indicating greater health or service needs.
Results
Description of the Study Population
A total of 450 participants started the survey. Of these, 27 did not meet inclusion criteria and 24 failed the consistency test. This resulted in a sample of 399 completed surveys. Only respondents (n = 399) who completed all choice sets were included in the analysis. Demographic characteristics of the sample are presented in Table 2. Our participants were generally older, less educated and had lower family incomes. Most of the respondents think they are relatively healthy, and their service demand is high. Most of the respondents take the physical examination every year. Due to the fact that the city has not disclosed the basic characteristics of the population who actually receive health examination services at community health service centers, but considering some high-income individuals will purchase higher quality services on their own instead of receiving services at community health service centers, we believe that the basic characteristics of the survey subjects are similar to those of the population receiving physical examination services at community health service centers. Notably, 62% of the sample never opted out of their chosen service program. Most respondents (89%) chose the opt-out in 3 or fewer of the choice sets they saw in the DCE. Only 30 respondents (7%) always chose the opt-out.
MIXL Model
Table 3 presents the main effect results of the MIXL. Participants more preferred to receive health advice service. The services of the basic team with clinical experts is preferred to those of the basic team. The results also indicate a preference for a participant to be serviced by face-to-face or telephone compared with WeChat. Low cost is also preferred. The magnitude of each standard deviation (for 7 attribute levels) is also statistically significant, indicating that variability in individual participants preferences exists.24
Table 4 presents the main effect and interaction effect results of the MIXL. As participants get older, participants more preferred to be serviced by face to face or telephone. As participants’ service demand increase, participants more preferred to receive interpretation of physical examination report and follow-up of important abnormal results. As participants’ service demand increase, participants more preferred to be serviced by basic team with clinical experts or basic team with health manager etc.
WTP and WTW
Because WTW or WTP was the wait time or cost to be serviced, it can be more readily interpreted as the measures of strength of preference for the service. As a first measure of willingness to pay, the cost attribute was used to calculate a WTP measure. As a secondary measure of willingness to pay, the attribute for waiting time was used to estimate a WTW.
The results that are presented in Figure 1 show that respondents place a high value on 3 aspects of a service program: additional services, service team and service mode. WTP for service mode is the highest, followed by WTP for service by the basic team with clinical experts and WTP for health advice service. WTP for health advice service was ұ9.59 compared with referral services. Service by the basic team with clinical experts was valued at ұ28.88 compared with the basic team. WTP for servicing by face to face was ұ43.47 and servicing by telephone was ұ45.54 compared with WeChat (base level). Other variables were not significant.
 |
Figure 1 WTP for physical examination service. Color reproduction on the Web and in print. |
Lclogit Analysis
With a 3-class model, 58.0% fall in class 1, 19.5% fall in class 2 and 22.5% fall in class 3. Class 3 prefer interpretation of physical examination report and follow-up of important abnormal results. Class 1 and Class 3 prefer health advice. Class 1 prefer review of important abnormal results. Class 1 and Class 3 prefer to be serviced by basic team with clinical experts. Class 3 prefer to be serviced by basic team with health manager, etc. Class 2 and Class 3 prefer to be serviced by face to face. Class 1 and Class 3 prefer to be serviced by telephone. Class 3 prefer low cost. The results showed that age, home of residence and health state significantly predicted class membership. Compared with class 3, class 1 and class 2 respondents have higher proportions of those who lived in urban. Compared with class 3, class 1 respondents were more young and more healthy. Table 5 presents the results of the lclogit model.
 |
Table 5 Latent Class Logit Results |
Due to the face-to-face level of the service mode attribute coefficients are large, we did further explored. A 2-class latent class model was used where Class 1 is used to represent the utility maximising data generation process and Class 2 predicts service mode by restricting all attributes to be zero except for service mode.26 In Class 2, the coefficient of face-to-face is 6.264 (P<0.01), so we thought it may be the dominant decision-making behaviour.
Discussion
The study found that participants did not exhibit significant preference for “Interpretation of physical examination report + Follow-up of important abnormal results”, which may indicate that community health service center could encounter low compliance issues when implementing related services in Tianjin in the future. In contrast, participants expressed a preference for health advice services, possibly due to the fact that these services can provide answers for their health queries and alleviate their discomfort. When additional services are converted from referral services to health advice services, residents are willing to pay an additional ¥ 9.59 for this transition.
Compared to basic teams, the services offered by basic teams with clinical experts are preferred, as residents have more trust in doctors from high-level hospitals and their technical expertise. When the service team transitions from basic team to basic team with clinical experts, residents are willing to pay an additional ¥ 28.88. This result is in line with previous studies. People often value doctors’ professionalism when choosing healthcare providers.27 It is believed that the service provided by doctors can be more professional.28 Jiang MZ et al showed that people are most willing to pay for the service that includes experts, and it also reflects the public is paying more attention to the quality of services.29
Low cost is also preferred, as supported by previous research. The results also show that the cost has a significant impact on the choice of medical services, especially among the elderly and low-income populations who tend to be more sensitive to the affordability of healthcare options. These individuals are more likely to prioritize cost considerations when making decisions about their medical care.30,31
As participants’ service demands increase, there is a growing preference for receiving interpretations of physical examination reports and follow-up on important abnormal results, which reflects the alignment of the different service offerings with the diverse needs of residents. In addition, as participants’ service demands grow, participants prefer to be serviced by basic teams with clinical experts or health managers, etc. This preference stems from the belief that high-quality service teams usually mean high service quality, aligning with the high expectation of residents.
As participants’ age increases, their preference for face-to-face or telephone services becomes stronger. Aging is often associated with declining health, and as participants’ requirements for the quality of health services increase, face-to-face or telephone services are more likely to improve the efficiency of doctor-patient communication, thereby facilitating the high-quality health services. Residents are willing to pay an additional ¥43.47 or ¥45.54 when the service mode switches from WeChat to face-to-face or telephone services. In latent class logit results, the coefficient values for face-to-face or telephone services in Class 2 and Class 3 are greater than those in Class 1, which is also related to the fact that the age of Class 2 and Class 3 is older than that of Class 1. The coefficient value in Class 3 is greater than that in Class 2, which may be due to the fact that Class 3 is mainly composed of rural residents who face greater social disadvantage than urban residents in Class 2, resulting in a stronger demand for high-quality services.
Class 1 is middle-aged urban residents who are relatively healthy and wish to receive more high-quality health services without disturbance. Therefore, they prefer physical examination service provided by basic teams with clinical experts and by telephone. This conclusion is consistent with previous studies. The research shows that urban participants tend to pay more attention to follow-up services by telephone11 due to their busy work schedules and limited time for face-to-face communication. Telephone service can effectively meet their needs by allowing them to address their requirements during fragmented or limited time periods. Class 3 is rural residents who have a preference for almost all services and levels that benefit them, which may be related to their relaxed life pace and the ability to receive more services. However, low education levels among rural residents may pose challenges in understanding and accepting appropriate combination of personalized services.32 This serves as a reminder that different service sets should be implemented for different service recipients. Furthermore, we should optimize the solution based on the specific needs of these recipients. By tailoring services to meet the unique requirements and preferences of each population, we can improve overall satisfaction and effectiveness of service delivery.
This study also has some limitations. The participants of this study are all from Tianjin, China. Whether the results of this study are applicable to other countries remains to be further studied and more research is required to validate our conclusions. In addition, the results of this study may be influenced by dominant decision-making behavior, and relevant issues should be noted in future related research.
Conclusion
We should improve the construction of the service team, optimize the service mode, expand the scope of examination services, reduce the cost of examination services, and meet the needs of residents for medical examination services. Personalized physical examination services should be provided for specific population groups, and more attention should be paid to the needs of elderly and rural residents for their physical examination services.
Acknowledgment
The authors wishes to express their gratitude to the journal editors and the anonymous peer reviewer whose comments were critical to the development of this article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Foundation of Philosophy and Social Sciences [grant numbers 19BGL247]. The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. You LL, Liu YL. National Essential Public Health Services Programs over the Past Decade Research Report One: significance and experiences of implementing National Essential Public Health Services Programs[J]. Chin General Practice. 2022;25(26):3203–3208.
2. Du M, Li P, Tang L, et al. Cognition, attitude, practice toward health checkup and associated factors among urban residents in southwest China, Sichuan province, 2022: a community-based study. Z Gesundh Wiss. 2023;18:1–12.
3. Zhang Y, Su D, Chen Y, et al. Effect of socioeconomic status on the physical and mental health of the elderly: the mediating effect of social participation. BMC Public Health. 2022;22(1):605. doi:10.1186/s12889-022-13062-7
4. Shimizu H, Shimada N, Otahara Y, et al. Relationship between low evaluation by recipients under 40 years old of health interviews by occupational health nurses and deterioration in health checkup results over one year. Keio J Med. 2008;57(2):90–98. doi:10.2302/kjm.57.90
5. Fang EF, Xie C, Schenkel JA, et al. A research agenda for ageing in China in the 21st century (2nd edition): focusing on basic and translational research, long-term care, policy and social networks. Ageing Res Rev. 2020;64:101174. doi:10.1016/j.arr.2020.101174
6. Chen J, Wu Z, Liu Y, et al. Prevalence, Association Relation, and Dynamic Evolution Analysis of Critical Values in Health Checkup in China: a Retrospective Study. Front Public Health. 2021;9:630356. doi:10.3389/fpubh.2021.630356
7. Kyoto-Kameoka study group, Yamaguchi M, Yoshida T, Yamada Y, et al. Sociodemographic and physical predictors of non-participation in community based physical checkup among older neighbors: a case-control study from the Kyoto-Kameoka longitudinal study, Japan. BMC Public Health. 2018;18(1):568. doi:10.1186/s12889-018-5426-5
8. Murphy SME, Hough DE, Sylvia ML, et al. Key Design Considerations When Calculating Cost Savings for Population Health Management Programs in an Observational Setting. Health Serv Res. 2018;53 Suppl 1(Suppl Suppl 1):3107–3124. doi:10.1111/1475-6773.12832
9. Abraham M, Lim MJ, Tan WS, et al. Global Trends Towards Population Health Management and Key Lessons and Initiatives in the Singapore Context. Int J Integr Care. 2022;22(3):19. doi:10.5334/ijic.7016
10. Eades CE, Ferguson JS, O’Carroll RE. Public health in community pharmacy: a systematic review of pharmacist and consumer views. BMC Public Health. 2011;11(1):582. doi:10.1186/1471-2458-11-582
11. Hu Q, Hu H, Hu M, et al. Patient Preferences For Specialty Pharmacy Services: a Stated Preference Discrete-Choice Experiment in China. Front Public Health. 2020;8:597389. doi:10.3389/fpubh.2020.597389
12. Ryan M. Using conjoint analysis to take account of patient preferences and go beyond health outcomes: an application to in vitro fertilisation. Soc Sci Med. 1999;48(4):535–546. doi:10.1016/S0277-9536(98)00374-8
13. Clark MD, Determann D, Petrou S, et al. Discrete choice experiments in health economics: a review of the literature. Pharmacoeconomics. 2014;32(9):883–902. doi:10.1007/s40273-014-0170-x
14. Soekhai V, de Bekker-Grob EW, Ellis AR, et al. Discrete Choice Experiments in Health Economics: past, Present and Future. Pharmacoeconomics. 2019;37(2):201–226. doi:10.1007/s40273-018-0734-2
15. Lieberz D, Borgeson H, Dobson S, et al. A Physical Therapy Mobility Checkup for Older Adults: feasibility and Participant Preferences From a Discrete Choice Experiment. J Patient Cent Res Rev. 2022;9(1):24–34. doi:10.17294/2330-0698.1874
16. Wagner AL, Zhang F, Ryan KA, et al. US Residents’ Preferences for Sharing of Electronic Health Record and Genetic Information: a Discrete Choice Experiment. Value Health. 2023;1:56.
17. Katz DA, Stewart KR, Paez M, et al. Development of a discrete choice experiment (DCE) questionnaire to understand veterans’ preferences for tobacco treatment in primary care. Patient. 2018;11(6):649–663. doi:10.1007/s40271-018-0316-6
18. Schildmann KE, Groeneveld IE, Denzel J, et al. Discovering the hidden benefits of cognitive interviewing in two languages: the first phase of a validation study of the integrated palliative care outcome scale. Palliat Med. 2015;30:599–610. doi:10.1177/0269216315608348
19. Cheraghi-Sohi S, Bower P, Mead N, et al. Making sense of patient priorities: applying discrete choice methods in primary care using ‘think aloud’ technique. Fam Pract. 2007;24(3):276–282. doi:10.1093/fampra/cmm007
20. Gomes B, de Brito M, Sarmento VP, et al. Valuing attributes of home palliative care with service users: a pilot discrete choice experiment. J Pain Symptom Manage. 2017;54(6):973–985. doi:10.1016/j.jpainsymman.2017.05.005
21. Kohler RE, Lee CN, Gopal S, et al. Developing a discrete choice experiment in Malawi: eliciting preferences for breast cancer early detection services. Patient Prefer Adherence. 2015;9:1459–1472. doi:10.2147/PPA.S87341
22. Tourangeau R, Rips LJ, Rasinski KA. The Psychology of Survey Response. Cambridge: Cambridge University Press; 2000.
23. Hole AR Mixed logit modelling in Stata - An overview. Available from: https://www.stata.com/meeting/uk13/abstracts/materials/uk13_hole.pdf.
24. Hauber AB, González JM, Groothuis-Oudshoorn CGM, et al. Statistical methods for the analysis of discrete choice experiments: a report of the ISPOR Conjoint Analysis Good Research Practices Task Force. Value Health. 2016;19(4):300–315. doi:10.1016/j.jval.2016.04.004
25. Pacifico D, Yoo HI. lclogit: a Stata command for fitting latent-class conditional logit models via the expectation-maximization algorithm. Stata J. 2013;13(3):625–639. doi:10.1177/1536867X1301300312
26. Veldwijk J, Marceta SM, Swait JD, et al. Taking the Shortcut: simplifying Heuristics in Discrete Choice Experiments. Patient. 2023;16(4):301–315. doi:10.1007/s40271-023-00625-y
27. Hoerger TJ, Howard LZ. Search behavior and choice of physician in the market for prenatal care. Med Care. 1995;33(4):332–349. doi:10.1097/00005650-199504000-00002
28. Liu X, Chen M, Li J, et al. How to Manage Diversity and Enhance Team Performance: evidence from Online Doctor Teams in China. Int J Environ Res Public Health. 2019;17(1):48. doi:10.3390/ijerph17010048
29. Jiang MZ, Fu Q, Xiong JY, et al. Preferences heterogeneity of health care utilization of community residents in China: a stated preference discrete choice experiment. BMC Health Serv Res. 2020;20(1):430. doi:10.1186/s12913-020-05134-4
30. Manthiram K, Blood EA, Kuppuswamy V, et al. Predictors of optional immunization uptake in an urban south Indian population. Vaccine. 2014;32:3417–3423. doi:10.1016/j.vaccine.2014.04.012
31. Zhu J, Li J, Zhang Z, et al. Exploring determinants of health provider choice and heterogeneity in preference among outpatients in Beijing: a labelled discrete choice experiment. BMJ Open. 2019;9:e023363. doi:10.1136/bmjopen-2018-023363
32. Zhao YC, Zhao M, Song S. Online Health Information Seeking Behaviors Among Older Adults: systematic Scoping Review. J Med Internet Res. 2022;24(2):e34790. doi:10.2196/34790
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.