")
Back to Journals » Patient Preference and Adherence » Volume 15
Preferences and Health-Related Quality-of-Life Related to Disease and Treatment Features for Patients with Hemophilia A in a Canadian General Population Sample
Authors Johnston K, Stoffman JM, Mickle AT, Klaassen RJ , Diles D , Olatunde S, Eliasson L , Bahar R
Received 28 April 2021
Accepted for publication 9 June 2021
Published 24 June 2021 Volume 2021:15 Pages 1407—1417
DOI https://doi.org/10.2147/PPA.S316276
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Karissa Johnston,1,2 Jayson M Stoffman,3 Alexis T Mickle,1 Robert J Klaassen,4 Demitri Diles,5 Shade Olatunde,5 Lina Eliasson,6 Roxana Bahar6
1Broadstreet HEOR, Vancouver, BC, Canada; 2School of Pharmacy, Memorial University, St John’s, NL, Canada; 3Department of Pediatrics and Child Health, Max Rady College of Medicine, University of Manitoba, Winnipeg, MB, Canada; 4Department of Pediatrics, Children’s Hospital of Eastern Ontario Research Institute, University of Ottawa, Ottawa, ON, Canada; 5Hoffmann-La Roche Limited, Mississauga, ON, L5N 5M8, Canada; 6Sprout Behavior Change Ltd, London, UK
Correspondence: Karissa Johnston
Broadstreet Health Economics and Outcomes Research, 201– 343 Railway Street, Vancouver, BC V6A 1A4, Canada
Email [email protected]
Background: Current treatments for hemophilia A in Canada include on-demand treatment as bleeds occur and regular intravenous prophylactic factor VIII (FVIII) infusions. The subcutaneous therapy emicizumab was recently approved for treatment of hemophilia A. The objective of this study was to estimate utility values associated with hemophilia A health and treatment states from a Canadian societal perspective, including preferences related to treatment efficacy and frequency and route of administration.
Methods: A vignette-based time trade-off (TTO) utilities elicitation was undertaken in Canadian adults to compare preferences for six hemophilia health states describing prophylactic and on-demand treatment, with varying bleed rates and frequency of treatment administration. A convenience sample was recruited via market research panels and snowball sampling. Health state/vignette definitions were informed by clinical experience, clinical trial results regarding bleed frequency, and validated by qualitative interviews of hemophilia patients and caregivers (n=10). Utilities were estimated via an online, trained interviewer-guided, vignette-based TTO exercise, where respondents valuated health states describing hemophilia patients (adults or children) receiving subcutaneous prophylaxis, intravenous prophylaxis, and on-demand treatments. Analyses included a descriptive analysis by health state; a mixed-effects analysis of utility values adjusted for subcutaneous vs infusion-based therapies and number of bleeds; and for prophylactic regimens, an analysis of utilities by frequency of infusions or injections.
Results: TTO interviews were conducted with 82 respondents. Mean utilities [95% CI] were highest for subcutaneous prophylaxis (0.90 [0.87– 0.93]), followed by intravenous prophylaxis (0.81 [0.78– 0.85]), and on-demand treatment (0.70 [0.65– 0.76]). In regression analysis, subcutaneous treatment health states were associated with a utility increment of +0.1112. Additional bleeds and more frequent infusions were associated with lower utility values (− 0.0027 per bleed and − 0.0003 per infusion).
Conclusion: Subcutaneous prophylaxis is associated with higher utility values compared to intravenous prophylactic and on-demand treatment, while increased bleeds and infusions are associated with reduced utility.
Keywords: Canadian societal perspective, health-related quality-of-life, utilities, hemophilia A
Background
Hemophilia is a rare congenital disorder that affects predominantly males, and is caused by a mutation of clotting factor genes on the X chromosome (X-linked) that result in a deficiency of factor VIII (FVIII) or -IX (FIX) in hemophilia A or B, respectively.1,2 Globally, 173,711 patients with hemophilia A were identified in 2018, and 3,018 were from Canada.1,3 Bleeding is the main symptom of hemophilia and it occurs after trauma or surgery (including minor/trivial injury), with the severity correlated with the degree of clotting factor deficiency.1,2 Bleeding can occur in muscles, joints, or soft tissue, and in life-threatening cases in the neck, throat, chest, gastrointestinal system, or intracranially.1,2 The main treatment goal is to prevent or treat bleeding; treatment of bleeds is generally via on-demand administration of specific factor concentrate to compensate for the deficient clotting factor, and historically prevention has included prophylaxis regimens of these factor-replacement therapies,1,2 with non-replacement factors having more recently become available.4 Other treatment goals are to prevent joint and muscle damage, prevent inhibitor development, prevent transmission of infections from blood products, and improve health-related quality-of-life (HRQoL).1,2
Until recently, prophylactic and on-demand treatments have consisted of intravenous exogenous FVIII replacement therapy with recombinant FVIII products or plasma-derived FVIII concentrates.1,2 Historically, hemophilia was primarily treated only when bleeding occurred (on-demand); however, over time the treatment paradigm shifted to prophylaxis with evidence that joint function is better preserved in patients with FVIII levels above 1% (>1 IU/dL)1,2 Based on high quality evidence of the superiority of prophylactic treatment over on-demand treatment, it has become standard of care in Canada for patients with severe hemophilia.1,2 Short-acting exogenous FVIII (eg, Elocta) have a short half-life (8–12 hours), and patients require three-to-four prophylactic infusions each week to maintain adequate trough levels.1,5,6 Extended half-life (EHL), or long-acting FVIII (eg, Advate; 40% increase in half-life) are also available in Canada, which lessen the frequency of infusions, but still require multiple infusions per week.7
Although exogenous FVIII concentrate is an effective treatment, one possible serious complication is the development of FVIII inhibitors.1,2 Inhibitors are immunoglobulin G antibodies that inactivate both exogenous and endogenous FVIII, making FVIII replacement treatment ineffective, at high titers.1,2,6 Approximately 5–10% of patients with mild-to-moderate hemophilia A, and 20–30% of patients with severe hemophilia A, develop inhibitors.1,2
Emicizumab is a monoclonal antibody that restores the natural function of activated FVIII by bridging activated factor IX and factor X in hemophilia A patients to allow for effective hemostasis.1,5,8,9 Emicizumab, administered subcutaneously, has been shown to be effective in reducing bleeding events in patients with hemophilia A with inhibitors in the HAVEN 1 and 2 trials,10,11 as well as in patients with hemophilia A without inhibitors in the HAVEN 3 and 4 trials.1,5,12 Across the clinical trial program, clinical benefits of emicizumab have been observed for weekly, once every 2 weeks (Q2W), and once every 4 weeks (Q4W) dosing schedules (with Q4W dosing recommended only for adults and/or adolescents >40 kg [in the Canadian label]).13
The HRQoL of patients with hemophilia is negatively affected by both the disease and treatment.14 Recurrent bleeding and resulting complications such as joint and muscle damage, and pain and disability, can significantly affect patients’ HRQoL.14 Treatment-related factors include the need for frequent infusions due to the half-life of available therapies, and specific infusion-related problems such as difficulty with accessing veins, the time required to administer treatment, and development of inhibitors – all of which can have a negative effect on treatment adherence, lifestyle, and HRQoL.15 In addition to hemophilia patients, having a family member with hemophilia inevitably increases the burden on the caregivers and the family, especially when a child is affected.16,17 The emotional and practical aspects of caregiver burden are especially high when the patient requires frequent infusions of hemophilia treatment. Worse social, physical, emotional, financial, and lifestyle impact were associated with more infusions per week in a large study of hemophilia caregivers.18
Numerous studies have been conducted to assess the HRQoL of hemophilia A as characterized by utilities, in Canada and internationally.19 Factors that have been found to be associated with a positive impact on HRQoL include increased effectiveness of treatments, reduced adverse events, and reduced dosing frequency.20 Patients generally prefer prophylactic to on-demand treatment, likely due to improved clinical outcomes with prophylactic treatment.20
However, the impact of frequent intravenous infusions and the type of treatment on HRQoL has not been explored adequately.21 Recently, subcutaneous treatments have become available for hemophilia A, and, while currently emicizumab is the only available subcutaneous therapy, other pipeline therapies are likely to become available in the future. There are challenges with understanding health state utilities for subcutaneous treatments because the impact of subcutaneous administration compared to intravenous administration has not been previously explored in hemophilia patients. However, there are studies in patients with other chronic conditions that found a preference for subcutaneous administration compared to intravenous administration.22–24 Current intravenous hemophilia treatments can be time-consuming, challenging, complex, and painful to administer, and can lead to difficulty in coordinating schedules (including work schedules) and maintaining a routine, cause anxiety, trauma, exhaustion, social stigma, and impact personal relationships and career opportunities.14 Participants in a Canadian survey study reported that delivery via an alternate route of administration (subcutaneous or oral), and treatments with longer-lasting effects in order to reduce the frequency of administration, would be substantial improvements over the current standard of care.25
The aim of this study was to estimate utility values associated with hemophilia A patients’ health and treatments (on demand, infusion prophylaxis, and subcutaneous prophylaxis) amongst members of the Canadian general public. Results of this analysis can be used to populate Canadian cost-utility analysis of subcutaneous therapy vs intravenous prophylaxis and on-demand therapy, respectively.
Methods
A de novo utilities study was conducted in a Canadian general population sample to compare HRQoL across treatment states, including the HRQoL implications of bleeds, treatment modality, and frequency of infusions. All adults currently residing in Canada were eligible. Specifically, inclusion criteria included: 1) a person who resides in Canada; 2) aged 18 years or older; 3) able to read and speak English fluently; 4) voluntarily provides recorded verbal informed consent/assent, as applicable, after all relevant aspects of the study have been explained and discussed with them; and 5) able to understand the nature, scope, and possible consequences of the study, and agree to comply with the interview. Exclusion criteria included 1) aged 17 years or younger at screening; and 2) have any medical or psychiatric illness, or indication of cognitive impairment, that could, in the opinion of the study staff, potentially interfere with the participant’s ability to participate in the interview. A convenience sample was recruited via market research panels and snowball sampling, with demographics intended to approximate the Canadian population. Participants were recruited from May 1, 2020 to May 18, 2020 by a specialist recruitment agency, Global Perspectives, who reached out to patients using ad-hoc recruitment techniques (e-mail invitations, recruiter databases/panels, patient associations, physician referrals, and social media advertisements). All patients, or caregivers of child/adolescent patients, who expressed interest in the project were screened by an experienced professional healthcare recruiter on the phone, giving a chance for the recruiter to discuss the project with the respondent and ensure that the respondent meets the rest of the eligibility criteria.
A vignette-based time trade-off (TTO) utilities elicitation was undertaken to compare population preferences for subcutaneous treatment compared to intravenous prophylaxis and on-demand treatment. The general population study conducted here allows for consideration of a Canadian societal perspective. Hemophilia A health states were developed based on clinical investigator experience (two clinicians) with treating this population, and Independent Review Board (IRB)-approved in-depth, semi-structured qualitative interviews with eight Canadian adult caregivers of children with moderate-to-severe hemophilia A and two Canadian adults with moderate-to-severe hemophilia A. Unconditional IRB approval was granted by Veritas IRB on December 13, 2019 (IRB tracking number 16556–17:21:0124-04-2020). The objective was to understand the specific disease and treatment burdens that patients with hemophilia A face, as well as their preferences for treatment options. Transcripts were analyzed with Hyper Research software and a content and thematic analysis was conducted.26 Participants were compensated with CAD $138.00 for their participation in the utility elicitation study, which was approved by Veritas IRB on April 24, 2020 (IRB Tracking Number: 16556–17:21:0124-04-2020). This study was conducted in accordance with the Declaration of Helsinki, and both the qualitative interview participants and TTO survey respondents provided recorded verbal informed consent after all relevant aspects of the study, including the nature, scope, and possible consequences of the study, were explained and discussed with them. In all phases of this study, personal information and study data were accessible only to the persons mentioned in the Informed Consent Form unless required by law, personal information was protected according to the Tri-Council Policy Statement 2: Ethical Conduct for Research involving humans (TCPS 2) 2018.27 The confidentiality of records that could potentially be used to identify participants (ie, encrypted and password protected file with consented participants name and participant identification numbers) was protected in accordance with applicable laws, regulations, and guidelines. After participants consented to take part in the project, the Sponsor and/or its representatives took all reasonable precautions to maintain the confidentiality of participants’ identities. For the TTO utilities survey, personal identifiable data was collected at the point of obtaining verbal informed consent. The participant was asked to provide their first name, or an alias of their choice, as well as a telephone number/email address for the videoconference survey to the interviewer. The interviewer then recorded this information against a unique participant ID number. The participants’ ID was then used to link the responses from the data collection. The participant ID number was not shared with the participant. All identifiable data was kept and transferred using encrypted and password-protected files. No other person-identifiable data was collected, ensuring the anonymity of the participant throughout the project. Audio recordings and transcripts were only available to the study team; both were stored on secured, password-protected data servers. After generation of the final report and manuscript(s), audio recordings and transcripts were irreversibly destroyed using methods recommended by the Office of the Privacy Commissioner of Canada’s Personal Information Retention and Disposal: Principles and Best Practices.28 In brief, all hard copy media was physically destroyed through shredding and pulverizing; whereas all electronic copy media was destroyed by methods that resist simple recovery methods as described in the National Institute of Standards and Technology’s Guidelines for Media Sanitization.29
Clinical Inputs
Clinical inputs into health states, where available, were sourced from the HAVEN 3 and HAVEN 4 trials and published literature. HAVEN 3 was a randomized, multicenter, open-label, Phase III clinical study in 152 adult and adolescent males (age ≥12 years) with severe hemophilia A without FVIII inhibitors who previously received either episodic (on demand) or prophylactic treatment with FVIII.5,30 Two different treatment regimens were evaluated relative to episodic treatment with FVIII: prophylactic treatment with emicizumab at doses of 1.5 mg/kg weekly (QW) or 3 mg/kg Q2W. Patients who received episodic FVIII prior to enrolment were randomized to one of the two emicizumab maintenance regimens (Arm A: 1.5 mg/kg QW, Arm B: 3 mg/kg Q2W, or Arm C: no prophylaxis). In addition to the randomized component, HAVEN 3 included a non-interventional study (NIS) in which patient characteristics and clinical outcomes such as bleed rates were retrospectively extracted from charts of patients receiving FVIII prophylaxis, both short- and long-acting (EHL), prior to study initiation.5 HAVEN 4 is an open-label, multicenter, Phase III clinical study in adults and adolescents (≥12 years) with severe congenital hemophilia A or hemophilia A with FVIII inhibitors who were previously treated with FVIII concentrates or recombinant factor VII (rFVIIa), or were willing to switch to rFVIIa to treat breakthrough bleeds.30 Participants received a loading dose of subcutaneous emicizumab 3 mg/kg Q1W (monthly), followed by 6 mg/kg Q4W for 24 weeks as prophylaxis.30
Interventions
Health states were designed to describe prophylactic subcutaneous treatment, prophylactic intravenous infusion, and on-demand interventions.
Outcomes
Overall, six health states were evaluated:
●Health State A: On-demand therapy, with 36 bleeds per year (3 per month)
●Health State B: intravenous prophylaxis with 2–3 infusions per week and 4–5 bleeds per year
●Health State C: intravenous prophylaxis with 2–3 infusions per week and 10 bleeds per year
●Health State D: intravenous prophylaxis with daily infusions and 4–5 bleeds per year
●Health State E: Subcutaneous prophylaxis with weekly injections and 1–2 bleeds per year
●Health State F: Subcutaneous prophylaxis with monthly injections and 1–2 bleeds per year
Health states A, B, and E correspond closely to the HAVEN 3 results, while Health states C, D, and F were included to assess the impact on number of bleeds, frequency of infusions, and frequency of injections on reported utilities. All health states and vignettes were drafted in two distinct versions: one based on the experience of a child with hemophilia, and one based on the experience of an adult with hemophilia, and respondents were randomly allocated to one of the two versions.
TTO utilities were elicited from the Canadian general population via a “ping-pong” protocol for question ordering,31–34 as well as a VAS rating. For the TTO utilities elicitation, the value range included states better than death (BTD) and worse than death (WTD), both valuated using the “ping-pong” method. Best possible health was defined as “perfect health”. For valuation of the BTD health states, the duration of disease was fixed at 10 years while the duration of perfect health varied with no lead/lag time (eg, living with hemophilia for 10 years followed by a quick and painless death vs living in perfect health for 4 years followed by a quick and painless death). For valuation of the WTD scale, the time spent in perfect health was followed by time spent with hemophilia for a total of 10 years (eg. 9 years in perfect health followed by 1 year with hemophilia), followed by a quick and painless death, vs an immediate quick and painless death. For both the BTD and WTD elicitations, the option “they are about the same” was provided, the smallest tradeable unit of perfect health was 0.5 years and final responses were titrated 0.25 years to represent the value between the prior question and the point of indifference, unless “they are about the same” was chosen (Appendix 1). This process was completed for all six health states for either the adult or child version for each participant.
For BTD health states, utilities (U(h)) were calculated as:
x = years in perfect health (varies)
t = years with hemophilia (fixed)
U(h) = x/t,
While for WTD health states, U(h) were calculated as:
x = years in perfect health
t-x = years with hemophilia
U(h) = -x/(t-x), where t+x = 10 years.
Interviews were intended to be conducted as face-to-face interviews; however, due to the current COVID-19 pandemic, were conducted by trained interviewers via videoconference and data were entered directly into the secure server. A brief preamble was followed by a warm-up task. Visual aids, with viewing options at all times during the survey, were used to describe life with severe hemophilia, including descriptions of severe hemophilia and associated bleeds, and intravenous infusion prophylaxis, subcutaneous prophylaxis, and on-demand treatment health-states, with different versions for adult and child (Appendix 2). All six health states (A–F) were directly valuated and described in disease-specific terms. Health state descriptions were generated using clinical investigator experience and information acquired from 10 qualitative interviews.
Analyses
Three key analyses were undertaken for both TTO utilities and VAS scores: 1) a descriptive analysis of mean and 95% confidence interval (CI) by health state, 2) a mixed-effects (random-intercept by patient) analysis of utility values as predicted by subcutaneous vs infusion-based therapies and number of bleeds, and 3) for prophylactic regimens, an analysis of utilities by frequency of infusions or injections, to understand the impact and potential disutility of infusions and injections. In the first random-intercept model, adjustments were made for subcutaneous vs intravenous treatment modalities and the number of bleeds per year. Note that in this regression analysis, covariates for age, sex, and adult vs child survey were tested, but none of these parameters were found to be statistically significant and thus were not included in the final models and associated results.
To assess the impact of respondent comprehension, a sensitivity analysis was conducted amongst only patients who reported estimated utility values that were plausible based on dominant health states (ie, only individuals who ranked health state B above health states C and D, and health state F above health state E).
In the second model, only prophylactic regimens were considered, and utilities and VAS scores were assessed based on frequency of infusions and injections, respectively (ie, by fitting one model to compare results of Health States B vs D and a second to compare results of Health States E vs F).
Results
The sample consisted of 82 adult respondents, of whom 59% were women and 41% were men. Fifty-four percent answered the adult version of the survey, while the remaining 46% answered the pediatric version. Crude mean and 95% CI results are reported in Table 1 and can be visualized in Figure 1A. Utilities were highest for subcutaneous health states and lowest for on-demand therapy. Health states A, B, and E, which correspond to base case model health states, were associated with utilities of 0.70 (on-demand), 0.81 (intravenous prophylaxis), and 0.90 (subcutaneous prophylaxis). Additional bleeds and more frequent infusions and injections were associated with lower utility values, although the values for weekly vs monthly subcutaneous injections were close (0.90 vs 0.91, with highly overlapping CIs). The VAS results followed similar trends, although with relatively lower results on the 0–100 scale compared to TTO utilities on the 0–1 scale (Table 1; Figure 1B).
 |
Table 1 Mean and 95% Confidence Intervals (CI) for Utility and Visual Analogue Scale (VAS) Results |
 |
Figure 1 Mean and 95% confidence intervals (CI) for (A) utility and (B) visual analogue scale (VAS) results. |
In the regression analysis, subcutaneous treatment was associated with a utility increment of +0.1112, and each bleed per year a decrement of −0.0027 (Table 2). Thus, while respondents indicated a preference for health states with fewer bleeds, the preference for a subcutaneous vs intravenous treatment was stronger. For health state E, the regression-predicted utility was 0.903. Health state B was associated with a regression-predicted utility of 0.784, reflecting lower utility than health state E related to intravenous vs subcutaneous route of administration, and increased bleeds (4.5 vs 1.5). However, in a hypothetical health state where the number of bleeds is decreased from 4.5 to 1.5 but intravenous route of administration, the resulting predicted utility is 0.792 – higher than that of health state B, but notably lower than that of health state E.
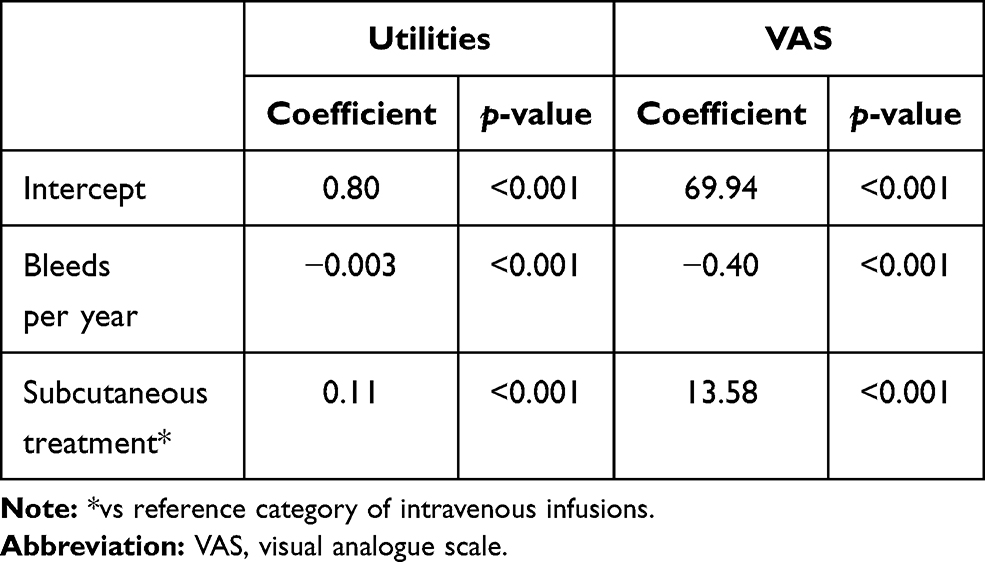 |
Table 2 Regression Coefficients in Random-Intercept Analysis of Utilities and Visual Analogue Scale (VAS) Results |
In the sensitivity analysis, 37% of patients were excluded due to having at least one implausible estimate across health states B with C or D, or E with F. When the regression analysis was repeated with the remaining 63% of respondents, results were similar to the main analysis reported in Table 1, with an estimated intercept of 0.801, increment of +0.1091 for subcutaneous treatment, and decrement per bleed of −0.0025. Thus, lack of comprehension was not found to influence results.
In the second set of regression analyses regarding preferences for frequency of infusions or injections, for the intravenous prophylaxis model, each annual intravenous infusion was associated with a statistically significant disutility of −0.0003, while each annual subcutaneous injection was associated with an estimated disutility of −0.0002, although this latter difference was not found to be statistically significant due to wider variability in patient responses (Table 3). This is generally consistent with the results reported in Table 1 and Figure 1A, in which similar utility estimates were found for weekly vs monthly subcutaneous injection regimens.
 |
Table 3 Regression Coefficients in Random-Intercept Analysis of Utilities on the Frequency of Injections/Infusions |
Discussion
This paper reports utility values from a Canadian societal perspective for different health and treatment states, including the HRQoL implications of bleeds, treatment modality [prophylactic subcutaneous treatment vs intravenous infusion prophylaxis and on-demand therapy], and frequency of infusions. Members of the Canadian population preferred subcutaneous health states compared to intravenous infusions, and to a lesser extent health state utilities also reflected a desire to avoid additional bleeding episodes and infusions. Therefore, evidence suggests that the benefit of subcutaneous administration was more important than the number of bleeding episodes within the likely range of bleeding episodes to occur with prophylactic regimens. VAS results were 56.2 for on-demand treatment, 71.1 for intravenous infusion prophylaxis, and 81.6 for subcutaneous prophylaxis, while utilities were 0.70 for on-demand treatment, 0.81 for intravenous prophylaxis, and 0.90 for subcutaneous prophylaxis. This aligns with a study in 22 hemophilia patients with inhibitors which compared prophylaxis with on-demand treatment and found that prophylaxis resulted in a reduction in bleeding frequency which improved HRQoL.35 Additionally, prophylactic treatment decreased absenteeism and pain, and increased mobility and median VAS and TTO scores (from 66–73, p=0.048; and from 0.62–0.76, p=0.054, respectively).35 Other studies had similar findings.36–38 A study of 401 boys with hemophilia from nine countries, including 168 from Canada (82.7% with hemophilia A), assessed the effect of prophylaxis and disease severity on HRQoL and found that prophylactic treatment significantly increased HRQoL compared to on-demand treatment (mean Canadian Hemophilia Outcomes-Kids’ Life Assessment Tool (CHO-KLAT) score (SD) of 74.5 (12.7) vs 71.7 (13.1), respectively), whereas increased disease severity was associated with significantly lower HRQoL compared to mild or moderate disease.39 Mean CHO-KLAT score (SD) of Canadian boys was 75.0 (13.0).39 A CUA comparing primary prophylactic treatment with on-demand treatment in Canadian boys with severe hemophilia A found that HRQoL and clinical outcomes are substantially improved with prophylaxis compared to on-demand treatment, but it comes at a substantial incremental cost per QALY.40 In a prior study it was not found that prophylactic treatment improved HRQoL, but there were several limitations noted, including not taking into account the impact of frequent intravenous infusions on HRQoL.41
Although a societal perspective is important, patient perspective is also important, since treatment improvements may have positive impacts on treatment adherence, employment (economic), social, and health aspects.25 The Institute for Clinical and Economic Review (ICER; United States) recently released a report assessing the clinical effectiveness and value of current hemophilia A therapies indicating that, compared to factor VIII prophylaxis, subcutaneous therapy reduces patient and caregiver burden and may improve patient outcomes.42 A qualitative study of 12 Canadian patients with hemophilia A and eight caregivers found several challenges with current treatments which negatively affect participants’ quality-of-life, including their physical, social, and psychological well-being.25 Based on the findings of studies in patients with other conditions, treatments with a different route of administration may address some of these problems. A systematic review compared patient-preference for intravenous vs subcutaneous administration across a diverse patient population and treatments, and found that patients clearly preferred subcutaneous administration over intravenous administration, primarily due to factors related to time and convenience.24 This may have implications for HRQoL and adherence to treatment.24 Another systematic review of patient preferences regarding treatment for rheumatoid arthritis found that sociodemographic characteristics influenced patient preferences, but that the benefit of the treatment was more important than the route of administration, adverse events, or costs.22 However, patients often preferred subcutaneous treatment over intravenous treatment.22 A systematic review to determine the burden of treatment in patients with primary immunodeficiency disorders found that the burden of treatment was generally low overall and patients were satisfied with both intravenous and subcutaneous immunoglobulin treatment, however once patients switched from intravenous to subcutaneous, subcutaneous treatment was preferred.23 These studies were not conducted specifically in patients with hemophilia, and an interesting question would be whether patients with hemophilia A who are currently being treated with intravenous FVIII would still rank their HRQoL with current treatment as high once they have experienced treatment with a different treatment modality that is administered subcutaneously.
Limitations
To our knowledge, this is the first study to compare preferences for intravenous vs subcutaneous prophylaxis in hemophilia. This study used a vignette-based TTO method in a general population sample. Thus, we captured preferences indicated by the general public based on descriptions of relevant health states; actual experience of such health states by hemophilia patients are additionally of interest but given the recent introduction of subcutaneous treatments for this patient population, such a study is not feasible at this time.
According to a study that compared the agreement between EQ-5D-3L and vignette-based TTO, vignette-based TTO methods tend to generate lower utility scores than the EQ-5D, and disagreement between the two methods are increased with chronic diseases compared to acute disease.43 This can lead to systematic differences between resulting cost-effectiveness calculations across the two methods; the aim with TTO health states is to develop them to be sufficiently nuanced as to capture the key features of living with the disease, but not to the point where complexity and/or subjectivity create challenges for respondents.43 Of note, however, the impact of TTO vs EQ-5D utilities is not anticipated to affect different health states differentially. Although the absolute values of all utilities may have been higher in an EQ-5D study, there is no a priori expectation that the incremental difference between intravenous and subcutaneous health states would have been different.
An additional limitation was the limited variability explored in efficacy outcomes across health states; the bleed rates assumed for intravenous health states was based on the observed NIS outcomes from HAVEN3. However, this may be influenced by adherence levels to FVIII in a real-world setting and/or the threshold used by clinicians to define a bleed, outside of a standardized clinical trial definition. As HAVEN3 represents the key data source for subcutaneous therapy in hemophilia A without inhibitors it was used to inform health states, although the inclusion of health states C, D, and F allow for exploration of varying bleed rates and infusion schedules on stated preferences.
Next Steps
As real-world data accrue from hemophilia A patients with and without inhibitors, having experience with both intravenous and subcutaneous regimens, a companion HRQoL study from the patient perspective would provide valuable insights to the general population results described here. Obtaining results from a patient population would incorporate the full range of patient characteristics and bleed rates across therapy types rather than a fixed set of assumed efficacy levels, and patients who have experience with both intravenous and subcutaneous treatment modalities would add further nuance to degree of preference. Further, within a patient sample, direct elicitation can be made regarding treatment experience and adherence levels, and impact on physical and mental health, and the ability to conduct activities of daily living. Of particular interest is whether patients and families with less resources available to support regular infusions have differential preferences for alternative treatment options.
Conclusions
Subcutaneous prophylaxis is associated with higher utility values compared to intravenous prophylaxis and on-demand treatment, while increased bleeds and infusions resulted in lower utility values. The observed preference for subcutaneous therapies and less frequent dosing schedules is consistent with observed results in other disease areas and may be a consideration for hemophilia A patients who would prefer to avoid frequent infusions.
Abbreviations
ABR, annual bleed rate; BTD, better than death; CHO-KLAT, Canadian Hemophilia Outcomes-Kids’ Life Assessment Tool; CI, confidence interval; CUA, cost utility analysis; EQ-5D, EuroQuol-5D; FVIII, factor VIII; FVIX, factor IX; HIV, human immunodeficiency virus; HRQoL, health-related quality-of-life; HUI3, Health Utilities Index Mark 3; IRB, Independent Review Board; ITI, immune tolerance induction; NIS, non-interventional study; Q1W, once weekly; Q2W, once bi-weekly (every 2 weeks); Q4W, once monthly (every 4 weeks); QALY, quality-adjusted life years; QW, once weekly; rFVIIa, recombinant factor VII; TTO, time trade-off; VAS, visual analogue scale; WTD, worse than death.
Data Sharing Statement
Anonymized data from this study can be provided upon request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and was approved by Veritas Institutional Review Board on April 24, 2020 (IRB Tracking Number: 16556-17:21:0124-04-2020). All survey respondents provided verbal informed consent (recorded) prior to participation.
Consent for Publication
The publication of study results was not contingent on the sponsor’s approval or censorship of the manuscript.
Acknowledgments
We would like to acknowledge Sarah Clifford’s and Inka Karppinen’s contributions to the development of this manuscript.
Author Contributions
SO and DD contributed to the study design, LE and RB conducted hemophilia A patient recruitment and qualitative interviews, KJ, ATM, SO, and DD designed the TTO utilities and VAS study protocol, JK and ATM conducted the online interviews, JMS and RJK provided expert clinical experience, KJ analyzed the data, KJ, ATM, SO, and DD were main contributors in writing the manuscript. All authors read and approved the final manuscript. All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This work was sponsored by Hoffmann-La Roche Ltd.
Disclosure
Dr Jayson M Stoffman received consulting honorarium from Hoffman-La Roche Ltd, during the conduct of the study; and consulting honorarium from Hoffman-La Roche and Bayer Inc., outside the submitted work. Dr Robert J Klaassen reports personal fees from Amgen Inc, personal fees from Hoffman-LaRoche Ltd, personal fees from Novo Nordisk, personal fees from Octapharma EG, personal fees from Takeda Canada Inc, and personal fees from Sanofi Canada, during the conduct of the study. Ms Shade Olatunde is an employee of Hoffmann-La Roche Ltd. Dr Lina Eliasson is an employee of Sprout Behaviour Change, who were subcontracted to assist the conduct of the qualitative interviews by Broadstreet HEOR. Dr. Karissa Johnston and Alexis Mickle are employees of Broadstreet HEOR, who received funding from Hoffmann-La Roche Ltd. for the conduct of the study.
The authors report no other conflicts of interest in this work.
References
1. Srivastava A, Santagostino E, Dougall A, et al. WFH Guidelines for the Management of Hemophilia, 3rd edition. Haemophilia. 2020;26:1–158.
2. Srivastava A, Brewer A, Mauser-Bunschoten E, et al. WFH Guidelines for the management of hemophilia. Haemophilia. 2013;19:e1–e47.
3. World Federation of Hemophilia. Report on the Annual Global Survey 2018: Montréal, Québec; 2019.
4. Weyand AC, Pipe SW. New therapies for hemophilia. Blood. 2019;133:389–398.
5. Mahlangu J, Oldenburg J, Paz-Priel I, et al. EmicizumaB prophylaxis in patients who have Hemophilia A without Inhibitors. N Engl J Med. 2018;379:811–822.
6. Peyvandi F, Garagiola I, Seregni S. Future of coagulation factor replacement therapy. J Thromb Haemost. 2013;11:84–98.
7. Cafuir LA, Kempton CL. Current and emerging factor VIII replacement products for hemophilia A. Ther Adv Hematol. 2017;8:303–313.
8. Institute for Clinical and Economic Review. Emicizumab for Hemophilia a with Inhibitors: Effectiveness and Value. CEPAC. 1–162. 2018.
9. Roche Canada. Positive phase III results for Roche’s Hemlibra for haemophilia A without factor VIII inhibitors. N Engl J Med. 2018.
10. Oldenburg J, Mahlangu J, Kim B, et al. Emicizumab prophylaxis in hemophilia A with inhibitors. N Engl J Med. 2017;377:809–819.
11. Young G, Sidonio R, Liesner R et al. HAVEN 2 updated analysis: multicenter, open-label, Phase 3 study to evaluate efficacy, safety and pharmacokinetics of subcutaneous administration of emicizumab prophylaxis in pediatric patients with hemophilia A with inhibitors. The Annual meeting of the American Society of Hematology. Atlanta, GA 2017.
12. Pipe S, Shima M, Lehle M, et al. Efficacy, safety, and pharmacokinetics of emicizumab prophylaxis given every 4 weeks in people with haemophilia A (HAVEN 4): a multicentre, open-label, non-randomised phase 3 study. Lancet Haematol. 2019;6:e295–e305.
13. Hoffmann-La Roche Limited. Product Monograph: Pr HEMLIBRA® Subcutaneous Emicizumab Injection. Mississauga, ON: Health Canada; 2019.
14. Naraine V, Risebrough N, Oh P, et al. Health-related quality-of-life treatments for severe haemophilia: utility measurements using the Standard Gamble technique. Haemophilia. 2002;8:112–120.
15. Santagostino E, Lentz S, Busk A, et al. Assessment of the impact of treatment on quality of life of patients with haemophilia A at different ages: insights from two clinical trials on turoctocog alfa. Haemophilia. 2014;20:527534.
16. DeKoven M, Karkare S, Lee W, et al. Impact of haemophilia with inhibitors on caregiver burden in the United States. Haemophilia. Haemophilia. 2014;20:822–830.
17. Khair K, Von Mackensen S. Caregiver burden in haemophilia: results from a single UK centre. The Journal of Haemophilia Practice. J Haemophilia Pract. 2017;4:40–48.
18. Schwartz C, Powell V, Su J, et al. The impact of extended half-life versus conventional factor product on hemophilia caregiver burden. Qual Life Res. 2018;27:1335–1345.
19. Barr R, Saleh M, Furlong W, et al. Health status and health‐related quality of life associated with hemophilia. Am J Hematol. 2002;71:152–160.
20. Chaugule S. Hay J and Young G. Understanding patient preferences and willingness to pay for hemophilia therapies. Patient Prefer Adherence. 2015;9:1623–1630.
21. Grosse S. Chaugule S and Hay J. Estimates of utility weights in hemophilia: implications for cost utility analysis of clotting factor prophylaxis. Expert Rev Pharmacoecon Outcomes Res. 2015;15:267–283.
22. Durand C, Eldoma M, Marshall D, et al. Patient preferences for disease-modifying antirheumatic drug treatment in rheumatoid arthritis: a systematic review. J Rheumatol. 2020;47:176–187.
23. Jones G, Vogt K, Chambers D, et al. What is the burden of immunoglobulin replacement therapy in adult patients with primary immunodeficiencies? A systematic review. Front Immunol. 2018;9:1308.
24. Stoner K, Harder H, Fallowfield L, et al. Intravenous versus subcutaneous drug administration. Which do patients prefer? A systematic review. The Patient. 2015;8:145–153.
25. Wiley R, Khoury C, Snihur A, et al. From the voices of people with haemophilia A and their caregivers: challenges with current treatment, their impact on quality of life and desired improvements in future therapies. Haemophilia. 2018;25:433–440.
26. Joffe H, Yardley L. Content and thematic analysis. In: Marks DF, & Yardley L, Editors. Research Methods for Clinical and Health Psychology. London: SAGE Publications, Ltd.; 2004:56–68.
27. Government of Canada Canadian Institutes of Health Research NSaERCoC, and the Social Sciences and Humanities Research Council. Tri-Council Policy Statement - Ethical Conduct for Research Involving Humans (TCPS2 2018). 2018.
28. Office of the Privacy Commissioner of Canada. Personal Information Retention and Disposal: Principles and Best Practices. 2014.
29. National Institute of Standards and Technology. US Department of Commerce. Guidelines for Media Sanitization: Computer Security; 2014.
30. ClinicalTrials.gov. A Study to Evaluate the Efficacy, Safety, Pharmacokinetics, and Pharmacodynamics of Emicizumab Given Every 4 Weeks in Participants With Hemophilia A (HAVEN 4) NCT03020160. 2020.
31. Lenert LA, Cher DJ, Goldstein MK, et al. The effect of search procedures on utility elicitations. Med Decision Making. 1998;18:76–83.
32. Attema AE, Edelaar-Peeters Y, Versteegh MM, Stolk EA. Time trade-off: one methodology, different methods. Eur j Health Econom. 2013;14(Suppl 1):S53–64.
33. Oppe M, Rand-Hendriksen K, Shah K, et al. EuroQol protocols for time trade-off valuation of health outcomes. PharmacoEconomics. 2016;34:993–1004.
34. Shen J, Hill S, Mott D, et al. Conducting a time trade-off study alongside a clinical trial: a case study and recommendations. PharmacoEconomics. 2019;3:5–20.
35. Hoots W, Ebbesen L, Konkle B, et al. Secondary prophylaxis with recombinant activated factor VII improves health‐related quality of life of haemophilia patients with inhibitors. Haemophilia. 2008;14:466–475.
36. Noone D, O’Mahony B, Prihodova L. A survey of the outcome of prophylaxis, on-demand or combined treatment in 20-35 year old men with severe haemophilia in four European countries (letter). Haemophilia. 2011;17:E842–E3.
37. Oladapo A, Epstein J, Williams E, et al. Health-related quality of life assessment in haemophilia patients on prophylaxis therapy: a systematic review of results from prospective clinical trials. Haemophilia. 2015;21:e344–e58.
38. Stasyshyn O, Antunes S, Mamanov V, et al. Prophylaxis with anti‐inhibitor coagulant complex improves health‐related quality of life in haemophilia patients with inhibitors: results from FEIBA NF Prophylaxis Study. Haemophilia. 2014;20:644–650.
39. Usuba K, Price V, Blanchette V, et al. Impact of prophylaxis on health‐related quality of life of boys with hemophilia: an analysis of pooled data from 9 countries. Res Pract Thromb Haemost. 2019;3:397–404.
40. Risebrough N, Oh P, Blanchette V, et al. Cost‐utility analysis of Canadian tailored prophylaxis, primary prophylaxis and on‐demand therapy in young children with severe haemophilia A. Haemophilia. 2008;14:743–752.
41. Buchbinder D, Ragni V. What is the role of prophylaxis in the improvement of health-related quality of life of patients with hemophilia? Hematology Am Soc Hematol Educ Program. 2013;52-5.
42. Institute for Clinical and Economic Review. Valoctocogene Roxaparvovec and Emicizumab for Hemophilia A without Inhibitors: Effectiveness and Value: Final Report. Institute for Clinical and Economic Review. 2020.
43. Briggs A. Belozeroff V and Feeny D. Comparison of health state utility estimates from instrument-based and vignette-based methods: a case study in kidney disease. BMC Res Notes. 2019;12:385.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.