")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Predicting End-of-Life in a Hospital Setting
Authors Giwangkancana GW , Anina HN, Sukandar H
Received 6 October 2023
Accepted for publication 14 December 2023
Published 9 February 2024 Volume 2024:17 Pages 619—627
DOI https://doi.org/10.2147/JMDH.S443425
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Gezy Weita Giwangkancana,1 Heni Nur Anina,2 Hadyana Sukandar3
1Department of Anesthesia and Intensive Care, Faculty of Medicine Universitas Padjadjaran /Dr. Hasan Sadikin National Referral and Teaching Hospital, Bandung, Indonesia; 2Department of Nursing Dr. Hasan Sadikin National Referral and Teaching Hospital, Bandung, Indonesia; 3Department of Public Health Faculty of Medicine Universitas Padjadjaran, Bandung, Indonesia
Correspondence: Heni Nur Anina, Palliative Care Team, Dr. Hasan Sadikin National Referral and Teaching Hospital, RSUP Dr Hasan Sadikin, Bandung, Pasteur Street No. 38, Bandung, 40161, Indonesia, Tel +6281546562490, Email [email protected]
Background: The ability to predict the prognosis of a disease and anticipate death is valuable for patients and families especially in an acute care setting for chronically ill patient. Multiple scoring systems are used to measure disease progression and predict hospital mortality in patients with life-threatening illnesses, taking into account acute conditions, catastrophic events, and slow decline.
Aim: Our primary aim is to assess palliative performance score (PPS), early warning score (EWS) and local rumah sakit Dr Hasan Sadikin (RSHS) score to predict 14 days in-hospital mortality.
Methods: This was a single-center prospective cohort study from November 2022 to April 2023. Patients with World Health Organization category of terminal illnesses were scored using PPS, EWS and RSHS score and were followed up for 14 days in hospital. Multivariate analysis were conducted and The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines were used.
Results: A multivariable model was calculated using Cox regression. The final model results indicate that EWS (HR: 2.9, 95% CI: 1.1– 7.7) and a decrease in consciousness (HR: 3.6, 95% CI: 1.2– 10.22) were statistically significant in predicting mortality.
Discussions: Most patient in the cohort that died had cancer and were admitted in the previous 6 months. Relying solely on single prediction may not provide enough accuracy, within a 14-day timeframe. Therefore, the results of multivariate analysis were not statistically significant due to Several factors contribute to the complexity of this prediction challenge. As a multifaceted disease with varying stages, treatments, and outcomes, cancer presents a diverse landscape of patient experiences.
Conclusion: EWS and decreased consciousness are significant predictors of in-hospital mortality. It is crucial in clinical setting to use multiple indicators to predict death and improve patient care.
Keywords: accreditation, care op patient, continuity of care, end of life, hospice, palliative care
Introduction
Monitoring in-hospital mortality is essential to ensuring quality care in healthcare and hospital settings. It is a crucial indicator of the effectiveness of high-level processes in these settings. As such, keeping a close eye on in-hospital mortality rates is essential to ensure patients receive the best care possible.1–3Although many diseases can be prevented, mortality and disability are often inevitable, especially as people age and face chronic illnesses defined by the World Health Organization (WHO), such as cardiovascular, lung, and renal diseases, cancer, AIDS, and neurodegenerative diseases like multiple sclerosis, Parkinson’s disease, stroke, epilepsy, and brain tumors. Therefore, palliative and end-of-life care have become standard, monitored, and accredited in hospital care.3–6
One of the main challenges in end-of-life care is identifying which patients are approaching the end of their lives. Another challenge is predicting how long the patient will live in the hospital setting, whether days or weeks. The ability to predict the prognosis of a disease and anticipate death is valuable for patients and families. It allows for a focus on patient comfort and well-being and preparation for a peaceful death.4,5 Health professionals benefit from making informed decisions and discussing treatment choices, including withholding combative treatment and care goals. There is a discussion about the cost-efficiency impact of palliative and end-of-life services in healthcare, as these patients often require more emergency services and advanced technologies, leading to social inequality.2,6
In developing countries, especially Muslim countries, there is a complex relationship between death, family devotion, and religious beliefs. Therefore, even in the face of incurable diseases, families still “wait for a miracle”, making palliative and end-of-life care slow to develop in these regions.7–9 Providing an objective, data-driven predictor score, and checklist can ease friction and rejection of terminal care. Earlier intervention can balance patient dignity and family satisfaction with health resource limitations.2–5
Multiple scoring systems are used to measure disease progression and predict hospital mortality in patients with life-threatening illnesses, taking into account acute conditions, catastrophic events, and slow decline. In acute setting, in hospital care in considered as prolong when the patient is admitted for 14 days as prolonged and may impact general quality of care in the hospital.1,5,6 Our primary aim is to assess palliative performance score (PPS), early warning score (EWS) and local rumah sakit Dr Hasan Sadikin (RSHS) score to predict 14 days in-hospital mortality.
Methods
Study Setting, Study Design, and Data Collection
This is a single-center prospective cohort study conducted at a government-owned tertiary referral and teaching hospital in Indonesia with an average of 33,600 patients per year. The study obtained clearance from the Dr Hasan Sadikin Hospital Ethical and Research Committee with the number LB.02.01/X.6.5/430/2022, after approval from the Institutional Review Board. The process of informed consent involved a thorough explanation of the study’s objective, risks, benefits, and alternatives, followed by the signature of either the patient or a family member. The study was conducted from November 2022 to April 2023.
The study involved patients with terminal illnesses, according to WHO5, such as cancer, stroke, chronic kidney disease, or heart failure, who completed a screening form (SFigure 1) upon admission, according to the hospital’s palliative care screening policy. Patients under 18 years old, unable to consent without a guardian present, and those who refused participation were excluded. A loss of follow-up was defined as termination from the study during observation, transfer to another hospital, or the subject leaving against medical advice. A minimum of 104 patients were included in the study, conducted from November 2022 to April 2023. Data was collected via guided interviews using a case report form administered by trained nurses. Information gathered included age, sex, occupation, region of residence, surgical/non-surgical case, care history, pain therapy, primary caregiver, PPS score, modified early warning score (EWS), and Rumah Sakit Dr.Hasan Sadikin (RSHS) palliative score. RSHS palliative score is a local score we have. Patients were followed for 14 days to determine outcome, death, or survival. Data analysis was conducted using IBSS 21. The writing of this manuscript is as follows: The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.10
Results
The total number of participants in this study was 113 patients (Figure 1: Strobe Diagram), whereas previously 13 patients refused to participate in the research, and four were lost to follow-up due to the subject leaving against medical advice.
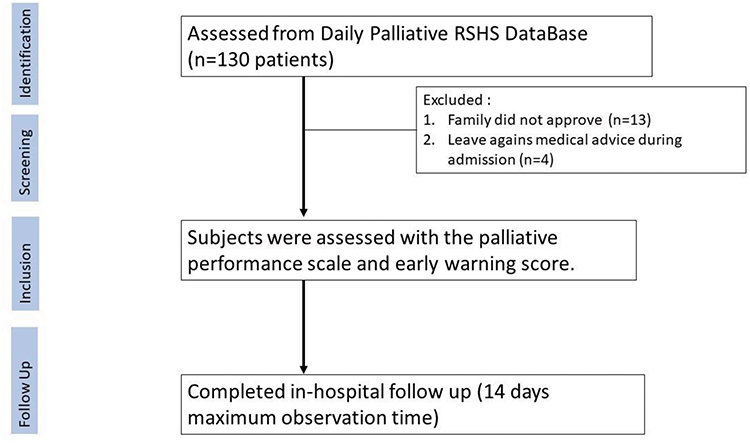 |
Figure 1 The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. |
Out of the 150 participants in the study, 50.4% were female, and 49.6% were male. Most (60.2%) were aged between 31 and 60, while 24.8% were over 60. About 37% of the participants were unemployed, and 43.4% had no income. Only 11.5% of the participants had undergone surgery, while 88.5% had not. Among the participants, 66.4% (75) were diagnosed with cancer. Over two-thirds of participants (66.5%) had been hospitalized in the previous six months, and 27.4% had experienced loss of consciousness. Most participants (81.4%) went home alive, while 18.6% died (Table 1).
 |
Table 1 Subject Demographic |
Data collected from Table 1 underwent statistical analysis to compare different groups based on their outcomes, ie, whether they survived or died. Chi-square and Fisher’s exact tests were used for the study, which revealed significant differences in mortality rates for individuals with cancer, a history of hospitalization within the past six months, and those who experienced a decrease in consciousness during the 14-day observation period. Furthermore, the analysis of predictive scores using Mann–Whitney concluded that there is a significant difference in PPS score, EWS score, and RSHS palliative score between the survivor and non-survivor groups. It was also found that there is no significant correlation between gender, age, occupation, income, and history of surgery concerning the outcomes.
Prognostic determinants of all three scores were identified using logistic regression to establish a cut-off (Figure 2). According to statistical analysis, PPS has a higher AUC value of 0.901 than EWS and RSHS, which have AUC values of 0.772 and 0.761, respectively. All three scores show significant statistical significance with p < 0.0001. PPS is more sensitive in predicting mortality (90.48%) than EWS and RSHS (61.9% and 76.19%, respectively). However, EWS is more specific than PPS and RSHS Palliative Score (84.78% vs 75% vs 65%). The cut-off value for the PPS score is less than or equal to 40 (OR: 16.06, 95% CI: 3.94–65.53), while for EWS, it is above 5 (OR: 5.176, 95% CI: 2.40–11.15), and for RSHS Palliative Score it is greater than 8 (OR: 4.34; 95% CI: 1.71–11.09).
 |
Figure 2 Comparison of survival prediction using logistic regression of Palliative Performance Scale (PPS), Early Warning Score (EWS), and Rumah Sakit Dr.Hasan Sadikin (RSHS) Palliative Score. Legend: AUC: area under curve; CI: confidence interval. |
Cox regression was used (Table 2) to develop a multivariable model. According to the final model results, a decrease in consciousness (HR: 3.6, 95% CI: 1.2–10.22) and EWS (HR: 2.9, 95% CI: 1.1–7.7) were found to be statistically significant in predicting mortality. The survival function of mean covariates (STable 1) revealed that 85.4% of patients survived on day 14, 35.4% survived on day 26, and none of the patients with mean covariates survived on day 40. Upon analyzing the EWS scores, the data exhibits a substantial disparity. Specifically, patients with a score in excess of 5 demonstrated a higher mortality rate on the first day and a more significant decrease on the tenth day compared to those with a score of 5 or less. This finding highlights the criticality of monitoring patients with elevated EWS scores, as they may be at increased risk of adverse outcomes (STable 2).
 |
Table 2 A Multivariate Model of Mortality Predictors |
Discussion
This study is the first to use PPS and EWS in a developing country as a predictive tool for 14 days in-hospital mortality. Additionally, we used our original palliative score, the RSHS palliative score, which was developed for screening patients needing palliative care at our hospital. Due to advancements in patient care and accreditation requirements, hospitals are now required to filter and provide services for end-of-life patients using different protocols and systems.11–14 Predicting a patient’s medical condition and prognosis, especially the likelihood of their death, can be complex. However, it is essential to ensure effective and efficient care.15–17 Objective scores, widely used in the clinical world, can help reduce miscommunication between healthcare providers, patients, and families. In addition, they can help bridge interdisciplinary differences in therapy courses, thereby ensuring that patients receive the best possible care.17–19
During our observation period, it was observed that there was a significant difference between the survivor and non-survivor groups for the presence of cancer and prior admissions to the emergency room in the previous six months. Of the 21 patients who died during the observation period, 19 were cancer patients admitted before (p-value: 0.01 and 0.08). This year, cancer caused almost 10 million deaths globally, accounting for nearly one-sixth of all deaths, similar to WHO findings.19 Since deaths from cancer are now more common than those from cardiovascular disease, mortality from cancer will become the leading cause of death.20,21 Our research has found a significant correlation between cancer diagnosis and the initial admission diagnosis in survivors and non-survivors, which may serve as a useful tool for predicting end-of-life scenarios. It’s important to note that relying solely on these factors may not provide enough accuracy, especially when forecasting mortality within a 14-day timeframe. Therefore, the results of multivariate analysis were not statistically significant (Table 2). Several factors contribute to the complexity of this prediction challenge. As a multifaceted disease with varying stages, treatments, and outcomes, cancer presents a diverse landscape of patient experiences. Moreover, while reflecting a patient’s initial condition, the admission diagnosis may not capture subsequent developments or complications that can impact the prognosis. Furthermore, predicting imminent death within a 14-day window is highly intricate and influenced by many variables, including comorbidities, treatment responses, and individual patient trajectories.4,5,19–21
Our study discovered that the cut-off values were a PPS score below 40 and an EWS score of 5. This study found that the local score used to screen patients who required support from the palliative care team resulted in a score of 8, which was linked with a higher risk of in-hospital death. Interestingly, the previous score used to predict death was 7; hence, this finding may change how we interpret this score when analyzing past data.
Another study has shown that the PPS score significantly predicts mortality (p < 0.001). However, our study differs in terms of the observation period, which was 14 days, compared to the six months in the previous studies where findings indicate that if the PPS scores are below 20, the mortality rates are 96%.22 Another study found that patients with cancer and non-cancer illnesses died within 14 days (days 2–13), but the proportion was lower, and most patients died after 30 days of care.23 PPS might be relevant in predicting survival in terminally ill patients with cancer, although the time to death could be studied further.24–27 Hence, we conclude that the severity of admission, as measured by the EWS, is more relevant to predicting short-term death since it reflects the acute state of the patient’s current condition regardless of its chronic illness state.
It is crucial to note that relying solely on PPS to predict 14-day mortality has a low specificity rate of only 75%. This means there is a higher likelihood of obtaining “false positive” results. In clinical practice, it is essential to recognize that over-reliance on PPS may cause unnecessary anxiety and distress for distraught patients and their families.2–5 it may lead to underutilizing inappropriate medical treatments.
EWS for inpatient risk stratification has been identified to predict death in patients with and without infection and is currently the standard model in many accreditation systems for risk stratification programs.3–6,28 Our research has shown that a score of 5 or higher is linked with death (p = 0.031) and a decrease in consciousness (p = 0.017). This decrease in consciousness is a component of EWS and is a strong indicator. These findings are consistent with previous studies, which have identified a slightly higher score of ≥7 points as the cut-off point. At this score, the 24-hour mortality rate increased from 1.8% for a NEWS score of ≥3 to 7.8% for a NEWS score of ≥7.28 This result is likely due to the availability and promptness of intervention for higher EWS, which requires further study to assess our center’s effectiveness in managing increasing EWS scores since many studies reported that many aspects of the EWS such as decrease of consciousness, blood pressure and saturation can be managed quickly to improve outcome.29–31
Our study has an important point to consider for general applicability, specifically regarding the 14-day-study period. It is comparatively shorter than other studies, which may not accurately reflect the required mortality rates in different perspectives, such as 30-day or in-hospital mortality. However, our analysis (STable 1 and STable 2) indicates that patients with analyzed covariates may not survive beyond day 40 after their first admission.
End-of-life care, a profoundly sensitive and complex aspect of healthcare, varies significantly across different countries, each guided by its unique set of cultural, ethical, and legal frameworks. In the UK, the Gold Standards Framework provides comprehensive guidance to support the delivery of high-quality end-of-life care. This framework emphasizes personalized care plans, clear communication, and coordinated support across different healthcare settings using different scores and predictive tools.15,32
In contrast, the United States approaches end-of-life care with a focus on advanced directives, patient autonomy, and various assessment frameworks. The use of the Palliative Performance Scale (PPS) forms are pivotal in assessing patient needs and documenting care preferences. This emphasis on living wills and healthcare proxies allows individuals to make decisions about their care in advance, reflecting the value placed on individual rights and autonomy in American society.18,21
Our study stands out as it promotes the adoption of an early warning score (EWS) as the initial tool for assessing the risk of end-of-life. Although other standards have been discussed, they are not commonly used in our center. On the other hand, EWS is already widely recognized and utilized by hospital staff according to Indonesian and International accreditation standards. Our study, therefore, builds upon the existing practices within our hospital and represents a natural progression towards them.
Our study exhibits several limitations that warrant careful consideration. Firstly, we acknowledge the absence of our assessment of the direct impact of the intervention on patient outcomes, which represents a notable gap in our research. It is crucial to recognize that interventions, particularly in healthcare settings, have the potential to influence patient outcomes significantly. The absence of this measurement might introduce an element of uncertainty in interpreting our study’s results. Moreover, the inherent variability in the quality of care across different healthcare centers is a prominent limitation. The diverse standards of care, expertise, and resources available at each center can introduce variability in patient experiences and outcomes. This heterogeneity must be taken into account when interpreting our findings. While our study provides valuable insights into the general trends and associations, it is essential to exercise caution when generalizing the results to diverse healthcare settings. When making decisions about end-of-life care, it’s important to consider more than just cost efficiency or length of hospital stay. It’s crucial to have structured and objective discussions about end-of-life care while always prioritizing the mental health and needs of both the patient and their family.15,17,18,21,34 Therefore, relying solely on a single predictor score is not ethical or suitable if not applied with compassion and empathy.
Conclusion
Decreased consciousness and Early Warning Score are statistically significant predictors of in-hospital mortality. We stress the importance of using a combination of predictors instead of relying on a single indicator to predict death and improve patient care.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work the author(s) used [Grammarly service] in order to [correct English language and uniform style of writing]. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.
Ethical Declaration
The author ensures that this study is conducted in accordance with the principles outlined in the Declaration of Helsinki.
Acknowledgments
We want to acknowledge the contributions of Ms. Dewi Lusiana, Ms. Nita Mulyantini, Ms. Elli Br Sitepu, Ms. Nining Saritesa Hidayat, and who provided on the ground support for this paper. We salute the palliative care team, led by Dr. Gatot, including Dr. Ade, Dr. Yanti, Ms. Tere, Ns Meitha, and other dedicated members. Despite limitations and difficulties, the RSHS team is committed to achieving peaceful deaths for patients.
Author Statement
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from funding agencies in public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Ngantcha M, Le-Pogam MA, Calmus S, et al. Hospital quality measures: are process indicators associated with hospital standardized mortality ratios in French acute care hospitals? BMC Health Serv Res. 2017;17:578. doi:10.1186/s12913-017-2534-
2. Hillman K. Dying safely. Int J Qual Health Care. 2010;22:339–340. doi:10.1093/intqhc/mzq045
3. National Health Service. End of Life Care Strategy. Promoting high quality care for all adults at the end of life. July. Secondary End of Life Care Strategy. Promoting high quality care for all adults at the end of life; 2008. Available from: http://webarchive.nationalarchives.gov.uk/20130107105354/http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_086345.pdf.
4. The Scottish Government. Living and dying well: building on progress. Secondary living and dying well: building on progress 2011. Available from: http://www.scotland.gov.uk/Resource/Doc/340076/0112559.pdf.
5. World Health Organization. Palliative care: key. facts; 2020. Available form: https://www.who.int/news-room/fact-sheets/detail/palliative-care.
6. The Ministry of Health of Indonesia. Hospital Accreditation Standard, (pp.268–269), The Ministry of Health of Indonesia, Jakarta-Indonesia; 2022.
7. Nafratilova M, Allenidekania A, Wanda D. Still hoping for a miracle: parents’ experiences in caring for their child with cancer under palliative care. Indian J Palliat Care. 2018;24(2):127. doi:10.4103/IJPC.IJPC_195_17
8. Abdullah R, Guo P, Harding R. Preferences and experiences of Muslim patients and their families in Muslim-majority countries for end-of-life care: a systematic review and thematic analysis. J Pain Sympt Manage. 2020;60(6):1223–1238. doi:10.1016/j.jpainsymman.2020.06.032
9. Alam N, Hobbelink EL, van Tienhoven AJ, van de Ven PM, Jansma EP, Nanayakkara PW. The impact of the use of the Early Warning Score (EWS) on patient outcomes: a systematic review. Resuscitation. 2014;85(5):587–594. doi:10.1016/j.resuscitation.2014.01.013
10. Poorolajal J, Cheraghi Z, Irani AD, Rezaeian S. Quality of cohort studies reporting post the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. Epidemiol Health. 2011;3:33.
11. Akdemir N, Peterson LN, Campbell CM, Scheele F. Evaluation of continuous quality improvement in accreditation for medical education. BMC med educ. 2020;20:1–6. doi:10.1186/s12909-020-02124-2
12. Cotogni P, Saini A, De Luca A. In-hospital palliative care: should we need to reconsider what role hospitals should have in patients with end-stage disease or advanced cancer? J Clin Med. 2018;7(2):18. doi:10.3390/jcm7020018
13. Luo L, Du W, Chong S, Ji H, Glasgow N. Patterns of comorbidities in hospitalised cancer survivors for palliative care and associated in-hospital mortality risk: a latent class analysis of a statewide all-inclusive inpatient data. Palliat Med. 2019;33(10):1272–1281. doi:10.1177/0269216319860705
14. Devery K, Winsall M, Rawlings D. Teams and continuity of end-of-life care in hospitals: managing differences of opinion. BMJ Open Qual. 2022;11(2):e001724. doi:10.1136/bmjoq-2021-001724
15. Thomas K, Armstrong-Wilson J, Clifford C. The Gold Standards Framework hospital programme: implementation and progress. Int J Palliat Nurs. 2022;28(4):172–177. doi:10.12968/ijpn.2022.28.4.172
16. Leonhardt KK Joint Commission International
17. Wright AA, Zhang B, Ray A, et al. Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment. JAMA. 2008;300:1665–1673. doi:10.1001/jama.300.14.1665
18. Cardona-Morrell M, Hillman K. Development of a tool for defining and identifying the dying patient in hospital: criteria for Screening and Triaging to Appropriate aLternative care (CriSTAL). BMJ Support Palliat Care. 2015;5(1):78–90. doi:10.1136/bmjspcare-2014-000770
19. World Health Organization. Cancer; 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/cancer#:~:text=Cancer%20is%20a%20leading%20cause,and%20rectum%20and%20prostate%20cancers.
20. Dagenais GR, Leong DP, Rangarajan S, Lanas F, Lopez-Jaramillo P, Gupta R. Variations in common diseases, hospital admissions, and deaths in middle-aged adults in 21 countries from five continents (PURE): a prospective cohort study. Lancet. 2019;395:10226.
21. Harrold JE, Carroll JT, McGrath J, Morales K, Kapo J, Casarett D. Is the palliative performance scale a useful predictor of mortality in a heterogeneous hospice population? J Palliat Med. 2005;8(3):503–509. doi:10.1089/jpm.2005.8.503
22. Prompantakorn P, Angkurawaranon C, Pinyopornpanish K, et al. Palliative Performance Scale and survival in patients with cancer and non-cancer diagnoses needing a palliative care consultation: a retrospective cohort study. BMC Palliat Care. 2021;20(74). doi:10.1186/s12904-021-00773-8
23. Smith MEB, Chiovaro JC, O’Neil M, et al. Early warning system scores for clinical deterioration in hospitalized patients: a systematic review. Ann Am Thoracic Soc. 2014;11(9):1454–1465. doi:10.1513/AnnalsATS.201403-102OC
24. Holland M, Kellett J. A systematic review of the discrimination and absolute mortality predicted by the National Early Warning Scores according to different cut-off values and prediction windows. Eur J Intern Med. 2022;98:15–26). doi:10.1016/j.ejim.2021.12.024
25. Baik D, Russell D, Jordan L, Dooley F, Bowles KH, Creber RMM. Using the palliative performance scale to estimate survival for patients at the end of life: a systematic review of the literature. J Palliat Med. 2018;21(11):1651–1661. doi:10.1089/jpm.2018.0141
26. Yoon SJ, Choi SE, Suh SY. Palliative performance scale score at 1 week after palliative care unit admission is more useful for survival prediction in patients with advanced Cancer in South Korea. Sage J. 2018;35:9).
27. Medeiros RB, Stamm AMNF, Moritz RD, Freitas PF, Kretzer LP, Gomes JV. Serial palliative performance scale assessment in a university general hospital: a pilot study. J Palliat Med. 2018;21(6):842–845. doi:10.1089/jpm.2017.0412
28. Liu VX, Lu Y, Carey KA, et al. 2020, comparison of early warning scoring systems for hospitalized patients with and without infection at risk for in-hospital mortality and transfer to the intensive care unit. JAMA Network Open. 2020;3(5):e205191. doi:10.1001/jamanetworkopen.2020.5191
29. Gerry S, Bonnici T, Birks J, et al. Early warning scores for detecting deterioration in adult hospital patients: systematic review and critical appraisal of methodology. BMJ. 2020;369. doi:10.1136/bmj.m1501
30. Alotaibi AS, Mahroos RA, Al Yateem SS, Menezes RG. Central nervous system causes of sudden unexpected death: a comprehensive review. Cureus. 2022. doi:10.7759/cureus.20944
31. Jones D, Moran J, Winters B, et al. The rapid response system and end-of-life care. Curr Opin Crit Care. 2013;19:616–623.
32. Shaw KL, Clifford C, Thomas K, Meehan H. Improving end-of-life care: a critical review of the Gold Standards Framework in primary care. Palliat Med. 2010;24(3):317–329. doi:10.1177/0269216310362005
33. Oshima Lee E, Emanuel EJ. Shared decision making to improve care and reduce costs. N Engl J Med. 2013;368:6–8. doi:10.1056/NEJMp1209500
34. Rosenwax LK, McNamara BA, Kevin murray K, et al. Hospital and emergency department use in the last year of life: a baseline for future modifications to end-of-life care. Med J Aust. 2011;194:570–573. doi:10.5694/j.1326-5377.2011.tb03106.x
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.