")
Back to Journals » Infection and Drug Resistance » Volume 17
Nosocomial Infections After Pediatric Congenital Heart Disease Surgery: Data from National Center for Cardiovascular Diseases in China
Authors Wang X, Li S, Huo D, Zhu Z, Wang W, He H, Zhang Q, Li J, Wang X
Received 4 January 2024
Accepted for publication 23 April 2024
Published 26 April 2024 Volume 2024:17 Pages 1615—1623
DOI https://doi.org/10.2147/IDR.S457991
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Xiaofeng Wang,1,2,* Shuo Li,3,* Da Huo,4,* Zhiyuan Zhu,1,2,* Wenlong Wang,1,2 Hongxia He,1,2 Qian Zhang,1,2 Jiantao Li,2,5 Xu Wang1,2
1Department of Pediatric Intensive Care Unit, National Center for Cardiovascular Disease and Fuwai Hospital, Beijing, People’s Republic of China; 2School of Clinical Medicine, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 3Department of Infection Control, Peking University First Hospital, Beijing, People’s Republic of China; 4Institute for Infectious Disease and Endemic Disease Control, Beijing Center for Disease Prevention and Control, Beijing, People’s Republic of China; 5Department of Infection Control, National Center for Cardiovascular Disease and Fuwai Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xu Wang, Department of Pediatric Intensive Care Unit, National Center for Cardiovascular Disease and Fuwai Hospital, No. 167 North Lishi Road, Xicheng District, Beijing, 100037, People’s Republic of China, Email [email protected]
Purpose: Infection prevention and control (IPC) has a significant impact on the prognosis after pediatric cardiac surgery. This study aimed to provide surveillance data on the incidence and density of various infections during the COVID-19 epidemic and explore the influence of multi-drug resistant organisms (MDRO) on in-hospital prognosis after congenital heart disease surgery.
Methods: This single-center retrospective study included pediatric patients who underwent cardiac surgery between 2021 and 2022. The results of the postoperative bacterial and fungal cultures and antimicrobial stewardship were collected. The demographic characteristics (age and weight), operation-related parameters (RACHS-1 grade, duration of cardiopulmonary bypass, and aortic cross clamp), and surgical outcomes (extracorporeal membrane oxygenation, delayed sternal closure, mortality, duration of mechanical ventilation, length of intensive care unit stay and hospital stay, and hospitalization costs) of MDRO and non-MDRO patients were compared.
Results: A total of 4776 patients were included. There were 101 infectious culture results after the operation, with a nosocomial infection rate of 2.1%. There were 40 MDRO specimens from 36 patients, 50 non-MDRO specimens from 30 patients, and 11 fungal specimens from 10 patients. The incidence of pneumonia was 1.5%, with a ventilator-associated pneumonia incidence density of 7.2/1000 patient-days. The incidence of sepsis was 0.4%, with a catheter-related bloodstream infection incidence density of 0.24/ 1000 patient-days. The incidence density of catheter-associated tract infection was 0.45/ 1000 patient-days. The incidence of surgical site infection was 0.06%. The culture proportion before commencing antibiotics was 93% and the antibiotic consumption intensity was 30.7 DDD/100 bed-days. The length of intensive care unit stay in MDRO infection patients increased compared with that in non-MDRO infection patients, 30 (18,52) vs 17 (7,62) days, p=0.05).
Conclusion: The IPC performance of Fuwai Hospital achieved satisfactory results. MDRO infection can lead to prolonged intensive care unit stay.
Plain Language Summary: Developed countries have advanced infection prevention and control systems and comprehensive postoperative infection monitoring data for congenital heart disease. While developing countries have initiated efforts in infection prevention and control, global attention remains substantial. This study aimed to provide comprehensive infection surveillance data and identify possible implementation for further improvement in the National Center for Cardiovascular Diseases in China (Fuwai Hospital).
This was a retrospective single-center study. We included pediatric patients who underwent cardiac surgery at a pediatric surgical center between 2021 and 2022, with an age limit of 14 years. Exclusion criteria included patients undergoing medical therapy, interventional therapy, or surgical therapy in other centers in Fuwai Hospital.
This study, for the first time, reports the incidence of comprehensive healthcare-associated infection surveillance and targeted surveillance (encompassing device-associated infection, surgical site infection, and multi-drug resistant organisms) after pediatric cardiac surgery at the National Center for Cardiovascular Diseases in China. In addition, we report the data on antimicrobial stewardship. We compared the surgical outcome and hospitalization costs between patients with multi-drug resistant organism infection and those without multi-drug resistant organism infection and found that multi-drug resistant organism infection can lead to prolonged intensive care unit length of stay.
The Fuwai Hospital achieved satisfactory infection prevention and control results. However, because China is a large developing country exhibiting notable variations in medical conditions across its diverse regions, prospective, multicenter, observational studies should be carried out for future research based on existing evidence.
Keywords: nosocomial infections, pediatric cardiac surgery, multidrug-resistant organism, surgical outcomes
Introduction
Congenital heart disease is the most common congenital malformation, with an overall incidence of 1%.1 Approximately 70,000 patients with congenital heart disease undergo annual surgical treatment.2 All patients require postoperative care in the intensive care unit (ICU). Many factors affect postoperative recovery, and the level of infection prevention and control (IPC) is very important.3,4 To achieve the best IPC performance, it is necessary to build an IPC system, which is a complex systematic profession.
Developed countries have advanced IPC systems and comprehensive postoperative infection monitoring data for congenital heart disease. Pasquali SK and colleagues,5 utilizing data from the STS Congenital Heart Surgery Database and Pediatric Health Information System for 32,856 patients across 28 centers from 2006 to 2010, reported a postoperative infection rate of 3.7%. Significant variations existed among hospitals, ranging from 0.9% to 9.8%. Kansy et al,6 drawing data from the STS Congenital Heart Surgery Database from 1995 to 2010 including 6314 patients, identified 197 cases (3.1%) with significant infections (3% sepsis, 0.015% infective endocarditis, and 0.09% mediastinitis). Using data from the Vizient Clinical Database/Resource Manager from 2013 to 2015, Haughey et al7 reported the incidence of catheter-related bloodstream infections after congenital heart disease surgery. This study included 1386 neonatal and 2913 infant patients, with an incidence of 1.5% in neonates and 0.8% in infants.
While developing countries have initiated efforts in IPC, global attention remains substantial. According to Chau NT and colleagues,4 who analyzed data from the International Quality Improvement Collaborative Group spanning 2010 to 2012, involving 27 regions from 16 developing countries, a total of 14,545 patients were included. Among them, 793 cases (5.5%) experienced bacterial sepsis and 306 (2.1%) had surgical site infections. Murni IK and colleagues8 conducted a literature review of infection data from high-income and middle-to-low-income countries. In high-income countries, the postoperative infection rate ranged from 1.2% (12/981) to 48% (22/46). Postoperative bacteremia rates varied from 1.5% (15/992) to 10.2% (12/127), and the incidence of fungal infections or invasive candidiasis ranged from 0.4% (6/1540) to 5.9% (10/169). Concerning pulmonary infections, the postoperative pneumonia rate in infants was 6.2% (8/127), with a ventilator-associated pneumonia incidence density of 17.1/1000 patient-days. In middle-to low-income countries, the incidence of postoperative infections varies widely. The incidence ranges from 7.8% to 40% for overall postoperative infections, 7% to 21% for postoperative sepsis in neonates, and 2.5% to 12.7% for surgical site infections. The incidence of candidemia was 0.07%. The postoperative pneumonia rates vary from 21% to 44%, and the incidence of ventilator-associated pneumonia ranges from 6.2% to 18.3%. The incidence of catheter-related urinary tract infections was 7%.
China also provides congenital heart disease postoperative IPC data for CHDs. In a single-center study conducted from 2012 to 2018, Yu et al9 reported a nosocomial infection (NIs) rate of 10.8% among 11,651 pediatric patients. Another single-center study conducted by Ren C and colleagues10 from 2012 to 2017 with 2171 patients revealed that 708 patients experienced pulmonary infections, resulting in an incidence of 32.6%.
Notably, these data suggest that IPC results in China lagged behind those in developed countries during that period. However, the past three years of the COVID-19 epidemic have witnessed tremendous developments in IPC management in China.11 Because NIs surveillance serves as the cornerstone of IPC management, our study aimed to provide comprehensive surveillance data on the incidence and density of various infections and antimicrobial stewardship (AMS) during the COVID-19 epidemic to facilitate implementation of IPC measures and AMS bundles in the next step. Moreover, owing to the current lack of research on the effect of multi-drug resistant organisms (MDRO) on the in-hospital prognosis of pediatric cardiac surgery patients, our study compared the demographic characteristics, operation-related parameters, and surgical outcomes of MDRO and non-MDRO patients to determine the effect of MDRO infection on postoperative prognosis.
Methods and Materials
Inclusion and Exclusion Criteria
This retrospective, single-center study was conducted at the National Center for Cardiovascular Diseases in China (Fuwai Hospital).
The inclusion criteria were as follows: (1) pediatric patients with an age limit of 14 years. 2) Patients who underwent cardiac surgery at the pediatric surgical center between 2021 and 2022. The exclusion criteria were as follows: 1) patients undergoing medical therapy only, 2) patients undergoing interventional therapy only, and 3) patients undergoing surgical therapy at another center in the Fuwai hospital.
Diagnostic Criteria for Specific Infections
Postoperative pneumonia diagnostic criteria12 include the presence of new or progressive pulmonary infiltration accompanied by infectious symptoms and signs (such as newly developed fever, purulent sputum, increased white blood cell count, decreased oxygenation, and changes in respiratory mechanics) with positive respiratory tract culture results.
Ventilator-associated pneumonia diagnostic criteria12 include the presence of new or progressive pulmonary infiltration accompanied by infectious symptoms and signs (such as newly developed fever, purulent sputum, increased white blood cell count, decreased oxygenation, and changes in respiratory mechanics), and positive respiratory tract culture results in patients ventilated for ≥48 hours.
The sepsis diagnostic criteria:13 positive blood culture results accompanied by low blood pressure, tachycardia, fever, increased white blood cell count, signs of shock (such as cold and cyanotic skin), and signs of organ dysfunction (such as oliguria, acute kidney injury, and altered mental status).
Catheter-related bloodstream infection diagnostic criteria:14 patients with vascular catheters in place or those who had catheters removed within 48 h of bacteremia or fungemia, accompanied by fever (T > 38 °C), chills, hypotension, and at least one positive result from peripheral venous blood culture, with no other clear source of infection except the catheter.
Catheter-associated urinary tract infection diagnostic criteria:15 patients with catheters in place or those who had catheters removed within 48 hours, exhibiting signs and symptoms consistent with urinary tract infection or systemic infection and not explainable by other causes, with positive urine culture.
Surgical site infection diagnostic criteria:16 Within 30 days after the surgical procedure, the wound showed signs of redness, swelling, heat, and poor healing, with positive cultures.
Determination of contamination/colonization: Whether in sterile or non-sterile sites, if the culture result is positive without accompanying infection-related manifestations, contamination was considered and not included in the infection statistics. If common colonizing organisms are cultured in non-sterile sites without infection-related manifestations, colonization is considered and not included in the infection statistics.
Multi-drug resistant organisms (MDRO) mainly include methicillin-resistant staphylococcus aureus/staphylococcus epidermidis, carbapenem-resistant Enterobacteriaceae, carbapenem-resistant Acinetobacter baumannii, carbapenem-resistant pseudomonas aeruginosa, vancomycin-resistant enterococcus, and extended-spectrum beta-lactamases.
Data Collection
Postoperative bacterial and fungal culture results, along with drug resistance results, were collected from the medical records and infection control system. The infection rate was expressed as a percentage (%) and calculated as the number of positive cultures related to infection divided by the total number of patients. Device-associated infections were expressed as infection intensity (per 1000 patient-days), calculated as the number of related infection cultures divided by the number of days the patient used the device, multiplied by 1000%. The parameters related to antimicrobial stewardship included antibiotic consumption intensity (DDD/100 bed-days), rate of antibiotic prophylaxis withdrawal in patients receiving cardiac operations within 48 h, and the rate of culture before commencing antibiotics (%).
For all patients, the demographic characteristics (age and weight), surgery-related indicators (RACHS-1 grade, duration of cardiopulmonary bypass, and duration of aortic cross clamp), surgical outcomes (Extracorporeal Membrane Oxygenation assistance, delayed sternal closure, mortality, duration of mechanical ventilation, ICU length of stay (LOS), total LOS, and hospitalization costs) were collected from the medical records system and databases.
Statistical Analysis
All statistical analyses were performed using SPSS 25.0 (IBM Corp., Armonk, NY, USA). The expectation-maximization method was employed to estimate missing data. The Shapiro–Wilk test was used to assess the conformity of the continuous variables to the normal distribution. Normal distribution was expressed as the mean plus or minus the standard deviation, while non-normal distribution was expressed as the median accompanied by the interquartile range. Categorical variables are displayed in a numerical form, accompanied by their respective percentages. An independent t-test was used for normally distributed continuous variable analysis. Otherwise, the Wilcoxon rank-sum test was used for nonnormally distributed variables. Categorical variables were analyzed using the chi-squared test and Fisher’s exact test. Statistical p-value ≤0.05.
Ethical Review
Approval was obtained from the Fuwai Hospital Ethics Committee in 2022 (ID: 2022–1859. The ethical principles followed the 1975 Declaration of Helsinki. This was a retrospective analysis based on anonymized data collected for routine clinical care and administrative purposes; therefore, the requirement for individual informed consent was waived.
Results
There are 5903 pediatric patients in the pediatric ICU between 2021–2022. After excluding patients undergoing medical therapy, interventional therapy, and surgical therapy in other center (1127 cases in total), 4776 pediatric patients were included in this study.
Following the exclusion of 131 community infection specimens and 29 colonization/contamination specimens, 101 positive postoperative culture results were obtained, indicating an NIs rate of 2.1%. Among these, 40 MDRO cultures were identified in 36 patients, 50 non-MDRO cultures in 30 patients, and 11 fungal cultures in 10 patients. The clinical data of the patients with MDRO and non-MDRO infections are shown in Table 1. The clinical data of patients with fungal infections are shown in Table 2. Details of the infection sites, microbial types, and drug resistance are shown in Table 3.
 |
Table 1 The Clinical Data Between Patients with MDRO and Non-MDRO Infections |
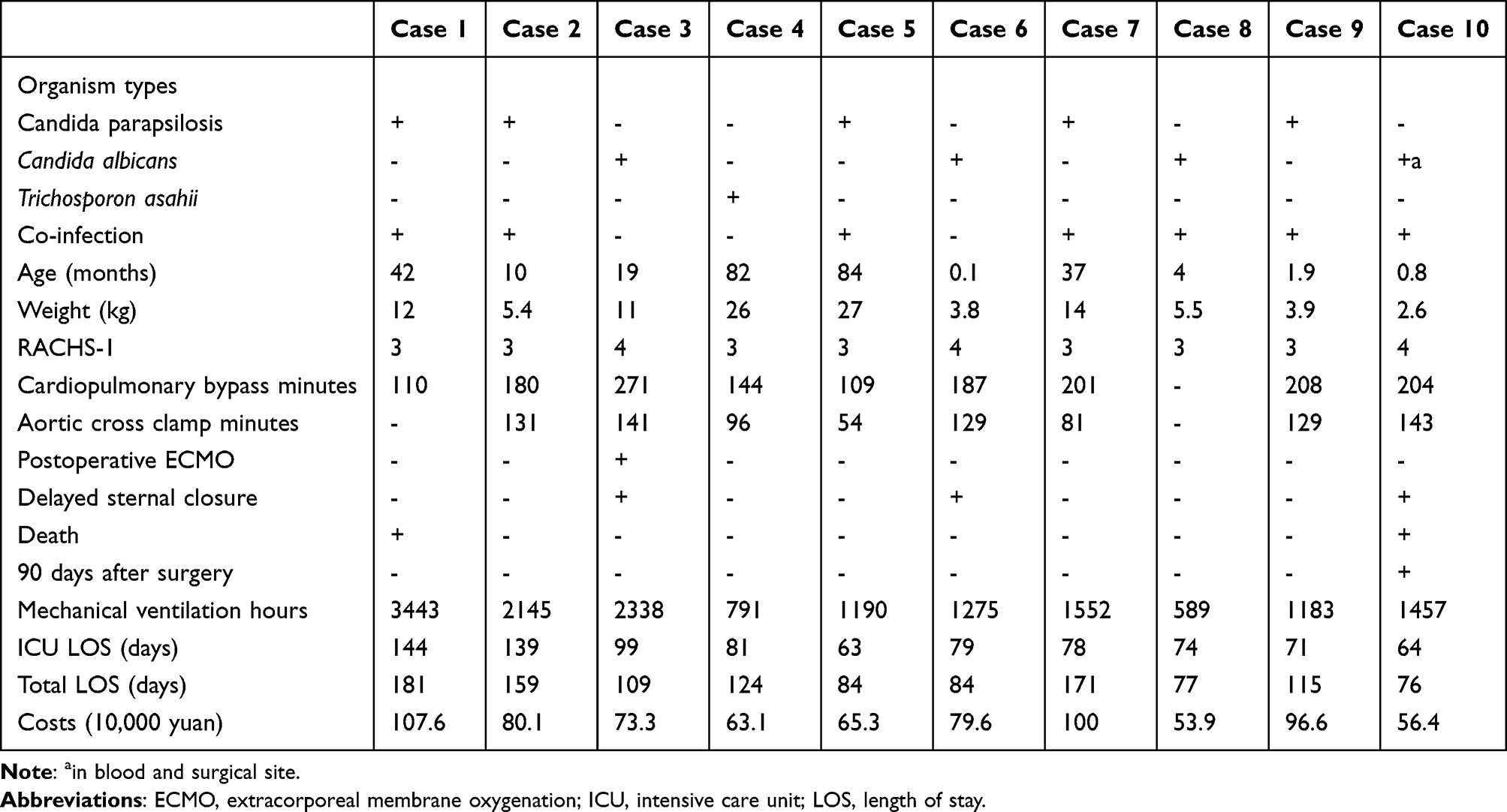 |
Table 2 The Clinical Data of Patients with Fungus Infections |
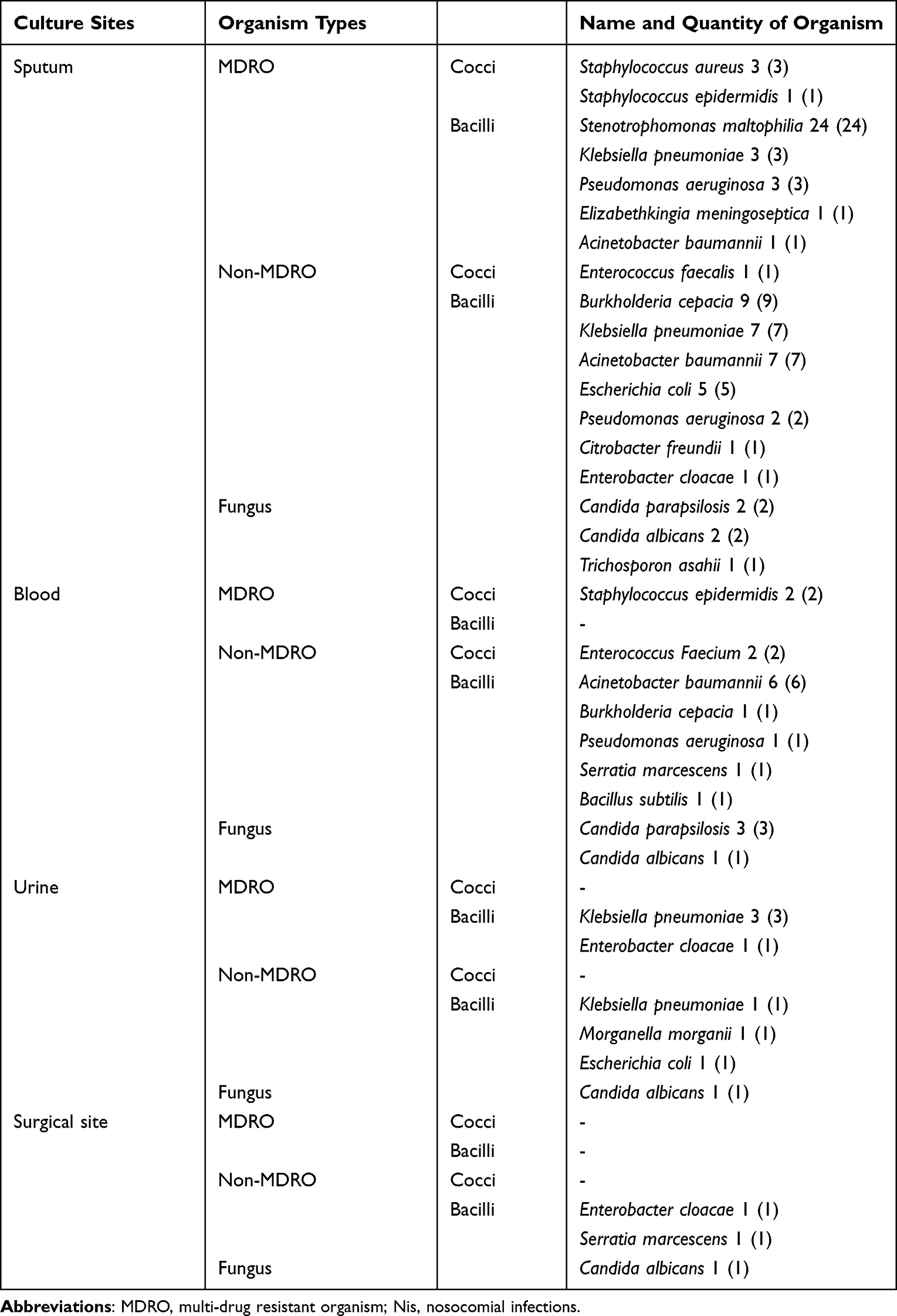 |
Table 3 The Details of NIs Sites, Microbial Types and Drug Resistance |
The postoperative nosocomial pneumonia, sepsis rate was 0.4% and surgical site infection rates were 1.5%, 0.4%, and 0.06%, respectively. The infection intensity was 7.2 /1000 patient-days for ventilator-associated pneumonia, 0.24/1000 patient-days for catheter-related bloodstream infections, and 0.45/1000 patient-days for catheter-associated urinary tract infections.
In terms of antimicrobial stewardship, the rate of culture before commencing antibiotics was 93% and the antibiotic consumption intensity was 30.7 DDD/ 100 bed-days. In China, the goal of antibiotic prophylaxis in patients undergoing cardiac operations is within 48 hours after the end of the operation; however, the actual compliance rate was only 8.5%.
The demographic characteristics, surgery-related indicators, postoperative mortality rates, mechanical ventilation hours, total LOS, and hospitalization costs between patients with postoperative MDRO infections (n=36) and those without MDRO infections (n=30) showed no statistically significant differences (p>0.05). However, there was an increase in pediatric ICU stay in patients with MDRO infections (30 (18,52) vs 17 (7,62) days, p=0.05). The details of the clinical data comparisons are shown in Table 2.
Discussion
During the COVID-19 pandemic, Fuwai Hospital strengthened the IPC system in comprehensive aspects, such as the performance of infection control departments, NIs surveillance, implementation of IPC measures, and antimicrobial stewardship. Among these, NIs surveillance is the cornerstone. Our pediatric ICU actively receives relative cultures from all patients with signs of infection. Based on the NIs surveillance data provided in this study, the overall rate of NIs was 2.1%, nosocomial pneumonia was 1.5%, sepsis rate was 0.4%, surgical site infection rate was 0.06%, infection intensity was 7.2 /1000 patient-days for ventilator-associated pneumonia, 0.24/1000 patient-days for catheter-related bloodstream infection, and 0.45/1000 patient-days for catheter-associated urinary tract infections, all of which suggest that, in our center, IPC performance has reached the standards of developed countries.9
However, through data analysis, we found some methods for further improvement. The intensity of ventilator-associated pneumonia in our center was relatively high. Although this is likely associated with delayed recovery in critically ill patients requiring prolonged mechanical ventilation for complex congenital heart disease, there is still room for improvement. In addition to the current bundle implementation, such as hand hygiene, early extubation, chlorhexidine oral care, head of the bed elevated about 30–45 degree, maintaining cuff pressure in endotracheal tubes, reducing sedation, preventing gastric distension, and preventing deep vein thrombosis, future efforts could explore the addition of nebulized inhalation of antimicrobial drugs to reduce the incidence of ventilator-associated pneumonia.17
Regarding MDRO, the proportion of gram-negative bacteria currently exceeds that of gram-positive cocci, aligning with the prevailing trend of MDRO in the ICU.18 At our center, we have not yet identified vancomycin-resistant Enterococcus. This trend emphasizes the need for heightened attention when selecting antimicrobial drugs for congenital heart disease surgery. However, there is a relatively high proportion of Stenotrophomonas maltophilia, possibly because of the empirical use of broad-spectrum antibiotics in critically ill conditions after complex congenital heart disease surgery. To solve this problem, it is important to obtain relevant cultures before commencing antibiotics and de-escalate or discontinue antimicrobial drugs based on culture results.19
When comparing patients with and non-MDRO infection, there was no statistically significant difference in the demographic characteristics and surgery-related indicators between the two groups. However, differences were observed in terms of the surgical prognosis. Notably, patients with MDRO infection had an increased ICU-LOS compared to those without MDRO infection (30 (18, 52) vs 17 days (7, 62), p=0.05). Mortality, mechanical ventilation hours, total LOS, and hospitalization costs showed no statistically significant differences between the two groups. This result highlights the need to strengthen the IPC of MDRO (antimicrobial stewardship and IPC measures) after surgery20 to improve surgical outcomes.
In the results of antimicrobial stewardship at our center, the culture proportion before commencing antibiotics was 93%, and the antibiotic consumption intensity was 30.7 DDD/100 bed-days. These results meet the national antimicrobial stewardship standards in China.21 However, the actual compliance rate for antibiotic prophylaxis withdrawal in patients undergoing cardiac operations within 48 h was very poor (only 8.5%). In the future, it will be necessary to strengthen the AMS measures and standardize the application of antibacterial drugs.
In terms of bundled IPC measures, our pediatric ICU has implemented single-room isolation, hand hygiene, environmental hygiene, wearing gloves when caring for patients, and wearing protective clothing at risk of contamination. In the future, additional measures such as preoperative active screening22 and postoperative daily chlorhexidine bathing23 could be considered to further enhance IPC measures for MDRO infection.
In terms of fungal infections, statistical analysis was not performed due to the small number of cases, and 70% of them had a co-infection status. However, based on the current trend, due to the high mortality of patients with fungal infections (20%), the long LOS (112 days in median), and the high cost of hospitalization (764,500 CNY in median, approximately $113,500 at the exchange rate in 2022), early and proper antifungal prophylaxis and treatment with combined multidrug therapy are needed to reduce mortality and morbidity.24
Study limitations
Although this study provided detailed infection monitoring data, due to the limited sample size and the low positive rate of infection after surgery, the sample size was relatively insufficient when comparing the prognosis of infected patients. In the future, we will continue to expand the sample size and conduct research on the risk factors for postoperative infections.
Conclusion
The IPC performance of Fuwai Hospital achieved satisfactory results. In the future, it will be necessary to strengthen the AMS measures and standardize the application of antibacterial drugs. Gram-negative bacteria are the most common type of MDRO. Infection with MDRO can lead to prolonged ICU-LOS in pediatric cardiac surgery patients. Fungal infections may radically influence morbidity and mortality rates.
Data Sharing Statement
All the data collected for the study, including individual participant data (only deidentified individual participant data will be shared), a data dictionary defining each field in the set, and related documents such as study protocol and statistical analysis results, will be made available to others with publication by Email addresses with the consent of the corresponding author.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Clinical Research Foundation of the National Health Commission of the People’s Republic of China (grant number 2022-GSP-GG-32) and Research Foundation of Artificial Intelligence and Information Application (grant number: 2022-IT02).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
This paper has been uploaded to SSRN as a preprint (https://papers.ssrn.com/sol3/papers.cfm?abstract_id=4657436). This paper is not currently under consideration with any other journal or publisher.
References
1. Tennant PW, Pearce MS, Bythell M, Rankin J. 20-year survival of children born with congenital anomalies: a population-based study. Lancet. 2010;35(9715):649. doi:10.1016/S0140-6736(09)61922-X
2. Ma K, He Q, Dou Z, et al. Current treatment outcomes of congenital heart disease and future perspectives. Lancet Child Adolesc Health. 2023;7(7):490–501. doi:10.1016/S2352-4642(23)00076-7
3. Kollef MH, Torres A, Shorr AF, Martin-Loeches I, Micek ST. Nosocomial Infection. Crit Care Med. 2021;49(2):169–187. doi:10.1097/CCM.0000000000004783
4. Sen AC, Morrow DF, Balachandran R, et al. Postoperative Infection in Developing World Congenital Heart Surgery Programs: data From the International Quality Improvement Collaborative. Circ Cardiovasc Qual Outcomes. 2017;10(4):e002935. doi:10.1161/CIRCOUTCOMES.116.002935
5. Pasquali SK, He X, Jacobs ML, et al. Hospital variation in postoperative infection and outcome after congenital heart surgery. Ann Thorac Surg. 2013;96(2):657–663. doi:10.1016/j.athoracsur.2013.04.024
6. Kansy A, Jacobs JP, Pastuszko A, et al. Major infection after pediatric cardiac surgery: external validation of risk estimation model. Ann Thorac Surg. 2012;94(6):2091–2095. doi:10.1016/j.athoracsur.2012.07.079
7. Haughey BS, White SC, Seckeler MD. Catheter-associated bloodstream infection incidence and outcomes in congenital cardiac surgery. Congenit Heart Dis. 2019;14(5):811–813. doi:10.1111/chd.12809
8. Murni IK, MacLaren G, Morrow D, Iyer P, Duke T. Perioperative infections in congenital heart disease. Cardiol Young. 2017;27(S6):S14–S21. doi:10.1017/S1047951117002578
9. Yu X, Chen M, Liu X, et al. Risk factors of nosocomial infection after cardiac surgery in children with congenital heart disease. BMC Infect Dis. 2020;20(1):64. doi:10.1186/s12879-020-4769-6
10. Ren C, Wu C, Pan Z, Wang Q, Li Y. Pulmonary infection after cardiopulmonary bypass surgery in children: a risk estimation model in China. J Cardiothorac Surg. 2021;16(1):71. doi:10.1186/s13019-021-01450-w
11. Su C, Zhang Z, Zhao X, et al. Changes in prevalence of nosocomial infection pre- and post-COVID-19 pandemic from a tertiary Hospital in China. BMC Infect Dis. 2021;21(1):693. doi:10.1186/s12879-021-06396-x
12. Torres A, Niederman MS, Chastre J, et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS, European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT)). Eur Respir J. 2017;50(3):1700582. doi:10.1183/13993003.00582-2017
13. Srzić I, Nesek Adam V, Tunjić Pejak D. Sepsis definition: what’s new in the treatment guidelines. Acta Clin Croat. 2022;61(Suppl 1):67–72. doi:10.20471/acc.2022.61.s1.11
14. Kotwal S, Cass A, Coggan S, et al. Multifaceted intervention to reduce haemodialysis catheter related bloodstream infections: REDUCCTION stepped wedge, cluster randomised trial. BMJ. 2022;377:e069634. doi:10.1136/bmj-2021-069634
15. Hooton TM, Bradley SF, Cardenas DD, et al. Diagnosis, prevention, and treatment of catheter-associated urinary tract infection in adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America. Clin Infect Dis. 2010;50(5):625–663. doi:10.1086/650482
16. Berríos-Torres SI, Umscheid CA, Bratzler DW, et al. Centers for Disease Control and Prevention Guideline for the Prevention of Surgical Site Infection, 2017. JAMA Surg. 2017;152(8):784–791. doi:10.1001/jamasurg.2017.0904
17. Monsel A, Torres A, Zhu Y, et al. Nebulized antibiotics for ventilator-associated pneumonia: methodological framework for future multicenter randomized controlled trials. Curr Opin Infect Dis. 2021;34(2):156–168. doi:10.1097/QCO.0000000000000720
18. Gupta V, Datta P. Next-generation strategy for treating drug resistant bacteria: antibiotic hybrids. Indian J Med Res. 2019;149(2):97–106. doi:10.4103/ijmr.IJMR_755_18
19. Bassetti M, Gaudio R, Mazzei T, et al. A survey on infection management practices in Italian ICUs. Crit Care. 2012;16(6):R221. doi:10.1186/cc11866
20. Teerawattanapong N, Kengkla K, Dilokthornsakul P, et al. Prevention and Control of Multidrug-Resistant Gram-Negative Bacteria in Adult Intensive Care Units: a Systematic Review and Network Meta-analysis. Clin Infect Dis. 2017;64(suppl_2):S51–S60. doi:10.1093/cid/cix112
21. Wang H, Wang H, Yu X, et al. Impact of antimicrobial stewardship managed by clinical pharmacists on antibiotic use and drug resistance in a Chinese hospital, 2010-2016: a retrospective observational study. BMJ Open. 2019;9(8):567.
22. Schwaber MJ, Lev B, Israeli A, et al. Containment of a country-wide outbreak of carbapenem-resistant Klebsiella pneumoniae in Israeli hospitals via a nationally implemented intervention. Clin Infect Dis. 2011;52(7):848–855. doi:10.1093/cid/cir025
23. Climo MW, Yokoe DS, Warren DK, et al. Effect of daily chlorhexidine bathing on hospital-acquired infection. N Engl J Med. 2013;368(6):533–542. doi:10.1056/NEJMoa1113849
24. Jaworski R, Haponiuk I, Irga-Jaworska N, et al. Fungal infections in children in the early postoperative period after cardiac surgery for congenital heart disease: a single-centre experience. Interact Cardiovasc Thorac Surg. 2016;23(3):431–437. doi:10.1093/icvts/ivw156
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.