")
Back to Journals » Journal of Asthma and Allergy » Volume 17
Neural Biomarkers for Identifying Atopic Dermatitis and Assessing Acupuncture Treatment Response Using Resting-State fMRI
Authors Lee IS , Yoon DE, Lee S, Kang JH , Chae Y , Park HJ , Kim J
Received 13 December 2023
Accepted for publication 10 April 2024
Published 18 April 2024 Volume 2024:17 Pages 383—389
DOI https://doi.org/10.2147/JAA.S454807
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
In-Seon Lee,1 Da-Eun Yoon,1 Seoyoung Lee,2 Jae-Hwan Kang,3,4 Younbyoung Chae,1 Hi-Joon Park,1 Junsuk Kim5
1College of Korean Medicine, Kyung Hee University, Seoul, Republic of Korea; 2Department of Physics and Computational Radiology, Division of Radiology and Nuclear Medicine, Oslo University Hospital, Oslo, Norway; 3Digital Health Research Division, Korea Institute of Oriental Medicine, Daejeon, Republic of Korea; 4Aging Convergence Research Center, Korea Research Institute of Bioscience and Biotechnology, Daejeon, Republic of Korea; 5School of Information Convergence, Kwangwoon University, Seoul, Republic of Korea
Correspondence: Junsuk Kim, School of Information Convergence, Kwangwoon University, 20 Kwangwoon-ro, Seoul, 01897, Republic of Korea, Tel +82-2-940-8477, Email [email protected] Hi-Joon Park, College of Korean Medicine, Kyung Hee University, 26 Kyunghee-daero, Seoul, 02447, Republic of Korea, Tel +82-2-961-9435, Email [email protected]
Purpose: Only a few studies have focused on the brain mechanisms underlying the itch processing in AD patients, and a neural biomarker has never been studied in AD patients. We aimed to develop a deep learning model-based neural signature which can extract the relevant temporal dynamics, discriminate between AD and healthy control (HC), and between AD patients who responded well to acupuncture treatment and those who did not.
Patients and Methods: We recruited 41 AD patients (22 male, age mean ± SD: 24.34 ± 5.29) and 40 HCs (20 male, age mean ± SD: 26.4 ± 5.32), and measured resting-state functional MRI signals. After preprocessing, 38 functional regions of interest were applied to the functional MRI signals. A long short-term memory (LSTM) was used to extract the relevant temporal dynamics for classification and train the prediction model. Bootstrapping and 4-fold cross-validation were used to examine the significance of the models.
Results: For the identification of AD patients and HC, we found that the supplementary motor area (SMA), posterior cingulate cortex (PCC), temporal pole, precuneus, and dorsolateral prefrontal cortex showed significantly greater prediction accuracy than the chance level. For the identification of high and low responder to acupuncture treatment, we found that the lingual-parahippocampal-fusiform gyrus, SMA, frontal gyrus, PCC and precuneus, paracentral lobule, and primary motor and somatosensory cortex showed significantly greater prediction accuracy than the chance level.
Conclusion: We developed and evaluated a deep learning model-based neural biomarker that can distinguish between AD and HC as well as between AD patients who respond well and those who respond less to acupuncture. Using the intrinsic neurological abnormalities, it is possible to diagnose AD patients and provide personalized treatment regimens.
Keywords: Atopic Dermatitis, deep learning, functional MRI, biomarkers, personalized medicine
Introduction
Atopic Dermatitis (AD) is a complex inflammatory skin disease, characterized by intense itching and recurrent eczematous lesions.1 To treat AD, topical corticosteroids, calcineurin inhibitors, and immunomodulatory agents have been used; however, responsiveness to a treatment can vary.2 The diagnosis and severity assessment of AD currently relies solely on subjective tools (e.g., patient self-reports, visual inspection of skin).3 Therefore, attempts have been made to identify more reliable and objective indicators, known as biomarkers, that may help with the diagnosis of AD, and even potentially predict treatment response.4–6
Despite studies suggesting neurological dysfunctions in AD patients (e.g., cingulate, dorsolateral prefrontal cortex),7,8 the use of neural biomarkers in AD patients has never been investigated. In this study, we aimed to investigate whether a neural network model (Long Short-Term Memory; LSTM) can (1) extract the relevant temporal dynamics, which can discriminate between mild-moderate AD and healthy control (HC), (2) and between high and low responders to acupuncture treatment in AD patients. We employed recurrent neural networks to the resting-state functional magnetic resonance imaging (rs-fMRI).
Materials and Methods
The study received approval from the institutional review board of Kyung Hee University Korean Medicine Hospital (KOMCIRB 2020-06-003) and was registered with the Korean Clinical Trial Registry (KCT0005422). Furthermore, the study adhered to the principles outlined in the Declaration of Helsinki. We recruited 41 mild-moderate AD patients (22 male, age mean ± SD: 24.34 ± 5.29) and 40 HCs (20 male, age mean ± SD: 26.4 ± 5.32; Table 1). We considered a sample size of at least 18 people per group, based on the SCORing Atopic Dermatitis (SCORAD) total score from the previous study.9 However, it is important to acknowledge that studies identifying neural biomarkers may necessitate larger sample sizes, often exceeding 100 participants. Therefore, this study is limited by its small sample size. All participants provided informed consent. We obtained resting-state functional magnetic resonance imaging (rs-fMRI) data before the acupuncture treatment (manual acupuncture, 8 sessions, 15 minutes/session). AD participants randomly received real acupuncture (n=27) and sham acupuncture treatment (n=14; see protocol paper for more details;10 Table 1.), without the incorporation of any additional adjunctive therapies. After the real acupuncture treatment, 11 patients were classified as high responders and 16 as low responders. A patient was classified as a high responder if their SCORAD total score decreased by more than 8.7 on a scale of 0 to 10, according to the minimal clinically important difference.11
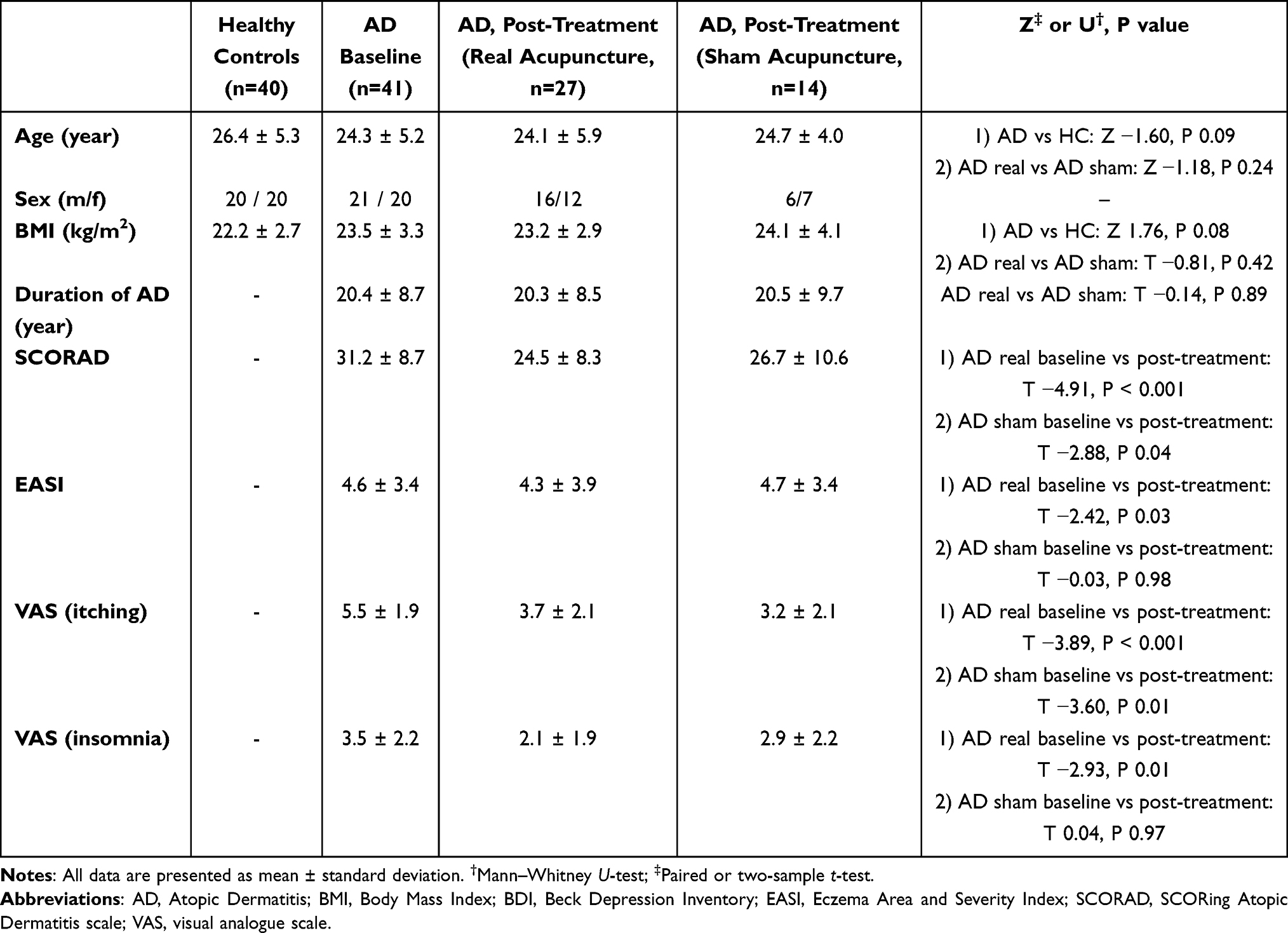 |
Table 1 Demographic and Baseline Clinical Characteristics of Participants and Clinical Effects of Real and Sham Acupuncture Treatment in Patients with Atopic Dermatitis |
Neuroimaging Acquisition and Analysis
All images were obtained with a 3T scanner (Siemens Trio Tim). A T1-weighted anatomical image was recorded (repetition time=2000ms, echo time=2.37ms, voxel size=0.9×0.9×1mm3). Whole brain blood oxygenation level–dependent data were obtained with the use of the standard T2*-weighted echo planar sequence (150 volumes, repetition time=2000ms, echo time=30ms, voxel size =3.8×3.8×4.0mm3). Data were preprocessed with the FMRIB’s Software Library, and the pipeline involved the motion correction, spatial smoothing, and registration. LSTM models keep the contextual information of the input sequences, therefore, the use of LSTM was appropriate to capture dynamic brain activity over time. LSTM models keep the contextual information of the input sequences,12 therefore, the use of LSTM was appropriate to capture dynamic brain activity over time. An LSTM was used to extract the relevant temporal dynamics for classification using scikit-learn,13 Keras,14 and TensorFlow15 libraries in Python 3.8.10 (Figure 1). The preprocessed rs-fMRI data were used as input for the neural network sequential model, which has two LSTM layers and one dense layer. We applied Power’s 38 pre-defined regions of interest (ROIs, Table 2).16 The significance of the classification accuracy and area under receiver operating characteristic curve (AUC), obtained from bootstrapping (n=100) and 4-fold cross-validation, were tested to a chance level (0.5) using a t-test with a significance level of p < 0.05.
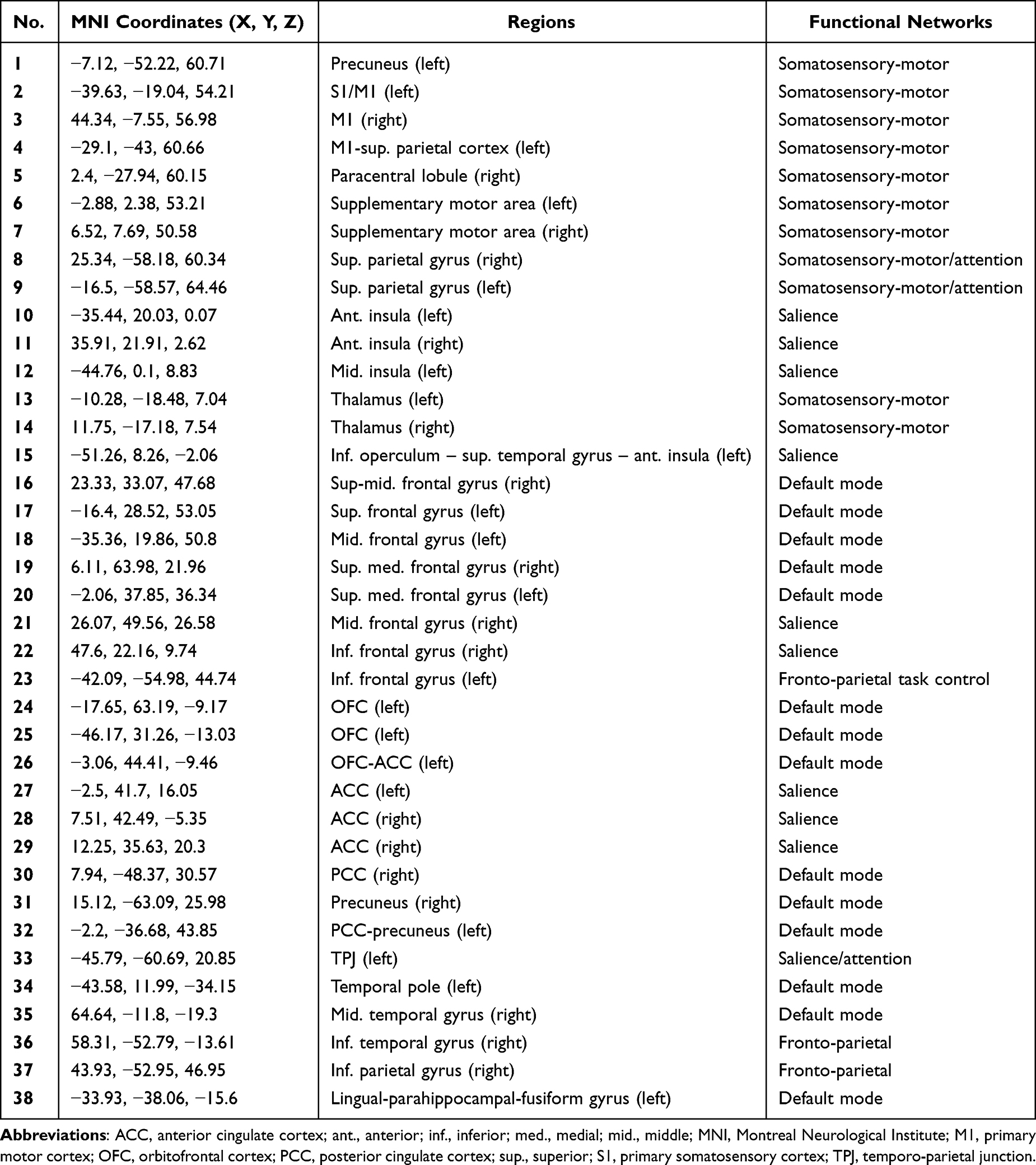 |
Table 2 Functional Regions of Interest Employed in Long Short-Term Memory Models for AD Patients |
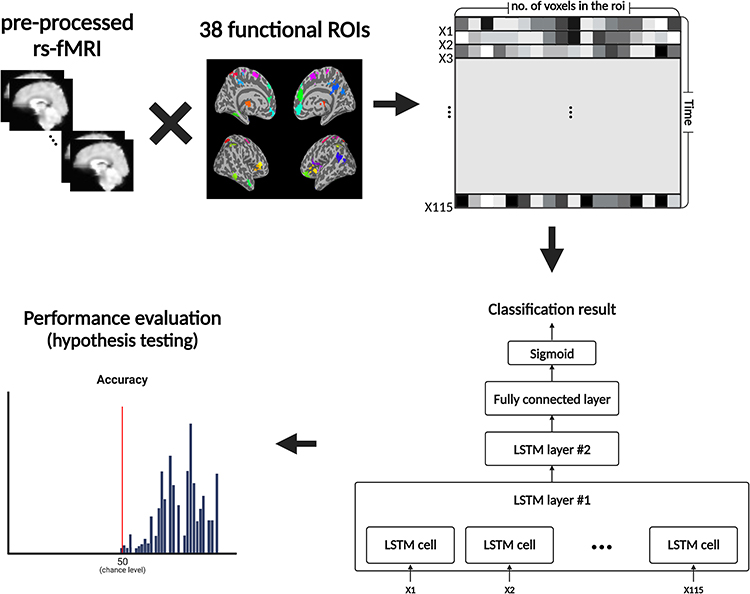 |
Figure 1 The Long Short-Term Memory analysis procedure. The resting-state fMRI data (Atopic Dermatitis [AD] n=41, healthy controls n=40) was pre-processed using FSL to remove artifacts, correct motion, smooth spatially, and functional data were registered to standard space. Blood oxygen level-dependent signals of each time point (n=115) were extracted for 38 pre-defined regions of interest (ROIs) of Power’s functional atlas. We identified two Long Short-Term Memory (LSTM) models; a model to identify mild-moderate AD patients and healthy controls and another model to identify high and low responders to acupuncture treatment among AD patients. The signals were input into a dual-layer LSTM network designed to capture temporal dependencies within the fMRI data. Each layer is composed of multiple LSTM cells that process data from the corresponding time points, allowing the network to retain information over time. The final layer’s output is forwarded through a fully connected layer followed by a sigmoid activation function to generate the classification result. We tested models’ prediction performance of each ROI based on the classification accuracy and area under receiver operating characteristic curve, assessed from a 4-fold cross-validation test. A t-test against a chance level (0.5) was conducted for the accuracy, computed by bootstrapping (n=100). The significance threshold was set at p < 0.05. Abbreviations: LSTM, Long Short-Term Memory; no., number; ROI(s), region(s) of interest; rs-fMRI, resting-state functional magnetic resonance imaging. |
Results
Neural Biomarker for Atopic Dermatitis
The model evaluation results are shown in Figure 2. For the identification of AD patients and HC, we found that the left supplementary motor area (SMA; mean accuracy 0.85, mean AUC 0.85), right posterior cingulate cortex (PCC; 0.82, 0.81), left superior/middle frontal gyrus (0.81, 0.81, p < 0.001/0.80, 0.80, p < 0.01), temporal pole (0.79, 0.80), PCC (0.82, 0.81), precuneus (0.79, 0.80), right SMA (0.78, 0.78), dorsolateral prefrontal cortex (0.78, 0.78, p < 0.001), middle temporal gyrus (0.77, 0.78), and superior medial frontal gyrus (0.75, 0.75, p < 0.01) showed significantly greater prediction accuracy than the chance level.
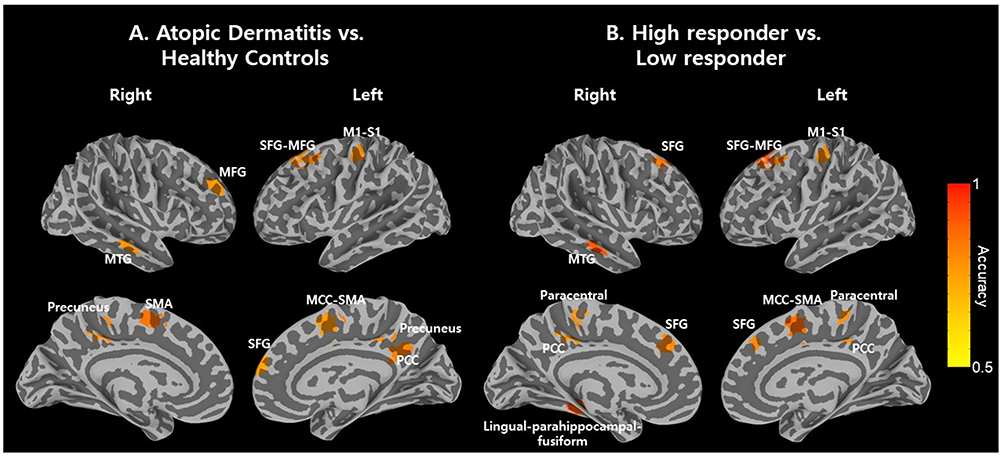 |
Figure 2 Neural biomarkers classification accuracies achieved by Long Short-Term Memory Models. We observed that patients with Atopic Dermatitis (AD) were accurately distinguished, and the outcomes of their acupuncture treatment were solely determined by the signals from resting-state functional magnetic resonance imaging (rs-fMRI) and long short-term memory models. (A) We identified distinct temporal features in the left supplementary motor area (SMA; mean accuracy 0.85, mean area under receiver operating characteristic curve [AUC] 0.85), right SMA (0.78, 0.78), right middle/posterior cingulate cortex (0.79–0.82, 0.79–0.81), left superior/middle/medial frontal gyri including the dorsolateral prefrontal cortex (0.71–0.81, 0.79–0.81), right superior/middle frontal gyrus (0.75–0.78, 0.75–0.79), left precentral gyrus (0.80, 0.80), right temporal pole (0.77, 0.77), left fusiform gyrus (0.74, 0.74), and right precuneus (0.71, 0.70) between patients with AD and healthy participants. These differences contributed to the classification of AD patients from healthy controls. (B) Using rs-fMRI signals obtained even before the acupuncture treatment, it was revealed that the right lingual-parahippocampal-fusiform gyrus (0.90, 0.89), right SMA (0.87, 0.87), left fusiform gyrus (0.90, 0.89), right superior middle frontal gyrus (0.84, 0.83), left superior/middle frontal gyrus (0.81–0.82, 0.80–0.84), left posterior cingulate cortex and precuneus (0.79, 0.68) have temporal characteristics that can distinguish high and low responders to acupuncture treatment in AD patients. The brain regions identified for diagnosing and predicting treatment responses may provide a basis for further research on the neural mechanisms of AD and the exploration of innovative treatment modalities in the future. Abbreviations: MCC, midcingulate cortex; MFG, middle frontal gyrus; MTG, middle temporal gyrus; M1, primary motor cortex; PCC, posterior cingulate cortex; SFG, superior frontal gyrus; SMA, supplementary motor area; S1, primary somatosensory cortex. |
Neural Biomarker for Treatment Responses
For the identification of high and low responders to acupuncture treatment, we found that the left lingual-parahippocampal-fusiform gyrus and superior frontal gyrus (0.90, 0.89, p < 0.01), right middle temporal gyrus (0.89, 0.89, p < 0.001), SMA (0.87, 0.87), superior middle frontal gyrus (0.84, 0.83, p < 0.01), left superior medial/middle frontal gyrus (0.82, 0.80/0.81, 0.84), PCC and precuneus (0.79, 0.68, p < 0.05), right paracentral lobule (0.78, 0.68), and left primary motor (MI) and somatosensory cortex (SI; 0.78, 0.67, p < 0.01) showed significantly greater prediction accuracy than the chance level.
Discussion
This study represents the novel investigation to identify neural biomarkers that could be beneficial for patients with AD using brain imaging data and deep learning algorithms. We found that the neural network model successfully captures differentiating dynamic brain activities, which can distinguish AD patients from HC and predict responses to acupuncture treatment. The most important features were found in the default mode and somatosensory-motor networks, which implies that AD patients and their response to a treatment might be mediated by the neural processing of their internal and external body state and sensations. The majority of significant regions discovered by deep learning models have been associated with the processing of itches, including the SMA, MI, SI, prefrontal cortex, and PCC.17 Although the results suggest the potential for temporal properties of these regions to be used as a biomarker for AD, additional study is required to replicate and generalize our findings.
Upon examination of prior studies employing machine learning or deep learning algorithms for prediction research on patients with AD to identify potential biomarkers, it becomes apparent that these studies primarily utilize skin and serum samples18,19 or skin lesion images.3,20 Most studies have focused on diagnosing AD,3 predicting its severity,19,20 or forecasting the efficacy of treatments such as dupilumab,18 similar to our study. However, our study demonstrates the feasibility of identifying neural biomarkers in patients with AD by solely utilizing neuroimaging data to predict diagnosis and acupuncture treatment outcomes. Particularly, the brain regions that can be commonly used for diagnosing and predicting treatment outcomes may serve as a foundation for future research on the brain mechanisms of AD and the development of new treatments. For example, this could include devices designed to alleviate itching by stimulating the brain directly or by targeting specific areas of the skin, known as acupoints in acupuncture treatment, to alleviate itching through brain mechanisms. As we used rs-fMRI without a task, our method has a distinct advantage as a useful biomarker for clinical application. As more healthcare devices have become available in recent years, a wearable and wireless instrument which measures and analyzes intrinsic neuronal activity may help in the early identification and treatment of AD in near future. We also suggest that patients would benefit more from using a cost-effective neuroimaging technique, such as Functional Near-Infrared Spectroscopy (fNIRS). For instance, to propose optimal diagnostic and treatment methods for patients, neuroimaging techniques can be utilized. Initially, utilizing MRI machines with superior spatial and temporal resolution, neural biomarker regions and signal characteristics can be identified. Following this, the results can be applied to research utilizing a brain imaging device that is more clinically accessible, such as fNIRS, which offers ease of installation, portability, and adaptability to diverse experimental and clinical settings.
This study has two limitations: a small sample size, and a lack of fresh data validation. A larger clinical trial is necessary to confirm the models’ accuracy and reliability. The findings, in our opinion, suggest potential applications for intrinsic neural distortions as well as potential research targets for certain regions of the brain. For instance, given that we have identified several cortical areas that can be measured by fNIRS, such as the frontal gyrus, SMA, primary motor, and somatosensory cortex, further investigation is required to determine whether the models can be successfully applied to signals from more approachable and cost-effective neuroimaging techniques to offer individualized diagnosis and treatment for patients with AD.
Conclusion
Our neural network model effectively distinguishes AD patients from healthy controls, predicting responses to acupuncture treatment. Key features in the default mode and somatosensory-motor networks suggest a link between AD and neural processing of body states. Significant regions, particularly in itch processing, may serve as potential biomarkers for AD. Our rs-fMRI approach, without a task, provides a valuable clinical biomarker. With the rise of wearable devices, a tool analyzing intrinsic neuronal activity could aid in early AD identification and treatment. Further studies are needed for validation and generalization.
Data Sharing Statement
All data presented in the manuscript, including fMRI and clinical data devoid of identifiable participant information, may be shared solely for research purposes. Requests from other parties will be directed to the corresponding authors for consideration.
Funding
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (NRF-2020R1A4A1018598, NRF-2021R1F1A1055814, RS-2023-00279315). The present research has been conducted by the Research Grant of Kwangwoon University in 2023.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Weidinger S, Novak N. Atopic dermatitis. Lancet. 2016;387(10023):1109–1122. doi:10.1016/S0140-6736(15)00149-X
2. Cabanillas B, Brehler AC, Novak N. Atopic dermatitis phenotypes and the need for personalized medicine. Curr Opin Allergy Clin Immunol. 2017;17(4):309–315. doi:10.1097/ACI.0000000000000376
3. Pan K, Hurault G, Arulkumaran K, Williams HC, Tanaka RJ. EczemaNet: automating detection and severity assessment of atopic dermatitis.
4. Renert-Yuval Y, Thyssen JP, Bissonnette R, et al. Biomarkers in atopic dermatitis-a review on behalf of the International Eczema Council. J Allergy Clin Immunol. 2021;147(4):1174–1190 e1171. doi:10.1016/j.jaci.2021.01.013
5. Mastraftsi S, Vrioni G, Bakakis M, et al. Atopic dermatitis: striving for reliable biomarkers. J Clin Med. 2022;11(16):4639. doi:10.3390/jcm11164639
6. Yu L, Li L. Potential biomarkers of atopic dermatitis. Front Med. 2022;9:1028694. doi:10.3389/fmed.2022.1028694
7. Napadow V, Li A, Loggia ML, et al. The imagined itch: brain circuitry supporting nocebo-induced itch in atopic dermatitis patients. Allergy. 2015;70(11):1485–1492. doi:10.1111/all.12727
8. Schut C, Mochizuki H, Grossman SK, et al. Brain processing of contagious itch in patients with Atopic Dermatitis. Front Psychol. 2017;8:1267. doi:10.3389/fpsyg.2017.01267
9. Park JG, Park H-J, Chae Y, Kim Y-K, Lee H, Kim K. Acupuncture treatment for symptom management in atopic dermatitis: a study protocol for a randomized, participant-and assessor-blind, sham-controlled trial. Evid Based Complement Alternat Med. 2019;2019:1–11. doi:10.1155/2019/1907578
10. Kim J, Kwon SK, Lee IS, et al. Effect of acupuncture on gut-brain axis parameters in patients with Atopic Dermatitis: a study protocol for a randomized, participant- and assessor-blind, sham-controlled trial. Evid Based Complement Alternat Med. 2021;2021:5584247. doi:10.1155/2021/5584247
11. Schram ME, Spuls PI, Leeflang MM, Lindeboom R, Bos JD, Schmitt J. EASI, (objective) SCORAD and POEM for atopic eczema: responsiveness and minimal clinically important difference. Allergy. 2012;67(1):99–106. doi:10.1111/j.1398-9995.2011.02719.x
12. Hochreiter S, Schmidhuber J. Long short-term memory. Neural Comput. 1997;9(8):1735–1780. doi:10.1162/neco.1997.9.8.1735
13. Pedregosa F, Varoquaux G, Gramfort A, et al. Scikit-learn: machine learning in Python. J Mach Learn Res. 2011;12:2825–2830.
14. Chollet F. Keras: the python deep learning library. Astrophysics source code library; 2018:ascl–1806.1022.
15. Abadi M, Agarwal A, Barham P, et al. Tensorflow: large-scale machine learning on heterogeneous distributed systems; 2016.
16. Power JD, Cohen AL, Nelson SM, et al. Functional network organization of the human brain. Neuron. 2011;72(4):665–678. doi:10.1016/j.neuron.2011.09.006
17. Najafi P, Dufor O, Ben salem D, Misery L, Carre JL. Itch processing in the brain. J Eur Acad Dermatol Venereol. 2021;35(5):1058–1066. doi:10.1111/jdv.17029
18. Wu Y, Gu C, Wang S, et al. Serum biomarker-based endotypes of atopic dermatitis in China and prediction for efficacy of dupilumab. Br J Dermatol. 2023;188(5):649–660. doi:10.1093/bjd/ljad032
19. Lee IS, Yeom M, Kim K, Hahm DH, Kang S, Park HJ. Prediction of disease severity using serum biomarkers in patients with mild-moderate Atopic Dermatitis: a pilot study. PLoS One. 2023;18(11):e0296370. doi:10.1371/journal.pone.0296370
20. Medela A, Mac Carthy T, Aguilar Robles SA, Chiesa-Estomba CM, Grimalt R. Automatic SCOring of Atopic Dermatitis using deep learning: a pilot study. JID Innov. 2022;2(3):100107. doi:10.1016/j.xjidi.2022.100107
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.