")
Back to Journals » Orthopedic Research and Reviews » Volume 14
Morphology of Humeral Head and Glenoid in Normal Shoulder of Indonesian Population
Authors Suroto H , Licindo D , Wibowo PA, Gultom GRR, Aprilya D , Setiawati R, Samijo S
Received 4 July 2022
Accepted for publication 15 November 2022
Published 7 December 2022 Volume 2022:14 Pages 459—469
DOI https://doi.org/10.2147/ORR.S378658
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Heri Suroto,1 Daniel Licindo,1 Pramono Ari Wibowo,1 Goklas Ridwan Ricardo Gultom,1 Dina Aprilya,2 Rosy Setiawati,3 Steven Samijo4
1Department of Orthopaedic & Traumatology, Dr. Soetomo General Academic Hospital / Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia; 2Orthopaedic & Traumatology, Indonesian Association for Upper Limb and Microsurgery, Jakarta, Indonesia; 3Department of Radiology, Dr Soetomo General Academic Hospital / Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia; 4Department of Orthopaedic Surgery and Traumatology, Zuyderland Medisch Centrum, Heerlen, Netherlands
Correspondence: Heri Suroto, Department of Orthopaedic & Traumatology, Dr. Soetomo General Academic Hospital / Faculty of Medicine, Universitas Airlangga, Mayjen Prof. Dr. Moestopo Street No. 47, Surabaya, East Java, 60132, Indonesia, Tel +62 31 5020251, Fax +62 31 5022472, Email [email protected]
Purpose: Shoulder prostheses designed and used around the world may not fit an Asian shoulder. Normal shoulder morphology in Asian population had been reported, ie, Chinese, Indian, Japanese, and Thai populations, but no data from the Indonesian population. The aim of this study was to evaluate the three-dimensional (3D) morphology of the glenohumeral joint in the normal Indonesian population, identify its normal values, and compare them with those of other populations in the literature.
Patients and Methods: Images for analysis were computed tomography (CT) scans of 85 normal shoulders from 71 patients who had CT scans for another diagnosis. Morphometry of the humeral head and glenoid were measured using 3D reconstruction. Gender differences and correlations between age, height, and glenohumeral morphometry were evaluated. Indonesians’ glenohumeral morphometry was compared with those of other populations in the literature.
Results: In the normal Indonesian population, the mean of humeral head inclination (HHI), height (HHH), diameter in sagittal plane (DS), diameter in frontal plane (DF), radius of curvature in sagittal plane (RS), and radius of curvature in frontal plane (RF) were 134.1°, 15.6mm, 39.3mm, 41.3mm, 20.4mm, and 21.4mm, respectively. The glenoid height (GH), upper width (GUW), lower width (GLW), inclination (GI), and version (GV) mean values were 34.2mm, 18.4mm, 24.5mm, 74.0mm, and 12.3mm, respectively. There was a significant difference in HHH, DS, DF, RS, RF, GH, GUW, GLW between males and females. Except for HHI and GI, glenohumeral morphometry was correlated with patient height. Age was not correlated with any glenohumeral morphometry.
Conclusion: In the Indonesian population, males had a larger humeral head and glenoid than females, and the size of the humeral head and glenoid was correlated to body height. Indonesians’ humeral head and glenoid sizes were smaller than those of Western populations, but close to those of other Asian populations.
Keywords: head humerus, glenoid, Asian shoulder, CT shoulder, Indonesian shoulder morphology
Introduction
Shoulder arthroplasty as a treatment option for shoulder pathologies is gaining popularity for the last few decades. In the United States, the number of total shoulder arthroplasty procedures has increased by 1373% from 1997 to 2016, and it is estimated to continue increasing.1 Prosthetic design plays an important role in improving the clinical outcomes of shoulder arthroplasty. The design of the shoulder prostheses must consider the normal anatomical morphology of the glenohumeral joint itself in order to restore normal shoulder function. Studies using three-dimensional (3D) geometry and morphology of the normal human glenohumeral shoulder in different races showed that there were racial differences in glenohumeral dimensions.2–8 Shoulder prostheses, which are designed based on European and American populations, had been reported not to fit Asian shoulders.3,7–9 There is also no guarantee that shoulder prostheses, which were designed using other Asian populations’ morphometry, will be suitable for Indonesian shoulders.
Normal shoulder morphology in Asian population had been reported for Chinese7–9, Japanese5,10, Thai2 and Indian6 populations. However, the details of the normal glenohumeral joints in Indonesian population have not been reported. The aim of this study was to evaluate the three-dimensional (3D) morphology of the glenohumeral joint in the normal Indonesian population, identify its normal values, and compare them with those of other populations in the literature. The hypothesis was that the normal value of Indonesian glenohumeral morphometry were smaller than Western populations, but close to other Asian populations.
Materials and Methods
Images for analysis were collected from computed tomography (CT) scans of patients with normal shoulder who underwent chest CT scans for other medical reasons at Dr. Soetomo General Hospital Surabaya, Indonesia. Only chest CT scans with fully visualized shoulder joints were included in this study. Subjects with past illnesses, injuries, deformities, or degenerative processes of the shoulder joint were excluded. Patient characteristics such as gender, age, weight, height, and medical diagnosis were collected from medical records.
High-resolution CT (HRCT) of the chest was performed using a 64-slice MDCT scanner. Thin-slice images were obtained and post-processed in a high-spatial-frequency algorithm for bone multi-planar reconstruction. Ford and Decker’s11 study discovered that when attempting 3D reconstructions of anatomical features or other fine details, a maximum slice thickness of 1.25 mm is recommended. This standard requirement has been fulfilled in our study since the slide thickness in HRCT of the chest ranged between 0.625–1.25 mm.12 Glenohumeral morphometry was measured using 3D reconstruction of the shoulder joint. The study protocol was approved by the Health Research Ethics Committee of our hospital (certificate number: 1724/KEPK/XII/2019).
Morphometry Measurement
Humeral head morphometries evaluated in this study were humeral head height, inclination diameter in frontal and sagittal planes, and radius of curvature in frontal and sagittal planes. Humeral head height (HHH) was defined as the distance between the humeral head base at the anatomical neck and the furthest point from it at the humeral head articular surface (Figure 1A).
 |
Figure 1 Humeral head measurement in (A) Frontal plane, and (B) Sagittal plane. Abbreviations: HHH, humeral head height; DF, humeral head diameter in frontal; O, center of humeral head; RF, radius of curvature in frontal plane; HHI, humeral head inclination; HHA, humeral head axis; and HSA, humeral shaft axis; DS, humeral head diameter in sagittal plane; RS, radius of curvature in sagittal plane. |
Humeral head is not a perfect sphere, and there is a mismatch in the frontal and sagittal planes.3,7,13–15 The Humphrey et al14 study found that the elliptical shape of the base of the humeral head seemed to elongate in the frontal plane as head size increased. Humeral head diameter was defined as the diameter of the humeral head at its base. Superior-inferior distance was measured in the frontal plane (DF), while the anterior-posterior distance was measured in the sagittal plane (DS) (Figure 1B).
Radius of curvature was defined as a line drawn from the center of the humeral head to the furthest point on the humeral head surface. Radius of curvature was also measured in the frontal (RF) and sagittal (RS) planes. Humeral head inclination (HHI) is the angle between the humeral head axis and the humeral shaft axis. The humeral head axis is a line drawn perpendicular to the anatomical neck plane, while the humeral shaft axis is a best-fit line through the center of the humeral shaft.
Glenoid morphometries in this study were glenoid inclination, height, width, and version. Glenoid height (GH) was the distance between the highest and the lowest point on the glenoid (Figure 2A). Various shapes of the glenoid cavity made the anterior-posterior distance between the upper half and the lower half of the glenoid cavity were different. This study used glenoid upper and lower width terms to measure those distances. Glenoid upper width (GUW) was defined as the anterior-posterior distance of the upper half of the glenoid cavity at the midpoint between the mid-equator and the superior edge. The maximum width of the glenoid cavity was usually found in the lower half part and not always in the midpoint between the mid-equator and the inferior edge. This is why the glenoid lower width (GLW) was defined as the maximum distance between the most anterior and most posterior points in the lower half of the glenoid cavity.
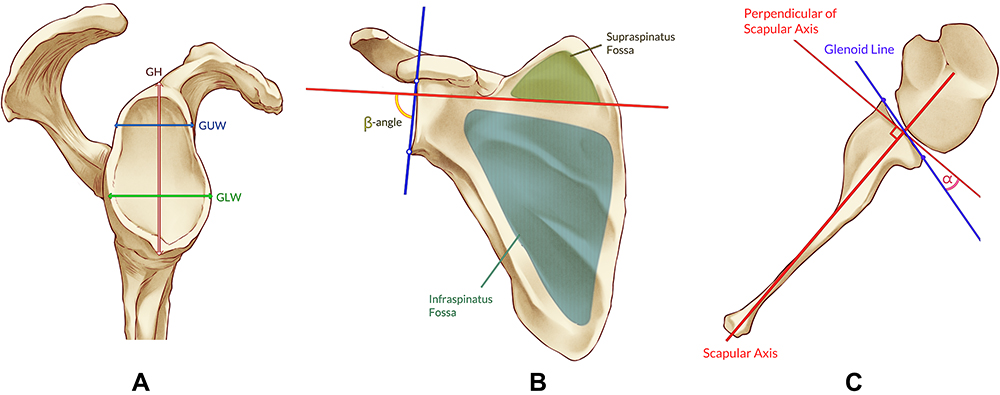 |
Figure 2 Glenoid measurement. Abbreviations: GH, glenoid height; GUW, glenoid upper width; GLW, glenoid lower width. Notes: (A) Glenoid cavity parameters from lateral view: GH, GUW, and GLW. (B) Glenoid inclination (GI) was measured using β-angle. (C) α-angle represents glenoid version (GV)16,17 |
Many different methods were used to measure both the glenoid inclination and the glenoid version. In our study, the glenoid inclination (GI) was measured using the β angle, which was the most reproducible measurement for glenoid inclination as described by Maurer et al16 The β angle was defined as the angle between a line connecting the superior-inferior glenoid edges and a line drawn through the floor of supraspinatus fossa (Figure 2B). The glenoid version (GV) was measured using the Friedman et al18 method, which was the most common method used to measure the glenoid version. The glenoid version was defined as an angle between a line connecting the anterior-posterior glenoid edges and a line perpendicular to the scapula axis (Figure 2C). The scapula axis was a line connecting the tip of the medial border of the scapula to the center of the glenoid cavity.
Statistical Analysis
Statistical analysis was performed using the SPSS Statistics 25 Software for Windows. The normality test was performed using Kolmogorov–Smirnov tests to examine the distributions of all parameters. Differences between males and females were analyzed using the Student’s T-test if the data was normal, otherwise, Mann–Whitney U was used. Correlations between patients’ height, age, and shoulder morphometry were analyzed using the Spearman test. The significance level was set at 0.05 for all analyses.
Results
CT scans of 85 normal shoulders from 71 patients met the criteria and included in this study. The mean age of the subjects was 57.8 years, the mean height was 163.9 cm and the mean weight was 63.8 kg. Patients’ demographics are shown in Table 1.
 |
Table 1 Demographic Data in Subjects |
The means of HHH, DS, DF, RS, RF, and HHI were 15.6 ± 1.1mm (range, 13.3–18.5) mm, 39.3 ± 2.4mm (range, 34.0–45.9), 41.3 ± 3.5mm (range, 33.6–50.9), 20.4 ± 1.5mm (range, 17.0–24.6), 21.4 ± 1.9mm (range, 17.3–26.5), and 134.1° ± 0.8° (range, 131.9–135.9), respectively. This study showed that the humeral head diameter in the frontal plane (DF) was longer than its diameter in the sagittal plane (DS). Radius of curvature in the frontal (RF) was also longer than its radius in the sagittal plane (RS). The mean of GH, GUW, GLW, and GI were 34.2 ± 3.4mm (range, 28.8–41.8), 18.4 ± 2.2mm (range, 13.8–24.0), 24.5 ± 2.8mm (range, 19.5–31.7), and 74.0 °± 1.0° (range, 71.4–76.8), respectively. The average Indonesian glenoid version was 12.3 ± 1.2° (range, 9.5–15.6) retroversion. Details about the humeral head and glenoid morphometry are shown in Table 2.
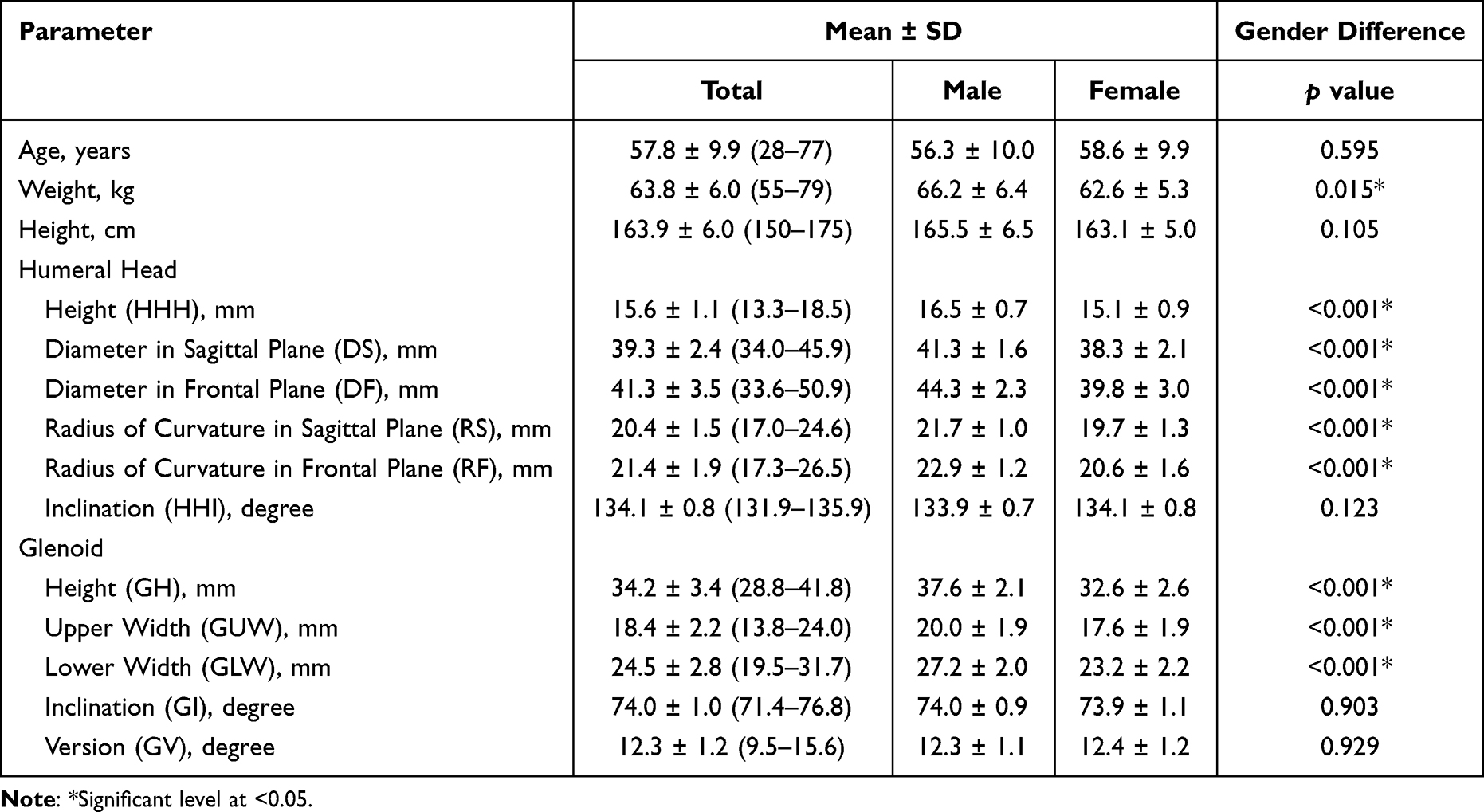 |
Table 2 Humeral Head and Glenoid Morphometry in Normal Indonesian Adults |
Kolmogorov–Smirnov tests showed normal distribution only for HHI and GUW. Thus, comparison and correlation studies were performed using Mann–Whitney U-test and Spearman test. Comparison studies between males and females showed significant differences for glenohumeral dimensions such as HHH (p<0.001), DS (p<0.001), DF (p<0.001), RS (p<0.001), RF (p<0.001), GH (p<0.001), GUW (p<0.001), and GLW (p<0.001) in all analysis), but not for glenohumeral orientations such as HHI (p=0.123), GI (p=0.903) and GV (p=0.929). In this comparison study, male subjects had larger humeral heads and glenoid than female subjects.
Body height was correlated with HHH (r (83)=0.303, p=0.002), DS (r (83)=0.303, p=0.002), DF (r (83)=0.303, p=0.002), RS (r (83)=0.303, p=0.002), RF (r (83)=0.306, p=0.002), GH (r (83)=0.319, p=0.001), GUW (r (83)=0.313, p=0.004), GLW (r (83)=0.283, p=0.002), GD (r=0.313) and GV (r (83)= −0.233, p=0.016). The correlation study showed that subjects with higher body height tend to have larger humeral head and glenoid. Among the Indonesian population, no correlation was found between age and any glenohumeral morphometry. Details on correlation analysis are shown in Table 3.
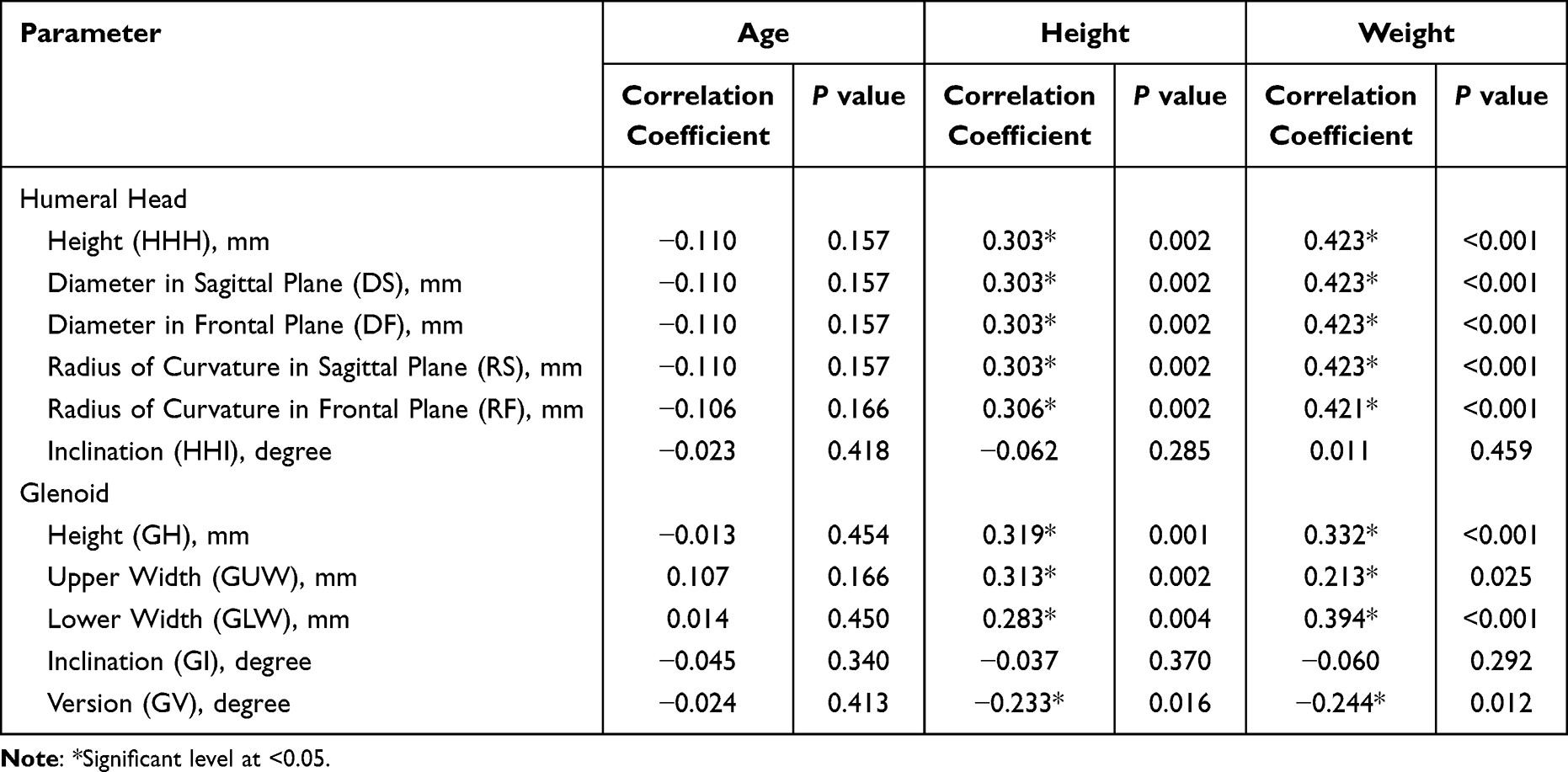 |
Table 3 Correlations Between Glenohumeral Morphometry with Age, Height, and Weight |
Discussion
Prosthetic that resembles normal shoulder anatomy can improve joint kinematics and final outcomes. Improperly sized may lead to stiffness, pain, component loosening, and a potentially inferior outcome.3 Studies showed that most of the shoulder prostheses currently used worldwide, which were designed for the American and European populations, did not fit for Asian shoulders.5–10 Knowledge about normal glenohumeral morphometry in a specific population is necessary for prosthetic design, sizing, and positioning during arthroplasty.
Morphometry
Previous studies reported that the humeral head size in the Asian population was smaller than in the Western populations.2,3,14,15 The normal Indonesian humeral head height, diameter, and radius of curvature in this study were also smaller than in western populations (Table 4). Compared to other studies in Asian populations, normal Indonesian humeral head size was greater than Japanese population but close to Chinese and Indian populations. Despite its geographical proximity, a Singaporean cadaveric study by Manoharan et al19 reported a significantly huge humeral head size, even the greatest among all studies. In their study, Manoharan et al19 used direct measurement on a fresh cadaver in which the articular cartilage was still intact. The presence of articular cartilage combined with direct measurement could be the reason for these differences since most other studies were using CT scan, which neglected the presence of articular cartilage.
 |
Table 4 Humeral Head Morphometry in Other Studies |
Our study showed that the mean humeral head diameter in the frontal plane (41.3 mm) was greater than the sagittal plane (39.3 mm). In addition, Hertel et al15 Humphrey et al14 and Sahu et al6 also reported a greater humeral head diameter in the frontal plane compared to the sagittal plane. Analysis done by Humphrey et al found that the shape of the base of small humeral heads was closer to being spherically shaped, whereas the shape of larger humeral heads was typically more elongated in the frontal plane. Our results showed that the shape of the humeral head base in the Indonesian population was not spherical and elongated in the frontal plane.
The mean Indonesian humeral head radius of curvature in the frontal plane (21.4 mm) was greater than that in the sagittal plane (20.4 mm). Hertel et al15 and Humphrey et al14 also reported similar endings. Another study by Cabezas et al3 found that the humeral head radius of curvature in the frontal plane was also greater than in the axial plane. However, the relationship between the radius of curvature in the axial and sagittal planes was unknown because their study did not measure the radius of curvature in the sagittal plane.
Wataru et al20 in their cadaveric study equally divided the humeral head’s articular surface into 3 portions from superior to inferior and 3 portions from anterior to posterior, with a final result of 9 parts. Their study found that the mean radii of all parts were changed from superior to inferior and from anterior to posterior. The superior portion radius of curvature was significantly greater than the central portion and the mean radii of curvature in anterior and posterior portions were significantly less than that of the central portion. Since the radius of curvature in the frontal plane was measured in the central portion between the anterior and posterior, it explains why the radius of curvature in the frontal plane was greater than the sagittal plane in our study and previous studies. From our findings and supporting literature, we conclude that the shape of the surface of the humeral head is a complex 3D spheroid of which curvature changes from superior to inferior and from anterior to posterior.
The normal value of Indonesian humeral head inclination was close to Japanese, Indian and Chinese populations, and slightly greater than Thai and Singaporean populations. Humeral head inclinations in the Indonesian population were smaller than those studies in the Western population.3,14,15 However, there was a study on Caucasians bones which had a smaller humeral head inclination compared to our study.2 It is hard to determine whether Indonesian humeral head inclination is smaller or greater compared to Western populations because the normal value of humeral head inclination in previous studies was varied.
Another important morphometry for prosthetic design was the humeral head version. The previous study showed that humeral head retroversion in Asian populations was greater than in Western populations.2 However, this study was unable to measure the humeral head version due to the lack of distal humerus imaging in Chest CT.
Indonesian glenoid height is the greatest among other Asian populations, but it is still considered small compared to Western populations (Table 5). The Indonesian glenoid lower width or glenoid maximum width was also close to other Asian populations and smaller than Western populations. The data showed that the glenoid lower width was greater than its upper width. This is similar to previous studies.3,21
 |
Table 5 Glenoid Morphometry in Other Studies |
The mean of the normal Indonesian glenoid inclination, which was measured using β angle, was 74.0° and the mean of the normal Indonesian glenoid version was 12.3° retroversion.6 It was difficult to compare both the glenoid inclination and version with previous studies due to differences in measurement methods. The authors only compared these study results with other studies that used similar measurement methods. The mean of Indonesian glenoid inclination was slightly smaller than the Indian population. The mean of the Indonesian glenoid version was more retroverted than Hongkong and Indian populations.
Gender Analysis
Gender analysis found that Indonesian males had a larger humeral head height, diameter, and radius of curvature than females (p<0.001 in all analyses), but no difference was found in humeral head inclination (p=0.123). Previous studies also found that gender difference affected the values of humeral head height, diameter, and radius of curvature, but did not affect the value of humeral head inclination.2,3,6,7,10,14
Indonesian glenoid height and width in males were also greater than the females (p <0.001 in all analyses), similar to previous studies.3–8,10,21,22 In this study, no gender difference was found in both glenoid inclination (p =0.903) and glenoid version (p=0.929). The Slocum et al8 study also found no significant difference in the glenoid version between males and females. However, Matsumura et al23 reported that Japanese males had a higher retroversion for both humeral head and glenoid than Japanese females. This study showed that age was not correlated with all glenohumeral morphometry. In contrast with age, body height was found to be correlated with humeral head height, humeral head diameter, the humeral head radius of curvature, glenoid height, and glenoid width, but not to humeral head inclination, glenoid inclination, and glenoid version. Similar to our study, body height had been reported to correlate with humeral head size7,10,14,23,24 and glenoid size.5,10,21–23 Thus, it is proved that body height affects both the humeral head and the glenoid size regardless race.
Limitations
This study had several limitations. First, subjects in this study were patients who had chest CT scans for any medical reason other than the shoulder, thus the subjects were not truly come from the healthy population. Our study excluded subjects with past illnesses, injuries, deformities, or degenerative processes of the shoulder joint. However, the accuracy of our subjects to represent the normal shoulder of Indonesian is difficult to determine.
Second, the extraction of shoulder imaging from chest CT had several limitations. The difference in positioning, slice thickness, and focus area between shoulder CT and chest CT may affect the quality of 3D reconstruction and shoulder measurement. However, this study used thin-slice HRCT of the chest with a post-processing bone algorithm to optimize the 3D reconstruction quality. The humerus was not completely visible on the chest CT. This explains why this study could not measure the humeral head version, medial and posterior offset.
Finally, the limitation of CT scan in visualizing soft tissues made our measurement neglect the thickness of the articular cartilage. This may result in slight differences between the glenohumeral morphometry that we measured and its actual morphometry.
Conclusion
This study presented the morphology of glenohumeral joint in the normal Indonesian population. The size of Indonesian humeral head and glenoid were greater in males than females and were correlated to body height. Indonesians humeral head and glenoid size were smaller than Western populations, but close to other Asian populations. These results would be useful to determine the size of implants and to improve the development of shoulder prostheses design especially for Asian populations.
Ethical Committee Approval
This study was reviewed and approved by the Ethics Committee of the Dr. Soetomo General Hospital with reference number: 1724/KEPK/XII/2019. Patient consent to review their medical records was not required by the ethics committee. This study covered patient data confidentiality and compliance according to the Declaration of Helsinki.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rabinowitz J, Kothandaraman V, Lin J, Li X, Friedman RJ, Eichinger JK. Utilization of shoulder arthroplasty in the United States – an analysis of current trends and future predictions. Semin Arthroplasty JSES. 2020;30(3):200–209. doi:10.1053/j.sart.2020.08.004
2. Aroonjarattham P, Jiamwatthanachai P, Mahaisavariya B, Kiatiwat T, Aroonjarattham K, Sitthiseripratip K. Three-dimensional morphometric study of the Thai proximal humerus: cadaveric study. J Med Assoc Thai. 2009;92(9):1191–1197.
3. Cabezas AF, Krebes K, Hussey MM, et al. Morphologic variability of the shoulder between the populations of North American and East Asian. Clin Orthop Surg. 2016;8(3):280–287. doi:10.4055/cios.2016.8.3.280
4. Churchill RS, Brems JJ, Kotschi H. Glenoid size, inclination, and version: an anatomic study. J Shoulder Elbow Surg. 2001;10(4):327–332. doi:10.1067/mse.2001.115269
5. Mizuno N, Nonaka S, Ozaki R, Yoshida M, Yoneda M, Walch G. Three-Dimensional Assessment of the Normal Japanese Glenoid and Comparison with the Normal French Glenoid. Vol. 103. Elsevier Masson SAS; 2017:1271–1275.
6. Sahu D, Joshi M, Rathod V, Nathani P, Valavi AS, Jagiasi JD. Geometric analysis of the humeral head and glenoid in the Indian population and its clinical significance. JSES Int. 2020;4(4):992–1001. doi:10.1016/j.jseint.2020.06.008
7. Zhang Q, Shi LL, Ravella KC, et al. Distinct proximal humeral geometry in Chinese population and clinical relevance. J Bone Joint Surg Am. 2016;98(24):2071–2081. doi:10.2106/JBJS.15.01232
8. Slocum AMY, Siu YC, Ma CM, Lui TH. The study of 2-dimensional computed tomography scans of the glenoid anatomy in relation to reverse shoulder arthroplasty in the Southern Chinese population. JSES Int. 2021;5(4):714–721. doi:10.1016/j.jseint.2021.02.006
9. Zhang L, Yuan B, Wang C, Liu Z. Comparison of anatomical shoulder prostheses and the proximal humeri of Chinese people. Proc Inst Mech Eng H. 2007;221(8):921–927. doi:10.1243/09544119JEIM267
10. Matsumura N, Oki S, Ogawa K, et al. Three-dimensional anthropometric analysis of the glenohumeral joint in a normal Japanese population. J Shoulder Elbow Surg. 2016;25(3):493–501. doi:10.1016/j.jse.2015.08.003
11. Ford JM, Decker SJ. Computed tomography slice thickness and its effects on three-dimensional reconstruction of anatomical structures. J Forensic Radiol Imaging. 2016;4:43–46. doi:10.1016/j.jofri.2015.10.004
12. Di Muzio B, Fahrenhorst-Jones T. HRCT chest (protocol). Reference Article, Radiopaedia.org; 2022.
13. Kadavkolan AS, Jawhar A. Glenohumeral joint morphometry with reference to anatomic shoulder arthroplasty. Curr Orthop Pract. 2018;29(1):71–83. doi:10.1097/BCO.0000000000000552
14. Humphrey CS, Sears BW, Curtin MJ. An anthropometric analysis to derive formulae for calculating the dimensions of anatomically shaped humeral heads. J Shoulder Elbow Surg. 2016;25(9):1532–1541. doi:10.1016/j.jse.2016.01.032
15. Hertel R, Knothe U, Ballmer FT. Geometry of the proximal humerus and implications for prosthetic design. J Shoulder Elbow Surg. 2002;11(4):331–338. doi:10.1067/MSE.2002.124429
16. Maurer A, Fucentese SF, Pfirrmann CWA, et al. Assessment of glenoid inclination on routine clinical radiographs and computed tomography examinations of the shoulder. J Shoulder Elbow Surg. 2012;21(8):1096–1103. doi:10.1016/j.jse.2011.07.010
17. Mamatha T, Pai SR, Murlimanju BV, Kalthur SG, Pai MM, Kumar B. Morphometry of glenoid cavity. Online J Heal Allied Sci. 2011;10(3):1–4.
18. Friedman RJ, Hawthorne KB, Genez BM. The use of computerized tomography in the measurement of glenoid version. J Bone Joint Surg Am. 1992;74(7):1032–1037. doi:10.2106/00004623-199274070-00009
19. Manoharan V, Sheng JM, Chou SM, Soon Yew AK, Tan SH, Tjoen Lie DT. A normative anatomic study of the glenohumeral joint and rotator cuff tendons. Proc Singapore Healthc. 2014;23(3):201–208. doi:10.1177/201010581402300305
20. Wataru S, Kazuomi S, Yoshikazu N, Hiroaki I, Takaharu Y, Hideki Y. Three-dimensional morphological analysis of humeral heads: a study in cadavers. Acta Orthop. 2005;76(3):392–396. doi:10.1080/00016470510030878
21. Khan R, Satyapal KS, Lazarus L, Naidoo N. An anthropometric evaluation of the scapula, with emphasis on the coracoid process and glenoid fossa in a South African population. Heliyon. 2020;6(1):e03107. doi:10.1016/j.heliyon.2019.e03107
22. Singh SSL, Tengku Md Shihabudin TM, Pall Singh TS, Bin Musa AT, Mohd Daud NB, Dragoo JL. Morphological characteristics of Malaysian Malay shoulders for the Latarjet procedure: a cross-sectional CT scan based study. Curr Orthop Pract. 2020;31(2):8–12. doi:10.1097/BCO.0000000000000837
23. Matsumura N, Ogawa K, Kobayashi S, et al. Morphologic features of humeral head and glenoid version in the normal glenohumeral joint. J Shoulder Elbow Surg. 2014;23(11):1724–1730. doi:10.1016/j.jse.2014.02.020
24. Iannotti JP, Gabriel JP, Schneck SL, Evans BG, Misra S. The normal glenohumeral relationships. An anatomical study of one hundred and forty shoulders. J Bone Joint Surg. 1992;74(4):491–500. doi:10.2106/00004623-199274040-00004
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.