")
Back to Journals » Journal of Asthma and Allergy » Volume 7
Link between vitamin D and airway remodeling
Authors Berraies A, Hamzaoui K , Hamzaoui A
Received 16 December 2013
Accepted for publication 8 February 2014
Published 1 April 2014 Volume 2014:7 Pages 23—30
DOI https://doi.org/10.2147/JAA.S46944
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Anissa Berraies, Kamel Hamzaoui, Agnes Hamzaoui
Pediatric Respiratory Diseases Department, Abderrahmen Mami Hospital, Ariana, and Research Unit 12SP15 Tunis El Manar University, Tunis, Tunisia
Abstract: In the last decade, many epidemiologic studies have investigated the link between vitamin D deficiency and asthma. Most studies have shown that vitamin D deficiency increases the risk of asthma and allergies. Low levels of vitamin D have been associated with asthma severity and loss of control, together with recurrent exacerbations. Remodeling is an early event in asthma described as a consequence of production of mediators and growth factors by inflammatory and resident bronchial cells. Consequently, lung function is altered, with a decrease in forced expiratory volume in one second and exacerbated airway hyperresponsiveness. Subepithelial fibrosis and airway smooth muscle cell hypertrophy are typical features of structural changes in the airways. In animal models, vitamin D deficiency enhances inflammation and bronchial anomalies. In severe asthma of childhood, major remodeling is observed in patients with low vitamin D levels. Conversely, the antifibrotic and antiproliferative effects of vitamin D in smooth muscle cells have been described in several experiments. In this review, we briefly summarize the current knowledge regarding the relationship between vitamin D and asthma, and focus on its effect on airway remodeling and its potential therapeutic impact for asthma.
Keywords: vitamin D, asthma, airway remodeling, airway smooth muscle, supplementation
Introduction
Vitamin D is an essential nutrient with significant pleiotropic effects, and its role in immunomodulation is considered to be of major importance. Moreover, there is growing evidence that vitamin D also contributes positively to pulmonary health.1 Vitamin D is a secosteroid hormone synthesized by the skin following exposure to ultraviolet B light. Solar radiation photolyzes 7-dehydrocholesterol in the skin to previtamin D3, which is then converted to vitamin D3 (cholecalciferol).2 Cholecalciferol from the skin and diet is hydroxylated in the liver to 25-hydroxyvitamin D3 [25(OH)D]. Hydroxylation of 25(OH)D to its biologically active form, ie, calcitriol (1,25(OH)2D3), takes place mainly in the kidney, but also in other sites, such as immune cells. Vitamin D signaling occurs predominantly through binding of 1,25(OH)2D3 to the vitamin D receptor (VDR), formation of a heterodimer with the retinoid X receptor, and subsequent regulation of gene expression after translocation to the nucleus. Alternatively, 1,25(OH)2D3 can bind to the VDR on the plasma membrane to exert rapid responses via production of second messengers.3,4
Epidemiology
Worldwide, there have been many asthma cohorts looking at vitamin D status in association with asthma and allergy, and these have shown contradictory results. Most studies have demonstrated an association between vitamin D deficiency and increased asthma risk.5 Several case-control studies performed in different countries have shown a high prevalence of vitamin D deficiency in asthmatic children compared with controls, even in sunny areas.6–8 Two studies conducted in Italian children showed that hypovitaminosis D was very frequent in asthmatic children, with only 11% of children having adequate vitamin D levels.9,10 Several studies in children and adults concluded that low levels of vitamin D (defined as circulating 25(OH)D levels <30 ng/mL) were correlated with asthma severity, altered lung function, increased airway hyperresponsiveness, increased reactivity to exercise,9–15 and loss of control.4 Several authors have demonstrated the involvement of vitamin D deficiency in severity and control of asthma. Lower concentrations of vitamin D have been associated with an increased risk of exacerbations.16,17 In one study, children with decreased serum 25(OH)D levels had a risk of asthma exacerbation that was eight times higher than that in children with stable or increased serum 25(OH)D levels.18
However, the data are controversial. Some studies have reported conflicting results, ie, no association between vitamin D status and asthma in either children or adults.19,20 More time spent in the sun in winter between the ages of 6 and 15 years has been associated with an increased risk of hay fever.20
The vitamin D pathway has revealed a number of polymorphisms in its components, including the VDR (the major receptor for the bioactive form of 25(OH)D), the microsomal vitamin D hydroxylase enzyme cytochrome P450 (CYP)2R1, and the vitamin D-binding protein GC.21 Genetic variants in the VDR are variably associated with a risk of asthma.22–24 It is worth noting that, in addition to being expressed by immune cells, airway smooth muscle (ASM) cells also express functional VDR.25 Another interesting gene is sphingosine-1-phosphate phosphatase (SGPP2) that had significant differences in expression depending on serum 25(OH)D level. Single nucleotide polymorphisms of SGPP2 have been associated with forced expiratory volume in one second (FEV1) variations in the general population.26
Vitamin D and airway inflammation
Data from observational studies suggest a protective role of vitamin D in severe asthma. An immune-modulating potential of vitamin D has been implicated in asthma, and there is increasing evidence to support the role of the vitamin D pathway in the regulation of immune function. The VDR has been found on almost all immune cells, including macrophages and dendritic cells, as well as T-cells and B-cells;2,27–29 these receptors increase five-fold following activation of quiescent cells.30 In vivo studies in mouse models suggested this association, with Wittke et al demonstrating that VDR knockout mice do not develop experimental asthma, leading these authors to conclude that vitamin D is required for generation of T-helper (Th)2-driven inflammation in the airways.31
Vitamin D promotes immune regulation. Indeed, in vitro studies have demonstrated the capacity of vitamin D to induce a tolerogenic dendritic cell phenotype producing interleukin (IL)-10, which promotes generation of forkhead box P3 (FOXP3) regulatory T-cells (Tregs).32,33 In children with asthma, serum 25(OH)D levels were significantly correlated with CD25+ FOXP3+ Tregs and IL-10+ CD4+ T lymphocytes.34 These cells are associated with steroid sensitivity. Vitamin D deficiency could hinder expression of FOXP3 in CD4+ Tregs, thereby lowering steroid-induced production of IL-10 and decreasing the anti-inflammatory activity of glucocorticoids. In contrast, vitamin D supplementation reverses steroid resistance, probably via upregulation of FOXP3 in Tregs. Moreover, it has been recently shown that vitamin D inhibits proinflammatory Th17 responses.34–36 Glucocorticoids do not inhibit IL-17A cytokine expression in vivo or in vitro, whereas treatment with 1,25(OH)2D3 signi?cantly reduces IL-17A and IL-22 levels.37 Clinical studies show that the improvement in lung function obtained with inhaled steroid treatment is reduced in children with vitamin D deficiency.38
Lastly, adequate vitamin D status may prevent asthma by upregulating the production of antimicrobial proteins, such as cathelicidin and beta defensins, thereby inhibiting the inflammatory reaction arising from viral respiratory tract infection.39 Considering the major role of viruses in exacerbations of asthma, together with the consequences of recurrent exacerbations for airway remodeling, the potential therapeutic involvement of vitamin D to inhibit remodeling is discussed below.
Vitamin D and airway remodeling
The extensive airway remodeling occurring in asthma is characterized by structural changes that include abnormally thickened epithelium with mucous gland hypertrophy, subepithelial membrane thickening, fibrosis with altered composition and deposition of extracellular matrix, angiogenesis, and greatly increased ASM mass.40 Airway remodeling therefore often causes irreversible airflow limitation and increased airway hyperresponsiveness. The thickness of the basement membrane is negatively correlated with FEV1 and the provocative dose of methacholine.41 Traditionally, remodeling was thought to occur as a result of long-term inflammation but it is now clear that remodeling begins in early childhood before the age of 3 years.42 In ovalbumin-sensitized mice, vitamin D deficiency was associated with greater airway hyperresponsiveness and more marked signs of airway remodeling than that observed in vitamin D-replete mice. Vitamin D supplementation attenuated these proinflammatory effects, but did not completely reverse the features of allergic airway inflammation.43 In a murine model of chronic asthma, vitamin D treatment concomitant with ovalbumin challenge reduced chronic ovalbumin-induced inflammation and attenuated structural changes in the airways, including subepithelial fibrosis, goblet cell hyperplasia, and increased ASM mass. Nuclear translocation of nuclear factor-kappa B (NF-κB) p65 was inhibited, suggesting that vitamin D supplementation could attenuate airway remodeling in asthma via inhibition of NF-κB activation.44
Inflammatory cells such as eosinophils produce and secrete matrix metalloproteinase (MMP)-9, which is capable of digesting type IV collagen, a component of the basement membrane. Overproduction of tissue inhibitors of matrix metalloproteinase 1 (TIMP-1) allows deposition of extracellular matrix and subepithelial fibrosis. Fibroblasts play a critical role in this exaggerated deposition of collagen when activated by tumor growth factor-beta-1 (TGF-β1), a profibrotic cytokine.4,41 In asthma, inflammatory and resident cells such as macrophages, lymphocytes, eosinophils, fibroblasts, and airway epithelial cells synthesize TGF-β. Th2-derived cytokines, including IL-4, play an important role in airway remodeling.45 TGF-β induces TIMP-1 expression in a Th2-dependent manner.4,41 Vitamin D decreases CD4+ T-cell production of the signature Th2 cytokines, IL-4, IL-5, and IL-13, and promotes release of IL-10. The concentration of calcitriol in vitro may be critical in determining the effect on Th2 cell differentiation and function.46 In the same way, 1,25(OH)2D3 inhibited the proliferation and activation of murine fibroblasts treated with TGF-β1 and reduced the expression of extracellular matrix proteins (Figure 1).47 In vitro experiments have demonstrated that TGF-β1 induces epithelial–mesenchymal transition in bronchial epithelial cells, with a decrease in E-cadherin expression and an increase in expression of vimentin and α-smooth muscle actin.48 Bradykinin induces differentiation of lung fibroblasts into myofibroblasts.49
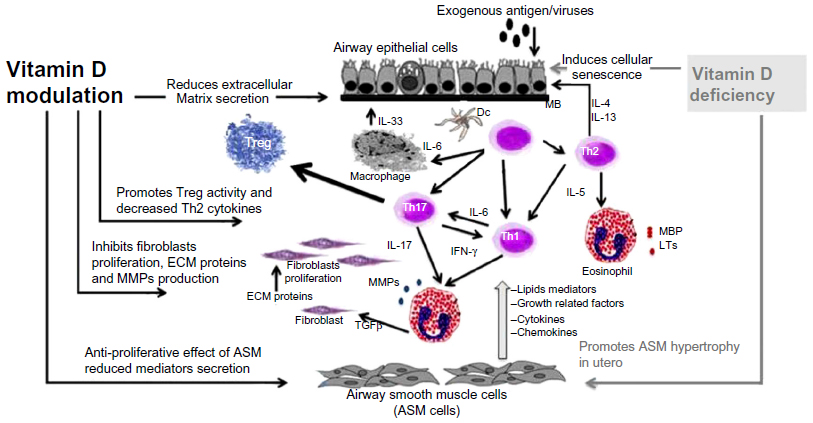 | Figure 1 Potential pathways involving vitamin D in airway remodeling. Airway remodeling can be defined as changes in the composition, content, and organization of the cellular and molecular constituents of the airway wall. These structural changes include epithelial detachment, subepithelial fibrosis, increased ASM mass, goblet cell hyperplasia, mucous gland hyperplasia, and proliferation of blood vessels. Asthma exacerbation is triggered by allergens or viruses, inducing T-helper cell-driven inflammation and resulting in production of growth factors (TGF-β, TNF-α, and VEGF), profibrotic mediators (TGF-β, LTs, PG), MMPs, and ECM protein. Vitamin D insufficiency is associated with alteration in lung development, cellular senescence with inflammation and MMP release, and ASM hyperplasia. Potential beneficial effects of vitamin D are increasing Treg activity, improving innate immunity against viruses, decreasing release of induced mediators, and decreasing production of LTs, PG, MMP, TNF-α and TGF-β, resulting in decreased subepithelial fibrosis and ASM hypertrophy. |
The antifibrotic effects of vitamin D have been described in several disease models. VDR knockout mice showed increased influx of inflammatory cells, phosphoacetylation of NF-κB associated with increased proinflammatory mediators, and upregulation of metalloproteinases in the lung. This was associated with emphysema and a decline in lung function associated with formation of lymphoid aggregates.50 Further, 1,25(OH)2D3 suppresses production of MMPs and enhances TIMP-1 levels in tuberculosis.51 In a human squamous carcinoma cell line, vitamin D3 significantly suppressed production of MMP-9 and MMP-13 mRNA and proteins in a dose-dependent manner.52 In a Crohn’s disease model, a vitamin D analog attenuated the profibrotic response of colonic myofibroblasts to high matrix stiffnesss.53 Calcitriol is known to attenuate epidermal inflammation. Exposure to tumor necrosis factor-alpha (TNF-α) markedly increased protein and mRNA levels of MMP-9, while pretreatment with calcitriol reduced this effect in a dose-dependent manner. This effect was associated with a reduction in activation of NF-κB.54 1,25(OH)2D3 attenuates TNF-α-induced p65 nuclear translocation and NF-κB activity in a VDR-dependent manner because VDR physically interacts with IκB kinase β to block NF-κB activation. This interaction is enhanced by 1,25(OH)2D3.55
Airway remodeling in asthma includes increased ASM mass, reflecting myocyte proliferation.56–58 Hypertrophy of ASM is correlated with a decrease in FEV1 after provocation by histamine.59 Interestingly, vitamin D has antiproliferative effects on ASM, decelerating cell cycling and decreasing hyperplasia.60 Asthmatic ASM cells express higher levels of MMP-9, and ADAM metallopetidase domain 33(ADAM33) suppress disintegrin, and metalloprotease 33 when compared with nonasthmatic ASM cells. Treatment of asthmatic cells with vitamin D reduced the mRNA and protein expression of MMP-9 and ADAM33 genes.4 Further, polymorphisms in the VDR gene have been linked to increased airway resistance in mice.61 A study demonstrated that calcitriol (but not dexamethasone), added to human ASM cultures, inhibited platelet-derived growth factor-induced DNA synthesis. These effects were associated with VDR-mediated expression of CYP24A1, with no effect on apoptosis of ASM cells.62
Gupta et al described major evidence for a role for vitamin D in remodeling in a study of children with severe therapy-resistant asthma. Remodeling was assessed by endobronchial biopsy. Lower vitamin D levels were associated with increased ASM mass and worse asthma control and lung function. ASM mass, but not epithelial shedding or reticular basement membrane thickness, was inversely related to 25(OH)D(3) levels.63
Cysteinyl leukotrienes (LTC4, LTD4) synthesized from arachidonic acid can increase ASM mass, and prostaglandins are even more effective than leukotrienes for inducing ASM remodeling.40 Vitamin D significantly reduced production of prostaglandin E2, regulating its synthesis and degradation by human lung fibroblasts, without any effect on production of TGF-β1, vascular endothelial growth factor (VEGF), or fibronectin. Vitamin D can modulate fibroblast-mediated tissue repair function via this mechanism.64
Human rhinovirus infections are the main trigger for asthma exacerbations.65 Viruses may contribute to airway remodeling by increasing deposition of extracellular matrix, which in turn may contribute to increased ASM mass via increased cell migration.66 Rhinovirus infection induces epithelial production of a number of growth factors and other mediators, eg, activin A and amphiregulin, that are linked to subepithelial membrane thickening, and MMP9 and VEGF, which could contribute to development and progression of the airway remodeling processes in asthma.42 In vitro, rhinovirus induces release of basic fibroblast growth factor by human airway epithelium, and stimulates fibroblast proliferation together with increased metalloproteinase activity.67 Primary human bronchial epithelial cells were treated with vitamin D, and rhinovirus replication and gene expression were evaluated by quantitative polymerase chain reaction.68 Vitamin D did not directly affect replication of rhinovirus in airway epithelial cells, but did influence chemokine synthesis and alter the growth and differentiation of airway epithelial cells. In vitro, treatment of epithelial lung cells with vitamin D significantly decreased H1N1-induced inflammatory cytokine transcription levels.69 Human cathelicidin LL-37 and murine cathelicidin (cathelin-related antimicrobial peptide), expression of which is regulated by VDR activation, showed antiviral activity and modulated the immune response to viral infections.70 Downregulation of expression of monocyte Toll-like receptors by calcitriol leads to reduced production of the proinflammatory cytokine TNF-α in response to stimulation with Toll-like receptor ligands.46 Therefore, vitamin D sufficiency may be important for overall maintenance of pulmonary health via control of innate and adaptive immune inflammatory responses.46
VEGF is a key mediator of angiogenesis and is able to modulate ASM.71 Blood levels of VEGF are significantly increased in asthmatic patients compared with healthy controls. Circulating VEGF levels are inversely correlated with percent predicted FEV1, suggesting a relationship between VEGF production and bronchial remodeling.72 Induction of VEGF may be a potential mechanism via which particulate matter in the urban environment influences lung function in children.73 Isocyanate-induced occupational asthma is associated with upregulated expression of vitamin D-binding protein. In vitro, exposure of epithelial cells to isocyanate induces increased production of VEGF which is reversed by treatment with calcitriol.74 However, in other situations, vitamin D promotes production of VEGF.75
Airway remodeling is considered to be a repair process occurring after injury to the epithelium. Cellular senescence has been examined in lung specimens from patients with asthma, and activation of cellular senescence was detected in epithelial airway samples. Moreover, induction of cellular senescence has been shown to be required for airway remodeling in vitro, and inhibition of cellular senescence blocked airway remodeling.76 Vitamin D deficiency is involved in senescence of different organs by inducing DNA damage, cellular senescence, and production of senescence-associated inflammatory cytokines and MMPs.77
Vitamin D involvement in lung development is important to consider, as remodeling occurs very early in the course of asthma. In fact, vitamin D stimulates synthesis of alveolar type II cell DNA and surfactant production.3 Mouse pups born to mothers with vitamin D deficiency were shown to have decreased lung function, primarily as a result of reduced lung volume. In the same way, lung compliance was decreased in rat pups born to vitamin D-deficient mothers.78 Moreover, the authors of a study on remodeling in severe asthma of childhood hypothesized that ASM hypertrophy resulted from vitamin D deficiency in utero.63 As such, vitamin D deficiency may predispose to asthma or increase the morbidity associated with asthma by altering lung development in early life.3
Potential prevention and reversal of remodeling
Recombinant adeno-associated virus containing antisense against the IL-4 gene (rAAV-asIL4) vector can significantly suppress the expression of IL-4 protein and airway inflammation in the rat. Interestingly, rAAV-asIL4 decreases collagen deposition beneath the basement membrane, suggesting the potential to attenuate the airway remodeling process by inhibition of airway inflammation.45 In the same way, treatment with anti-immunoglobulin E antibody inhibited the development of airway hyperresponsiveness, eosinophilic inflammation, and airway remodeling.79 Vitamin D, by inhibition of Th2 cytokine production, can enhance the effect of asthma drugs on remodeling. Budesonide and formoterol, both alone or in combination, were shown to effectively inhibit bradykinin-induced differentiation of fibroblasts into myofibroblasts and to have the potential to inhibit fibroblast-dependent matrix remodeling in the airways of asthmatic patients. However, there was no consistent evidence of an inhibitory effect of steroids on remodeling.49 Arachidonic acid-derived mediators, ie, cysteinyl leukotrienes and prostaglandins, production of which is decreased by vitamin D, constitute a potential target for modulation of remodeling.40 Monthly vitamin D doses of 60,000 IU significantly reduced the number of exacerbations and improved lung function tests.80 Further, vitamin D supplementation improved symptom scores and decreased steroid requirements, and also increased the Treg subset.81 One plausible mechanism for this reversibility effect on steroid resistance is upregulation of FOXP3 in Tregs by vitamin D.4
Vitamin D supplementation
Data suggesting that vitamin D deficiency results in an increased risk of asthma and allergy continues to accumulate. However, the amount of vitamin D required to decrease the risk for both development and severity of these disorders is still unknown, and the results of ongoing clinical trials on vitamin D supplementation are needed before recommendations can be firmly established.82
With regard to vitamin D supplementation during pregnancy, two epidemiologic studies have shown that higher vitamin D intake is associated with a reduction in the risk of recurrent wheeze in children.83,84 Further, Errkola et al found lower rates of allergic rhinitis and asthma in 5-year-old children whose mothers had a higher vitamin D intake during pregnancy.85 In contrast, a study from the UK reported an increased risk of eczema and asthma in children born to women with higher levels of vitamin D (>75 nmol/L or 30 ng/mL).86 Wjst et al suggested that exposure to higher doses of vitamin D in utero might be a risk factor for development of atopic disorders, and suggested that the current asthma epidemic may be due to food supplementation with vitamin D.87
The large, randomized, multicenter Vitamin D Antenatal Asthma Reduction Trial is testing the hypothesis that vitamin D supplementation in pregnant women can prevent asthma and allergic diseases.88 In the Prevention and Incidence of Asthma and Mite Allergy birth cohort, serum vitamin D concentrations at age 4 years were inversely associated with asthma at the age of 4–8 years.89 However, a trial of supplementation with vitamin D in late pregnancy showed no effect on wheeze frequency or lung function in offspring by the age of 3 years.90 In this study, supplementation improved but did not optimize vitamin D status.90
Even if more evidence is still required to support supplementation of vitamin D to prevent asthma, positive data have been reported with respect to vitamin D supplementation as a common treatment for asthma, with the effect of decreasing the frequency of exacerbation and improving steroid sensitivity.18,91 In a recent prospective study,18 vitamin D supplementation in asthmatic children appeared to prevent exacerbation of asthma triggered by acute respiratory infection. Further, Majak et al18 compared two groups of asthmatic children who were treated with inhaled corticosteroids with or without vitamin D3 supplementation. Children treated with steroids and placebo experienced more asthma exacerbations and had more severe clinical manifestations than children with treated with steroids and vitamin D3. In addition, vitamin D supplementation improved antimicrobial defense against respiratory tract infections.92,93
Conclusion
As shown in this review, airway remodeling involves structural changes in the walls of the airways induced by repeated injury and repair processes, and is characterized by changes in tissue, cellular, and molecular composition affecting the ASM, epithelium, blood vessels, extracellular matrix, and defective lung–blood barriers. Airway remodeling is an early event in asthma and other lung diseases, and is arguably one of the most intractable problems leading to irreversible loss of lung function. Vitamin D may influence airway remodeling by affecting the growth and contractility of ASM and inhibiting TGF-β and MMPs, as well as fibroblast proliferation, promoting antimicrobial pathways, and suppressing Treg activity, as summarized in Figure 1.
Our knowledge regarding direct mechanistic links between vitamin D and lung disease is limited. In view of the available data, vitamin D insufficiency can be said to be associated with the severity of childhood asthma and airway remodeling. According to experimental evidence, several pathways involve hypovitaminosis D in remodeling, ie, development of alterations in the lung and accelerated cellular senescence associated with an unbalanced process of repair, with excessive Th2 inflammation, fibroblast activation, and smooth muscle cell hypertrophy, suggesting a beneficial therapeutic impact of supplementation on reversal of remodeling. However, major evidence supporting the beneficial effect of vitamin D supplementation on remodeling is needed. Vitamin D supplementation does inhibit several profibrotic mediators and production of growth factors in vitro, but the results of clinical trials are still controversial. The issue lies within the link of causality between vitamin D insufficiency and asthma. Although vitamin D is definitely necessary for pulmonary health, the low levels observed in asthma could be due to the inflammatory process and simply considered as a marker of severity. Recommendations cannot be made regarding vitamin D in asthma until the results of ongoing clinical trials become available.
Disclosure
The authors report no conflicts of interests in this work.
References
Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357:266–281. | |
Nagpal S, Na S, Rathnachalam R. Noncalcemic actions of vitamin D receptor ligands. Endocr Rev. 2005;26:662–687. | |
Paul G, Brehm JM, Alcorn JF, Holguín F, Aujla SJ, Celedón JC. Vitamin D and asthma. Am J Respir Crit Care Med. 2012;185:124–132. | |
Poon AH, Mahboub B, Hamid Q. Vitamin D deficiency and severe asthma. Pharmacol Ther. 2013;140:148–155. | |
Camargo CA Jr, Ingham T, Wickens K, et al. Cord-blood 25-hydroxyvitamin D levels and risk of respiratory infection, wheezing, and asthma. New Zealand Asthma and Allergy Cohort Study Group Pediatrics. 2011;127:e180–e187. | |
Freishtat RJ, Iqbal SF, Pillai DK, et al. High prevalence of vitamin D deficiency among inner-city African American youth with asthma in Washington, DC. J Pediatr. 2010;156:948–952. | |
Bener A, Ehlayel MS, Tulic MK, Hamid Q. Vitamin D deficiency as a strong predictor of asthma in children. Int Arch Allergy Immunol. 2012;157:168–175. | |
Alyasin S, Momen T, Kashef S, Alipour A, Amin R. The relationship between serum 25 hydroxyvitamin D levels and asthma in children. Allergy Asthma Immunol Res. 2011;3:251–255. | |
Chinellato I, Piazza M, Sandri M, et al. Serum vitamin D levels and exercise-induced bronchoconstriction in children with asthma. Eur Respir J. 2011;37:1366–1370. | |
Chinellato I, Piazza M, Sandri M, Peroni D, Piacentini G, Boner AL. Vitamin D serum levels and markers of asthma control in Italian children. J Pediatr. 2011;158:437–441. | |
Burns JS, Dockery DW, Neas LM, et al. Low dietary nutrient intakes and respiratory health in adolescents. Chest. 2007;132:238–245. | |
Black PN, Scragg R. Relationship between serum 25-hydroxyvitamin D and pulmonary function in the third national health and nutrition examination survey. Chest. 2005;128:3792–3798. | |
Sutherland ER, Goleva E, Jackson LP, Stevens AD, Leung DY. Vitamin D levels, lung function, steroid response in adult asthma. Am J Respir Crit Care Med. 2010;181:699–704. | |
Li F, Peng M, Jiang L, et al. Vitamin D deficiency is associated with decreased lung function in Chinese adults with asthma. Respiration. 2011;81:469–475. | |
Searing DA, Zhang Y, Murphy JR, Hauk PJ, Goleva E, Leung DY. Decreased serum vitamin D levels in children with asthma are associated with increased corticosteroid use. J Allergy Clin Immunol. 2010;125:955–1000. | |
Brehm JM, Celedòn JC, Soto-Quiros ME, et al. Serum vitamin D levels and markers of severity of childhood asthma in Costa Rica. Am J Respir Crit Care Med. 2009;179:765–771. | |
Brehm JM, Schuemann B, Fuhlbrigge AL, et al. Serum vitamin D levels and severe asthma exacerbations in the childhood asthma management program study. J Allergy Clin Immunol. 2010;126:52–58. | |
Majak P, Olszowiec-Chlebna M, Smejda K, Stelmach I. Vitamin D supplementation in children may prevent asthma exacerbation triggered by acute respiratory infection. J Allergy Clin Immunol. 2011;127:1294–1296. | |
Devereux G, Wilson A, Avenell A, McNeill G, Fraser WD. A case-control study of vitamin D status and asthma in adults. Allergy. 2010;65:666–667. | |
Hughes AM, Lucas RM, Ponsonby AL, et al. The role of latitude, ultraviolet radiation exposure and vitamin D in childhood asthma and hayfever: an Australian multicenter study. Pediatr Allergy Immunol. 2011;22:327–333. | |
Huang H, Porpodis K, Zarogoulidis P, et al. Vitamin D in asthma and future perspectives. Drug Des Devel Ther. 2013;7:1003–1013. | |
Raby BA, Lazarus R, Silverman EK, et al. Association of vitamin D receptor gene polymorphisms with childhood and adult asthma. Am J Respir Crit Care Med. 2004;170:1057–1065. | |
Poon AH, Laprise C, Lemire M, et al. Association of vitamin D receptor genetic variants with susceptibility to asthma and atopy. Am J Respir Crit Care Med. 2004;170:967–973. | |
Maalmi H, Sassi FH, Berraies A, Ammar J, Hamzaoui K, Hamzaoui A. Association of vitamin D receptor gene polymorphisms with susceptibility to asthma in Tunisian children: a case control study. Hum Immunol. 2013;74:234–240. | |
Bosse Y, Maghni K, Hudson TJ. 1α,25-dihydroxy-vitamin D3 stimulation of bronchial smooth muscle cells induces autocrine, contractility, and remodeling processes. Physiol Genomics. 2007;29:161–168. | |
Reardon BJ, Hansen JG, Crystal RG, et al. Vitamin D-responsive SGPP2 variants associated with lung cell expression and lung function. BMC Med Genet. 2013;14:122. | |
Hewison M. Vitamin D and the intracrinology of innate immunity. Mol Cell Endocrinol. 2010;321:103–111. | |
Provvedini DM, Tsoukas CD, Deftos LJ, Manolagas SC. 1,25 dihydroxyvitamin D3 receptors in human leukocytes. Science. 1983;221:1181–1183. | |
Wang Y, Zhu J, DeLuca HF. Where is the vitamin D receptor? Arch Biochem Biophys. 2012;523:123–133. | |
Baeke F, Korf H, Overbergh L, et al. Human T lymphocytes are direct targets of 1,25-dihydroxyvitamin D3 in the immune system. J Steroid Biochem Mol Biol. 2010;121:221–227. | |
Wittke A, Weaver V, Mahon BD, August A, Cantorna MT. Vitamin D receptor-deficient mice fail to develop experimental allergic asthma. J Immunol. 2004;173:3432–3436. | |
Urry Z, Chambers ES, Xystrakis E, et al. The role of 1α,25-dihydroxyvitamin D3 and cytokines in the promotion of distinct Foxp3+ and IL-10+ CD4+ T cells. Eur J Immunol. 2012;42:2697–2708. | |
Gregori S, Casorati M, Amuchastegui S, Smiroldo S, Davalli AM, Adorini L. Regulatory T cells induced by 1 alpha,25-dihydroxyvitamin D3 and mycophenolate mofetil treatment mediate transplantation tolerance. J Immunol. 2001;167:1945–1953. | |
Maalmi H, Berraies A, Tangour E, et al. The impact of vitamin D deficiency on immune T cells in asthmatic children: a case-control study. J Asthma Allergy. 2012;5:11–19. | |
Tang J, Zhou R, Luger D, et al. Calcitriol suppresses antiretinal autoimmunity through inhibitory effects on the Th17 effector response. J Immunol. 2009;182:4624–4632. | |
Daniel C, Sartory NA, Zahn N, et al. Immune modulatory treatment of trinitrobenzene sulfonic acid colitis with calcitriol is associated with a change of a T helper (Th) 1/Th17 to a Th2 and regulatory T cell profile. J Pharmacol Exp Ther. 2008;324:23–33. | |
Nanzer AM, Chambers ES, Ryanna K, et al. Enhanced production of IL-17A in patients with severe asthma is inhibited by 1α,25-dihydroxyvitamin D3 in a glucocorticoid-independent fashion. J Allergy Clin Immunol. 2013;132:297–304. | |
Wu AC, Tantisira K, Li L, Fuhlbrigge AL, Weiss ST, Litonjua A; Childhood Asthma Management Program Research Group. Effect of vitamin D and inhaled corticosteroid treatment on lung function in children. Am J Respir Crit Care Med. 2012;186:508–513. | |
Beard JA, Bearden A, Striker R. Vitamin D and the anti-viral state. J Clin Virol. 2011;50:194–200. | |
Prakash YS. Airway smooth muscle in airway reactivity and remodeling: what have we learned? Am J Physiol Lung Cell Mol Physiol. 2013;305:L912–L933. | |
Yamauchi K, Inoue H. Airway remodeling in asthma and irreversible airflow limitation-ECM deposition in airway and possible therapy for remodeling. Allergol Int. 2007;56:321–329. | |
Proud D. Role of rhinovirus infections in asthma. Asian Pac J Allergy Immunol. 2011;29:201–208. | |
Agrawal T, Gupta GK, Agrawal DK. Vitamin D supplementation reduces airway hyperresponsiveness and allergic airway inflammation in a murine model. Clin Exp Allergy. 2013;43:672–683. | |
Lai G, Wu C, Hong J, Song Y. 1,25-dihydroxyvitamin D(3) (1,25-(OH)(2)D(3) attenuates airway remodeling in a murine model of chronic asthma. J Asthma. 2013;50:133–140. | |
Cao Y, Zeng D, Song Q, et al. The effects of antisense interleukin-4 gene transferred by recombinant adeno-associated virus vector on the airway remodeling in allergic rats. J Asthma. 2010;47:951–958. | |
Dimeloe S, Nanzer A, Ryanna K, Hawrylowicz C. Regulatory T cells, inflammation and the allergic response – the role of glucocorticoids and vitamin D. J Steroid Biochem Mol Biol. 2010;120:86–95. | |
Ramirez AM, Wongtrakool C, Welch T, Steinmeyer A, Zügel U, Roman J. Vitamin D inhibition of pro-fibrotic effects of transforming growth factor beta1 in lung fibroblasts and epithelial cells. J Steroid Biochem Mol Biol. 2010;118:142–150. | |
Yang ZC, Yi MJ, Ran N, et al. Transforming growth factor-β1 induces bronchial epithelial cells to mesenchymal transition by activating the Snail pathway and promotes airway remodeling in asthma. Mol Med Rep. 2013;8:1663–1668. | |
Sabatini F, Petecchia L, Usai C, et al. Pharmacological modulation of the bradykinin-induced differentiation of human lung fibroblasts: effects of budesonide and formoterol. J Asthma. 2012;49:1004–1011. | |
Sundar IK, Hwang JW, Wu S, Sun J, Rahman I. Deletion of vitamin D receptor leads to premature emphysema/COPD by increased matrix metalloproteinases and lymphoid aggregates formation. Biochem Biophys Res Commun. 2011;406:127–133. | |
Anand SP, Selvaraj P. Effect of 1, 25 dihydroxyvitamin D(3) on matrix metalloproteinases MMP-7, MMP-9 and the inhibitor TIMP-1 in pulmonary tuberculosis. Clin Immunol. 2009;133:126–131. | |
Meephansan J, Komine M, Tsuda H, Ohtsuki M. Suppressive effect of calcipotriol on the induction of matrix metalloproteinase (MMP)-9 and MMP-13 in a human squamous cell carcinoma cell line. Clin Exp Dermatol. 2012;37:889–896. | |
Johnson LA, Sauder KL, Rodansky ES, Simpson RU, Higgins PD. CARD-024, a vitamin D analog, attenuates the pro-fibrotic response to substrate stiffness in colonic myofibroblasts. Exp Mol Pathol. 2012;93:91–98. | |
Bahar-Shany K, Ravid A, Koren R. Upregulation of MMP-9 production by TNF alpha in keratinocytes and its attenuation by vitamin D. J Cell Physiol. 2010;222:729–737. | |
Chen Y, Zhang J, Ge X, et al. Vitamin D receptor inhibits nuclear factor κB activation by interacting with IκB kinase β protein. J Biol Chem. 2013;288:19450–19458. | |
Bentley JK, Hershenson MB. Airway smooth muscle growth in asthma: proliferation, hypertrophy, and migration. Proc Am Thorac Soc. 2008;5:89–96. | |
Bergeron C, Boulet LP. Structural changes in airway diseases: characteristics, mechanisms, consequences, and pharmacologic modulation. Chest. 2006;129:1068–1087. | |
Goleva E, Hauk PJ, Boguniewicz J, et al. Airway remodeling and lack of bronchodilator response in steroid-resistant asthma. J Allergy Clin Immunol. 2007;120:1065–1072. | |
Tsurikisawa N, Oshikata C, Tsuburai T, et al. Bronchial reactivity to histamine is correlated with airway remodeling in adults with moderate to severe asthma. J Asthma. 2010;47:841–848. | |
Iqbal SF, Freishtat RJ. Mechanism of action of vitamin D in the asthmatic lung. J Investig Med. 2011;59:1200–1202. | |
Berndt A, Savage HS, Stearns TM, Paigen B. Genetic analysis of lung functioning inbred mice suggests vitamin D receptor as a candidate gene. Mol Genet Genomics. 2011;286:237–246. | |
Damera G, Fogle HW, Lim P, et al. Vitamin D inhibits growth of human airway smooth muscle cells through growth factor-induced phosphorylation of retinoblastoma protein and checkpoint kinase 1. Br J Pharmacol. 2009;158:1429–1441. | |
Gupta A, Sjoukes A, Richards D, et al. Relationship between serum vitamin D, disease severity, and airway remodeling in children with asthma. Am J Respir Crit Care Med. 2011;184:1342–1349. | |
Liu X, Nelson A, Wang X, et al. Vitamin D modulates PGE2 synthesis and degradation in human lung fibroblasts. Am J Respir Cell Mol Biol. 2014;50:40–50. | |
Wark PA, Tooze M, Powell H, Parsons K. Viral and bacterial infection in acute asthma and chronic obstructive pulmonary disease increases the risk of readmission. Respirology. 2013;18:996–1002. | |
Kuo C, Lim S, King NJ, et al. Rhinovirus infection induces extracellular matrix protein deposition in asthmatic and nonasthmatic airway smooth muscle cells. Am J Physiol Lung Cell Mol Physiol. 2011;300:L951–L957. | |
Skevaki CL, Psarras S, Volonaki E, et al. Rhinovirus-induced basic fibroblast growth factor release mediates airway remodeling features. Clin Transl Allergy. 2012;2:14. | |
Brockman-Schneider RA, Pickles RJ, Gern JE. Effects of vitamin D on airway epithelial cell morphology and rhinovirus replication. PLoS One. 2014;9:e86755. | |
Khare D, Godbole NM, Pawar SD, et al. Calcitriol [1, 25(OH)2 D3] pre- and post-treatment suppresses inflammatory response to influenza A (H1N1) infection in human lung A549 epithelial cells. Eur J Nutr. 2013;52:1405–1415. | |
Vandamme D, Landuyt B, Luyten W, Schoofs L. A comprehensive summary of LL-37, the factotum human cathelicidin peptide. Cell Immunol. 2012;280:22–35. | |
Makinde T, Murphy RF, Agrawal DK. Immunomodulatory role of vascular endothelial growth factor and angiopoietin-1 in airway remodeling. Curr Mol Med. 2006;6:831–841. | |
Lee KY, Lee KS, Park SJ, et al. Clinical significance of plasma and serum vascular endothelial growth factor in asthma. J Asthma. 2008;45:735–739. | |
Iwanaga K, Elliott MS, Vedal S, Debley JS. Urban particulate matter induces pro-remodeling factors by airway epithelial cells from healthy and asthmatic children. Inhal Toxicol. 2013;25:653–660. | |
Kim SH, Choi GS, Nam YH, et al. Role of vitamin D-binding protein in isocyanate-induced occupational asthma. Exp Mol Med. 2012;44:319–329. | |
Grundmann M, Haidar M, Placzko S, et al. Vitamin D improves the angiogenic properties of endothelial progenitor cells. Am J Physiol Cell Physiol. 2012;303:C954–C962. | |
Wu J, Dong F, Wang RA, et al. Central role of cellular senescence in TSLP-induced airway remodeling in asthma. PLoS One. 2013;8:e77795. | |
Shen M, Luo Y, Niu Y, et al. 1,25(OH)2D deficiency induces temporomandibular joint osteoarthritis via secretion of senescence-associated inflammatory cytokines. Bone. 2013;55:400–409. | |
Gaultier C, Harf A, Balmain N, Cuisinier-Gleizes P, Mathieu H. Lung mechanics in rachitic rats. Am Rev Respir Dis. 1984;130:1108–1110. | |
Kang JY, Kim JW, Kim JS, et al. Inhibitory effects of anti-immunoglobulin E antibodies on airway remodeling in a murine model of chronic asthma. J Asthma. 2010;47:374–380. | |
Yadav M, Mittal K. Effect of vitamin D supplementation on moderate to severe bronchial asthma. Indian J Pediatr. November 6, 2013. [Epub ahead of print]. | |
Baris S, Kiykim A, Ozen A, Tulunay A, Karakoc-Aydiner E, Barlan IB. Vitamin D as an adjunct to subcutaneous allergen immunotherapy in asthmatic children sensitized to house dust mite. Allergy. 2014;69:246–253. | |
Litonjua AA. Vitamin D deficiency as a risk factor for childhood allergic disease and asthma. Curr Opin Allergy Clin Immunol. 2012;12:179–185. | |
Camargo CA Jr, Rifas-Shiman SL, Litonjua AA, et al. Maternal intake of vitamin D during pregnancy and risk of recurrent wheeze in children at 3 y of age. Am J Clin Nutr. 2007;85:788–795. | |
Devereux G, Litonjua AA, Turner SW, et al. Maternal vitamin D intake during pregnancy and early childhood wheezing. Am J Clin Nutr. 2007;85:853–859. | |
Erkkola M, Kaila M, Nwaru BI, et al. Maternal vitamin D intake during pregnancy is inversely associated with asthma and allergic rhinitis in 5-year-old children. Clin Exp Allergy. 2009;39:875–882. | |
Gale CR, Robinson SM, Harvey NC, et al. Maternal vitamin D status during pregnancy and child outcomes. Eur J Clin Nutr. 2008;62:68–77. | |
Wjst M, Dold S. Genes, factor X, and allergens: what causes allergic diseases? Allergy. 1999;54:757–759. | |
ClinicalTrials.gov. Maternal Vitamin D Supplementation to Prevent Childhood Asthma (VDAART). Available from: http://clinicaltrials.gov/ct2/show/NCT00920621. Accessed February 14, 2014. | |
Van Oeffelen AA, Bekkers MB, Smit HA, et al. Serum micronutrient concentrations and childhood asthma: the PIAMA birth cohort study. Pediatr Allergy Immunol. 2011;22:784–793. | |
Goldring ST, Griffiths CJ, Martineau AR, et al. Prenatal vitamin D supplementation and child respiratory health: a randomised controlled trial. PLoS One. 2013;8:e66627. | |
Xystrakis E, Kusumakar S, Boswell S, et al. Reversing the defective induction of IL-10–secreting regulatory T cells in glucocorticoid-resistant asthma patients. J Clin Invest. 2006;116:146–155. | |
Gunville CF, Mourani PM, Ginde AA. The role of vitamin D in prevention and treatment of infection. Inflamm Allergy Drug Targets. 2013;12:239–245. | |
Laaksi I, Ruohola JP, Mattila V, Auvinen A, Ylikomi T, Pihlajamäki H. Vitamin D supplementation for the prevention of acute respiratory tract infection: a randomized, double-blinded trial among young Finnish men. J Infect Dis. 2010;202:809–814. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.