")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 19
Lack of Evidence Regarding Markers Identifying Acute Heart Failure in Patients with COPD: An AI-Supported Systematic Review
Authors van Dijk SHB , Brusse-Keizer MGJ , Bucsán CC, Ploumen EH, van Beurden WJC , van der Palen J , Doggen CJM , Lenferink A
Received 26 September 2023
Accepted for publication 30 January 2024
Published 23 February 2024 Volume 2024:19 Pages 531—541
DOI https://doi.org/10.2147/COPD.S437899
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Sanne HB van Dijk,1,2 Marjolein GJ Brusse-Keizer,1,3 Charlotte C Bucsán,2,4 Eline H Ploumen,1,5 Wendy JC van Beurden,2 Job van der Palen,3,4 Carine JM Doggen,1,6 Anke Lenferink1,2,6
1Health Technology & Services Research, Technical Medical Centre, University of Twente, Enschede, the Netherlands; 2Department of Pulmonary Medicine, Medisch Spectrum Twente, Enschede, the Netherlands; 3Medical School Twente, Medisch Spectrum Twente, Enschede, the Netherlands; 4Cognition, Data & Education, Faculty of Behavioural, Management & Social Sciences, University of Twente, Enschede, the Netherlands; 5Department of Cardiology, Medisch Spectrum Twente, Enschede, the Netherlands; 6Clinical Research Centre, Rijnstate Hospital, Arnhem, the Netherlands
Correspondence: Anke Lenferink, Health Technology & Services Research, Technical Medical Centre, University of Twente, Hallenweg 5, Enschede, NH, 7522, the Netherlands, Tel +31 0534896311, Email [email protected]
Background: Due to shared symptoms, acute heart failure (AHF) is difficult to differentiate from an acute exacerbation of COPD (AECOPD). This systematic review aimed to identify markers that can diagnose AHF underlying acute dyspnea in patients with COPD presenting at the hospital.
Methods: All types of observational studies and clinical trials that investigated any marker’s ability to diagnose AHF in acutely dyspneic COPD patients were considered eligible for inclusion. An AI tool (ASReview) supported the title and abstract screening of the articles obtained from PubMed, Scopus, Web of Science, the Cochrane Library, Embase, and CINAHL until April 2023. Full text screening was independently performed by two reviewers. Twenty percent of the data extraction was checked by a second reviewer and the risk of bias was assessed in duplicate using the QUADAS-2 tool. Markers’ discriminative abilities were evaluated in terms of sensitivity, specificity, positive and negative predictive values, and the area under the curve when available.
Results: The search identified 10,366 articles. After deduplication, title and abstract screening was performed on 5,386 articles, leaving 153 relevant, of which 82 could be screened full text. Ten distinct studies (reported in 16 articles) were included, of which 9 had a high risk of bias. Overall, these studies evaluated 12 distinct laboratory and 7 non-laboratory markers. BNP, NT-proBNP, MR-proANP, and inspiratory inferior vena cava diameter showed the highest diagnostic discrimination.
Conclusion: There is not much evidence for the use of markers to diagnose AHF in acutely dyspneic COPD patients in the hospital setting. BNPs seem most promising, but should be interpreted alongside imaging and clinical signs, as this may lead to improved diagnostic accuracy. Future validation studies are urgently needed before any AHF marker can be incorporated into treatment decision-making algorithms for patients with COPD.
Protocol Registration: CRD42022283952.
Keywords: COPD, chronic heart failure, biomarkers, systematic review, differential diagnosis
Introduction
Chronic obstructive pulmonary disease (COPD) is the third most important cause of death worldwide,1 and known for progressive deterioration of lung function.2 In 8% to 23% of COPD patients, comorbid chronic heart failure (CHF) is diagnosed,3 doubling their risk of death and reducing their quality of life.4 The coexistence of COPD and CHF is not surprising, given that they share several risk factors, smoking giving the highest risk.3 Both COPD and CHF are chronic progressive diseases characterized by periods of deteriorated symptoms. However, acute exacerbations of COPD (AECOPD) and acute heart failure (AHF) require different additional treatment. In an acute situation, diagnosis of AHF in COPD patients can be particularly difficult, given that AECOPD and AHF share symptoms such as acute worsening of dyspnea,5 but also often occur simultaneously.6
A systematic review published in 2018 showed that none of the signs and symptoms, with which acutely dyspneic patients present at the emergency department (ED), are acceptably sensitive nor specific to rule in or out AECOPD and AHF.7 Although this review did not investigate other diagnostic approaches besides signs and symptoms,7 it endorses that relying solely on signs and symptoms is insufficient. Furthermore, most laboratory tests are neither sensitive nor specific enough to rule in or out cardiac or lung disease as the cause of dyspnea, as an expert narrative review stated.3 Timely recognition of AHF, however, is crucial in the treatment and management of COPD,2,8–10 given the fact that up to 26% of AECOPDs may be triggered by the heart.10 Despite this knowledge, AHF is often overlooked as a possible (co-existing) cause of acutely worsened dyspnea in COPD patients.4 Hence, many patients receive initial treatment for AECOPD only,11 whereas (additional) treatment for AHF would have been appropriate and important to limit further cardiac deterioration.12
(Bio)markers have proven to be useful in AECOPD diagnosis,13,14 and might also aid the diagnosis of AHF in COPD. The most recent clinical guidelines regarding COPD proposes the same diagnostic approach for AHF in COPD patients compared to non-COPD patients, which includes (bio)marker use.2 Currently, cardiac markers, such as N-terminal pro b-type natriuretic peptide (NT-proBNP), are commonly used to rule in or out AHF in suspect patients presenting at the hospital after interpretation of the results of physical examination, electrocardiography, and imaging.12 However, these markers might also be elevated in COPD patients and are, therefore, not as specific as compared to non-COPD patients.15–17 By using sensitive and specific diagnostic markers of AHF in COPD patients, appropriate and timely treatment could be given. Thereby, disease progression could be delayed,10 and the length of hospital stay may be shortened.
Given the mentioned limitations of the current diagnostic procedures, it is important to improve differentiating AHF from AECOPD in patients with COPD presenting with acute dyspnea in the clinic, as patients would clearly benefit from improved diagnostics. However, a systematic overview of potential useful (bio)markers for this purpose is still lacking, for laboratory as well as for non-laboratory markers. This systematic review therefore aimed to assess which markers are able to diagnose AHF in acutely dyspneic COPD patients presenting at the hospital. This provides a knowledge base that contributes to more accurate diagnoses and differentiation between AHF and AECOPDs.
Methods
This report is in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.18 The review protocol was registered in PROSPERO (CRD42022283952).
Search Strategy
To identify relevant articles, PubMed, Scopus, Web of Science, Embase, the Cochrane Library, and CINAHL were searched until April 24, 2023 without filters or search restrictions. This review combined the terms (and their synonyms) “COPD”, “Heart failure”, and “Marker”. A detailed search strategy can be retrieved from the registered protocol as well as from Supplementary Table 1.
Study Selection
All search results were combined into one dataset within the reference manager software EndNote X9. Covidence was used as review manager software in the reviewing process.19 Duplicates were removed in EndNote first, and a second time in Covidence, given that EndNote is not very sensitive in identifying duplicates.20 The title and abstract screening were supported by the artificial intelligence (AI) tool ASReview version 0.17.21 This tool ranks the titles and abstracts of all articles on their probability of being relevant, based on earlier decisions used to train the algorithm. The article ranked number one by the AI tool is proposed to the reviewer, who then decides whether or not to include this article for full text screening. This decision is then again taken into account in the next ranking, and, consequently, the next number one article is proposed to the reviewer (ie, active learning). It is, thus, the AI tool that proposes articles based on probability of being relevant, but a human who decides which articles to in- and exclude.
An extensive description of how the AI-supported screening was applied and what choices were made for this review has been reported elsewhere.22 In brief, the used algorithm was trained with three relevant and three randomly selected irrelevant articles. The first reviewer (SvD) used the AI tool in the selection of articles until the predefined stopping criterion was reached. Twenty percent of the decisions based on title and abstract were again checked by a second reviewer (MBK, AL). The inter-reviewer agreement was relevant to assess, given that the reliability of the proposed articles by the AI tool depends on the decisions made by the first reviewer.
Full text articles were reviewed in duplicate (SvD, MBK, AL, CB, JvdP, CD). All types of observational studies with human subjects that investigated any marker’s ability to diagnose AHF in acutely dyspneic COPD patients were considered eligible for inclusion. Also, clinical trials that measured markers for the same purpose were considered eligible. Reviews, case studies, letters, and conference abstracts were excluded. Reference lists of included articles and relevant reviews identified by the search were screened to identify additional relevant articles. Only studies reporting original research of which full texts could be retrieved were considered for inclusion. The complete study selection process is visualized by a PRISMA flowchart (Figure 1) and verifiable through Supplementary Figure 1 and data files referred to in the data availability statement.
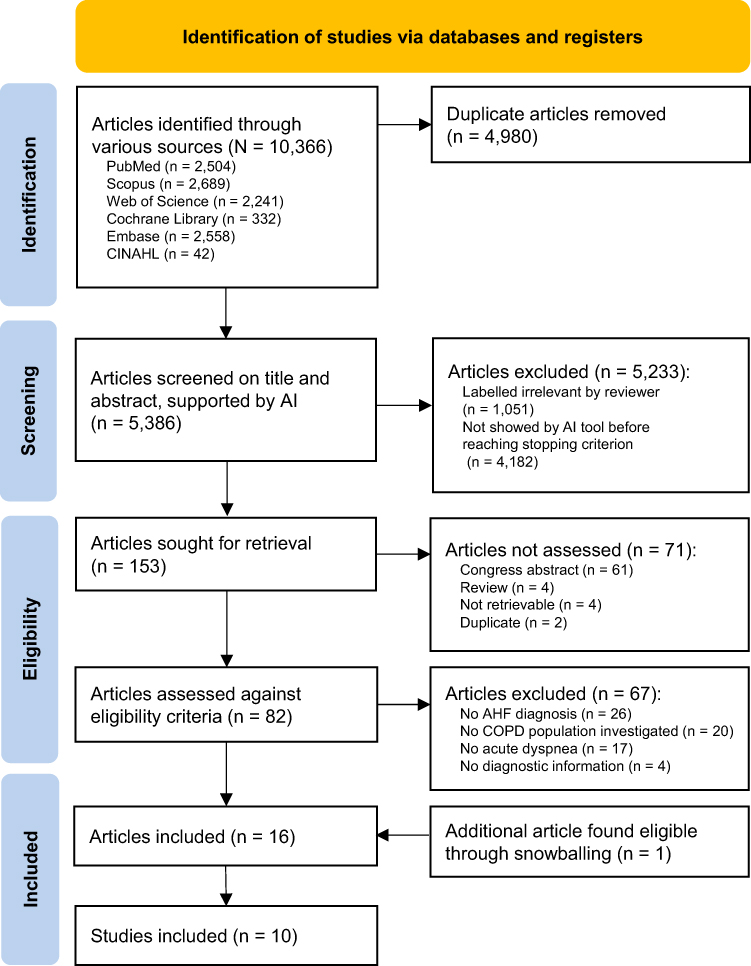 |
Figure 1 PRISMA flowchart reflecting the study selection process. Abbreviations: AHF, acute heart failure; COPD, Chronic Obstructive Pulmonary Disease. |
Data Extraction and Quality Assessment
The data extraction (ie, bibliographic and study information, population characteristics, performance of the marker) was performed by the first reviewer and a random 20% was checked by another reviewer (CB). In case the data for this review’s purpose was not sufficiently reported, authors were contacted and asked to provide the necessary data items. For example, in case a study was performed in the ED, subgroup data of only COPD patients were requested.
The study quality was assessed in duplicate (SvD, CB). For this purpose, the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) was used.23 The QUADAS-2 tool evaluates the individual studies’ risk of bias for four domains: patient selection, index test (ie, marker), reference standard (ie, AHF diagnostic criteria), and the flow of patients through the study and timing of the index test and reference standard (“flow and timing”, see Figure 2).23 A study was graded with an overall low risk of bias when it was assessed as low risk on all four risk of bias domains. When at least one risk of bias domain was assessed as unclear or with a high risk of bias, the overall study quality was judged as high risk of bias, in accordance with the QUADAS-2 guidelines.23 Furthermore, the extent to which the findings of a study are applicable to diagnostics in practice were assessed for the first three domains as low or high concern. Overall, applicability concerns with regard to a study were present when at least one of the three domains raised high concerns or was unclear.
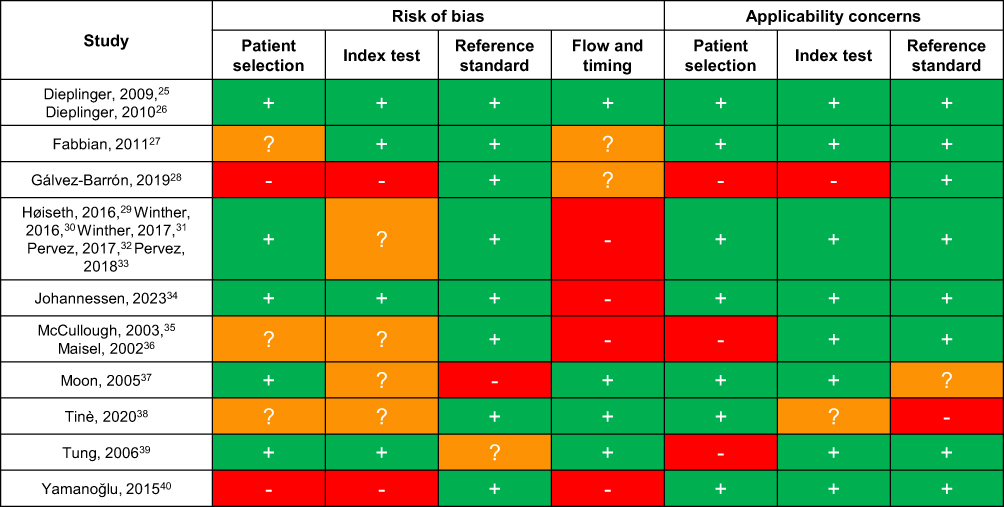 |
Figure 2 Risk of bias and applicability assessment, using the QUADAS-2 tool.22 Notes: red cells/-: high risk/concern; orange cells/?: unclear risk/concern; green cells/+: low risk/concern. |
Results
A concise overview of the study selection process is given in Figure 1. A more detailed overview of the AI-supported study selection is shown in Supplementary Figure 1. The search yielded 10,366 articles, of which 4,980 duplicates were removed. From the 5,386 articles that proceeded to the title and abstract screening, 1,204 (22%) articles were screened, whereafter the stopping criterion was reached and the 4,182 (78%) remaining articles were automatically excluded. Of the 1,204 articles screened on title and abstract, 153 were labelled relevant. The inter-reviewer agreement regarding titles and abstracts screened in the original search combined with the search update was strong (96% agreement, κ = 0.83).24 Of these relevant articles, 82 were original articles which could be retrieved full text, so these were screened in full text in duplicate. The other 71 were not assessed and, consequently, excluded. Additional data regarding subgroup analyses including only patients with a history of COPD or unclarities was requested from the authors of 24 out of the 82 articles. We received sufficient data of 7, but 17 articles had to be excluded. In total, 67 articles were excluded due to the reasons listed in Figure 1.
In total, 16 articles from 10 unique studies were included in this systematic review. The included studies are shown in Table 1, as are details regarding markers evaluated, inclusion period, study setting, AHF prevalence, reference standards and overall risk of bias. A more detailed assessment of the risk of bias and applicability is shown in Figure 2 and Supplementary Table 2. In the vast majority of studies, concerns or unclarities that may introduce a high risk of bias were observed. These concerns arise from inappropriate or unclear flow and timing domain in most studies. Also, concerns regarding the patient selection and index test domains result in a high risk of bias. Only one study25,26 had a low risk of bias. The overall impression is that the applicability (ie, whether included studies apply to the review question) of the included studies is of lower concern: five studies were assessed as low concern regarding applicability in practice (Figure 2).
 |
Table 1 Characteristics of 10 Included Studies |
Laboratory Tests
A summary of the diagnostic performances of the laboratory markers is shown in Table 2. Predominantly, B-type natriuretic peptide (BNP) was investigated, as was NT-proBNP. BNP was analyzed at different cut-off values across three studies showing sensitivities ranging from 92 to 100% and negative predictive values (NPV) from 94% to 100%.25,37,41 Good discriminative ability in terms of AUC (0.90) was reported in one study.39 NT-proBNP showed a sensitivity from 73% to 87% and NPV from 69% to 84%,27,39 and an AUC of 0.90.39 One study reported lower discriminative ability specifically among elderly COPD patients for NT-proBNP (AUC: 0.68, 95% CI: 0.48–0.88), although a higher cut-off value was used for the more elderly patients.27
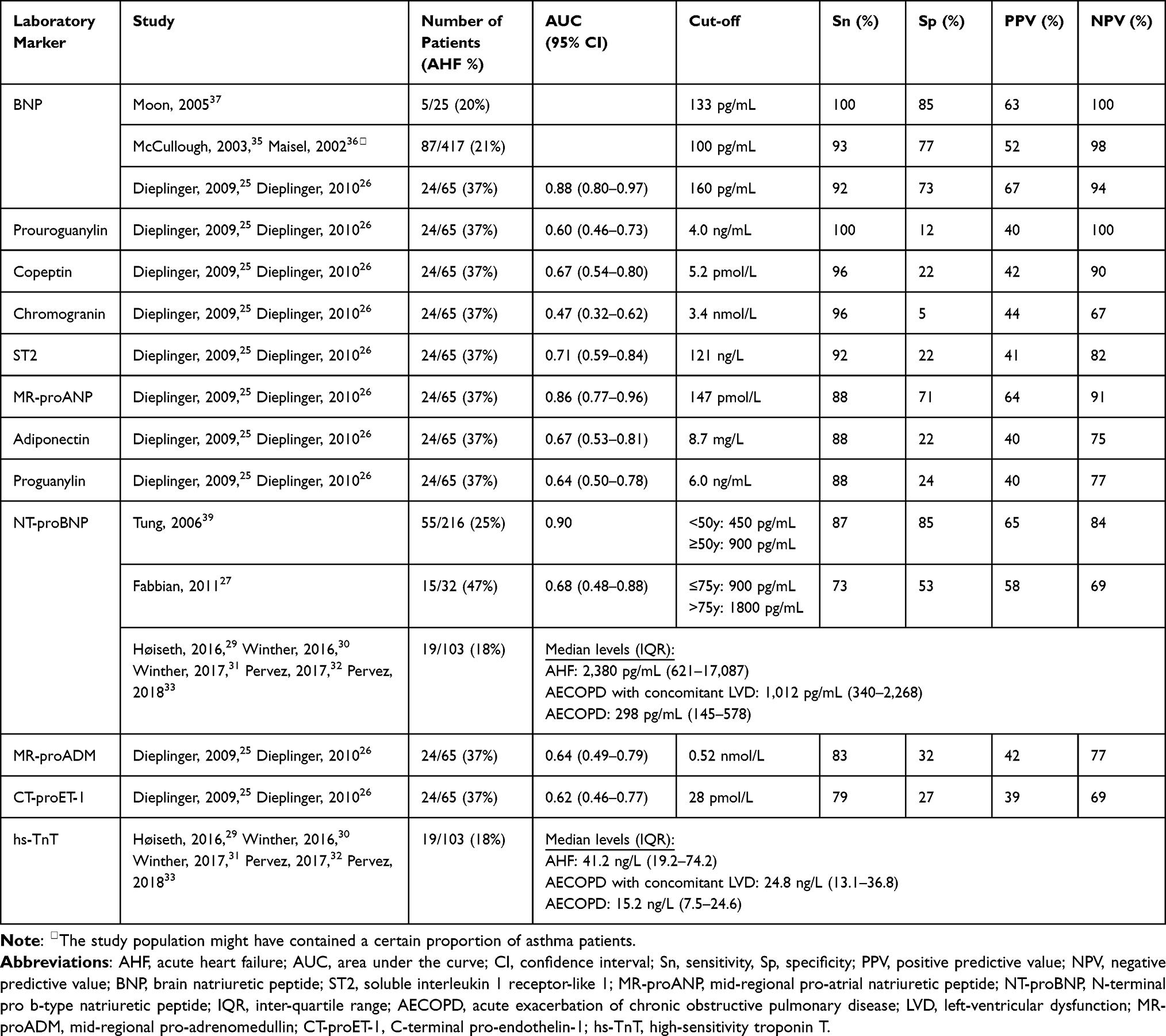 |
Table 2 Diagnostic Performances of Laboratory Markers Detecting AHF in Acutely Dyspneic Patients with COPD in a Hospital Setting |
One study25 evaluated several additional biomarkers in 65 patients with COPD that were not investigated in other studies. A few of these biomarkers showed an AUC significantly above 0.50, indicating discriminative ability better than random guessing. Midregional pro-atrial natriuretic peptide (MR-proANP) and copeptin showed a sensitivity of 88% and 96% and an NPV of 91% and 90%, respectively.25 The AUC of MR-proANP was 0.86 and of copeptin 0.67. The soluble interleukin 1 receptor-like 1 (ST2) cardiac biomarker had 92% sensitivity, 82% NPV and an 0.71 AUC. Adiponectin had 88% sensitivity, 75% NPV and a 0.67 AUC.25 The cut-off values that correspond to these sensitivity and NPV figures are shown in Table 2.
Non-Laboratory Tests
The diagnostic performance of several non-laboratory tests was assessed, including, for example, inferior vena cava (IVC) diameter and lung ultrasound which are also used as diagnostic tests in current clinical practice. The results of these tests are shown in Table 3. None of the vital signs showed discriminative performance. The maximum and minimum inspiratory IVC diameter were the only imaging markers with a high diagnostic accuracy (AUC significantly above 0.50), investigated in 55 COPD patients. The maximum IVC diameter (cut-off: 18.3 mm) showed a 74% sensitivity, an 83% NPV, and an AUC of 0.83 (95% CI: 0.72–0.94). The minimum IVC diameter (cut-off: 9.0 mm) had a 95% sensitivity, a 96% NPV, and an AUC of 0.90 (95% CI: 0.81–1.00).40
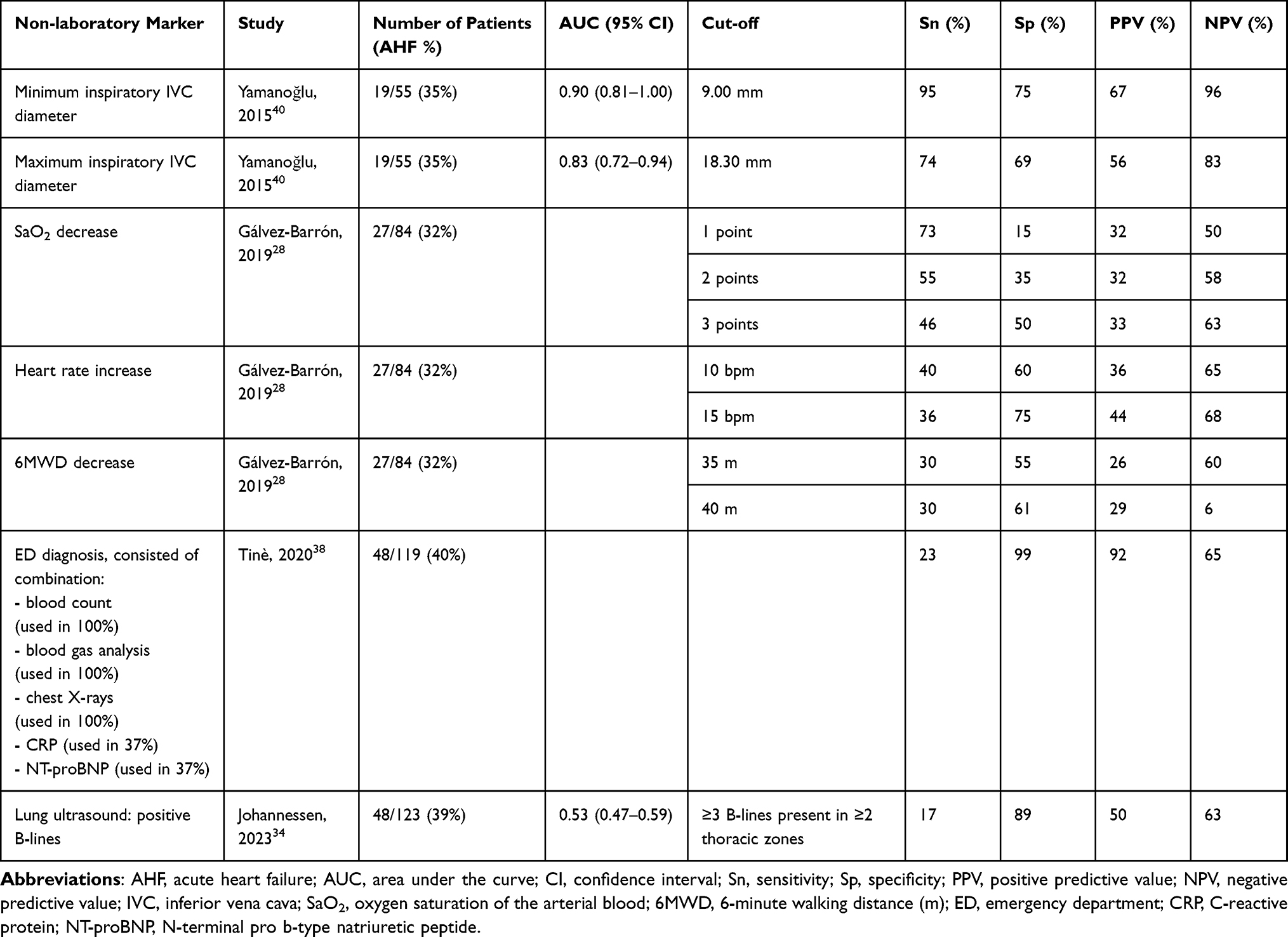 |
Table 3 Diagnostic Performances of Non-Laboratory Markers Detecting AHF in Acutely Dyspneic Patients with COPD in a Hospital Setting |
Discussion
This systematic review summarized the available evidence regarding markers investigated to diagnose AHF in acutely dyspneic patients with COPD, thereby differentiating between AHF and AECOPD or detecting AHF accompanying an AECOPD. In multiple studies, laboratory markers BNP and NT-proBNP were evaluated with modest to good discriminative ability in establishing AHF underlying acute dyspnea in COPD patients. Across the ten studies that were included, we observed a large variety in clinical settings, reference standards, markers, and cut-off values. The quality of the included studies was low, except for one. It is striking that so little, and low-quality, research has been conducted into such a well known, frequently occurring and important clinical problem.16
The fact that BNP and NT-proBNP were the only markers that showed discriminative ability in more than one study is in line with the view of experts and guidelines: heart failure guidelines dictate that NT-proBNP can rule in or out AHF in acutely dyspneic COPD patients following an initial assessment by electro- and echocardiography.12 This is in general described as a fairly good strategy to support the differential diagnosis in COPD patients presenting with acute dyspnea.2,42 Despite their evident discriminative ability, clinical use of BNP and NT-proBNP in COPD patients is still ambiguous because COPD-specific cut-off values are not sufficiently studied, hence cannot be presented in the COPD guidelines.2 To illustrate, two studies evaluated NT-proBNP in terms of sensitivity, specificity and predictive values, but used different cut-off values.27,39 Given that levels of BNP and NT-proBNP are already elevated in stable COPD patients,16,17 during an AECOPD,4,43 and in the elderly with COPD,4,27,43 it would be advisable to apply higher cut-off values for the differential diagnosis of acute dyspnea in these patients. Before the AHF diagnostic workflow can be specified for COPD patients, future research should define and validate an optimal cut-off value for BNP and NT-pro BNP with not only a high sensitivity, but also a high specificity.
Biomarkers MR-proANP, copeptin, ST2, and adiponectin had modest to good discriminative ability. However, these results were found in only one study with a small sample size.25,26 Because these markers are not yet validated in various high quality studies including large COPD populations, these are not ready for clinical use.44
We did not identify any vital signs or symptoms with a good discriminative ability in differentiating AHF from AECOPD in COPD patients. This seems to be in line with a systematic review that attempted to identify discriminative signs and symptoms.7 Although that review was not limited to COPD patients, it also did not find signs or symptoms with acceptable discriminative accuracy in a broad population of dyspneic patients.7 One study included in our review found minimum and maximum inspiratory capacity of the IVC as a good marker able to differentiate AHF from AECOPD in the ED.40 Especially, minimum IVC inspiratory capacity had a high sensitivity, a fairly good specificity, and a high NPV. The authors described the minimum inspiratory IVC diameter as the ideal marker to differentiate AHF from AECOPD.40 Given the increased use of handheld ultrasound devices in the ED,45 this marker could indeed have this potential. It is important to note, however, that this study had a high risk of bias due to concerns regarding the patient selection, interpretation of the index test, and patient flow. Furthermore, this marker was investigated in a limited sample size of 55 patients.40 Therefore, this marker needs validation in a large COPD population before it can be applied in clinical practice.
No firm advice can be provided on how to implement the use of certain (bio)markers into the acute disease management of CHF in patients with COPD, because our review found no markers that are able to diagnose AHF in acutely dyspneic COPD patients at an unambiguous cut-off value. NT-proBNP may have the potential to establish AHF in patients with COPD, but investigation of a specific cut-off value for this population is needed. Further research is still urgently needed before any COPD patient-specific marker can be incorporated into treatment decision-making algorithms, as CHF often remains undiagnosed in approximately 20.5% of COPD patients.46,47 Perhaps there is no single marker that can distinguish AHF in patients with AECOPD and the possibility of combining a marker with other markers, such as imaging, signs, symptoms and/or clinical characteristics, should be explored, as this approach may lead to improved diagnostic accuracy.48 This is also the approach that is currently used in clinical practice in varying strategies depending on the physician’s preference.
Our systematic review made clear that the methodological quality of studies, and consequently, the validity of the markers currently available, can be questioned due to methodological flaws or lack of transparent reporting of the chosen methodology of the included studies. There were unclarities and concerns mainly regarding the patient selection, use and interpretation of the index text (eg, the marker), and patient flow. The methodological approaches of future studies should, therefore, be streamlined by medical research authorities in the field to reach firm conclusions. A first suggestion would be to design a study following the STARD checklist,49 which meets the requirements of the QUADAS-2 tool, in order to report completely and transparently and hence achieve a low risk of bias assessment.23 Secondly, sub-analyses on COPD patients, for example as part of a study conducted in a broader ED study population, would help to define how to diagnose AHF early in COPD patients. Also stratification of disease severity groups (eg, GOLD or NYHA groups2,50) in diagnostic accuracy analyses might improve the understanding, and, consequently, personalized use of biomarkers. Clinical practice could profit from clear guidance regarding the differential diagnosis of acute dyspnea in COPD patients. But more importantly, it could mean much for our patients if we could draw meaningful and unambiguous conclusions about cardiac (bio)markers in COPD at some point.
Conclusion
This systematic review aimed to identify markers that can diagnose AHF underlying acute dyspnea in COPD patients in order to support physicians differentiating between AHF and AECOPD in patients with COPD presenting at the hospital. However, little evidence was found that supports implementation of (bio)marker use in clinical practice. Moreover, the overall risk of bias was high due to lacking methodological quality. BNPs are the most promising markers, but this review found no unambiguous cut-off value to be used in COPD patients, so (NT-pro)BNP values must still be interpreted alongside imaging and physical examination. Future studies should focus on validating the biomarkers in COPD patients specifically, and these should follow a sound methodology to reach high study quality and unbiased results.
Abbreviations
AECOPD, acute exacerbation of chronic obstructive pulmonary disease; AHF, acute heart failure, AI, artificial intelligence; AUC, area under the receiver operating characteristic curve; BNP, b-type natriuretic peptide; CHF, chronic heart failure; COPD, chronic obstructive pulmonary disease; ED, emergency department; IVC, inferior vena cava; MR-proANP, midregional pro-atrial natriuretic peptide; NT-proBNP, N-terminal pro b-type natriuretic peptide; NPV, negative predictive value.
Data Sharing Statement
The data files that provide insight into the AI-supported screening process and the choices made by the human reviewer are available from https://doi.org/10.5281/zenodo.10517334.
Acknowledgments
We would like to thank all authors of included studies who offered additional study information or data.
Funding
The research has been conducted as part of the RE-SAMPLE project, which has been supported by the European Union’s Horizon 2020 research and innovation program (grant number 965315).
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. The top 10 causes of death; 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death.
2. GOLD comittee. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2023 report); 2022.
3. Pellicori P, Cleland JGF, Clark AL. Chronic obstructive pulmonary disease and heart failure: a breathless conspiracy. Heart Fail Clin. 2020;16(1):33–44. doi:10.1016/j.hfc.2019.08.003
4. MacDonald MI, Shafuddin E, King PT, Chang CL, Bardin PG, Hancox RJ. Cardiac dysfunction during exacerbations of chronic obstructive pulmonary disease. Lancet Respir Med. 2016;4(2):138–148. doi:10.1016/S2213-2600(15)00509-3
5. Krahnke JS, Abraham WT, Adamson PB, et al. Heart failure and respiratory hospitalizations are reduced in patients with heart failure and chronic obstructive pulmonary disease with the use of an implantable pulmonary artery pressure monitoring device. Physiol Behav. 2016;176(1):139–148. doi:10.1016/j.cardfail.2014.12.008.Heart
6. van Dijk SHB, Brusse-Keizer MGJ, Effing T, et al. Exploring patterns of COPD exacerbations and comorbid flare-ups. Int J Chron Obstruct Pulmon Dis. 2023;18:2633–2644. doi:10.2147/COPD.S428960
7. Renier W, Hoogma-Von Winckelmann K, Verbakel JY, Aertgeerts B, Buntinx F. Signs and symptoms in adult patients with acute dyspnea: a systematic review and meta-analysis. Eur J Emerg Med. 2018;25(1):3–11. doi:10.1097/MEJ.0000000000000429
8. Hawkins NM, Virani S, Ceconi C. Heart failure and chronic obstructive pulmonary disease: the challenges facing physicians and health services. Eur Heart J. 2013;34(36):2795–2803. doi:10.1093/eurheartj/eht192
9. Hillas G, Perlikos F, Tsiligianni I, Tzanakis N. Managing comorbidities in COPD. Int J Chron Obstruct Pulmon Dis. 2015;10:95–109. doi:10.2147/COPD.S54473
10. Axson EL, Bottle A, Cowie MR, Quint JK. Relationship between heart failure and the risk of acute exacerbation of COPD. Thorax. 2021;76(8):807–814. doi:10.1136/thoraxjnl-2020-216390
11. Metra M, Teerlink JR. Heart failure. Lancet. 2017;390(10106):1981–1995. doi:10.1016/S0140-6736(17)31071-1
12. McDonagh TA, Metra M, Adamo M, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–3726. doi:10.1093/eurheartj/ehab368
13. Pantazopoulos I, Magounaki K, Kotsiou O, et al. Incorporating biomarkers in copd management: the research keeps going. J Pers Med. 2022;12(3):379. doi:10.3390/jpm12030379
14. Hoult G, Gillespie D, Wilkinson TMA, Thomas M, Francis NA. Biomarkers to guide the use of antibiotics for acute exacerbations of COPD (AECOPD): a systematic review and meta-analysis. BMC Pulm Med. 2022;22(1):1–16. doi:10.1186/s12890-022-01958-4
15. Aimo A, Vergaro G, Januzzi J, et al. Additive prognostic value of cardiac biomarkers in patients with chronic obstructive pulmonary disease and heart failure. Eur Heart J. 2021;42(Supplement_1):2021. doi:10.1093/eurheartj/ehab724.0987
16. Hawkins NM, Petrie MC, Jhund PS, Chalmers GW, Dunn FG, McMurray JJV. Heart failure and chronic obstructive pulmonary disease: diagnostic pitfalls and epidemiology. Eur J Heart Fail. 2009;11(2):130–139. doi:10.1093/eurjhf/hfn013
17. Su X, Lei T, Yu H. NT-proBNP in different patient groups of copd: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2023;18:811–825. doi:10.2147/COPD.S396663
18. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. J Clin Epidemiol. 2021;134:178–189. doi:10.1016/j.jclinepi.2021.03.001
19. Covidence systematic review software. Melbourne, Australia: Veritas Health Foundation.
20. McKeown S, Mir ZM. Considerations for conducting systematic reviews: evaluating the performance of different methods for de-duplicating references. Syst Rev. 2021;10(1):4–11. doi:10.1186/s13643-021-01583-y
21. van de Schoot R, de Bruin J, Schram R, et al. An open source machine learning framework for efficient and transparent systematic reviews. Nat Mach Intell. 2021;3(2):125–133. doi:10.1038/s42256-020-00287-7
22. van Dijk SHB, Brusse-Keizer MGJ, Bucsán CC, van der Palen J, Doggen CJM, Lenferink A. Artificial intelligence in systematic reviews: promising when appropriately used. BMJ Open. 2023;13:e072254. doi:10.1136/bmjopen-2023-072254
23. Reitsma JB. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155(4):529–536. doi:10.7326/0003-4819-155-8-201110180-00009
24. McHugh ML. Interrater reliability: the kappa statistic. Biochem Med. 2012;22(3):276–282. doi:10.11613/BM.2012.031
25. Dieplinger B, Gegenhuber A, Haltmayer M, Mueller T. Evaluation of novel biomarkers for the diagnosis of acute destabilised heart failure in patients with shortness of breath. Heart. 2009;95(18):1508–1513. doi:10.1136/hrt.2009.170696
26. Dieplinger B, Gegenhuber A, Kaar G, Poelz W, Haltmayer M, Mueller T. Prognostic value of established and novel biomarkers in patients with shortness of breath attending an emergency department. Clin Biochem. 2010;43(9):714–719. doi:10.1016/j.clinbiochem.2010.02.002
27. Fabbian F, De Giorgi A, Pala M, Tiseo R, Portaluppi F. Elevated NT-proBNP levels should be interpreted in elderly patients presenting with dyspnea. Eur J Intern Med. 2011;22(1):108–111. doi:10.1016/j.ejim.2010.07.013
28. Gálvez-Barrón C, Villar-álvarez F, Ribas J, et al. Effort oxygen saturation and effort heart rate to detect exacerbations of chronic obstructive pulmonary disease or congestive heart failure. J Clin Med. 2019;8(1):42. doi:10.3390/jcm8010042
29. Høiseth AD, Brynildsen J, Hagve TA, et al. The influence of heart failure co-morbidity on high-sensitivity troponin T levels in COPD exacerbation in a prospective cohort study: data from the Akershus cardiac examination (ACE) 2 study. Biomarkers. 2016;21(2):173–179. doi:10.3109/1354750X.2015.1126645
30. Winther JA, Brynildsen J, Høiseth AD, et al. Prevalence and prognostic significance of hyponatremia in patients with acute exacerbation of chronic obstructive pulmonary disease: data from the akershus cardiac examination (ACE) 2 study. PLoS One. 2016;11(8):1–14. doi:10.1371/journal.pone.0161232
31. Winther JA, Brynildsen J, Høiseth AD, et al. Prognostic and diagnostic significance of copeptin in acute exacerbation of chronic obstructive pulmonary disease and acute heart failure: data from the ACE 2 study. Respir Res. 2017;18(1):1–10. doi:10.1186/s12931-017-0665-z
32. Pervez MO, Lyngbakken MN, Myhre PL, et al. Mid-regional pro-adrenomedullin in patients with acute dyspnea: data from the Akershus Cardiac Examination (ACE) 2 Study. Clin Biochem. 2017;50(7–8):394–400. doi:10.1016/j.clinbiochem.2016.12.010
33. Pervez MO, Winther JA, Brynildsen J, et al. Prognostic and diagnostic significance of mid-regional pro-atrial natriuretic peptide in acute exacerbation of chronic obstructive pulmonary disease and acute heart failure: data from the ACE 2 Study. Biomarkers. 2018;23(7):654–663. doi:10.1080/1354750X.2018.1474258
34. Johannessen Ø, Uthaug Reite F, Bhatnagar R, Øvrebotten T, Einvik G, Myhre PL. Lung ultrasound to assess pulmonary congestion in patients with acute exacerbation of COPD. Int J Chron Obstruct Pulmon Dis. 2023;18(April):693–703. doi:10.2147/COPD.S396855
35. McCullough PA, Hollander JE, Nowak RM, et al. Uncovering heart failure in patients with a history of pulmonary disease: rationale for the early use of B-type natriuretic peptide in the emergency department. Acad Emerg Med. 2003;10(3):198–204. doi:10.1197/aemj.10.3.198
36. Maisel AS, Krishnaswamy P, Nowak RM, et al. Rapid measurement of b-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med. 2002;347(3):161–167. doi:10.1056/nejmoa020233
37. Moon JY, Bae JH, Kim TH, et al. The role of plasma B-type natriuretic peptide measurements in the differential diagnosis of acute dyspnea. Tuberc Respir Dis. 2005;59(6):656–663. doi:10.4046/trd.2005.59.6.656
38. Tinè M, Bazzan E, Semenzato U, et al. Heart failure is highly prevalent and difficult to diagnose in severe exacerbations of copd presenting to the emergency department. J Clin Med. 2020;9(8):1–12. doi:10.3390/jcm9082644
39. Tung RH, Camargo CA, Krauser D, et al. Amino-terminal pro-brain natriuretic peptide for the diagnosis of acute heart failure in patients with previous obstructive airway disease. Ann Emerg Med. 2006;48(1):66–74. doi:10.1016/j.annemergmed.2005.12.022
40. Yamanoğlu A, Çelebi Yamanoğlu NG, Parlak İ, et al. The role of inferior vena cava diameter in the differential diagnosis of dyspneic patients; best sonographic measurement method? Am J Emerg Med. 2015;33(3):396–401. doi:10.1016/j.ajem.2014.12.032
41. McCullough PA, Nowak RM, McCord J, et al. B-type natriuretic peptide and clinical judgment in emergency diagnosis of heart failure: analysis from Breathing Not Properly (BNP) multinational study. Circulation. 2002;106(4):416–422. doi:10.1161/01.CIR.0000025242.79963.4C
42. Pellicori P, Salekin D, Pan D, Clark AL. This patient is not breathing properly: is this COPD, heart failure, or neither? Expert Rev Cardiovasc Ther. 2017;15(5):389–396. doi:10.1080/14779072.2017.1317592
43. Nicolae B, Ecaterina L. Natriuretic peptides in elderly patients with chronic obstructive pulmonary disease. Egypt J Bronchol. 2022;16(1). doi:10.1186/s43168-022-00132-y
44. Sin DD, Vestbo J. Biomarkers in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2009;6(6):543–545. doi:10.1513/pats.200904-019DS
45. Malik AN, Rowland J, Haber BD, et al. The use of handheld ultrasound devices in emergency medicine. Curr Emerg Hosp Med Rep. 2021;9(3):73–81. doi:10.1007/s40138-021-00233-w
46. Wong CW, Tafuro J, Azam Z, et al. Misdiagnosis of heart failure: a systematic review of the literature. J Card Fail. 2021;27(9):925–933. doi:10.1016/j.cardfail.2021.05.014
47. Rutten FH, Cramer MJM, Grobbee DE, et al. Unrecognized heart failure in elderly patients with stable chronic obstructive pulmonary disease. Eur Heart J. 2005;26(18):1887–1894. doi:10.1093/eurheartj/ehi291
48. Liu C, Liu A, Halabi S. A min-max combination of biomarkers to improve diagnostic accuracy. Stat Med. 2011;30(161):2005–2014. doi:10.1002/sim.4238
49. Bossuyt PM, Reitsma JB, Bruns DE, et al. STARD 2015: an updated list of essential items for reporting diagnostic accuracy studies. BMJ. 2015;351:h5527.doi:10.1136/bmj.h5527
50. The Criteria Committee of the New York Heart Association; Nomenclature and Criteria for Diagnosis of Diseases of the Heart and Great Vessels. Little, Brown & Co; 1994.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.