")
Back to Journals » Advances in Medical Education and Practice » Volume 15
Knowledge, Attitude and Practice Toward Artificial Intelligence Among Healthcare Workers in Private Polyclinics in Jeddah, Saudi Arabia
Authors Serbaya SH , Khan AA , Surbaya SH, Alzahrani SM
Received 25 November 2023
Accepted for publication 27 March 2024
Published 5 April 2024 Volume 2024:15 Pages 269—280
DOI https://doi.org/10.2147/AMEP.S448422
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Suhail Hasan Serbaya,1,* Adeel Ahmed Khan,2,* Saud Hasan Surbaya,3,* Safar Majhood Alzahrani4,*
1Department of Industrial Engineering, Faculty of Engineering, King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia; 2Saudi Board Program of Preventive Medicine, Makkah Healthcare Cluster, Makkah, Kingdom of Saudi Arabia; 3Inter-Professional Training Director Administration, Makkah Healthcare Cluster, Makkah, Kingdom of Saudi Arabia; 4Inter-professional Training Administration, Makkah Healthcare Cluster, Makkah, Kingdom of Saudi Arabia
*These authors contributed equally to this work
Correspondence: Adeel Ahmed Khan, Saudi Board Program of Preventive Medicine, Makkah Healthcare Cluster, Makkah, Kingdom of Saudi Arabia, Tel +966-582265945, Fax +966-122366014, Email [email protected]
Purpose: The objective of our study was to assess awareness, attitudes, and practices regarding artificial intelligence (AI) among healthcare workers in private polyclinics in Jeddah, Saudi Arabia.
Methods: We conducted cross-sectional study among healthcare workers in private clinics in Jeddah. Data was collected using a structured, validated questionnaire in Arabic and English on awareness, attitudes, and behaviors regarding AI. Cronbach’s alpha for the questionnaire ranged from 0.6 to 0.8. Descriptive and bivariate analysis was done to assess the scores and their association of various sociodemographic variables with awareness, attitudes, and behaviors regarding AI. Multiple linear regression was performed to predict the scores of awareness, attitudes, and behaviors based on the sociodemographic variables.
Results: We recruited 361 participants for this study. Approximately, 62% of the healthcare workers were female. The majority (36%) of healthcare workers were nurses, while 25% were physicians. The median awareness, attitude, and behavioral scores were 5/6 (IQR 3– 6), 5/8 (IQR 4– 7), and 0/3 (IQR 0), respectively. Approximately three-fourths (74%) of the healthcare workers believed that they understood the basic computational principles of AI. Only half of the participants were willing to use AI when making future medical decisions. We found that male healthcare workers had better knowledge scores regarding AI as compared to female healthcare workers (Beta = 0.555, 95%, p value = 0.010), while for attitude scores, being administrative employee as compared to other employees was found to have negative attitude towards AI (Beta = 0.049, 95%, p value = 0.03).
Conclusion: We found that healthcare workers had an overall good awareness and optimistic attitude toward AI. Despite this, the majority is worried about the potential consequences of replacing their jobs with AI in the future. There is a dire need to educate and sensitize healthcare workers regarding the potential impact of AI on healthcare.
Keywords: artificial intelligence, awareness, attitude, practice, healthcare workers, Saudi Arabia
Introduction
In recent times, the healthcare system in many countries has started to use the data of the patients for the quality of care improvement. In this era of technological advancements, there are many developments that have the capacity to use hospital care data for the best interest of the patients. This will eventually result in more efficient services, and it will improve the outcomes as well.1,2 Nowadays, artificial intelligence (AI) has been used as an important tool for technological advancement in healthcare system.3
AI technologies are now helping and shaping the healthcare system for achieving their goals related to patient care.4 There is also a debate about how to transform human intellectual into AI. Looking from healthcare viewpoint, AI brings a “paradigm shift to healthcare, powered by increasing availability of healthcare data and rapid progress of analytics techniques”.5 Another review suggested that with the support of artificial intelligence, dental nurses play a key role in dental cone beam computed tomography (CBCT) data management during the consultation. It helps the consultants by preparing patients for imaging, and it assists the dentist with image interpretation and data analysis and preparation.6
There have been studies done globally that have assessed the role and use of AI in healthcare system to improve the outcome associated with medical decision-making and efficiency.7,8 There have been many promising improvements in the functioning of the healthcare systems, and it has been supported by accessibility of large medical datasets to assess the algorithms.9 The use of AI will eventually be implemented in healthcare system, as the physicians will be the foremost beneficiary of this technology as this will help them to take informed decision about their patient diagnosis and treatment plans.
Current evidence suggests that use of AI in healthcare system is increasing, and as a result, there is a need that healthcare workers should know about the concepts and fundamentals of AI. In United Kingdom (UK), there has been use of innovative digital technologies in healthcare system which has resulted in recent national governmental review.10 The behaviors of healthcare workers related to the use of AI is showing enthusiasm, and this is helping for the authorities to implement it smoothly. There have been previous experiences reported from Canada11 and Germany12 as well, where studies have been conducted about readiness of incorporating AI in healthcare personnel among medical students.
Sarwar et al13 reported findings from 54 countries; that is, positive attitudes have been reported among respondents about AI, with around 75% of the participants reported to be highly motivated for using AI as diagnostic tool for improving the patient outcomes related to pathology work. Maskara et al14 investigated the acceptance of AI among different clinical specialties and showed that they knew about AI technology use in their field, and few of their colleagues were using AI themselves; however, the physicians were positive about AI, but also they were spectacle that using AI would have an impact on cost and also empathy factor related to patient counselling. Another study15 found that physicians were very positive about AI implementation in healthcare system.
Most of the studies conducted on this topic assessed the respondent’s perception about AI implementation in their fields, they did not consider respondents’ knowledge, attitudes, and behaviors related to AI. There is very limited literature on this topic in the Saudi Arabian context, despite the technological advancement this region is seeing. Only a handful number of studies have assessed respondents’ knowledge and awareness about artificial intelligence in Saudi Arabia. The purpose of our study is to understand Saudi Arabian healthcare workers’ knowledge, attitudes, and practices related to AI and explore the factors that influence them. Hence, the objective of our study was to determine the level of AI knowledge, attitudes, and practices among healthcare workers working in private polyclinics in Jeddah, Saudi Arabia. We also evaluated the association of knowledge, attitudes, and practices regarding AI with other sociodemographic variables among the same population in Jeddah, Saudi Arabia.
Materials and Methods
Study Design and Setting
This cross-sectional study was conducted in Jeddah, Saudi Arabia, from March 2022 to May 2022. Jeddah, the coastal city of Saudi Arabia, is at the eastern coast of the Red Sea. Jeddah is considered as the economic and tourism capital of the country. The population is estimated to be approximately 3.4 million.16 The study population for this research were healthcare workers in private polyclinics in Jeddah. They included physicians, nurses, administrative personnel, and other staff members. A total of 22 private polyclinics in Jeddah were recognized at the time of our study. They operate under the supervision of the Jeddah Directorate for Health Affairs. These polyclinics encompass around 7798 healthcare workers belonging to all health specialties according to the Ministry of Health Statistical Yearbook (2020). Therefore, a study population was formed. Based on their geographical distribution, the polyclinics were divided into four sectors. We selected one of these sectors by simple randomization to include all healthcare workers in the polyclinics in our study.
Sample Size
We calculated the sample size by using the Statulator Inc. Calculator. With a population of 8000 healthcare workers and assuming the expected population standard deviation to be 0.517 for the mean scores of knowledge, favorable attitudes and practices, the study required a sample size of 388 participants to estimate a mean a 95% confidence interval and 5% margin of error.
Sampling Technique
After recruitment of all private polyclinics in the sector, staff members were identified. Healthcare workers were recruited from private clinics. Convenience sampling was used to enroll polyclinics in the selected sector until the number of healthcare workers from these private polyclinics reached the sample size. Employees or healthcare workers under training and those on leave during the study period were excluded.
Study Tools
We collected the data by using structured questionnaires in both Arabic and English languages. The questionnaire consisted of four sections. The first section concerned socio-demographics including age, gender, type of healthcare worker, professional qualifications, and years of work experience. The second, third, and fourth sections included variables on awareness (6 items), attitude (8 items), and behaviors (3 items) regarding AI. The awareness, attitude and behavior questionnaire were developed after reviewing the relevant literature that focused on assessing the knowledge, attitude and practice regarding AI. This task was performed by two independent investigators, and discrepancies were resolved through discussion. The questionnaire was checked and validated by university faculty members. The questionnaire was translated into Arabic by a bilingual expert. Next, the translated versions were back-translated into English by another set of bilingual experts to assess the accuracy of the translation. A pilot study was conducted on 10% of the target population. Content validity was reviewed by subject experts and expert physicians. A reliability analysis of the questionnaire was performed. Cronbach’s alpha value of awareness, attitude and behavior domains were 0.79, 0.77 and 0.62, respectively.
The second section (awareness of AI) included six items: “Do you have good familiarity with artificial intelligence?”; “I have an understanding of the basic computational principle of AI”; “I am comfortable with the nomenclature of AI”; “I have an understanding of the limitations of AI”; “AI abilities are superior to human experience”; and “AI has useful applications in the medical field”. The third section (attitudes regarding AI) includes eight items: “How useful do you think AI could be in your area of work?”; “The diagnostic ability of AI is superior to the clinical experience of a human doctor”; “AI can help reduce the number of medical errors”; “AI can deliver clinically relevant, vast amounts of high-quality data in real time”; “AI has no emotional exhaustion or physical limitation”; “Do you agree that you would always use AI when making medical decisions in the future?”; “Do you think there may be serious privacy issues with the use of AI?”; and “How worried are you that AI will replace you in your job?” The final section (behavior of AI) included three items: “AI cannot be used to provide opinions in unexpected situations”; “AI is not flexible enough to be applied to every patient”; and “AI has low ability to sympathize and consider the emotional well-being of the patient” (Supplementary File 1).
Data Collection Technique
After obtaining proper approval, the questionnaires were manually distributed to the participants. All questionnaires were stored in a private memory and only involved, and the authors would have the right to review them. If the criteria met the study inclusion criteria, a full explanation of the study objectives was communicated to them, and written informed consent was also obtained from willing participants.
Data Analysis
Data were statistically analyzed using SPSS software version 25. Descriptive analyses were performed by calculating the mean ± SD for quantitative data, such as age and experience in years; variables, frequency, and proportion of qualitative data were also computed, such as sex, type of healthcare worker, and professional qualification. Median and interquartile range (IQR) were reported for awareness, attitude and practice scores, as these variables were not normally distributed. For questions related to awareness, a score of “1” was assigned if the answer was strongly agree and agree, while “0” was assigned if the answer was strongly disagree, disagree and do not know. All six items were then summed up to calculate the total awareness score. Scores for each of the items in the attitude section range from “0” strongly disagree, disagree and do not know to “1” for strongly agree and agree. The sum of all items in the attitude section was used to calculate the total score. In the behavior domain, “0” was assigned for poor behavior and “1” was assigned to good behavior. Subsequently, the total behavior score was calculated by summing all items. For bivariate comparisons of awareness, attitudes, and behaviors, we used Mann–Whitney and Kruskal–Wallis tests. Multiple linear regression was performed to predict the scores of awareness, attitudes, and behaviors based on the sociodemographic variables. Results of the regression were presented as beta coefficients and p-values. A p-value of <0.05 was considered significant at a confidence interval of 95%.
Ethical Considerations
Our study was approved by the Research Ethics Committee of the Research and Studies Department of Jeddah Health Affairs (Research No. 1547, dated 2/9/2021). No personal identifiers such as names or phone numbers were collected. We ensured that no personal information was collected during the data collection, and access to data was only authorized to the primary investigator. All information was kept confidential.
Results
We recruited 361 individuals participated for our study. The response rate was 98.3%. The mean age of the participants was 35.2 ± 9.9 years. Approximately 43% (n = 155) of the healthcare workers were 30 years of age or younger, whereas approximately 42% (n = 152) were between 31 and 45 years of age. Approximately 62% of the healthcare workers were females. The majority (36%) of healthcare workers were nurses, while 25% were physicians. Half (51%) of them were graduates, followed by diploma holders (21%). Most participants (43%) had 6–15 years of experience, followed by up to five years of experience (41%) (Table 1).
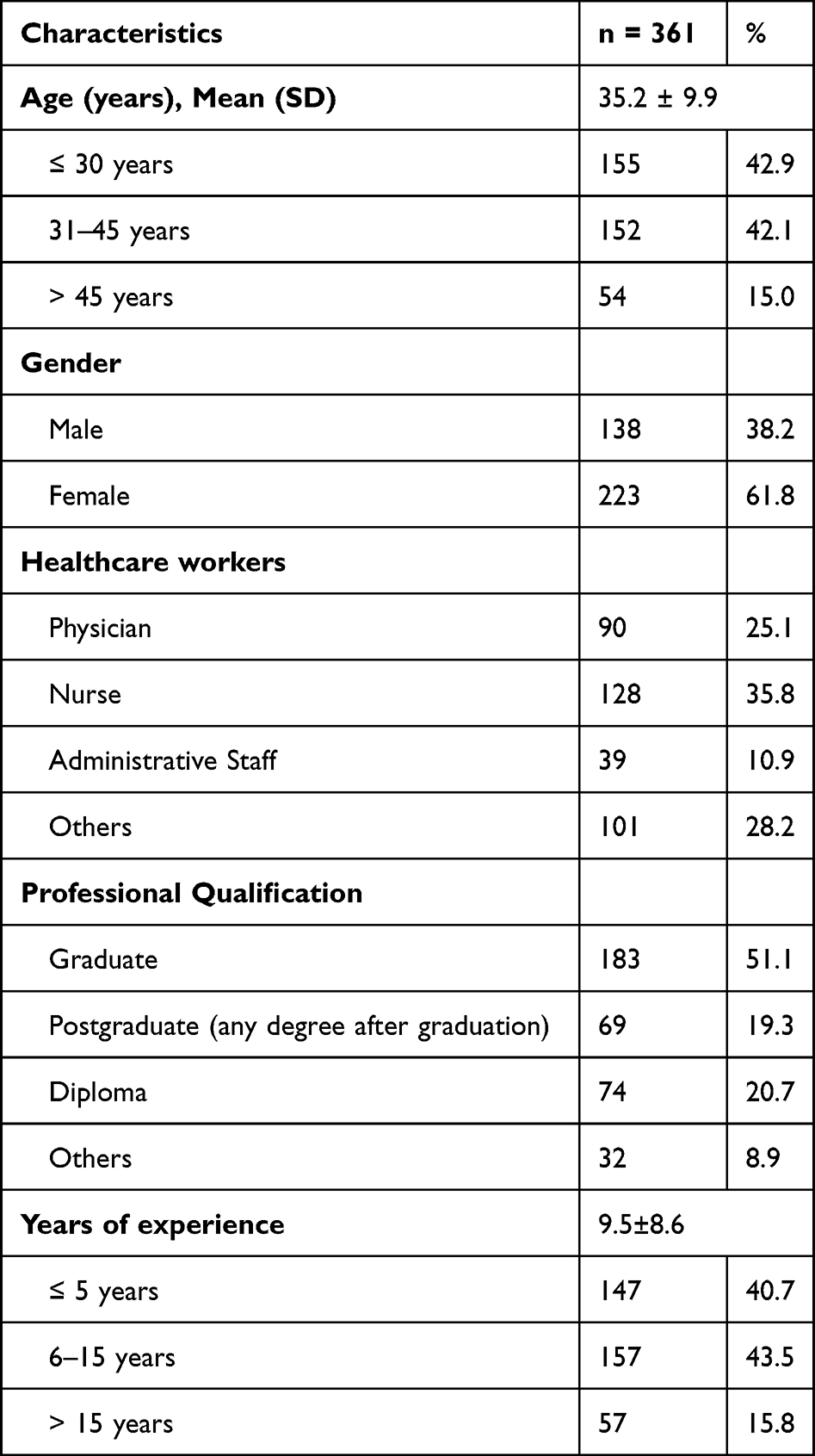 |
Table 1 Socio-Demographic Characteristics of Healthcare Workers Working in Private Polyclinics in Jeddah (n = 361) |
Table 2 presents the results of the knowledge, attitudes, and practices toward AI among healthcare workers in Jeddah. The median awareness score of participants was 5 (IQR 3–6) where the maximum possible score was 6. The median score for the attitude domain was 5 (IQR 4–7) from a possible 8. The median behavioral score was 0 (IQR 0) from a total of 3.
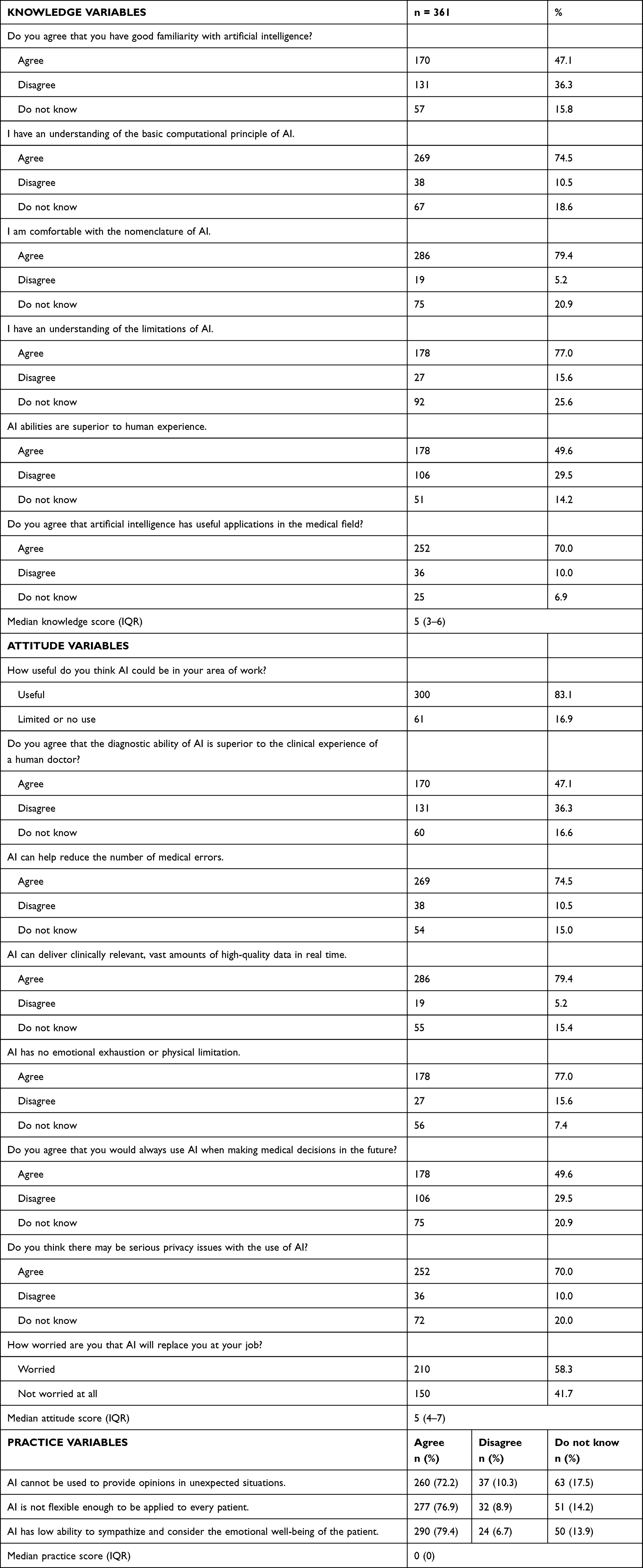 |
Table 2 Knowledge, Attitude, and Practices Toward Artificial Intelligence (AI) Among Healthcare Workers in Jeddah (n = 361) |
Approximately half (47%) of the participants agreed that they were familiar with AI. Approximately three-fourths (74%) of the healthcare workers thought that they understood the basic computational principles of AI. Half (50%) of the respondents believed that AI abilities were superior to human experience. Approximately, two-thirds (70%) of participants agreed that AI has useful applications in the medical field. Approximately 83% of participants thought that AI could be useful in their area of work. Only 47% believed that the diagnostic ability of AI was superior to that of a human doctor. Approximately three-fourths (75%) of healthcare workers agreed that AI could help reduce the number of medical errors. The majority of participants (79%) reported that AI could deliver clinically relevant, vast amounts of high-quality data in real time. Half (50%) of the participants agreed that they would use AI to make medical decisions in the future. Approximately, 70% of respondents believed that there may be serious privacy issues associated with the use of AI. Approximately 58% of healthcare workers were worried that AI would replace their jobs. The majority of participants (79%) responded that AI has a low ability to sympathize with and consider the emotional well-being of the patient.
Figure 1 shows the concerns of healthcare workers regarding the application of AI in medicine. Approximately 25% believed that AI is not flexible enough to be applied to every patient, while one-fourth responded that AI has a poor ability to consider the emotional well-being of the patient. Figure 2 presents the different domains in which participants thought that the use of AI would be useful. Approximately one-fourth of participants thought that AI would be useful in providing medical assistance in underserved areas, whereas 23% believed that it would be more useful in biopharmaceutical research.
 |
Figure 1 Participant’s concerns about application of AI in medicine (n=361). |
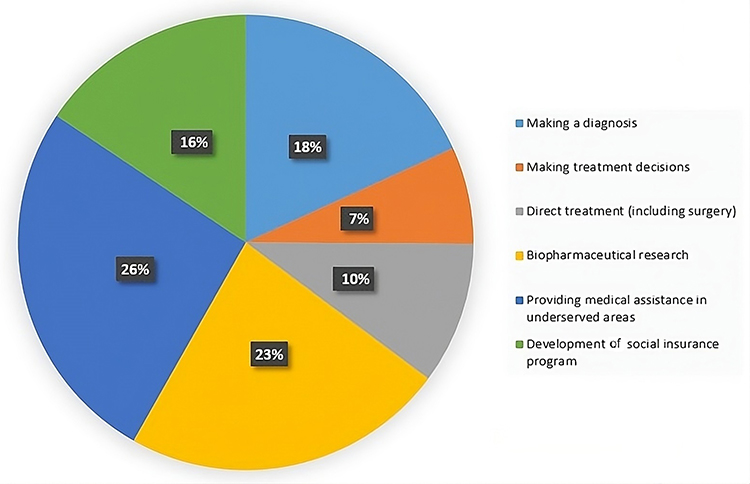 |
Figure 2 Participant’s think use of Artificial Intelligence would be most useful in. |
Table 3 shows the bivariate association of AI knowledge, attitude, and practice scores with other sociodemographic variables among healthcare workers in Jeddah. We found that nurses had the highest knowledge scores compared to other types of healthcare workers (p = 0.032), and administrative staff had the highest practice scores compared to other healthcare workers (p = 0.031). No significant differences were observed among gender, age, and years of experience with respect to knowledge, attitude, and practice scores related to AI.
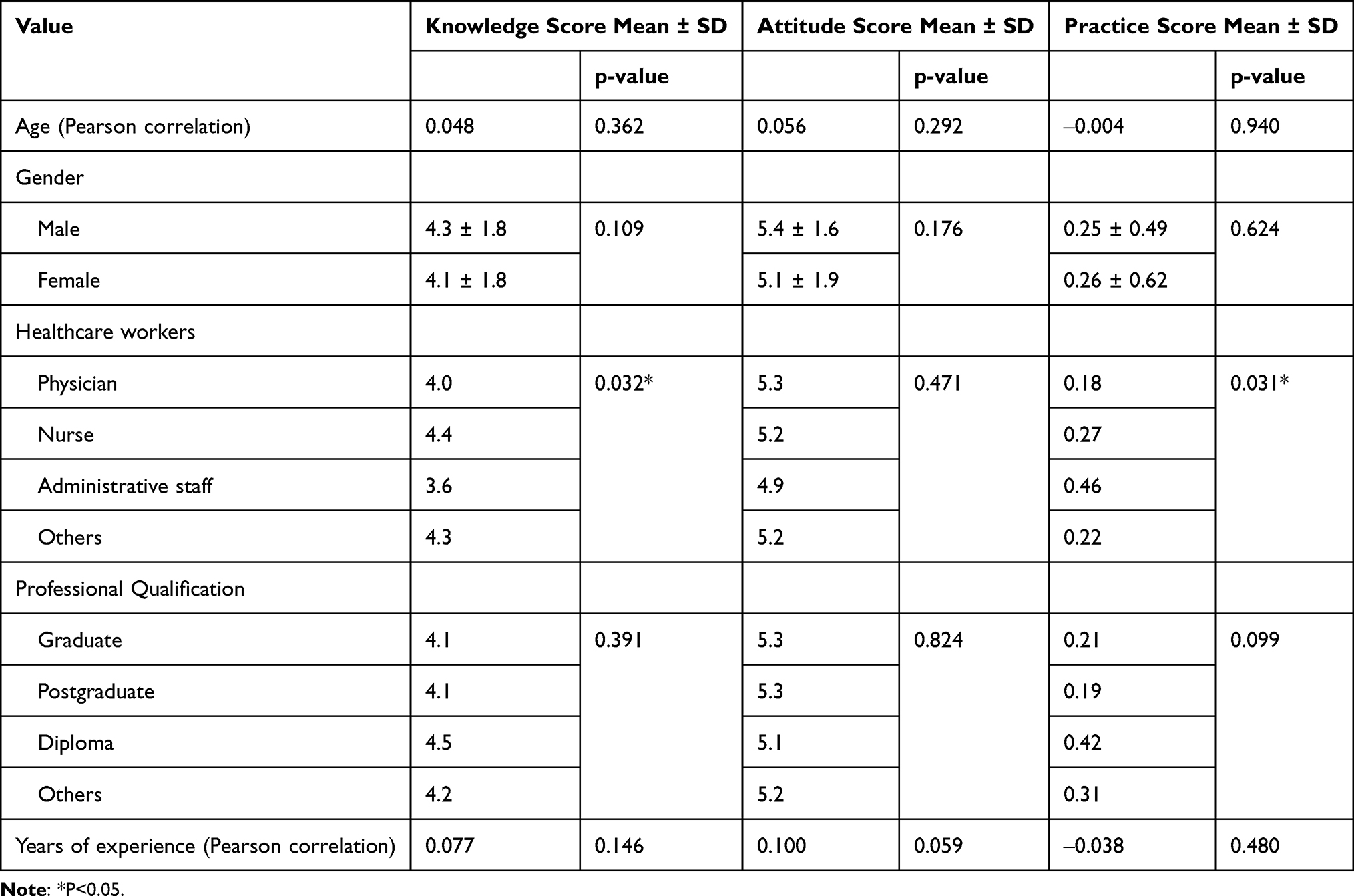 |
Table 3 Bivariate Association of Knowledge, Attitude, and Practice Scores of Artificial Intelligence (AI) with Other Variables Among Healthcare Workers in Jeddah (n = 361) |
In Table 4, the multiple linear regression shows the predictors of knowledge, attitude, and practice scores of Artificial Intelligence (AI) with other socio-demographic variables among healthcare workers in Jeddah. We found that male healthcare workers had better knowledge scores regarding AI as compared to female healthcare workers (Beta = 0.555, 95%, p value = 0.010). While for attitude scores, being administrative employee as compared to other employees was found to have negative attitude towards AI (Beta = −0.923, 95%, p value = 0.037). Additionally, more experience years were found to possess positive attitude towards AI (Beta = 0.049, 95%, p value = 0.03). Rest of the variables were found to be insignificant for knowledge, attitude and practice scores.
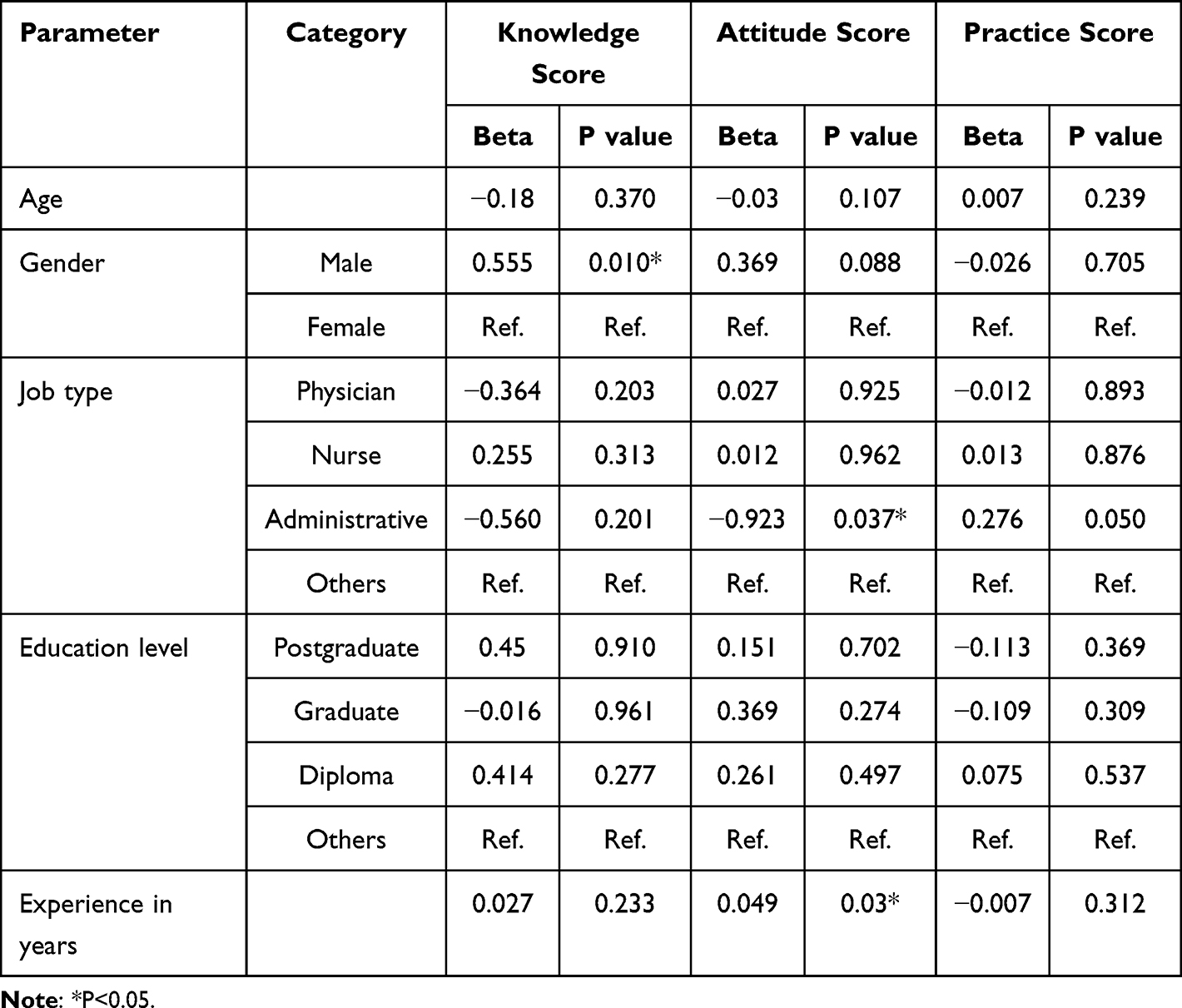 |
Table 4 Linear Regression Showing the Relation Between Knowledge, Attitude, and Practice Scores of Artificial Intelligence (AI) with Other Socio-Demographic Variables Among Healthcare Workers in Jeddah (n = 361) |
Discussion
This is one of the very few epidemiological studies conducted in Saudi Arabia on awareness, attitude, and practice regarding AI among healthcare workers. Compared with the government sector, the private sector had less direct supervision and operation from the Ministry of Health in terms of computerized systems and technical issues. Therefore, this was the main focus of our study.
Overall, we found good awareness and optimistic attitudes toward AI among healthcare workers in Jeddah, Saudi Arabia. Despite having a positive awareness and attitude, the majority were worried about the potential consequences of AI replacing their jobs. This finding was similar to the previous study conducted in Saudi Arabia, which also reported that around 78% of the healthcare workers were of the opinion that their job was at risk to be replaced after application of AI in their work setting.17 Another study among community pharmacist in Saudi Arabia reported contrasting findings that only 25.6% believed that AI would eventually replace healthcare individuals.18 There is another contrasting finding from a Korean study15 conducted among physicians, which reported that only 35% reported that their job could be replaced by AI. Another study from UK among healthcare workers reported that only 28% were worried that AI would replace their jobs.19 This difference may be due to difference in advancement and application of AI in healthcare systems, as, in Saudi Arabia, the transformation has only recently been introduced, while in western and developed countries like Korea, AI has been used for a few years and the healthcare workers are aware of the advantages related to the potential impact of AI in their healthcare system.
We also enquired about healthcare workers’ understanding of AI principles. Around half of the healthcare workers believed that they had good familiarity with AI in our survey, while around three-fourths replied that they understood the basic computational principles of AI. This has also been reported in other studies as well.20–22 Fifty percent of our participants also believed that AI abilities were superior to human experience. Approximately 70% of participants agreed that AI has useful applications in the medical field.
In the attitude section, most healthcare workers believed in the usefulness of AI in their area of work. This finding is also consistent with those of previous studies.21,23 We also enquired about the diagnostic ability of AI compared with the clinical experience of a human doctor; approximately half of the participants agreed that AI would be clinically superior. This has been supported by previous studies that reported that, in radiology and pathology, AI will replace doctors based on diagnostic superiority.24,25 Krittanawong26 believed that AI cannot replace doctors, as the patient–doctor relationship cannot be completed without the sympathy and empathy that AI has not been able to achieve. In complex situations, physicians’ experience is still needed to integrate history, examination, and laboratory tests to arrive at a final plan for the patient.26 The majority of our participants also believed that AI can help in reducing medical errors and deliver clinically relevant, high-quality data in real time. This has been supported by the findings of previous studies that have also reported similar results.20,27 In a study conducted in Pakistan among physicians and medical students, 74.4% of our study population acknowledged the importance of AI in modern diagnostics.20 It was also reported in the same study that 66.6% of participants agreed that implementation of AI in medicine will reduce diagnostic errors.20 We also asked about the emotional exhaustion of AI, for which the majority of participants reported that AI has no emotional exhaustion. Only half of them believed that they would use AI when making medical decisions in the future.
Regarding the practical aspect of using AI in their practice, our healthcare workers were not convinced that AI could provide opinions in difficult situations. Moreover, the majority thought that AI is not sufficiently flexible to be applied to every patient. The majority also thought that AI had a poor ability to sympathize with patients and is less considerate about the emotional well-being of the patient. These findings are consistent with previous studies that reported that healthcare workers, including physicians and medical students, were unaware of the practical utilization of AI in the medical field.15,17 Surovková et al also explored the impact of AI on the role of dental supporting staff in orthodontic practices, highlighting the transformative effects of AI-powered workflows and the emergence of new responsibilities for these professionals. Their study, conducted over a three-year period, assessed the implementation of an AI solution called Dental Monitoring in an orthodontic practice, and it was found that AI can enhance patient care and personalized treatment while also raising ethical and legal considerations for dental practices.28
We also found that male healthcare workers had better knowledge than female healthcare workers. This finding is similar to other studies, which also reported that males had better knowledge than other females.29 We also reported that administrative employees were having negative attitude towards AI as compared to other employees. This needs to be further explored, as for meaningful comparison, a larger sample size and appropriate number of each type of healthcare workers according to their specialty would be required.
During recent times, the use of AI in Saudi Arabia has increased dramatically with 2030 vision in Saudi Arabia. Saudi Arabia has launched several platforms for its national digitalization mission. The National Healthcare Command and Control Center [NHCCC] and Saudi Data and Artificial Intelligence Authority (SDAIA) have led this initiative to integrate AI into the healthcare system.19 During COVID-19, the development of mobile apps and their sensitization to the local population was the cornerstone of preventive efforts against the COVID-19 pandemic in Saudi Arabia.30
This is one of the very few studies that has assessed awareness, attitudes, and practices regarding AI among healthcare workers in Saudi Arabia. We only enrolled healthcare workers from private polyclinics, so the generalizability would be limited. However, we believe that the responses from the public sector would, to some extent, not have been much different. Second, we were not able to collect information from our Information Technicians (ITs), which would be interesting to compare with the awareness and attitude regarding AI because they, for sure, would have more exposure to AI.
Conclusion
In summary, our results showed that healthcare workers working in Jeddah, Saudi Arabia, showed good overall awareness and optimistic attitudes toward AI. Despite having a positive awareness and attitude, the majority were worried about the potential consequences of AI replacing their jobs in the future. There is a dire need to educate and sensitize healthcare workers about the impact of AI in healthcare system. We found that our results were mixed between fear of job replacement by AI and good overall awareness about AI technologies and advancements. The findings of our study highlighted the need for sensitizing healthcare workers on the pros, cons, and challenges associated with the implementation of AI in healthcare and the potential of these evolving technologies to improve healthcare outcomes. Different institutions like college and universities can play the pivotal role in making the environment conductive for accepting the role of AI in improving the health services. Moreover, the current market dynamics and situation of healthcare system in Saudi Arabia also makes it a perfect case for developing and implementing the use of AI by AI solution developers.
Regarding strengths, we think that this study adds to the existing knowledge and perceptions about AI among healthcare workers in Saudi Arabia. It emphasizes the need for determined efforts to address the gaps in AI together with healthcare individuals and preparing for coupling the potential of AI to improve outcome related with patient care and advancements in the medical. Regarding limitations, our study design does not allow for the assessment of awareness and optimistic attitudes toward AI over time. For studying this over a period of time, longitudinal studies could be conducted in future. The study sample was restricted to healthcare workers working in private polyclinics in Jeddah, limiting the applicability of our results to other population. Future studies should be planned to gain insights from different sub-group of population, and different contexts to have a better understanding of the application of AI in healthcare settings. We used self-reported measures of awareness and attitudes towards AI, which may be subject to biases, such as social desirability bias. Follow-up studies could utilize the impartial metrics to evaluate the proficiency of learners in the AI domain, such as pre- and post-evaluations based on performance. Our study does not address the potential for AI to exacerbate existing health inequities. Future studies are recommended AI to address this important point, which could lead to discrimination against certain groups of people. The study also does not collect data on the healthcare workers’ prior exposure to AI or their experience with AI-powered tools. This could bias the results, as individuals who are already familiar with AI may have more positive attitudes towards it.
Lastly, it would be beneficial to assess the perceptions and opinions of healthcare administrators, executives and other relevant stakeholders in establishing and implementing AI technologies in healthcare system. The knowledge about the potential barriers in implementing AI technologies in healthcare system could be used to find answers and solutions to increase AI literacy among healthcare individuals.
In conclusion, our study emphasized on the positive attitude of Saudi Arabian healthcare workers towards AI awareness and its utilization. By working on the gaps found in AI awareness and understanding of AI’s potential and limitations in healthcare system, our system can plan for our future health professionals, to couple the utilization of AI in improving patient care and healthcare system betterment.
Acknowledgments
The authors would like to thank all the healthcare workers who gave their precious time to us for participating in the study.
Disclosure
The authors report that there is no conflict of interest.
References
1. Lovis C. Unlocking the power of artificial intelligence and big data in medicine. J Med Internet Res. 2019;21(11):e16607. doi:10.2196/16607
2. van Hartskamp M, Consoli S, Verhaegh W, et al. Artificial intelligence in clinical health care applications: viewpoint. Interact J Med Res. 2019;8(2):e12100. doi:10.2196/12100
3. Yu K, Beam AL, Kohane IS. Artificial intelligence in healthcare. Nat Biomed Eng. 2018;2(10):719–731. doi:10.1038/s41551-018-0305-z
4. Wu H, Chan N, Zhang CJP, et al. The role of the sharing economy and artificial intelligence in health care: opportunities and challenges. J Med Internet Res. 2019;21(10):e13469. doi:10.2196/13469
5. Jiang F, Jiang Y, Zhi H, et al. Artificial intelligence in healthcare: past, present and future. Stroke Vasc Neurol. 2017;2(4):230–243. doi:10.1136/svn-2017-000101
6. Urban R, Haluzová S, Strunga M, et al. AI-assisted CBCT data management in modern dental practice: benefits, limitations and innovations. Electronics. 2023;12(7):1710. doi:10.3390/electronics12071710
7. Rajkomar A, Dean J, Kohane I. Machine Learning in Medicine. N Engl J Med. 2019;380(14):1347–1358. doi:10.1056/NEJMra1814259
8. Topol EJ. High-performance medicine: the convergence of human and artificial intelligence. Nat Med. 2019;25(1):44–56. doi:10.1038/s41591-018-0300-7
9. Oakden-Rayner L. Exploring large-scale public medical image datasets. Acad Radiol. 2020;27(1):106–112. doi:10.1016/j.acra.2019.10.006
10. Department of Health and Social Care. The Topol review: preparing the healthcare workforce to deliver the digital future, 2019. Her Majesties Government, United Kingdom; 2019. Available from: https://topol.hee.nhs.uk/wp-content/uploads/HEE-Topol-Review-2019.pdf.
11. Gong B, Nugent JP, Guest W, et al. Influence of artificial intelligence on Canadian medical students’ preference for radiology specialty: a national survey study. Acad Radiol. 2019;26:566–577. doi:10.1016/j.acra.2018.10.007
12. Dos Santos D P, Giese D, Brodehl S, et al. Medical students’ attitude towards artificial intelligence: a multicentre survey. Eur Radiol. 2019;29:1640–1646. doi:10.1007/s00330-018-5601-1
13. Sarwar S, Dent A, Faust K, et al. Physician perspectives on integration of artificial intelligence into diagnostic pathology. NPJ Digit Med. 2019;2:28. doi:10.1038/s41746-019-0106-0
14. Maskara R, Bhootra V, Thakkar D, et al. A study on the perception of medical professionals towards artificial intelligence. Int J Multidiscip Res Dev. 2017;4(4):34–39.
15. Oh S, Kim JH, Choi S, et al. Physician confidence in artificial intelligence: an online mobile survey. J Med Internet Res. 2019;21(3):e12422. doi:10.2196/12422
16. Jeddah Municipality. About Jeddah City; 2022. Available from: https://www.jeddah.gov.sa/english/jeddahcity/about/index.php.
17. Abdullah R, Fakieh B. Health care employees’ perceptions of the use of artificial intelligence applications: survey study. J Med Internet Res. 2020;22(5):e17620. doi:10.2196/17620
18. Syed W, Al-Rawi MBA. Community pharmacists awareness, perceptions, and opinions of artificial intelligence: a cross-sectional study in Riyadh, Saudi Arabia. Technol Health Care. 2024;32(1):481–493. doi:10.3233/THC-230784
19. Castagno S, Khalifa M. Perceptions of artificial intelligence among healthcare staff: a qualitative survey study. Front Artif Intell. 2020;3:578983. doi:10.3389/frai.2020.578983
20. Ahmed Z, Bhinder KK, Tariq A, et al. Knowledge, attitude, and practice of artificial intelligence among doctors and medical students in Pakistan: a cross-sectional online survey. Ann Med Surg Lond. 2022;76:103493. doi:10.1016/j.amsu.2022.103493
21. Syed W, Basil A, Al-Rawi M. Assessment of awareness, perceptions, and opinions towards artificial intelligence among healthcare students in Riyadh, Saudi Arabia. Medicina. 2023;59(5):828. doi:10.3390/medicina59050828
22. Alghamdi SA, Alashban Y. Medical science students’ attitudes and perceptions of artificial intelligence in healthcare: a national study conducted in Saudi Arabia. J Radiat Res Appl Sci. 2024;17(1):100815. doi:10.1016/j.jrras.2023.100815
23. Laï MC, Brian M, Mamzer MF. Perceptions of artificial intelligence in healthcare: findings from a qualitative survey study among actors in France. J Transl Med. 2020;18(1):14. doi:10.1186/s12967-019-02204-y
24. Dreyer KJ, Geis JR. When machines think: radiology’s next frontier. Radiology. 2017;285(3):713–718. doi:10.1148/radiol.2017171183
25. Diprose W, Buist N. Artificial intelligence in medicine: humans need not apply? N Z Med J. 2016;129(1434):73–76.
26. Krittanawong C. The rise of artificial intelligence and the uncertain future for physicians. Eur J Intern Med. 2018;48:e13–e14. doi:10.1016/j.ejim.2017.06.017
27. Sit C, Srinivasan R, Amlani A, et al. Attitudes and perceptions of UK medical students towards artificial intelligence and radiology: a multicentre survey. Insights Imaging. 2020;11(1):14. doi:10.1186/s13244-019-0830-7
28. Surovková J, Haluzová S, Strunga M, et al. The new role of the dental assistant and nurse in the age of advanced artificial intelligence in telehealth orthodontic care with dental monitoring: preliminary report. Appl Sci. 2023;13(8):5212. doi:10.3390/app13085212
29. Al Hadithy ZA, Al Lawati A, Al-Zadjali R, et al. Knowledge, attitudes, and perceptions of artificial intelligence in healthcare among medical students at sultan Qaboos university. Cureus. 2023;15(9):e44887. doi:10.7759/cureus.44887
30. Aljizawi J, Dalloul D, Ghryani L, et al. A survey of artificial intelligence solutions in response to the COVID-19 pandemic in Saudi Arabia. Procedia Comput Sci. 2021;194:190–201. doi:10.1016/j.procs.2021.10.073
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.