")
Back to Journals » Nature and Science of Sleep » Volume 16
Investigating the Causal Relationship Between Sleep Behaviors and Primary Open-Angle Glaucoma: A Bidirectional Two-Sample Mendelian Randomization Study
Authors Zhang J , Chen X, Zhu Y, Wan S, Hu S, Yang Y
Received 8 September 2023
Accepted for publication 8 February 2024
Published 15 February 2024 Volume 2024:16 Pages 143—153
DOI https://doi.org/10.2147/NSS.S439274
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Jun Zhang,1,* Xiaoyan Chen,2,* Yan Zhu,1,* Shanshan Wan,1 Shuqiong Hu,3 Yanning Yang1
1Department of Ophthalmology, Renmin Hospital of Wuhan University, Wuhan, Hubei, People’s Republic of China; 2Department of Obstetrics and Gynecology, Women and Children’s Hospital of Chongqing Medical University, Chongqing Health Center for Women and Children, Chongqing, People’s Republic of China; 3Aier Eye Hospital of Wuhan University (Wuhan Aier Eye Hospital), Wuhan, Hubei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yanning Yang, Department of Ophthalmology, Renmin Hospital of Wuhan University, Jiefang Road 238, Wuhan, Hubei Province, People’s Republic of China, Tel/Fax +86-27-88041911, Email [email protected]
Background: Although previous studies of sleep-related behaviors in relation to primary open-angle glaucoma (POAG) have been noted, the causal relationship remains unclear. The purpose of our present study was to investigate the relationships of genetically predicted sleep traits with POAG using a two-sample bidirectional Mendelian randomization (MR) method.
Methods: Summary-level data collected from publicly available genome-wide association studies (GWAS) of European decent were applied for the bidirectional MR analysis. After quality control steps, independent single-nucleotide polymorphisms for eight sleep behaviors and POAG were selected as the genetic instruments. The inverse-variance weighted (IVW) approach was adopted as the primary method, which was complemented by a series of sensitivity analyses to assess the robustness of the results by estimating heterogeneity and pleiotropy. Multivariable MR (MVMR) was used to assess the direct effect of sleep traits on POAG, after adjusting for several confounding factors.
Results: Our investigation revealed a positive correlation between genetically predicted ease of getting up in the morning and sleep duration and POAG using the IVW method (odds ratio (OR)=1.78, 95% confidence interval (CI):1.29– 2.46, P = 4.33× 10− 4; OR = 1.66, 95% CI:1.18– 2.34, P = 3.38× 10− 3, respectively). Other supplementary MR methods also confirmed similar results. Moreover, the MVMR results also revealed that the adverse effects of these two sleep traits on POAG persisted after adjusting for body mass index, smoking, drinking, and education (all P < 0.05). Conversely, the relationships between genetic liability of POAG and different sleep behaviors were not statistically significant in the reverse-direction MR estimate (all P > 0.05).
Conclusion: Our study demonstrated that genetic prediction of getting up easily in the morning or sleep duration were associated with a higher risk of POAG, but not vice versa, in a European population. Further validation and clinical interventions are required to offer potential strategies to prevent and manage POAG.
Keywords: genome-wide association study, mendelian randomization, sleep behaviors, primary open-angle glaucoma, risk factors
Introduction
Glaucoma is a heterogeneous group of irreversible diseases characterized by progressive optic neuropathy, which commonly impairs the visual field and is the second leading cause of permanent blindness worldwide.1,2 Primary open-angle glaucoma (POAG) is the most common form of disease. The total number of POAG cases in the world was around 68.56 million in 2020 and will rise to 111.8 million by 2040, with Asia and Africa accounting for the vast majority.3 Despite tremendous research efforts, the etiology of POAG remains poorly understood and the risk factors contributing to its progression have not been fully characterized.4
In the past decade, considerable effort has been devoted to elucidating the genetic causes and risk factors of POAG. A recently published genome-wide association study (GWAS) identified 127 novel genetic variants associated with POAG.5 Currently, it is widely accepted that sleep-related behavioral phenotypes and POAG have bidirectional relationships, that is, growing evidence indicates that patients with poor sleep traits are more likely to develop a risk of POAG.6–8 In contrast, patients with glaucoma are more susceptible than healthy people to sleep dysfunction such as obstructive sleep apnea (OSA), snoring, or insomnia.9–13
Despite increasing evidence from observational studies suggesting a correlation between sleep behaviors and POAG, there have also been several clinical studies reporting no association between them,14–16 with the existing literature on the subject being inconclusive and debatable. Additionally, whether demographics, socioeconomic status, and comorbidities are potential confounding factors in this relationship remains to be elucidated. Recently, Zhou et al conducted a pooled meta-analysis of sleep duration and risk of major eye disorders, suggesting no association between inadequate sleep duration and glaucoma.17 In addition, to date, no systematic, evidence-based randomized controlled trial (RCT) has summarized the association between sleep behaviors and POAG globally. Therefore, a better understanding of sleep-related phenotypes causally related to POAG may contribute to the prevention of adverse outcomes.
Given the tendency of the RCT approach to be expensive and time-consuming, Mendelian randomization (MR) analysis has been widely used to determine the causal estimate of risk factors for disease outcomes by utilizing genetic variants such as single nucleotide polymorphisms (SNPs) as instrumental variables (IVs). In contrast to observational studies, MR is an alternative estimation technique in which SNPs are randomly assigned during conception and are irrelevant to environmental confounding factors, which could strengthen the causal inference by eliminating substantial confounding bias and avoiding reverse causality.18 To the best of our knowledge, no effort has yet been made to combine different sleep-related phenotypes and POAG outcomes using an MR design. Here, we employed a two-sample MR framework to thoroughly disentangle the causal associations between different sleep traits and the risk of POAG, and explore whether there was a bidirectional relationship in both directions.
Materials and Methods
Study Design
A schematic representation of the research design is shown in Figure 1. The key component of our MR study was to examine the causal role of genetically predicted sleep-related phenotypes in the susceptibility to POAG. Our main analysis was constructed to meet the following assumptions for valid genetic variants: (a) reliably and robustly associated with exposure, (b) independent of any risk factor-outcome confounders, and (c) influence the outcome only via exposure.19 The Coordinating Ethics Committee of the Hospital District of Helsinki and Uusimaa approved the FinnGen study protocol Nr HUS/990/2017. The FinnGen study was approved by Finnish Institute for Health and Welfare. The remaining analyses of publicly available datasets did not require ethical approval.
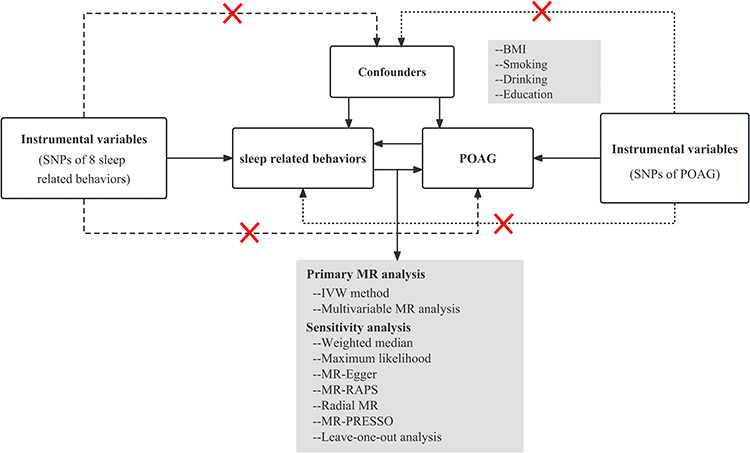 |
Figure 1 Workflow of bidirectional Mendelian randomization analysis demonstrating causality between sleep-related behaviors and POAG. Three principal assumptions of a valid genetic instrument for MR analysis. The dotted line and the “×” represent variables that are invalid once correlated with the outcome or potential confounders. Abbreviations: POAG, primary open-angle glaucoma; IVW, inverse variance weighted; MR-RAPS, MR robust adjusted profile score; MR-PRESSO, MR pleiotropy residual sum and outlier; BMI, body mass index. |
GWAS Summary Statistics of Sleep-Related Phenotypes
We used published genome-wide association studies (GWAS) summary-level data of eight sleep-related phenotypes from large genetic consortia20 in the PubMed and IEU databases (https://gwas.mrcieu.ac.uk). A summary of the data sources for each sleep-related phenotype is presented in Table 1. The eight sleep traits were self-reported chronotype (morning/evening person), ease of getting up in the morning, sleep duration, napping during the day, insomnia, daytime dozing/narcolepsy, snoring, and OSA. A detailed description of the data sources is presented in Table S1. Genetic variant relationships for all sleep phenotypes were measured using available participants of European ancestry. To assess the potential for genetic confounding through clinical traits such as body mass index (BMI), smoking, drinking, and education,6 we further applied the conventional linear multivariable MR (MVMR) approach to disentangle the direct effect of sleep traits on POAG by adjusting for these factors. The summary statistics for these factors were obtained from the corresponding GWASs.21–23
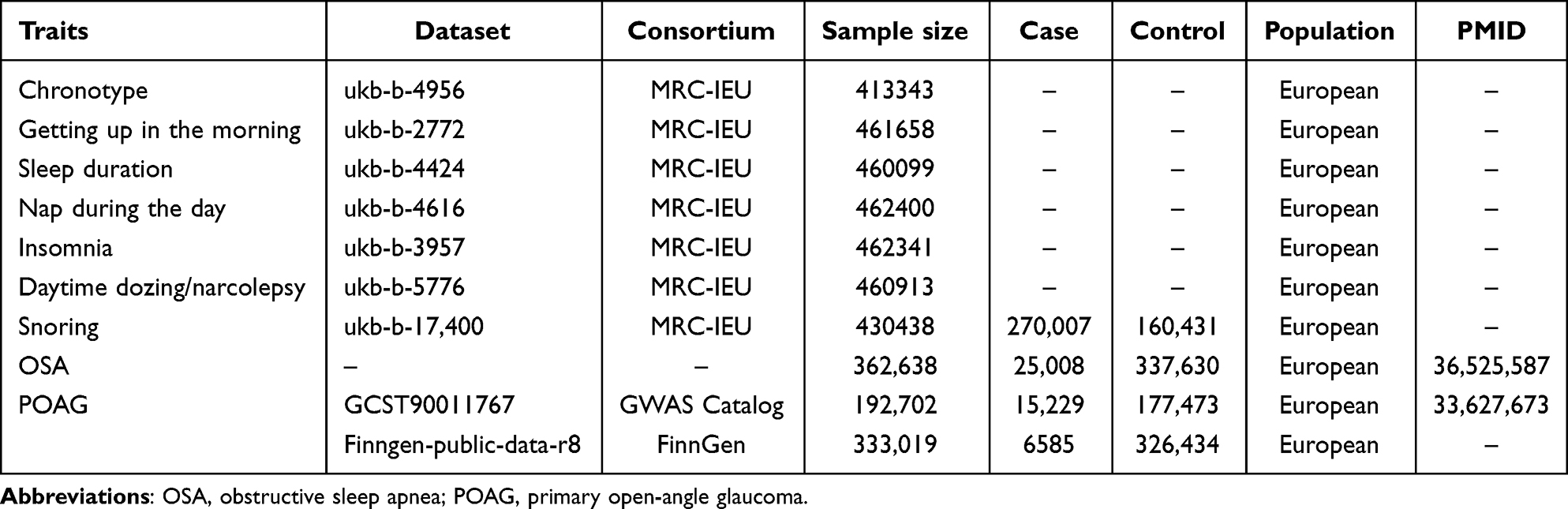 |
Table 1 Detailed Information on Included Traits in this Study |
GWAS Summary Statistics of POAG
The genetic variant relationships with the risk of POAG were retrieved from a meta-analysis of GWAS on 18 independent studies of European ancestry,5 which included UKBB datasets. Most studies have restricted glaucoma to POAG based on the ICD9/ICD10 criteria. Considering the potential bias of overlapping samples between sleep phenotypes and POAG, the POAG GWAS summary statistics without UKBB individuals (15,229 POAG cases and 177,473 controls) were used in the bidirectional MR analysis (Table 1). Moreover, summary statistics for POAG were acquired from the FinnGen study (https://www.finngen.fi/en/access_results; 6585 POAG cases and 326,434 controls) for external validation. GWAS adjusted for age, sex, and study-specific principal components.5
Selection of Genetic Instruments
We identified SNPs robustly associated with sleep traits to obtain eligible genetic instruments at a genome-wide significance threshold of P < 5×10−8. Because the number of eligible IVs (P < 5×10−8) was null, SNPs with a relatively relaxed and previously used instrument threshold (P < 5×10−5) for OSA were selected to obtain a more comprehensive result.24 Based on the 1000 Genomes Project European reference panel, the candidate set of SNPs was located in different gene regions without linkage disequilibrium LD (R2<0.001 and a window size = 10,000 kb) estimation. We searched for instrumental variables using PhenoScanner (http://www.phenoscanner.medschl.cam.ac.uk/) to identify any previous associations with potential confounders. We further harmonized the exposure and outcome datasets to obtain genetic instrument effects on POAG and to remove palindromic SNPs. Specially, when genetic instruments associated with exposure factor were not available in the outcome GWAS dataset, proxy SNPs with a high LD (R2> 0.8) corresponding to the summary statistics in the outcome GWAS dataset were applied for the causal estimation procedure. If no proxy SNP was found with this framework, we abandoned the unavailable SNP instrument. Regarding existing weak instrument bias, SNPs with an F statistic >10 were considered sufficiently strong instruments for our analysis.25 In addition, the proportion of variance (R2) explained by the SNPs was used to verify the strength of the instruments for exposure factors. The F statistic and R2 were calculated using previously reported methods to evaluate the strength of the eligible SNPs.26
Statistical Analysis
MR Analysis
In this study, we firstly used sleep-related phenotypes as the exposure and POAG as the outcome to perform MR with “TwoSampleMR” package. Inverse-variance weighting (IVW) was used as the primary approach,19 which calculated and combined the Wald ratio of each SNP through a meta-analysis to estimate the overall causal association between sleep traits and POAG. However, this may be biased by horizontal pleiotropy.27 We therefore adopted multiple MR analysis as complementary methods, including weighted median, maximum likelihood, MR-Egger, MR Robust Adjusted Profile Score (MR-RAPS), and radial MR, to estimate the robustness and reliability for MR estimates.28–32 Additionally, we assessed the impact of adding potential confounders to the adjusted model individually in any MVMR analysis. Details of the SNPs for the four confounders are listed in Table S2.
For the primary analysis, Bonferroni correction was used to account for multiple comparisons, and a threshold P-value of 0.05/8 (P < 6.25 × 10−3) was used to prioritize the results for further analysis. A value between 6.25 × 10−3 and 0.05 was regarded as evidence of suggestive causal inference. A replication MR analysis was also conducted on the preliminarily identified estimation for external validation using the GWAS databases of the FinnGen study.
Reverse Causality Detection
Following the same screening criteria for sleep-related phenotypes, eligible genetic instruments for POAG exposure were also selected from publicly available GWAS for bidirectional MR analysis to detect potential reverse causality. The main effect was estimated by applying the aforementioned MR method. The results were considered statistically significant at P < 0.05.
Pleiotropy and Sensitivity Analysis
In our study, IVW, MR-Egger regression, and radial MR analyses were used to detect heterogeneity, and Cochran’s Q-test was used to assess the heterogeneity between the SNP-specific estimates. Cochrane’s Q value and I2 were calculated to appraise heterogeneity and a fixed-effect model would be adopted if there was no significant heterogeneity existed (I2≤50%). SNPs that exhibited significant heterogeneity were removed and MR estimates were reassessed. The MR-Egger method assumes no intercept term in the model, and the intercept is considered to be zero. When the P value is larger than 0.05 in the MR-Egger intercept test, it can provide evidence for absence of pleiotropic bias.30 In addition, pleiotropy was examined using the MR Pleiotropy Residual Sum and Outlier (MR-PRESSO) global tests. Thus, P-values were calculated according to 5000 simulations, which could detect the outlier SNPs reflecting likely pleiotropy with a P-value of 0.05, and correct for horizontal pleiotropy by removing outlier.33 Furthermore, the directionality that exposure causes the outcome was determined using the MR Steiger test.34 Leave-one-out sensitivity analysis was applied to evaluate whether the MR results relied on any single SNP.
The associations between sleep-related phenotypes and POAG from different databases, including the UK Biobank and FinnGen studies, were combined by meta-analysis using the R software. Causal effect estimates were interpreted per category increase in the sleep-related phenotypes. Additionally, we presented our MR results as odds ratios (ORs) accompanied by their respective 95% confidence intervals (CIs), which represented the outcome risk associated with unit changes in exposure. All statistical analyses were performed using the “TwoSampleMR”, “mr.raps”, and “MR-PRESSO” MR-PRESSO packages in R software version 4.3.0.
Results
After removing palindromic and unavailable proxy SNPs, 132 SNPs were used to instrument chronotype, 66 for getting up in the morning, 58 for sleep duration, 88 for nap during the day, 32 for insomnia, 30 for daytime dozing/narcolepsy, 35 for snoring, and 77 for OSA exposure. Based on the selection criteria, we selected 51 SNPs for POAG as IVs for the analysis of the causal effects of POAG on sleep trait outcomes. Detailed information on each SNP for sleep traits and POAG used in the current study is shown in Tables S3–S11. Finally, the screened SNPs with F-statistics > 10, indicating no weak tool bias, were selected as IVs for further MR analysis.
Univariable MR Analyses
The results of the MR analysis are presented in Table 2 and Figures S1, S2 and S3. With the IVW method providing the main results, genetic liability to ease of getting up in the morning and sleep duration were associated with a higher risk of POAG outcome (getting up easily in the morning and POAG, IVW OR = 1.78, 95% CI:1.29–2.46, P = 4.33 × 10−4; sleep duration and POAG, IVW OR = 1.66, 95% CI:1.18–2.34, P = 3.38 × 10−3). MR estimates were significant and consistent across various methods, including the weighted median, maximum likelihood, MR-PRESSO, MR-RAPS, and radial MR methods (Table 2). Correct causal direction was also confirmed using the MR-Steiger directionality test (P for Steiger = 1.99 × 10−102, 3.90 × 10−90, respectively). The MR-Egger regression test showed no evidence of pleiotropy (getting up easily in the morning and sleep duration for POAG, P = 0.489 and 0.145, respectively), and the Cochran’s Q statistic showed no significant heterogeneity with I2 statistics ranging from 27.94% to 34.99% using IVW, maximum likelihood, MR-Egger, and radial MR (IVW getting up easily in the morning and sleep duration for POAG, P-value=2.00×10−2 and 6.00 × 10−3) as presented in Table 2. Although leave-one-out analysis indicated that one outlier SNP was detected in the analysis of POAG (Figure S1), similar results were obtained after excluding the respective SNP (IVW OR = 1.44, 95% CI:1.04–2.00, P = 0.027), suggesting that the overall estimates of causal effects were not driven by a single SNP. Moreover, the MR-PRESSO global test did not detect any outlier SNPs or horizontal pleiotropic effects of getting up easily in the morning or sleep duration on the risk of POAG (P > 0.05, Table 2).
 |
Table 2 Mendelian Randomization Positive Results and Heterogeneity Analysis for Effect of Genetically Predicted Sleep Related Behaviors on POAG |
However, few significant causal inferences were identified for other genetically predicted sleep traits with POAG (all P > 0.05), without any evidence of significant heterogeneity in MR estimates among selected SNPs. As delineated in Table S12, the aforementioned complementary MR methods produced similar results with that using IVW method. All MR-Egger intercept tests indicated no horizontal pleiotropy (P > 0.05). Consistent with the main MR analysis, leave-one-out analysis revealed that the main causal associations were not directly driven by SNPs (Figure S1).
External Validation of Sleep Behaviors for POAG
Using the significant-variant strategy in different datasets, we decided to perform an MR analysis between sleep-related phenotypes and POAG derived from the FinnGen dataset. To further verify the positive association, the validated analysis using the FinnGen GWAS cohort for POAG outcome yielded similar estimates as the main finding that POAG might be influenced by getting up easily in the morning rather than sleep duration (IVW OR = 1.57, 95% CI:1.02–2.40, P = 3.89×10−2, Table S13).
Multivariable MR Analyses
Given the possible effects of BMI, smoking, drinking, and education on estimating causal inferences, we further performed an MVMR analysis adjusting for these confounding factors to infer the direct effect of sleep-related phenotypes on POAG. As for the overall association between genetically predicted ease of getting up in the morning and POAG susceptibility, MR estimates were not attenuated after adjustments were made for BMI, smoking initiation, drinking, and educational attainment (all P < 0.05, Table S14). Additionally, the patterns between genetic liability, sleep duration, and POAG outcome were still significant after adjusting for multivariable factors (IVW, all P < 0.05, Table S14). However, the results from our MVMR estimation did not reveal a possible causal relationship between other sleep traits and higher POAG risk when these factors were accounted for.
Reverse Mendelian Randomization
Regarding the reverse direction, genetic liabilities for POAG were used as exposure.
No clear evidence supported a causal association between POAG and the different sleep-related phenotypes in the seven analyses mentioned above, including the IVW method (IVW, all P > 0.05, Table S15). Similar results were obtained in subsequent sensitivity analyses. The statistical results for reverse-direction MR are presented in Figures S4, S5 and S6. The overall estimations were not driven by a single genetic variant tested in “leave-one-out” analysis (Figure S4).
Discussion
To the best of our knowledge, this is the first study to explore the effect of multiple sleep-related behaviors on POAG outcomes using two-sample bidirectional MR analysis across GWAS datasets of the European population. The results demonstrated that a genetic predisposition to ease getting up in the morning or sleep duration could be the cause of POAG susceptibility, and POAG might not change sleep-related behaviors in reverse-direction MR analysis. In addition, genetically predicted getting up easily in the morning was also found to be associated with POAG, using a similar approach to reassess in the FinnGen cohorts, further suggesting the reliability of the causal estimates identified in this study. Moreover, our multivariable MR estimates were consistent with the univariate MR findings after adjusting for potential confounding factors. Therefore, it can be concluded with strong evidence from this study that genetic liability to sleep traits, especially the ease of getting up in the morning and sleep duration, is an important risk factor for POAG.
Poor sleep quality and disruption are commonly observed in patients with POAG or glaucoma. A Pittsburgh Sleep Quality Index survey demonstrated that glaucoma patients had higher (worse) scores compared with controls for sleep latency, sleep duration, and subjective sleep quality.35 A prospective cross-sectional study with consecutive sampling in the Southeast Asian population indicated that patients with primary glaucoma have poorer sleep quality than controls.13 On the other hand, although we identified a detrimental impact of ease of getting up in the morning on POAG development, there was inadequate previous evidence for causal associations between them. Consistent with our findings, the development of getting up easily in the morning has been observed in 24.5% of patients with glaucoma at various disease stages.36 Notably, the prevalence of glaucoma and waking up in the early morning tends to increase with age, the higher risk of POAG in individuals with waking up early may be attributed to age age-related bias. Thus, the relative age effect in both clinical phenotypes could not be neglected. To the best of our knowledge, no previous MR study has investigated the association between genetically predicted getting up easily in the morning with POAG, and several MR analyses have reported that trouble getting up in the morning is associated with an increased risk of nonalcoholic fatty liver disease, end-stage renal disease, and auditory hallucinations.37–39
In addition, we expanded on these findings by demonstrating the effects of sleep duration on POAG. Genetic association data estimated for sleep duration was retrieved from UKBB dataset of European ancestry. The data was assessed by answering the question “About how many hours sleep do you get in every 24 hours? (please include naps)” and the results show the mean time of sleep duration is about 7h. And over 80% of the samples range from 6 to 8 h. In comparison with normal sleep, poor sleep duration increases a 1.66-fold higher risk of POAG in our MR estimate. Observational studies have suggested that sleep duration is an independent risk factor for glaucoma. A prospective, case-control study of matched patients with advanced glaucoma proposed that these patients showed more awakenings at night, shorter sleep duration, and lower sleep efficiency than the control subjects.40 Another prospective cohort study in the UK Biobank concluded that short or long sleep duration, individually or jointly, was associated with the risk of glaucoma, but not with POAG subtype.6 In addition, a cross-sectional study stratified by obesity status using data from the Korean National Health and Nutrition Examination Survey revealed a U-shaped association between sleep duration and the prevalence of POAG.41 However, a systematic meta-analysis showed that inappropriate sleep duration was not associated with the incidence of glaucoma,17 which contradicts the present findings of the MR analysis.
Several observations and systematic analyses suggest an equivocal relationship between POAG and other sleep traits. A Munich chronotype questionnaire indicated that no clear changes were identified in the chronotype, as determined by the sleep phase of patients with glaucoma.42 Similarly, Sun et al found an excess risk of glaucoma among individuals with late-chronotype sleep pattern.6 An interviewer-administered semi-structured questionnaire suggested that patients showed a high prevalence of insomnia, excessive daytime dozing/narcolepsy, and snoring.43 An observational, prospective, non-exposed-exposed study with a period of 18 months found that insomnia was a potential risk factor for POAG.44 Despite the opposite result reported in another prospective cohort study involving 3468 subjects, the results indicated that severe snoring was not significantly associated with POAG prevalence of POAG.45 Balbay et al concluded that a higher prevalence of OSA is observed in patients with POAG.46 Conversely, a population-based, cross-sectional study of Indian and Malay adults indicated that a non-significant increase was confirmed in the likelihood of having POAG in those with an intermediate/higher risk of OSA than in those with a low risk.47 A cross-sectional telephone survey using the STOP-BANG questionnaire demonstrated no evidence that glaucoma patients were more likely to have OSA or develop more severe OSA than others.16 Furthermore, Chan et al argued that the presence of glaucoma increased the risk of moderate-to-severe OSA compared with the control group.12 In contrast, a population-based nationwide cohort study showed no significant increase in the risk of OSA in patients with POAG.10 A meta-analysis of OSA in patients with glaucoma confirmed that OSA is associated with a significantly increased risk of glaucoma.48 A recently published meta-analysis suggested that OSA is associated with a higher risk of glaucoma and its subtype.49 These inconsistent conclusions may be attributed to different risk biases, including the control of confounding factors and reverse caution. Considering the wide range of potential confounders, the findings about the causal effects of OSA on glaucoma in our MR analysis are consistent with a previous MR study conducted by Ingold Nathan et al.50 Different from their MR design, we used MVMR to avoid horizontal pleiotropy, which allowed us to further consider the influence of additional factors and draw a more solid conclusion. After adjusting for these confounding factors, the previously identified MR associations were retained, which suggested that confounding factors did not drive the observed estimate between sleep traits and POAG. Moreover, we extended the scope of our study by including chronotype, napping during the day, insomnia, daytime dozing/narcolepsy, snoring, and OSA as studied outcomes. Although there was no potential causal inference between these genetically predicted sleep traits and POAG, we still need to pay attention to sleep-related health to mitigate the incidence of POAG.
To this end, reverse MR analysis was performed to determine the influence of POAG on sleep-related behaviors. However, no clear evidence of a causal relationship between POAG and sleep traits has been identified, suggesting that sleep traits are more likely to be a cause rather than a consequence of POAG. Furthermore, the aim of building a multivariate MR analysis in our study was to investigate the causal effect of multiple sleep-related behaviors on POAG outcomes, with the advantage that the direct effect of sleep traits on POAG could be robustly estimated in different scenarios. Thus, possible confounding factors, reverse direction, or pleiotropic pathway effects exerted by secondary exposures.51 More convincingly, our results demonstrated that increasing the ease of getting up in the morning or sleep duration was associated with a high risk of POAG, after adjusting for BMI, smoking, drinking, and education. This finding is in accordance with that of a previous observational study showing that the associations of sleep patterns with glaucoma did not differ according to BMI, lifestyle factors such as smoking status and physical activity.6
The underlying mechanisms that explain the association between sleep-related behaviors and POAG are biologically plausible. One such common pathogenetic mechanism may involve systemic inflammation-related processes, such as C-reactive protein, neutrophil-to-lymphocyte ratio, systemic immune inflammation index, and cytokine TNF-α, which are more relevant to the development of optic nerve neuropathy and vision in POAG.52–54 Vascular factors, including recurrent hypoxia with increased vascular resistance and oxidative stress damage to the optic nerve, have been implicated in POAG pathogenesis of POAG.55 Evidence also shows that OSA predisposes patients to optic nerve head ischemia and damage through mitochondrial dysregulation and hemodynamic changes to retinal blood vessels, which are subjected to the progress of POAG.48,56 Furthermore, chronic insomnia and its related physiological responses may stimulate neurotransmitter secretion and the autonomic nervous system, thereby affecting the regulation of IOP and optic nerve perfusion.57–59 Additionally, mood disorders, such as anxiety and depression, co-occur often with insomnia and may also result in elevated IOP through dysregulation of cortisol hormone.60,61 Nonetheless, the complex interactions between poor sleep behaviors and an increased risk of POAG have not been sufficiently elucidated.
This study, following the MR guidelines, elucidated the causal inferences between the genetic liability for eight sleep behaviors and POAG, with several important implications. Our research has the main strength of obtaining less confounded estimates from the largest summary-level GWAS datasets of sleep behaviors and POAG with replication and external validation, along with multiple sensitivity analyses. Thus, the reality and robustness of the MR results were ensured. Our study was a bidirectional MR study that can strongly determine whether reverse causation exists. All strong and reliable IVs from different large-scale GWASs were introduced to avoid potentially weak instrumental biases and enhance credibility. In addition, we stratified the population according to European descent and minimized the bias due to ethnic heterogeneity.
Nevertheless, it is inevitable that there are also some potential limitations needed to be noted. First, the results were obtained from European individuals and might not be generalized to other ethnic populations. Further replication based on cohorts of different ancestry was still warranted. Second, although all eligible IVs associated with sleep-related behaviors were selected, they could only represent a relatively small proportion of complex phenotypes. Thus, our analysis cannot be considered an accurate proxy for exposure. Third, our study mainly chose the clinical data of sleep traits from a self-reported questionnaire instead of accelerometer estimation, which might have led to a potential bias. Fourth, potential confounders, such as stress or depression may affect sleep duration and needed to be investigated in the future observational study. Fifth, although the potential causal relationships between sleep traits and POAG could be retrieved from a genetic perspective, the underlying mechanisms and specific biological pathways are uncertain and require further investigation.
Conclusion
In summary, this comprehensive bidirectional two-sample MR analysis demonstrated that individuals with suboptimal sleep patterns, such as ease of getting up in the morning and poor sleep duration, were at increased risk of POAG. To better understand and manage both phenotypes in our clinical implications, potential ophthalmologic screening and intervention among individuals with chronic sleep problems should be made to help prevent POAG.
Data Sharing Statement
The data used in our Mendelian randomization analysis were obtained from the UK Biobank and the MRC IEU Open GWAS Project. We also acknowledge the participants and investigators of the FinnGen Study. Further inquiries can be directed to the corresponding author.
Ethics Approval
The present study was strictly conducted in accordance with the Declaration of Helsinki and International Ethical Guidelines for Health-related Research Involving Humans. This study was approved by the Medical Ethics Committee of Renmin Hospital of Wuhan University. Additional ethics approval or participate informed consent have been obtained in the original studies.
Acknowledgments
The authors thank all the investigators of the UK Biobank and the MRC IEU Open GWAS Project for publicly providing data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Fundamental Research Funds for Central Universities (2042023kf0047); National Natural Science Foundation of China (82301193); and Hubei Provincial Natural Science Foundation of China (2023AFB223).
Disclosure
The authors declare that they have no conflict of interest.
References
1. Tham YC, Li X, Wong TY, et al. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
2. Stein JD, Khawaja AP, Weizer JS. Glaucoma in adults-screening, diagnosis, and management: a review. JAMA. 2021;325(2):164–174. doi:10.1001/jama.2020.21899
3. Zhang N, Wang J, Li Y, Jiang B. Prevalence of primary open angle glaucoma in the last 20 years: a meta-analysis and systematic review. Sci Rep. 2021;11(1):13762. doi:10.1038/s41598-021-92971-w
4. Nickells RW, Howell GR, Soto I, John SW. Under pressure: cellular and molecular responses during glaucoma, a common neurodegeneration with axonopathy. Annu Rev Neurosci. 2012;35(1):153–179. doi:10.1146/annurev.neuro.051508.135728
5. Gharahkhani P, Jorgenson E, Hysi P, et al. Genome-wide meta-analysis identifies 127 open-angle glaucoma loci with consistent effect across ancestries. Nat Commun. 2021;12(1):1258. doi:10.1038/s41467-020-20851-4
6. Sun C, Yang H, Hu Y, et al. Association of sleep behaviour and pattern with the risk of glaucoma: a prospective cohort study in the UK Biobank. BMJ Open. 2022;12(11):e063676. doi:10.1136/bmjopen-2022-063676
7. Lee TE, Kim JS, Yeom SW, et al. Long-term effects of obstructive sleep apnea and its treatment on open-angle glaucoma: a big-data cohort study. J Clin Sleep Med. 2023;19(2):339–346. doi:10.5664/jcsm.10334
8. Gubin DG, Malishevskaya Capital Te C, Astakhov YS, et al. Progressive retinal ganglion cell loss in primary open-angle glaucoma is associated with temperature circadian rhythm phase delay and compromised sleep. Chronobiol Int. 2019;36(4):564–577. doi:10.1080/07420528.2019.1566741
9. Friedlander AH, Graves LL, Chang TI, et al. Prevalence of primary open-angle glaucoma among patients with obstructive sleep apnea. Oral Surg Oral Med Oral Pathol Oral Radiol. 2018;126(3):226–230. doi:10.1016/j.oooo.2018.01.021
10. Lee SY, Yu H, Kim DK. Glaucoma is associated with the risk of obstructive sleep apnea: a population-based nationwide cohort study. Diagnostics. 2022;13(1):12. doi:10.3390/diagnostics13010012
11. Fan YY, Su WW, Liu CH, et al. Correlation between structural progression in glaucoma and obstructive sleep apnea. Eye. 2019;33(9):1459–1465. doi:10.1038/s41433-019-0430-2
12. Chan YH, Chuang LH, Yu CC, et al. Prospective evaluation of the comorbidity of obstructive sleep apnea in patients with glaucoma. J Clin Sleep Med. 2022;18(1):47–56. doi:10.5664/jcsm.9488
13. Chin JY, Toh ZH, Lo YT, et al. Effects of primary glaucoma on sleep quality and daytime sleepiness of patients residing at an equatorial latitude. Int J Ophthalmol. 2020;13(9):1451–1458. doi:10.18240/ijo.2020.09.18
14. Lee CY, Chien HW, Huang JY, et al. The need for glaucoma management in glaucoma patients with concurrent obstructive sleep apnea: a population-based cohort study. Biomedicines. 2023;12(1):11. doi:10.3390/biomedicines12010011
15. Davanian A, Williamson L, Taylor C, et al. Optical coherence tomography angiography and Humphrey visual field in patients with obstructive sleep apnea. J Clin Sleep Med. 2022;18(9):2133–2142. doi:10.5664/jcsm.10054
16. Alotaibi M, Alsubaie M, Alharthi A, et al. The risk of obstructive sleep apnea in open-angle glaucoma patients. Cureus. 2021;13(10):e18699. doi:10.7759/cureus.18699
17. Zhou M, Li DL, Kai JY, Zhang XF, Pan CW. Sleep duration and the risk of major eye disorders: a systematic review and meta-analysis. Eye. 2023;37(13):2707–2715. doi:10.1038/s41433-023-02403-4
18. Davies NM, Holmes MV, Davey Smith G. Reading Mendelian randomisation studies: a guide, glossary, and checklist for clinicians. BMJ. 2018;362:k601. doi:10.1136/bmj.k601
19. Lawlor DA, Harbord RM, Sterne JA, Timpson N, Davey Smith G. Mendelian randomization: using genes as instruments for making causal inferences in epidemiology. Stat Med. 2008;27(8):1133–1163. doi:10.1002/sim.3034
20. Campos AI, Ingold N, Huang Y, et al. Discovery of genomic loci associated with sleep apnea risk through multi-trait GWAS analysis with snoring. Sleep. 2023;3:46.
21. Yengo L, Sidorenko J, Kemper KE, et al. Meta-analysis of genome-wide association studies for height and body mass index in approximately 700000 individuals of European ancestry. Hum Mol Genet. 2018;27(20):3641–3649. doi:10.1093/hmg/ddy271
22. Liu M, Jiang Y, Wedow R, et al. Association studies of up to 1.2 million individuals yield new insights into the genetic etiology of tobacco and alcohol use. Nat Genet. 2019;51(2):237–244. doi:10.1038/s41588-018-0307-5
23. Okbay A, Wu Y, Wang N, et al. Polygenic prediction of educational attainment within and between families from genome-wide association analyses in 3 million individuals. Nat Genet. 2022;54(4):437–449. doi:10.1038/s41588-022-01016-z
24. Lin Y, Yang Y, Fu T, et al. Impairment of kidney function and kidney cancer: a bidirectional Mendelian randomization study. Cancer Med. 2023;12(3):3610–3622. doi:10.1002/cam4.5204
25. Palmer TM, Lawlor DA, Harbord RM, et al. Using multiple genetic variants as instrumental variables for modifiable risk factors. Stat Methods Med Res. 2012;21(3):223–242. doi:10.1177/0962280210394459
26. Anderson EL, Richmond RC, Jones SE, et al. Is disrupted sleep a risk factor for Alzheimer’s disease? Evidence from a two-sample Mendelian randomization analysis. Int J Epidemiol. 2021;50(3):817–828. doi:10.1093/ije/dyaa183
27. Lee CH, Cook S, Lee JS, Han B. Comparison of two meta-analysis methods: inverse-variance-weighted average and weighted sum of Z-Scores. Genomics Inform. 2016;14(4):173–180. doi:10.5808/GI.2016.14.4.173
28. Bowden J, Davey Smith G, Haycock PC, Burgess S. Consistent estimation in mendelian randomization with some invalid instruments using a weighted median estimator. Genet Epidemiol. 2016;40(4):304–314. doi:10.1002/gepi.21965
29. Nguyen LT, Schmidt HA, von Haeseler A, Minh BQ. IQ-TREE: a fast and effective stochastic algorithm for estimating maximum-likelihood phylogenies. Mol Biol Evol. 2015;32(1):268–274. doi:10.1093/molbev/msu300
30. Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. 2015;44(2):512–525. doi:10.1093/ije/dyv080
31. Zhao Q, Wang J, Hemani G, Bowden J, Small DS. Statistical inference in two-sample summary-data Mendelian randomization using robust adjusted profile score. Ann Statist. 2020;48(3):1742–1769. doi:10.1214/19-AOS1866
32. Bowden J, Spiller W, Del Greco MF, et al. Improving the visualization, interpretation and analysis of two-sample summary data mendelian randomization via the radial plot and radial regression. Int J Epidemiol. 2018;47(4):1264–1278. doi:10.1093/ije/dyy101
33. Verbanck M, Chen CY, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat Genet. 2018;50(5):693–698. doi:10.1038/s41588-018-0099-7
34. Lutz SM, Wu AC, Hokanson JE, Vansteelandt S, Lange C. Caution against examining the role of reverse causality in mendelian randomization. Genet Epidemiol. 2021;45(5):445–454. doi:10.1002/gepi.22385
35. Stoner AM, Patnaik JL, Ertel MK, et al. Subjective and objective measurement of sleep quality and activity in glaucoma. J Glaucoma. 2023;32(4):265–271. doi:10.1097/IJG.0000000000002186
36. Qiu M, Ramulu PY, Boland MV. Association between sleep parameters and glaucoma in the United States Population: national health and nutrition examination survey. J Glaucoma. 2019;28(2):97–104. doi:10.1097/IJG.0000000000001169
37. Fan H, Liu Z, Zhang X, et al. Investigating the association between seven sleep traits and nonalcoholic fatty liver disease: observational and mendelian randomization study. Front Genet. 2022;13:792558. doi:10.3389/fgene.2022.792558
38. Li K, Zhao J, Yang W, Ye Z. Sleep traits and risk of end-stage renal disease: a mendelian randomization study. BMC Med Genomics. 2023;16(1):76. doi:10.1186/s12920-023-01497-9
39. Yu M, Du Y, Liu K, et al. Sleep duration and auditory hallucinations: genetic correlation and two-sample Mendelian randomization study. J Affect Disord. 2021;291:409–414. doi:10.1016/j.jad.2021.04.038
40. Lanzani MF, de Zavalia N, Fontana H, et al. Alterations of locomotor activity rhythm and sleep parameters in patients with advanced glaucoma. Chronobiol Int. 2012;29(7):911–919. doi:10.3109/07420528.2012.691146
41. Lee JA, Han K, Min JA, Choi JA. Epidemiologic Survey Committee of the Korean Ophthalmological S, (2016) Associations of sleep duration with open angle glaucoma in the Korea national health and nutrition examination survey. Medicine. 2016;95(52):e5704. doi:10.1097/MD.0000000000005704
42. Bierings R, Gordijn MCM, Jansonius NM, Challet E. Chronotyping glaucoma patients with the Munich ChronoType Questionnaire: a case-control study. PLoS One. 2019;14(3):e0214046. doi:10.1371/journal.pone.0214046
43. Onen SH, Mouriaux F, Berramdane L, et al. High prevalence of sleep-disordered breathing in patients with primary open-angle glaucoma. Acta Ophthalmol Scand. 2000;78(6):638–641. doi:10.1034/j.1600-0420.2000.078006638.x
44. Marc A, Stan C. Effect of physical and psychological stress on the course of primary open angle glaucoma. Oftalmologia. 2013;57(2):60–66.
45. Wang YX, Xu L, Li JJ, et al. Snoring and glaucoma. PLoS One. 2014;9(2):e88949. doi:10.1371/journal.pone.0088949
46. Balbay EG, Balbay O, Annakkaya AN, et al. Obstructive sleep apnoea syndrome in patients with primary open-angle glaucoma. Hong Kong Med J. 2014;20(5):379–385. doi:10.12809/hkmj134021
47. Mehta A, Man REK, Gan AT, et al. Association between risk of obstructive sleep apnea and glaucoma: the singapore epidemiology of eye diseases study. J Glaucoma. 2022;31(12):935–940. doi:10.1097/IJG.0000000000002105
48. Garcia-Sanchez A, Villalain I, Asencio M, Garcia J, Garcia-Rio F. Sleep apnea and eye diseases: evidence of association and potential pathogenic mechanisms. J Clin Sleep Med. 2022;18(1):265–278. doi:10.5664/jcsm.9552
49. Cheong AJY, Wang SKX, Woon CY, et al. Obstructive sleep apnoea and glaucoma: a systematic review and meta-analysis. Eye. 2023;37(15):3065–3083. doi:10.1038/s41433-023-02471-6
50. Ingold N, Campos AI, Han X, et al. Is genetic risk for sleep apnea causally linked with glaucoma susceptibility? Invest Ophthalmol Vis Sci. 2022;63(1):25. doi:10.1167/iovs.63.1.25
51. Sanderson E, Davey Smith G, Windmeijer F, Bowden J. An examination of multivariable Mendelian randomization in the single-sample and two-sample summary data settings. Int J Epidemiol. 2019;48(3):713–727. doi:10.1093/ije/dyy262
52. Jonas JB, Wei WB, Xu L, Wang YX, Liu G-S. Systemic inflammation and eye diseases. The Beijing Eye Study. PLoS One. 2018;13(10):e0204263. doi:10.1371/journal.pone.0204263
53. Tang B, Li S, Han J, Cao W, Sun X. Associations between blood cell profiles and primary open-angle glaucoma: a retrospective case-control study. Ophthalmic Res. 2020;63(4):413–422. doi:10.1159/000504450
54. Kondkar AA, Sultan T, Almobarak FA, et al. Association of increased levels of plasma tumor necrosis factor alpha with primary open-angle glaucoma. Clin Ophthalmol. 2018;12:701–706. doi:10.2147/OPTH.S162999
55. Chaitanya A, Pai VH, Mohapatra AK, Ve RS. Glaucoma and its association with obstructive sleep apnea: a narrative review. Oman J Ophthalmol. 2016;9(3):125–134. doi:10.4103/0974-620X.192261
56. Yamazaki Y, Drance SM. The relationship between progression of visual field defects and retrobulbar circulation in patients with glaucoma. Am J Ophthalmol. 1997;124(3):287–295. doi:10.1016/S0002-9394(14)70820-7
57. Wan Y, Lv M, Zhou K, et al. Mood disorders are correlated with autonomic nervous function in chronic insomnia patients with OSA. Nat Sci Sleep. 2023;15:511–522. doi:10.2147/NSS.S396773
58. Jones RT, Benowitz NL, Herning RI. Clinical relevance of cannabis tolerance and dependence. J Clin Pharmacol. 1981;21:143S–152S.
59. Karakucuk S, Goktas S, Aksu M, et al. Ocular blood flow in patients with obstructive sleep apnea syndrome (OSAS). Graefes Arch Clin Exp Ophthalmol. 2008;246(1):129–134. doi:10.1007/s00417-007-0656-8
60. Vera J, Redondo B, Alvarez-Rodriguez M, Molina R, Jimenez R. The intraocular pressure responses to oral academic examination: the influence of perceived levels of public speaking anxiety. Appl Ergon. 2020;88:103158. doi:10.1016/j.apergo.2020.103158
61. Abe RY, Silva TC, Dantas I, et al. Can psychologic stress elevate intraocular pressure in healthy individuals? Ophthalmol Glaucoma. 2020;3(6):426–433. doi:10.1016/j.ogla.2020.06.011
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.