")
Back to Journals » Nature and Science of Sleep » Volume 15
Impact of Sleep Profiles on Multimorbidity Among US Active-Duty Service Members in the 2018 Health-Related Behaviors Survey
Authors Weinberger M , Ahmed AE , Singer DE
Received 7 September 2023
Accepted for publication 23 November 2023
Published 5 December 2023 Volume 2023:15 Pages 1019—1032
DOI https://doi.org/10.2147/NSS.S434813
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Marina Weinberger,1 Anwar E Ahmed,1,2 Darrell E Singer1,2
1School of Medicine, Uniformed Services University of the Health Sciences, Bethesda, MD, USA; 2Department of Preventive Medicine and Biostatistics, Uniformed Services University of the Health Sciences, Bethesda, MD, USA
Correspondence: Anwar E Ahmed, Email [email protected]
Purpose: Sleep is a modifiable factor affecting chronic diseases and conditions in the Active-Duty (AD) United States (US) military population. This study assesses the impact of reported sleep health behaviors and sleep profiles on reported multimorbidity in active-duty service members (ADSMs).
Participants and methods: The study used a military representative sample of 17,166 active duty SMs from the 2018 Department of Defense Health Related Behaviors Survey (HRBS) to explore sleep patterns and profiles, and medical conditions. Multimorbidity was defined as the presence of two or more medical conditions which we limited to include obesity, hypertension, and hyperlipidemia. The adjusted odds ratios for six sleep-related health behaviors and their unobservable sleep profiles were calculated using a weighted multinomial logistic model.
Results: Sleep-related health behaviors were associated with increased odds of obesity, hypertension, and hyperlipidemia. We found higher odds of reported multimorbidity in SMs who reported lack of energy due to poor sleep (adjusted odds ratio [aOR] = 2.35, 95% CI:1.88– 2.93), sleep 6 hours or less per night (aOR = 1.95, 95% CI:1.53– 2.50), trouble sleeping (aOR = 2.19, 95% CI:1.76– 2.72), and use of sleep medications (aOR = 2.10, 95% CI:1.64– 2.68). Latent class analysis (LCA) identified three unobservable sleep profiles in SMs: minimal or low-risk sleep patterns (37.43%), moderate-risk sleep patterns (31.11%), and high-risk sleep patterns (31.46%). SMs with high-risk sleep patterns were significantly associated with reported multimorbidity (adjusted odds ratio [aOR] = 3.54, 95% CI:2.75– 4.56).
Conclusion: We found a strong association between sleep-related health behaviors and their unobservable sleep profiles with multimorbidity in this AD population. Future studies should investigate whether other chronic diseases may be influenced by sleep impairment in the US military population.
Keywords: sleep, multimorbidity, hypertension, obesity, hyperlipidemia, military
Introduction
Poor sleep quality and quantity is a prevalent issue within the general population of the United States (US). According to Healthy People 2020 (HP2020), 1 in 3 adults do not get enough sleep, defined as at least 7 hours of sleep over a 24-hour period for adults 22 and over, or at least 8 hours for adults ages 18–21.1 Sleep serves a vital role in maintaining healthy mental, physical, and metabolic states.2 The inability to achieve seven hours of sleep regularly is closely associated with and predictive of the presence of chronic diseases and adverse health outcomes, including metabolic weight gain and obesity, hypertension, hyperlipidemia and depression.2–6 The military is a healthier population as compared to the general US population; paradoxically, the military appears to have higher levels of sleep problems with almost 50% of personnel reporting poor sleep quality.7
The US military is a small but significant component of the general US population. The military is highly active, with most personnel rotating through one of three segments of the military lifecycle: 1) recovery and refit, 2) training and preparation to deploy, or 3) ready for deployment, or deployed.8 Preparation and development of combat-ready forces include accession and retention standards, individual and unit training programs, fitness and warfighter testing.9–12 Military operations, whether training or “real-world”, eg, conflict or combat, are physically, mentally, emotionally, and psychologically demanding. Missions are conducted 24 hours daily; off-duty time is minimal, and if any is typically spent conducting personal hygiene, eating, or sleeping in austere conditions that are inherently not conducive to quality sleep or maintaining sleep hygiene. The level of stress on active-duty service members (ADSMs) rises significantly during conflict and combat actions and compounds the risk of illness, injury, and death. Most significantly, training exercises have an end-of-exercise point, or “END-EX”, followed by an expected refit and recovery period. The endpoints of conflict and combat operations are far less certain.13 Since 9/11, the number and length of deployments have disrupted the cycle of phases resulting in inadequate recovery periods, which include periods of restorative sleep—and has contributed directly to the degraded metabolic, cardiovascular, skeletomuscular, and cognitive health of ADSMs.14
Studies have documented pronounced levels of insomnia and sleep disorders among ADSMs. Surveillance data from 2000–2009 reveals a crude overall incident rate of 48.4 diagnoses of insomnia per 10,000 person-years, starting at 7.2 per 10,000 in 2000 and rising to 135.8 per 10,000 in 2009.15 A Millennium Cohort study of ADSMs slept 7 hours or less during the period 2001–2008. Those sleeping less than 6 hours per day were more likely to have received an early discharge from service (HR 1.3 [1.10–1.55]) and were also associated with lower self-rated health (HR 0.74, [0.69–0.75]).16 In 2022, a prospective cohort study of over 300 ADSMs from all four services reported 32.7% of participants were diagnosed with insomnia, 30.4% with obstructive sleep apnea, and 36.9% with both.13
Parallel to the general US population is the rise of overweight, obesity, and hypertension among military servicemembers. The military provides a unique population within the US of individuals who are required to undergo annual health screenings as part of their service requirement, and thus these chronic conditions may be more likely to be identified than in the civilian population, whose frequency of healthcare interactions varies considerably more. A study of ADSMs published in 2015 described an increase in the combined rate of overweight and obesity (BMI ≥ 25), from 50.6% in 1995 to 60.8%, likely secondary to a rise in obesity (BMI ≥ 30) from 5.0% in 1995 to 12.7% in 2008.17 Surveillance data demonstrates the percentage of obesity (BMI ≥ 30) among ADSMs of all services was 16.1% in 2018, rising to 18.8% in 2021.18
Investigations are limited into the association of sleep behaviors or sleep profiles of ADSMs and multimorbidity, defined as two or more medical conditions existing simultaneously but independently with each other.19 Studies of sleep and other comorbid conditions within the military community primarily include servicemembers who have deployed or former military (veterans and retirees), and those referred for care of their comorbid sleep conditions (eg, insomnia, obstructive sleep apnea, disturbances).7,20–23 This study aimed to assess whether an association exists within a sample of ADSMs between sleep behaviors, their unobservable sleep profiles, and reported multimorbidity, which we defined as two or more medical conditions (hypertension, hyperlipidemia, or obesity).
Methods
Data Source
The Department of Defense Survey of Health-Related Behaviors (HRBS) is a cross-sectional instrument used to collect information and support estimates of health problems, factors associated with those problems, and risk behaviors among military servicemembers. The survey was first conducted in 1980 and approximately every three years since to support trend analysis and progress toward DOD and national health goals.24 This study analyzed data from the 2018 Health Related Behaviors Survey (HRBS), in which data on chronic conditions and sleep habits questions were collected along with other health behavior information.25 The survey was administered online and was confidential but not anonymous. The survey was administered until representation of groups within the military was achieved. In addition to the 2018 HRBS, survey data from the 2011 and 2015 HRBSs were also used to examine whether the prevalence of obesity, hyperlipidemia, and hypertension changed with the daily average hours of sleep per night in each survey.
Study Sample
The study population included 1,357,219 eligible ADSMs in the US military from different service branches: Army, Navy, Air Force, Marine Corps, and Coast Guard. Email surveys were randomly sent to 199,996 ADSMs, of which 17,166 usable surveys were returned. The overall weighted response rate was 9.6%. Weighting was performed by the 2018 HRBS in two phases. First, design weights were estimated to counteract the slight oversampling of some groups (eg, Marines, women, junior enlisted personnel). Second, nonresponse weights were calculated to make the data representative of those who were selected for sampling. The final weights were the product of the design and nonresponse weights, which make the final sample representative of the US military population. The weighting procedures and response rate are described in further detail elsewhere.25 This study has been reviewed and approved by the Uniformed Services University of the Health Sciences (USUHS) Institutional Review Board.
Sleep-Related Health Behaviors
Lack of Energy
Sleep habits were measured using the following item: “In the past week, how much were you bothered by lack of energy because of poor sleep?” Four response options were included: 1= not bothered at all, 2= slightly, 3= moderately bothered, and 4= severely bothered. We collapsed categories 3 and 4 to create moderate to severe lack of energy due to poor sleep where respondents were assigned a “yes” (moderate or severe), and other respondents were assigned a “no” (not bothered at all or slightly).
Sleep Quantity and Quality
Respondents were asked, “On average, over the PAST 30 DAYS, how many hours of actual sleep do you get in a 24-hour period?”. We created two categories to represent if the daily average amount of sleep was below the recommended amount (6hrs or less) (yes/no): ≤ 4 hours and 5–6 hours (yes) versus ≥ 7 hours per night (no). Respondents were asked, “During the PAST 30 DAYS, how would you rate your overall sleep quality?” Four response options were included: 1= very good, 2= fairly good, 3= fairly bad, and 4= very bad. We defined bad sleep quality by collapsing categories 1 and 2 (no) versus 3 and 4 (yes) to create two groups: 1= very good, 2= fairly good (no) versus 3= fairly bad, and 4= very bad (yes). Respondents were asked “During the PAST 30 DAYS, how much have you been bothered by any of the following problems? Trouble sleeping?” The response options were categorized into two levels yes/no: 1= not bothered at all (no) versus 2= bothered a little bit and 3= bothered a lot (yes).
Energy Drinks
Respondents were asked “During the PAST 30 DAYS, how often did you use the following TO HELP YOU STAY AWAKE? Energy drinks (eg, Monster, Red Bull, Rockstar, 5-Hour-Energy)?” Five response options were included: 1= never during the past 30 days, 2= less than once a week, 3= once or twice a week, 4= three or more times a week, and 5= daily. Two response options were created: 1= never during the past 30 days (no) versus 2= 1–2 times per week and 3= 3–7 times per week (yes).
Prescription Sleep Medications
Respondents were asked, “During the PAST 30 DAYS, how often did you take prescription or over-The-counter (OTC) medications TO HELP YOU SLEEP?” Four response options were included: 1= never during the past 30 days, 2= less than once a week, 3= once or twice a week, 4= three or more times a week, and 5= daily. Two response options were created: 1= never during the past 30 days (no) versus 2 =1-2 times per week and 3= 3–7 times per week (yes).
Outcome
In this study, we examined the relationship between sleep habits and three medical conditions: obesity, hypertension, and hyperlipidemia. Respondents were asked, “In the PAST 12 MONTHS has a doctor or other health professional told you that you had high blood pressure.” The response options were “yes” or “no”. Respondents were asked “In the PAST 12 MONTHS has a doctor or other health professional told you that you had high cholesterol.” The response options were “yes” or “no”. Body mass index (BMI) calculations were provided within the HRBS dataset and were calculated from the servicemember’s reported height and weight. BMI was calculated according to the standard Centers for Disease Control and Prevention (CDC) formula: weight in kilograms [kg] divided by height in meters squared [m2]. The CDC criteria for weight classification was used: underweight was classified as BMI less than 18.5 kg/m2, normal weight was BMI 18.5–24.9 kg/m2, overweight was BMI 25.0–29.9 kg/m2, and obese was BMI 30 or more kg/m2. The response options were “yes” or “no”. We created one multinominal dependent variable with five mutually exclusive categories to assess the sleep habits associated with each category: 1) obesity only 2) hyperlipidemia only, 3) hypertension only, and 4) the presence of two or more medical conditions (multimorbidity) as compared to the reference category, 0) No morbid conditions.
Control Variables
We assessed the association between sleep health behaviors and sleep profiles (defined by latent class analysis (LCA)) and reported multimorbidity before and after controlling for demographic factors, military characteristics, and socioeconomic indicators. Demographic variables included sex (male/female), race and ethnicity (non-Hispanic white/non-Hispanic black/Hispanic/non-Hispanic Asian/other), age groups (17-24/25-34/35-44/45+), marital status (married/cohabiting/never married/separated, divorced, or widowed), dependent children (yes/no). We included military characteristics and socioeconomic indicators such as service branch (Air Force/Army/Navy/Marine Corps/Coast Guard), pay grade (enlisted/officer), and education (high school or less, some college, Bachelor’s degree, or more).
Statistical Analysis
Statistical analysis was conducted using complex sample procedures such as PROC SURVEYFREQ and SURVEYLOGISTIC in SAS (SAS version 9.4, SAS Institute, Cary, NC). The analysis utilized sampling weights to account for selection bias and nonresponse. Overall weighted percentages were presented in Table 1. Two-way table associations between medical conditions and sleep habits were tested using the Rao-Scott chi-square test (Table 2). We examined the trend and the association between sleep duration (hours per night) and reported multimorbidity in 2011, 2015, and 2018 HRBS data (Figure 1). For each sleep habit (Table 3), weighted multinomial logistic regression analysis was performed to estimate the adjusted odds ratio of “obesity only”, “hyperlipidemia only”, “hypertension only”, and “multimorbidity” compared to no medical condition, adjusting for sociodemographic covariates. An LCA was constructed in Mplus (Version 8.8) to cluster SMs into unobservable sleep profiles according to six sleep-related health behaviors (Figure 2). We assessed whether the prevalence of estimates of obesity, hyperlipidemia, hypertension, and multimorbidity change with the selected sleep profiles (Figure 3 and Table 2). We used Akeike Information Criterion (AIC) to select an optimal number of sleep profiles. The optimal sleep profiles solution was used as a predictor of obesity only, hyperlipidemia only, hypertension only, and multimorbidity compared to no medical condition, adjusting for demographic factors, military characteristics, and socioeconomic covariates in a weighted multinomial logistic regression (Table 3). In addition, a log-linear model was employed to enable comparison of the medical conditions rate across different sleep profiles (Table 4).
 |
Table 1 Sociodemographic Characteristics, Medical Conditions, Sleep Behaviors, and Profiles of the HRBS Population |
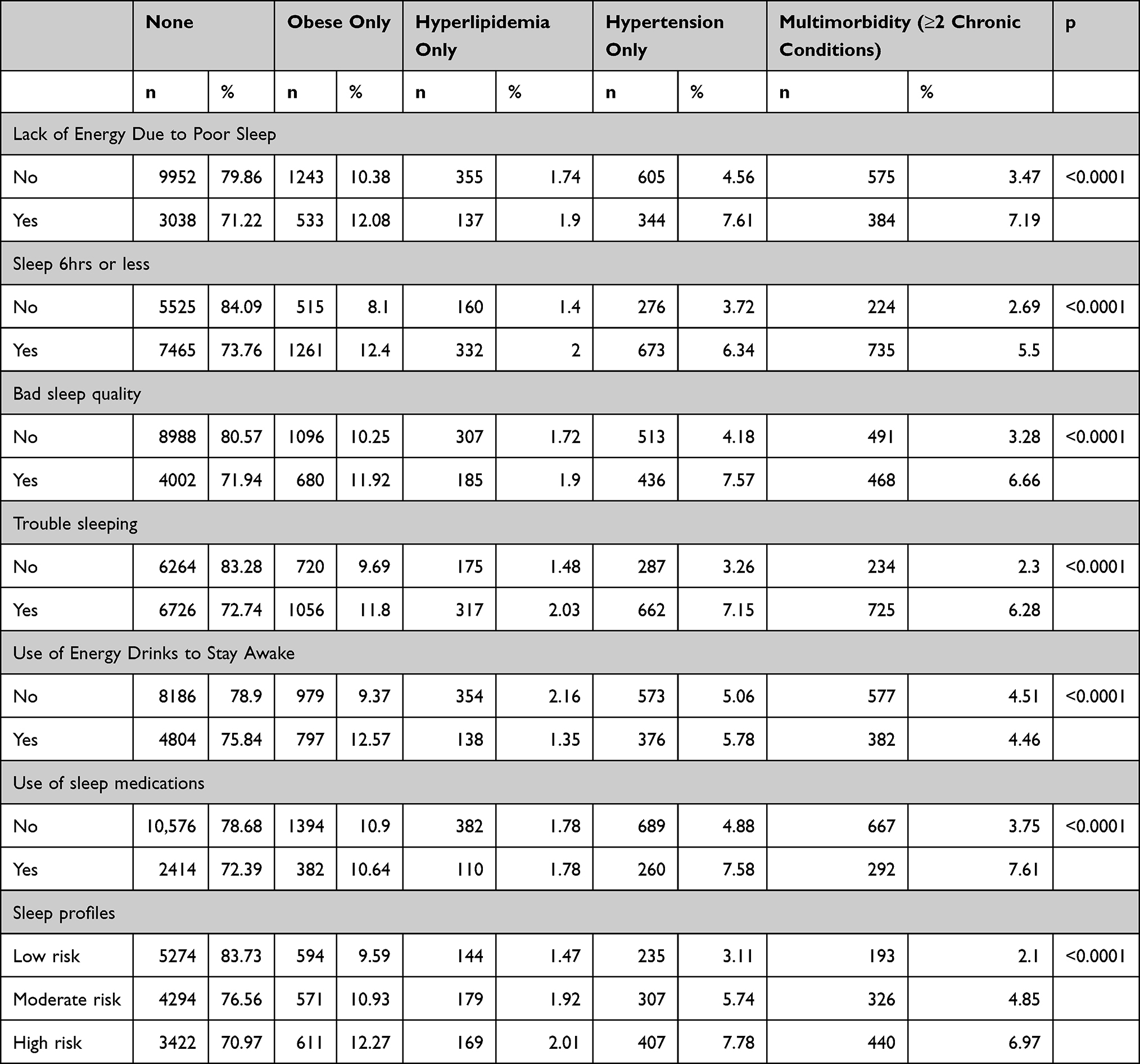 |
Table 2 Prevalence of Chronic Diseases and Multimorbidity by Sleep-Related Health Behaviors and Profiles |
 |
Table 3 Adjusted Odds Ratio of Obesity Only, Hyperlipidemia Only, Hypertension Only, and Multimorbidity Compared to No Medical Condition |
 |
Table 4 Medical Conditions Rate Across Different Sleep Profiles |
 |
Figure 1 The trend and the association between sleep duration (hours per night) with prevalence (%) of multimorbidity: 2011, 2015, and 2018 HRBS. Sleeping ≤ 6 hours per night is associated with higher prevalences of multimorbidity in 2011, 2015, and 2018 HRBS. |
 |
Figure 2 Latent class analysis (LCA) identified three unobservable sleep profiles in ADSMs: minimal or low-risk sleep patterns (37.43%), moderate-risk sleep patterns (31.11%), and high-risk sleep patterns (31.46%). |
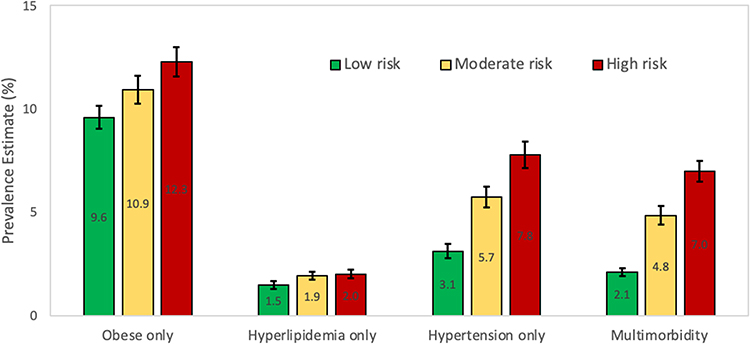 |
Figure 3 Compared to the minimal or low-risk sleep patterns group, the high-risk sleep patterns group had significantly greater prevalence estimates (%) of chronic conditions. |
Results
Among the 17,166 ADSMs, the 12-month prevalence estimates included the following: obesity only 10.85% (95% CI: 10.12–11.58%), hyperlipidemia only 1.78% (95% CI: 1.56–2.00%), hypertension only 5.40% (95% CI: 4.84–5.96%), and multimorbidity 4.49% (95% CI: 4.06–4.92%), Table 1. The prevalence of multimorbidity was significantly changed with sleep-related health behaviors (p-value <0.0001, Table 2). For instance, sleeping six hours or less a night significantly increases the prevalence of multimorbidity (5.50% vs 2.69%). Figure 1 shows servicemembers who reported sleeping ≤ 6 hours per night had a higher prevalence of multimorbidity than those who reported sleeping ≥ 7 hours per night.
Three unobservable sleep profiles were identified among participants by LCA and labeled minimal or low-risk sleep patterns (37.43%), moderate-risk sleep patterns (31.11%), and high-risk sleep patterns (31.46%). The three-profile solution was found to fit the data better than the two-profile solution (AIC: 114,068.653 vs 114,612.149, respectively). Figure 2 shows the estimated individual probability of sleep profiles. The prevalence of multimorbidity decreased significantly from 6.97% for SMs with high-risk sleep patterns to 2.69% for SMs with low-risk sleep patterns (Figure 3 and Table 2).
Controlling for demographic factors, military characteristics, and socioeconomic covariates (Table 3), ADSMs who reported lack of energy due to poor sleep were more likely to have obesity (OR=1.30, 95% CI: 1.09–1.55), hyperlipidemia (OR=1.38,95% CI: 1.03–1.85), hypertension (OR=1.87,95% CI: 1.47–2.39), and multimorbidity (OR=2.35,95% CI: 1.88–2.93). Short sleep duration (≤ 6 hours per night) was associated with increased odds of obesity (OR=1.57,95% CI:1.32–1.87), hyperlipidemia (OR=1.58,95% CI: 1.22–2.04), hypertension (OR=1.75,95% CI:1.38–2.22), and multimorbidity (OR=1.95,95% CI:1.53–2.50).
ADSMs who rated their overall sleep quality as bad were associated with increased odds of obesity (OR=1.27, 95% CI: 1.07–1.50), hyperlipidemia (OR=1.40,95% CI: 1.07–1.83), hypertension (OR=1.95, 95% CI: 1.56–2.45), and multimorbidity (OR=2.19,95% CI: 1.76–2.72). In contrast, ADSMs who rated their sleep as very bad were associated with increased odds of hypertension (OR=2.13, 95% CI: 1.42–3.20) and multimorbidity (OR=2.17,95% CI: 1.53–3.07).
ADSMs who reported being bothered by their sleep were associated with an increased risk of obesity (OR=1.35,95% CI: 1.15–1.58), hyperlipidemia (OR=1.53,95% CI: 1.15–2.03), hypertension (OR=2.41,95% CI: 1.89–3.08), and multimorbidity (OR=2.78,95% CI: 2.21–3.51).
The use of energy drinks to help stay awake (OR=1.46, 95% CI: 1.24–1.72) was associated with increased odds of obesity. Using sleep medications to help with sleep was associated with increased odds of hypertension (OR=1.71,95% CI: 1.32–2.21) and multimorbidity (OR=2.10,95% CI: 1.64–2.68).
As compared to ADSMs with low-risk sleep patterns (reference), ADSMs with high-risk sleep patterns were associated with increased odds of risk of obesity (OR=1.45, 95% CI: 1.19–1.76), hyperlipidemia (OR=1.74, 95% CI: 1.22–2.47), hypertension (OR=2.79, 95% CI: 2.08–3.74), and multimorbidity (OR=3.54, 95% CI: 2.75–4.56).
When compared to ADSMs with low-risk sleep patterns (reference), ADSMs with moderate and high-risk sleep patterns had significantly higher rates of obesity (rate ratio (RR) =1.75, 95% CI: 1.58–1.95), RR=1.28, 95% CI: 1.15–1.42, respectively), hypertension (RR=2.84, 95% CI: 2.51–3.23, RR=1.74, 95% CI: 1.52–1.99, respectively), hyperlipidemia (RR=2.25, 95% CI: 1.92–2.63, RR=1.71, 95% CI: 1.45–2.01, respectively).
Discussion
Of the 17,166 participants, nearly one quarter reported having at least one chronic disease (obesity 14.3%, hyperlipidemia 4.2%, or hypertension 9.1%), and 4.49% reported having two or greater chronic diseases (multimorbidity). Insufficient sleep is also regrettably common in this sample, with approximately two-thirds (64%) of participants reporting sleeping fewer than seven hours within a 24-hour period. The presence of reported multimorbidity was significantly higher among those sleeping six hours or less a night than those who reported sleeping ≥ 7 hours per night (5.50% vs 2.69%).
We were able to identify homogeneous unobservable clusters of ADSMs, each with a different sleep risk profile: minimal or low-risk sleep patterns, moderate-risk sleep patterns, and high-risk sleep patterns. In this study, we noted a significant effect in the prevalence of reported multimorbidity in SMs who clustered in the high-risk sleep pattern group. The effects of unobservable sleep profiles on multimorbidity or medical conditions have not been defined in the AD population. The American Academy of Sleep Medicine released its 2015 Consensus Statement endorsing 7–9 hours of sleep per night as the necessary amount for optimal health- and found that individuals with < 7 hours were more likely to score poor health-related quality of life measures,26 though there have since been no guidelines released regarding sleep evaluation screening for high-risk populations.
We also observed a strong association with multimorbidity as sleep amount decreased: higher odds of multimorbidity were found in ADSMs averaging ≤ 6 hours of sleep. This study used various independent surveys to confirm this association. Figure 1 demonstrates a stepwise relationship in which the prevalence of multimorbidity was significantly increased in the 5–6 hours of sleep group compared to ≥ 7 hours of sleep, and the ≤ 4 hours of sleep group had significantly higher multimorbidity prevalence than the 5–6 hours of sleep group. This suggests that the cumulative amount of sleep, up to the recommended 7 hours, is significantly correlated with the presence of multimorbidity. This same pattern was observed across data provided from the 2011 and 2015 HRBS as well (Figure 1), strengthening the validity of this observation.
Previous studies that have investigated multimorbidity and sleep have done so in older populations—but with similar observations to the present study (eg, significantly higher rates of multimorbidity in groups that reported short sleep).27,28 Interestingly, one study found positive associations between sleep disturbance and neuropsychiatric and musculoskeletal disease, but not with cardiovascular disease28—a finding that contradicts our observations concerning hypertension and hyperlipidemia. However, this inconsistency could be due to the different age populations involved in each study.
When examining the association of sleep duration with each chronic disease individually, we observed the single strongest effect to be with hypertension (Figure 3). An association of sleep impairment with hypertension has been well-documented in the literature,3,4,6 with even one night of sleep restriction to ≤4 hours resulting in a 6 mmHg increase in mean systolic blood pressure.3 Strong evidence for this relationship includes a meta-analysis of 11 studies that found short sleep duration (either <5 or <6 hours per night) was associated with a significantly increased incidence of hypertension.4 This effect is not only documented in the civilian population: a study using data from the 2011 HRBS found that ADSMs with short sleep duration (<5 hours) had greater than double the odds of having hypertension29—a statistic that remains true for our analysis of the more recent 2018 HRBS data.
Chronic short sleep duration has also been linked to metabolic disease, potentially increasing the prevalence of obesity and diabetes through alterations in glucose metabolism, increased appetite, and decreased energy expenditure.5 It should also be noted that the effect seen by the use of energy drinks to stay awake might be related not only to sleep impairment—but also to the sugar and caffeine content of the drink itself, both of which have been shown to contribute to weight gain.30 Hyperlipidemia has demonstrated fewer clear results in the literature regarding sleep impairment. A cohort study of more than 20,000 Chinese individuals found significantly elevated odds of hyperlipidemia among people sleeping >9 hours per night, but no statistically significant association with shortened sleep.31 However, a different cross-sectional study reported <5 hours of sleep per night resulting in 41% higher odds of having hyperlipidemia,32 a finding that our study would support.
Aside from sleep quantity, the HRBS data also enabled us to assess reported multimorbidity using qualitative measures of sleep health. The three qualitative survey items associated with the highest chance of having multimorbidity were (1) reporting being bothered a lot by sleeping, (2) use of sleep medications 3–7 times per week, and (3) having a lack of energy due to poor sleep (Figure 2). This suggests that the perceived negative impact of sleep hygiene on one’s lifestyle, rather than the quantity of sleep alone, may be a correlated to the development of chronic disease. Additionally, we found that reporting very good sleep quality was a protective factor, with decreased odds of obesity, hypertension, and multimorbidity. Together, these findings indicate that perception of sleep quality goes both ways: positive perception is associated with decreased disease burden while negative perception is associated with increased disease burden. This is not to say that these sleep related health behaviors directly cause chronic disease. Rather, there is likely an association present in susceptible individuals who exhibit certain lifestyle behaviors such as poor diet and exercise, which may result in both unhealthy sleep behaviors and chronic disease.
Strengths and Limitations
This study’s conclusions are supported by the strengths of the 2018 HRBS study design. The HRBS provides the most recent data available to researchers to investigate health-related behaviors in current military AD populations—a group that largely turns over every 4 years. It draws from a very large pool of participants and uses a cross-sectional design, which enables the comparison of multiple variables. Furthermore, previous studies investigating this topic have been limited to either only using the quantity of sleep as their independent variable32—or assessing sleep quality in a narrow manner (eg, good vs poor).31 In contrast, the HRBS data provides a more detailed representation of sleep quality through its survey questions.
However, the study design of the HRBS also presents limitations. The cross-sectional nature of the HRBS prevents causal relationships from being inferred. However, our variables were intentionally selected based upon preexisting hypothesized relationships in the literature between poor sleep and each of the chronic diseases we evaluated.3–6,26 This lends more plausibility to the associations that we identified. Additionally, the response rate of the HRBS (8.6% unweighted) is considered relatively low for survey research,25 which could increase the probability of there being selection bias. However, the HRBS data was weighted as previously described in order to mitigate any significant selection bias and to achieve reasonable demographic representation of the general military population.2–6 There may additionally be a small amount of recall bias due to the nature of the HRBS being a survey that relies on self-reported data. Social desirability bias is also a concern—particularly with military populations who may tend to highly value conformity with fellow ADSMs.
The bounds of our investigation were limited by the information collected by the HRBS. For instance, ADSMs were not asked about whether they have obstructive sleep apnea (OSA), a condition which is becoming unfortunately prevalent among young adults. One study found that the prevalence of OSA is 14.9% among young adult females and 26.9% of young adult males aged 22 years.33 Collecting this information from ADSMs would provide a link between unhealthy sleep behaviors and chronic disease, and we encourage the study designers to consider including this data in future iterations of the study. Another limitation of this study is that we lack the data to compare our findings with individuals who have long sleep (>8 hours per night). Substantial evidence exists supporting an association between long sleep and increased morbidity and mortality.34 According to the 2018 HRBS, 33% of ADSMs met the recommended 8 hours of sleep per night, but this data did not specify how many ADSMs averaged >8 hours per night. While short sleep is certainly a more widespread issue in the Armed Forces than long sleep, being able to compare these two conditions could help further characterize the impact of short sleep on multimorbidity, should this data be collected in future iterations of the HRBS.
Lastly, the comparison of data used in this study with previous years of HRBS is limited by the methodologic differences in each year’s survey. Similar data were collected via slightly differently worded questions each year. Therefore, we were unable to extrapolate trends by directly comparing the 2011, 2015, and 2018 HRBS data.
Conclusions and Future Directions
In conclusion, we found significant associations between reports of sleep impairment and reported multimorbidity of chronic disease in the active-duty US military population. These associations are particularly important to characterize in the military population, given the large gap that exists between military and civilians in terms of meeting HP2030 sleep health targets. The record of studies examining sleep disorders and conditions among the military and veteran community is voluminous; however, a large subset focuses on post-deployment ADSMs, former military (veterans and retirees), and comorbid sleep disorders and conditions (eg, insomnia, obstructive sleep apnea, disturbances).20 While many studies have examined the question of short sleep on individual chronic diseases, few have attempted to characterize an association with multimorbidity of common chronic diseases, with the present study offering some insight into these problems for active-duty military servicemembers. We found strong evidence of associations between sleep-related health behaviors and their unobservable sleep profiles with multimorbidity in this population.
The US military is a small but strategic component of the US population and requires a healthy force for optimal battlefield performance. Over the past two decades, the near-continuous deployments and operations where sleep is often not attained or neglected may have negatively affected force readiness. Accession standards infer that recruits are within acceptable weight standards (not overweight) and free of chronic disease. Remaining in the military requires adherence to retention standards and members are still able to fulfill their job requirements; our data reaffirms the presence of chronic disease and overweight/obesity within the force and their association with poor sleep quality.
Future studies should be directed at better characterizing the effects observed in the present study, including prospective studies to more closely study the temporality of sleep quality with the development of chronic disease, expanding the definition of multimorbidity to include other types of chronic disease, comparing multimorbidity in short sleep to long sleep, and exploring whether there is a causal relationship between sleep health and chronic disease.
Data Sharing Statement
The data that support the findings of this study are available from the Defense Health Agency but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available.
Ethics Approval and Consent to Participate
This is a secondary analysis of existing de-identified data from the Defense Health Agency (DHA), the requirement for consent was waived by the Institutional Review Board (IRB) of the Uniformed Services University of the Health Sciences.
Acknowledgments
This work was prepared as part of the author’s official duties. Title 17, U.S.C., §105 provides that copyright protection under this title is not available for any work of the U.S. Government. Title 17, U.S.C., §101 defines a U.S. Government work as a work prepared by a military Service member or employee of the U.S. Government as part of that person’s official duties.
The 2018 DoD Health Related Behaviors Survey (HRBS) is the result of a collaboration between the Defense Health Agency and RAND. The authors thank the service members in the Air Force, Army, Marine Corps, Navy, and Coast Guard who contributed to this survey.
The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Uniformed Services University of the Health Sciences, Department of Defense, nor the U.S. Government.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Increase the proportion of adults who get enough sleep — SH-03. Healthy People 2030. Available from: https://health.gov/healthypeople/objectives-and-data/browse-objectives/sleep/increase-proportion-adults-who-get-enough-sleep-sh-03/data.
2. Watson NF, Badr MS, Belenky G, et al.; Consensus Conference Panel. Joint Consensus Statement of the American Academy of Sleep Medicine and Sleep Research Society on the Recommended Amount of Sleep for a Healthy Adult: methodology and Discussion. Sleep. 2015;38(8):1161–1183. doi:10.5665/sleep.4886
3. Tochikubo O, Ikeda A, Miyajima E, Ishii M. Effects of insufficient sleep on blood pressure monitored by a new multibiomedical recorder. Hypertens Dallas Tex. 1996;27(6):1318–1324. doi:10.1161/01.hyp.27.6.1318
4. Meng L, Zheng Y, Hui R. The relationship of sleep duration and insomnia to risk of hypertension incidence: a meta-analysis of prospective cohort studies. Hypertens Res. 2013;36(11):985–995. doi:10.1038/hr.2013.70
5. Knutson KL, Spiegel K, Penev P, Van Cauter E. The metabolic consequences of sleep deprivation. Sleep Med Rev. 2007;11(3):163–178. doi:10.1016/j.smrv.2007.01.002
6. Gottlieb DJ, Redline S, Nieto FJ, et al. Association of usual sleep duration with hypertension: the Sleep Heart Health Study. Sleep. 2006;29(8):1009–1014. doi:10.1093/sleep/29.8.1009
7. Troxel WM, Shih RA, Pedersen ER, et al. Sleep in the Military: promoting Healthy Sleep Among U.S. Servicemembers. Rand Health Q. 2015;5(2):19.
8. Flynn C. Challenges at many levels: holistic view of readiness allows Army to meet new demands; 2020. Available from: https://www.army.mil/article/233273/challenges_at_many_levels_holistic_view_of_readiness_allows_army_to_meet_new_demands.
9. Chronic Diseases and Military Readiness. Natl Cent Chronic Dis Prev Health Promot; 2022. Available from: https://www.cdc.gov/chronicdisease/resources/publications/factsheets/military-readiness.htm.
10. Physical Activity and Military Readiness. Cent Dis Control Prev Div Nutr Phys Act Obes Natl Cent Chronic Dis Prev Health Promot; 2023. Available from: https://www.cdc.gov/physicalactivity/resources/physical-activity-military-readiness.html.
11. Dod Instruction 6130.03, Volume 1 Medical Standards For Military Service: appointment, Enlistment, Or Induction. Available from: https://www.esd.whs.mil/Portals/54/Documents/DD/issuances/dodi/613003_vol1.PDF?ver=7fhqacc0jGX_R9_1iexudA%3D%3D.
12. Dod Instruction 6130.03, Volume 2 Medical Standards For Military Service: retention. Available from: https://www.esd.whs.mil/Portals/54/Documents/DD/issuances/dodi/613003_vol02.PDF.
13. Mysliwiec V, Brock MS, Pruiksma KE, et al. A comprehensive evaluation of insomnia, obstructive sleep apnea and comorbid insomnia and obstructive sleep apnea in US military personnel. Sleep. 2022;45(12):zsac203. doi:10.1093/sleep/zsac203
14. Good CH, Brager AJ, Capaldi VF, Mysliwiec V. Sleep in the United States Military. Neuropsychopharmacol Off Publ Am Coll. Neuropsychopharmacol. 2020;45(1):176–191. doi:10.1038/s41386-019-0431-7
15. Armed Forces Health Surveillance Center. Insomnia, active component, U.S. armed forces, January 2000–December 2009. MSMR. 2010;17(5):12-15.
16. Seelig AD, Jacobson IG, Donoho CJ, Trone DW, Crum-Cianflone NF, Balkin TJ. Sleep and Health Resilience Metrics in a Large Military Cohort. Sleep. 2016;39(5):1111–1120. doi:10.5665/sleep.5766
17. Reyes-Guzman CM, Bray RM, Forman-Hoffman VL, Williams J. Overweight and obesity trends among active duty military personnel: a 13-year perspective. Am J Prev Med. 2015;48(2):145–153. doi:10.1016/j.amepre.2014.08.033
18. Stiegmann RA, Payne CB, Kiel MA, Stahlman SL. Increased Prevalence of Overweight and Obesity and Incidence of Prediabetes and Type 2 Diabetes During the COVID-19 Pandemic, Active Component Service Members, U.S. Armed Forces, 2018 to 2021. MSMR. 2023;30(1):11–18.
19. Jakovljević M, Ostojić L. Comorbidity and multimorbidity in medicine today: challenges and opportunities for bringing separated branches of medicine closer to each other. Psychiatr Danub. 2013;25(Suppl 1):18–28.
20. Saconi B, Polomano RC, Compton PC, McPhillips MV, Kuna ST, Sawyer AM. The influence of sleep disturbances and sleep disorders on pain outcomes among veterans: a systematic scoping review. Sleep Med Rev. 2021;56:101411. doi:10.1016/j.smrv.2020.101411
21. Alexander M, Ray MA, Hébert JR, et al. The National Veteran Sleep Disorder Study: descriptive Epidemiology and Secular Trends, 2000-2010. Sleep. 2016;39(7):1399–1410. doi:10.5665/sleep.5972
22. Capaldi VF, Guerrero ML, Killgore WDS. Sleep disruptions among returning combat veterans from Iraq and Afghanistan. Mil Med. 2011;176(8):879–888. doi:10.7205/milmed-d-10-00440
23. Collen J, Orr N, Lettieri CJ, Carter K, Holley AB. Sleep disturbances among soldiers with combat-related traumatic brain injury. Chest. 2012;142(3):622–630. doi:10.1378/chest.11-1603
24. Survey of Health-Related Behaviors. Available from: https://www.health.mil/Military-Health-Topics/Access-Cost-Quality-and-Safety/Health-Care-Program-Evaluation/Survey-of-Health-Related-Behaviors.
25. RAND Corporation. 2018 Department of Defense Health Related Behaviors Survey (HRBS): Results for the Active Component. RAND Corporation; 2021. doi:10.7249/RR4222
26. Watson NF, Badr MS, et al. Consensus Conference Panel. Joint Consensus Statement of the American Academy of Sleep Medicine and Sleep Research Society on the Recommended Amount of Sleep for a Healthy Adult: methodology and Discussion. J Clin Sleep Med. 2015;11(08):931–952. doi:10.5664/jcsm.4950
27. Nicholson K, Rodrigues R, Anderson KK, Wilk P, Guaiana G, Stranges S. Sleep behaviours and multimorbidity occurrence in middle-aged and older adults: findings from the Canadian Longitudinal Study on Aging (CLSA). Sleep Med. 2020;75:156–162. doi:10.1016/j.sleep.2020.07.002
28. Sindi S, Pérez LM, Vetrano DL, et al. Sleep disturbances and the speed of multimorbidity development in old age: results from a longitudinal population-based study. BMC Med. 2020;18(1):382. doi:10.1186/s12916-020-01846-w
29. Hruby A, Lieberman HR, Smith TJ. Self-reported health behaviors, including sleep, correlate with doctor-informed medical conditions: data from the 2011 Health Related Behaviors Survey of U.S. Active Duty Military Personnel. BMC Public Health. 2018;18(1):853. doi:10.1186/s12889-018-5781-2
30. Marks R. Energy Drinks: a Potentially Overlooked Obesity Correlate. Adv Obes Weight Manag Control. 2015;2(3):65. doi:10.15406/aowmc.2015.02.00019
31. Wang D, Chen J, Zhou Y, et al. Association between sleep duration, sleep quality and hyperlipidemia in middle-aged and older Chinese: the Dongfeng–Tongji Cohort Study. Eur J Prev Cardiol. 2019;26(12):1288–1297. doi:10.1177/2047487319843068
32. Grandner MA, Chakravorty S, Perlis ML, Oliver L, Gurubhagavatula I. Habitual sleep duration associated with self-reported and objectively determined cardiometabolic risk factors. Sleep Med. 2014;15(1):42–50. doi:10.1016/j.sleep.2013.09.012
33. McArdle N, Ward SV, Bucks RS, et al. The prevalence of common sleep disorders in young adults: a descriptive population-based study. Sleep. 2020;43(10):zsaa072. doi:10.1093/sleep/zsaa072
34. Kripke DF, Garfinkel L, Wingard DL, Klauber MR, Marler MR. Mortality associated with sleep duration and insomnia. Arch Gen Psychiatry. 2002;59(2):131–136. doi:10.1001/archpsyc.59.2.131
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.