")
Back to Journals » Clinical Interventions in Aging » Volume 17
How to Effectively Monitor Aging Patients with Chronic Hepatitis B: A Review
Authors Kang CK, Brennan PN , Dillon JF
Received 1 September 2022
Accepted for publication 17 November 2022
Published 9 December 2022 Volume 2022:17 Pages 1811—1820
DOI https://doi.org/10.2147/CIA.S366255
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Chan Keat Kang, Paul N Brennan, John F Dillon
Division of Molecular and Clinical Medicine, School of Medicine, Ninewells Hospital and Medical School, University of Dundee, Dundee, UK
Correspondence: John F Dillon, Email [email protected]
Abstract: Hepatitis B virus (HBV) infection is a major global public health challenge associated with significant morbidity and mortality. Due to worldwide population aging, HBV infection in the elderly will become increasingly prevalent. Effective universal vaccination programs exist but these are largely targeted towards the younger population. Therefore, the elderly population remains at risk of higher disease burden. New diagnoses of HBV infection in the elderly are usually asymptomatic chronic infections which increases their risk of developing cirrhosis, hepatocellular carcinoma, and liver disease-related mortality, especially if left untreated. Physiological changes and the increasing prevalence of multimorbidity associated with aging also potentially worsen outcomes in elderly patients with chronic HBV infection. Therefore, this cohort of patients should be monitored closely and effectively. Current international clinical practice guidelines unfortunately do not provide hard treatment endpoints specific to elderly patients with chronic HBV infection. Management of these patients is complex and requires an individualized approach. Multiple factors such as physiological changes, comorbidities, compliance, treatment tolerability and efficacy, burden of treatment, and realistic treatment goals need to be considered. Shared decision-making between patient and clinician is essential to ensure that the final decision for or against treatment aligns with the patient’s values and preferences. This review article aims to summarize the monitoring and management of chronic HBV infection in the aging population.
Keywords: chronic hepatitis B, aging, elderly, effective monitoring
Introduction
In 1965, Baruch Blumberg discovered the “Australia antigen” which was subsequently identified as the hepatitis B virus surface antigen (HBsAg).1 Hepatitis B virus (HBV) infection remains incurable and a major global public health challenge associated with significant morbidity and mortality.2,3
Although universal vaccination programs have been shown to be highly effective in reducing the prevalence and incidence of HBV infection, these programs are largely targeted towards the younger population.4 The older population, therefore, remains at risk of higher disease burden as the uptake of the vaccine is potentially lower and even if vaccinated, responses may be suboptimal due to changes in the immune system associated with the aging process.5,6 HBV infection in the elderly will become relatively more prevalent due to global population aging.7
This review article will summarize the monitoring and management of chronic HBV infection in the aging population. While this article is focussed on the monitoring of chronic HBV infection predominantly for the risk of progression to cirrhosis and the development of hepatocellular carcinoma (HCC), it should always be considered that the risk factors for acute HBV infection are relevant to older populations as well.
Background
Epidemiology
The World Health Organization estimates that 296 million people were living with chronic HBV infection in 2019, with 1.5 million new cases annually.8 Approximately 820,000 deaths may be attributed to HBV infection, predominantly due to cirrhosis and HCC.8 The burden of HBV infection varies widely across different regions of the world, with prevalence rates of >8% in sub-Saharan Africa and <2% in North America and Western Europe.9
Pathophysiology
HBV is a double-stranded DNA virus and a member of the hepadnavirus group. The virus particle or virion consists of an electron-dense icosahedral nucleocapsid composed of the core antigen (HBcAg).10 The nucleocapsid encloses the viral DNA and a DNA polymerase that has reverse transcriptase activity.10,11 Surrounding the nucleocapsid is the outer envelope of surface proteins (HBsAg) which are embedded in a lipid membrane derived from the host hepatocyte.10
Integration of the viral genome into the host genome is not required for viral replication and occurs randomly. However, it is one of the most crucial mechanisms of HBV-induced HCC by promoting genomic instability and can cause direct insertional mutagenesis, especially if into cancer-related genes in the host hepatocyte.12 HBV is not directly cytopathic in and of itself, cellular damage occurs through the host immunologic or inflammatory responses directed toward the infected hepatocytes. Consequently, long-term chronic hepatocyte inflammation and ineffective immune-mediated viral clearance contribute to the development of cirrhosis and HCC.13,14
Natural History
Although acute HBV infection is potentially fatal with its most extreme presentation of fulminant hepatic failure, most immunocompetent adults (>95%) will recover spontaneously and undergo HBsAg seroconversion without antiviral therapy.15,16 The majority of complications are associated with chronic HBV infection in those who do not seroconvert. Chronic HBV infection is defined as the presence of HBsAg positivity for ≥6 months.16 The risk of developing chronic HBV infection depends on the age at which the primary infection occurred. Chronic HBV infection occurs in approximately 90% of newborns infected perinatally, 30% of children aged under 5 years, and <5% of immunocompetent adults.17–19 Immunosuppressed individuals are also more susceptible to developing chronic HBV infection after the acute infection.20,21
Chronic HBV infection is a dynamic process and can be divided into different clinical phases based on immunological features, virology, biochemistry, and histology. Current clinical practice guidelines published by the European Association for the Study of the Liver (EASL), American Association for the Study of Liver Diseases (AASLD), and Asian-Pacific Association for the Study of the Liver (APASL) use different terminologies to describe these phases (Table 1).15,16,22 However they are broadly similar, it is important to recognize that this is not a linear process and patients can move back and forth between phases. For instance, approximately 20% of patients who achieve HBeAg (HBV e antigen) seroconversion will undergo seroreversion back to HBeAg positivity, usually associated with flares of hepatitis. Some patients (∼10–30%) may even skip Phase 3 altogether and progress directly from Phase 2 to Phase 4 after achieving HBeAg seroconversion.23
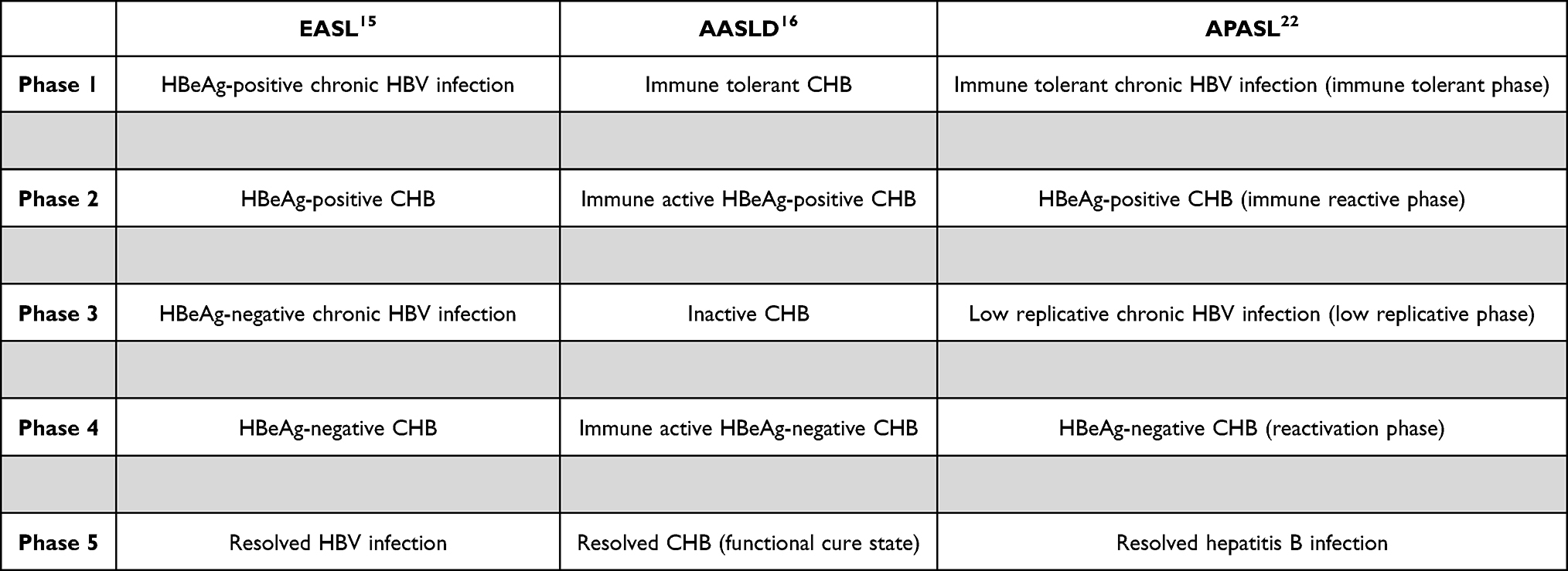 |
Table 1 Comparison of Terminology Used to Define the Natural History of Chronic Hepatitis B (CHB) |
Despite the distinct phases of chronic HBV infection described above, a single measurement of HBV replication markers (HBsAg, HBeAg, HBV DNA) and disease activity markers (alanine aminotransferase (ALT), fibrosis markers, liver biopsy) may not immediately allow classification to one of these phases. Serial monitoring of these biomarkers is often required.
Phase 1
Phase 1 is characterized by the presence of serum HBeAg, very high levels of HBV DNA (>107 IU/mL), and normal ALT (<40 IU/L, traditional upper limit of normal [ULN]). There is minimal or no liver necroinflammation or fibrosis.15 However, the process of hepatocarcinogenesis may have already commenced in this early phase of infection due to the detection of high levels of HBV DNA integration and clonal hepatocyte expansion.24 This phase is most commonly seen in patients infected with HBV perinatally due to its prolonged nature (may last > 30 years) and the likelihood of spontaneous HBeAg loss is very low in this phase. The risk of onward transmission is high due to the markedly elevated HBV DNA levels resulting in these patients being highly contagious.15
Phase 2
Phase 2 is characterized by the presence of serum HBeAg, high levels of HBV DNA (104–107 IU/mL), and elevated ALT (>40 IU/L). There is moderate or severe liver necroinflammation or fibrosis. This phase may occur several years after phase 1 and is more common in patients infected with HBV during adulthood. The outcome of this phase varies according to the degree of liver injury. Most patients will eventually achieve HBeAg seroconversion and HBV DNA suppression and enter the HBeAg-negative infection phase (phase 3). However, some may fail to do so and progress to the HBeAg-negative CHB phase (phase 4).15
Phase 3
Phase 3 is characterized by the absence of serum HBeAg, presence of serum antibodies to HBeAg (anti-HBe), undetectable or low HBV DNA (<2000 IU/mL), and normal ALT. Of note, some patients in this phase may have HBV DNA levels >2000 IU/mL but usually < 20,000 IU/mL and is accompanied by a persistently normal ALT with minimal or no liver necroinflammation or fibrosis. These patients have a favourable prognosis with a low risk of progression to cirrhosis if they remain in this phase. HBsAg loss with or without seroconversion may occur spontaneously in 1–3% of cases annually. Nevertheless, these patients remain at risk of progression to the HBeAg-negative CHB phase (phase 4) due to low level persistent viraemia.15
Phase 4
Phase 4 is characterized by the absence of serum HBeAg, presence of anti-HBe, moderate to high levels of HBV DNA (>2000 IU/mL), and intermittently or persistently elevated ALT. There is moderate or severe liver necroinflammation or fibrosis. This phase is associated with progression to cirrhosis and development of HCC with low rates of spontaneous disease remission.15
Phase 5
Phase 5 is characterized by the spontaneous loss of HBsAg, presence of antibodies to HBcAg (anti-HBc), with or without detectable antibodies to HBsAg (anti-HBs). ALT is normal and serum HBV DNA is usually undetectable. Risk of cirrhosis and HCC is minimal with an overall improved survival rate if loss of HBsAg occurs prior to the onset of cirrhosis. However if the loss of HBsAg occurs after cirrhosis has developed, the patient remains at risk of developing HCC and should undergo HCC surveillance. HBV reactivation may also occur in this phase in immunosuppressed individuals.15
Monitoring Chronic Hepatitis B in the Aging Population
There are three overlapping statuses or outcomes that require monitoring in CHB infection: activation of the virus, progression to cirrhosis, and surveillance for HCC. The risk of progression to cirrhosis or development of HCC also drives responses to any change in virus status in terms of initiation of treatment. It is worth considering how chronic HBV infections present in the elderly, may be those patients who have had a long-term diagnosis or a newly diagnosed chronic infection. New diagnoses of HBV infection in the elderly are much more likely to be asymptomatic chronic infections. These are usually detected from incidental findings of abnormal liver function tests or positive HBV screening prior to initiation of immunosuppressive medications.
Moreover, physiological changes associated with aging, increasing prevalence of multimorbidity, cumulative exposure to hepatotropic viruses and environmental hepatotoxins have the potential to worsen outcomes in elderly patients with chronic HBV infection.25 Elderly patients with chronic HBV infection are at real risk of HCC and liver disease-related mortality, especially if left untreated. The cumulative rates of HCC were found to be 6.5% and 15.6% at years 5 and 10, respectively. The cumulative rates of liver disease-related mortality were reported to be 3.3% and 12.3% at years 5 and 10, respectively.26 These results suggest that elderly patients with chronic HBV infection should be monitored closely and the ever-increasing burden of disease in this population should not be ignored or underestimated.
Assessment
At the initial visit, all patients with chronic HBV infection should have a thorough history taken and a systematic physical examination performed. In particular, clinicians should look for any signs of cirrhosis and should explore any risk factors for viral co-infection, alcohol misuse, metabolic syndrome, family history of HBV infection or HCC, and vaccination status.15,16 Blood samples, as detailed in Table 2 should be performed.
 |
Table 2 Initial Laboratory Investigations in Patients with Newly Diagnosed Chronic Hepatitis B |
The rationale for undertaking a detailed initial assessment for patients with chronic HBV infection is to determine the stage and severity of liver disease. This is because elderly patients with untreated CHB are at increased risk of HCC and liver disease-related mortality.26 This is essential to help stratify the group of patients who require antiviral therapy and HCC surveillance.
Monitoring of Hepatitis B Virus
This should be undertaken by measuring serology and HBV DNA at the frequency described in Figure 1, depending on viral phase, or if immunosuppressive therapies for other indications have been introduced. The results of the viral parameters in combination with results of monitoring for hepatic fibrosis may trigger the need for starting antiviral therapy.
 |
Figure 1 Algorithm for the monitoring of patients with chronic hepatitis B. |
Monitoring for Cirrhosis
Chronic HBV infection is a risk factor for developing cirrhosis and as described above, other risk factors for cirrhosis may also be present in individual patients. This monitoring is achieved by blood tests using indirect (eg FIB-4) or direct (eg ELF) methods, or by imaging-based modalities (eg Fibroscan), performed on an annual basis. Elevated results in any of these tests in the presence of active viral replication would be an indication to consider treatment. These measures of liver fibrosis are widely available, the choice of individual test is beyond the scope of this review and, in part, will be guided by local availability. Once cirrhosis has developed, the patient should be screened for oesophageal varices using endoscopy and entered into HCC surveillance.
Surveillance for Hepatocellular Carcinoma
Patients with chronic HBV infection are at increased risk of HCC and in those with additional cirrhosis, this risk is even higher. However, due to the aggressive curative treatment options available for HCC such as hepatic resection or liver transplantation, with transarterial chemoembolization usually only having palliative intent, HCC surveillance should only be undertaken in those fit enough to consider these treatments. In those with cirrhosis and chronic HBV infection, HCC surveillance with 6-monthly abdominal ultrasound and alpha-fetoprotein (AFP) should be offered to fit patients. In non-cirrhotic populations, several HCC risk scores have been developed and validated to identify CHB patients who are on treatment who would benefit from HCC surveillance. The GAG-HCC, CU-HCC, and REACH-B scores are validated in treated Asian CHB patients, whilst the PAGE-B score is validated in treated Caucasian CHB patients.27,28 Patients in the low HCC risk group may not require HCC surveillance due to their negligible risk whilst those deemed moderate or high risk should be offered HCC surveillance.15,27,28 As with all other clinical scoring systems, no single HCC risk score is perfect. Clinical rationalization between the utility and limitations of undertaking surveillance is essential, and shared decision-making between patient and clinician remains paramount.
When to Start Treatment?
Current international clinical practice guidelines unfortunately do not provide hard treatment endpoints specific to elderly patients with chronic HBV infection. Management of this cohort of patients is complex and requires an individualized approach. Multiple factors such as physiological changes, comorbidities, treatment compliance, treatment tolerability and efficacy, cost, patient’s values and preferences, and realistic treatment goals need to be considered.
Historically, antiviral therapy is generally not recommended for patients in the “immune tolerant” phase (phase 1). Current international clinical practice guidelines suggest monitoring of these patients with high HBV DNA levels and normal ALT.15,16,22 However, there is emerging evidence that administration of antiviral therapy in a subset of patients in the “immune tolerant” phase reduces the risk of developing cirrhosis and HCC but this remains controversial.29,30 Antiviral therapy is generally indicated for patients in the “immune active” phase (HBeAg-positive in phase 2, HBeAg-negative in phase 4) as it reduces the risk of cirrhosis, decompensation, and HCC.31–33 Treatment criteria however differ slightly between guidelines.15,16,22 For patients in the “immune inactive” phase (phase 3), current guidelines recommend monitoring these patients and antiviral therapy is generally not indicated.15,16,22
The threshold to commence antiviral therapy is much lower in patients with cirrhosis because there is good evidence that antiviral therapy improves outcome in both compensated and decompensated cirrhosis.31,34–36 IFNα is contraindicated in decompensated cirrhosis and therefore, these patients should be treated with a nucleoside or nucleotide analogue (NA) with high barrier to resistance and should be assessed for liver transplantation.15,16 For solid organ transplant recipients or patients undergoing immunosuppressive therapy or chemotherapy, treatment of chronic HBV infection is complex in these cases and beyond the scope of this review.
Choice of Antiviral Agents
Two main treatment options exist for chronic HBV infection which are NAs or pegylated IFNα (PegIFNα). NA is taken orally on a daily basis whilst PegIFNα is administered by subcutaneous injection on a weekly basis. Table 3 summarizes the choice of antiviral agents in chronic HBV infection.
 |
Table 3 Choice of Antiviral Agents in Chronic Hepatitis B |
NAs can be divided into those with a low barrier to HBV resistance (lamivudine [LAM], adefovir dipivoxil [ADV], telbivudine [TBV]) and those with a high barrier to HBV resistance (entecavir [ETV], tenofovir disoproxil fumarate [TDF], tenofovir alafenamide [TAF]). First-generation NAs such as LAM and ADV were widely used historically but have now fallen out of favour due to the major drawback of antiviral resistance.37 Current guidelines suggest a potent NA with high barrier to resistance regardless of the severity of liver disease, with either ETV, TDF, or TAF monotherapy as the preferred treatment regimen.15,16 The main advantage of using potent NAs with a high genetic barrier to resistance is their predictable long-term antiviral efficacy causing sustained HBV DNA suppression in a majority of patients who are compliant with treatment. NAs have also the added benefit of a generally favourable long-term safety profile.38–40 Although NAs are effective in suppressing viral replication, prolonged therapy is usually required and premature drug cessation may lead to loss of treatment benefits and clinical relapse. There is unfortunately no defined treatment duration based on current guidelines.15,16
PegIFNα is also recommended as an initial treatment option in chronic HBV infection. The main reason for a PegIFNα-based approach is to induce long-term immunological control with a finite and pre-defined treatment duration. The standard recommended duration of PegIFNα therapy is 48 weeks.15,16 Extension of treatment duration may be beneficial in selected HBeAg-negative CHB patients.15,41,42 The main disadvantages of PegIFNα therapy are the highly variable or unpredictable clinical response and considerable side effect profile leading to low tolerability. It is also contraindicated in patients with decompensated cirrhosis.15,16
Monitoring Response to Antiviral Treatment
For patients who are on NA treatment, liver function tests should be monitored every 3–4 months during the first year, and subsequently every 6 months. Serum HBV DNA levels should be measured every 3–4 months during the first year, and subsequently every 6–12 months. If HBV DNA level becomes undetectable, the presence of HBsAg should be checked on a yearly basis. Patients who achieve HBsAg loss should then be tested for any detectable anti-HBs.15
All patients on PegIFNα therapy should have ALT levels monitored on a monthly basis. Serum HBV DNA and HBsAg levels should be checked at 3, 6, and 12 months following initiation of PegIFNα therapy, and also at 6 and 12 months after completion of treatment. For HBeAg-positive patients, HBeAg status and presence of anti-HBe should additionally be checked at similar interval points. If HBV DNA level becomes undetectable, the presence of HBsAg should be checked on a yearly basis. Patients who achieve HBsAg loss should then be tested for any detectable anti-HBs. Patients who achieve virological response should still be kept under long-term surveillance due to the risk of clinical relapse.15 Figure 2 describes the algorithm for monitoring patients with chronic HBV infection who are on antiviral treatment.
 |
Figure 2 Algorithm for the monitoring of response to antiviral treatment. |
When to Stop Treatment?
Due to the risk of relapse following treatment cessation, duration of NA therapy is generally long-term in the majority of cases. In an ideal scenario, NA therapy can be safely discontinued if patients achieve HBsAg loss, with or without anti-HBs seroconversion.15 HBsAg clearance is associated with better clinical outcomes and relapse of viral replication is found to be rare if HBsAg clearance is achieved.43 Although regarded as the safest and optimal treatment endpoint, HBsAg clearance is however rare with NA therapy.15,16
For PegIFNα therapy, the standard recommended treatment duration is 48 weeks and can be stopped thereafter.15,16 Extension of treatment duration may be beneficial in selected HBeAg-negative CHB patients but is not routinely recommended.15,41,42
Due to the risk of life-threatening hepatic decompensation, current guidelines recommend that patients with chronic HBV infection and cirrhosis should remain on treatment indefinitely.15,16
Specific Considerations in the Treatment and Monitoring of Elderly Patients with Chronic Hepatitis B
Several studies have shown that the CHB patient population is aging and presenting with significantly more comorbidities.44–47 CHB has been reported to be associated with chronic kidney disease and osteoporosis.48,49 Recent large-scale nationwide studies in the USA, Hong Kong, and Taiwan revealed that patients with CHB are more likely to have a wide range of non-liver comorbidities such as cardiovascular disease, diabetes mellitus, renal impairment, hyperlipidaemia, and hypertension when compared to non-CHB controls.45–47 As a result of increasing comorbidities, the use of associated concomitant medications is also higher in CHB patients.45–47 This increases the likelihood of CHB patients of being exposed to medications, such as non-steroidal anti-inflammatory drugs (NSAIDs), angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), or diuretics, that can adversely affect their renal and bone profiles. Furthermore, the notable increase in conditions associated with metabolic syndrome in patients with CHB suggests the possibility of coexistent metabolic associated fatty liver disease (MAFLD), previously termed non-alcoholic fatty liver disease (NAFLD). MAFLD or NAFLD associated with CHB increases the risk of developing end-stage liver disease and mortality.50 Therefore, it is essential to take into account any comorbidities that elderly CHB patients may have as these have implications on the choice of antiviral treatment. Modifiable risk factors, especially for metabolic syndrome, should also be addressed accordingly.
Potent NAs with a high genetic barrier to resistance, such as ETV, TDF, or TAF, are preferable in elderly CHB patients given their tolerability profile compared to Peg IFNα. Long-term usage of NAs is generally safe, however, long-term ETV or TDF therapy has been associated with a decline in renal function and bone mineral density, especially with TDF.51–53 A baseline risk assessment should be performed for all patients prior to initiation of NA therapy. Patients at risk of renal disease who are on any NA and all patients treated with TDF, irrespective of renal risk, should have their renal function and serum phosphate levels monitored closely. These should be checked every 3 months during the first year of treatment and if stable, every 6 months thereafter. The dose of ETV and TDF should be adjusted appropriately for patients with eGFR < 50mL/min. No dose adjustment is required for TAF in patients with eGFR ≥ 15mL/min or in patients with eGFR < 15mL/min who are on chronic haemodialysis.15
Although there are specific treatment indications outlined in current international clinical practice guidelines as discussed, the decision to commence antiviral treatment in CHB is complex, especially in elderly patients. Given that NAs are the preferable treatment option in the elderly, there is significant treatment burden given the increased daily pill regime, need for prolonged therapy, and regular monitoring for treatment response and side effects. The financial cost is also a major factor that needs to be taken into consideration as healthcare systems vary widely across different countries and long-term treatment can incur a significant monetary burden on elderly patients. Therefore, shared decision-making between patient and clinician is essential to ensure that the final decision for or against treatment aligns with the patient’s values and preferences.
Although long-term NA therapy is shown to be effective in causing sustained HBV DNA suppression and slowing progression of liver disease in CHB, the risk of developing HCC is not completely eliminated.54,55 Therefore, elderly patients who are on long-term effective NA therapy should still be considered for HCC surveillance (see guidance above). However, it may not be practically feasible to undertake HCC surveillance on all patients for various legitimate reasons, including limited healthcare resources or excessive burden of treatment.
Conclusion
CHB infection remains a major global public health concern associated with significant morbidity and mortality. CHB in the elderly is becoming increasingly prevalent due to global population aging. Although international clinical practice guidelines exist, they do not provide hard treatment endpoints specific to elderly patients with CHB. Management of these patients is complex due to physiological changes associated with aging and multimorbidity, thereby necessitating an individualized approach.
Disclosure
Dr Paul N Brennan reports personal fees from Takeda, outside the submitted work. The authors report no conflicts of interest in this work.
References
1. Blumberg BS, Alter HJ, Visnich S. A “new” antigen in leukemia sera. JAMA. 1965;191:541–546. doi:10.1001/jama.1965.03080070025007
2. Schweitzer A, Horn J, Mikolajczyk RT, et al. Estimations of worldwide prevalence of chronic hepatitis B virus infection: a systematic review of data published between 1965 and 2013. Lancet. 2015;386(10003):1546–1555. doi:10.1016/S0140-6736(15)61412-X
3. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
4. Zanetti AR, Van Damme P, Shouval D. The global impact of vaccination against hepatitis B: a historical overview. Vaccine. 2008;26(49):6266–6273. doi:10.1016/j.vaccine.2008.09.056
5. Edelman R, Deming ME, Toapanta FR, et al. The SENIEUR protocol and the efficacy of hepatitis B vaccination in healthy elderly persons by age, gender, and vaccine route. Immun Ageing. 2020;17:9. doi:10.1186/s12979-020-00179-9
6. Wolters B, Junge U, Dziuba S, et al. Immunogenicity of combined hepatitis A and B vaccine in elderly persons. Vaccine. 2003;21(25–26):3623–3628. doi:10.1016/s0264-410x(03)00399-2
7. United Nations Department of Economic and Social Affairs. World Population Ageing 2019. Available from: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Report.pdf.
8. World Health Organization. Hepatitis B. Available from: https://www.who.int/news-room/fact-sheets/detail/hepatitis-b.
9. Ott JJ, Stevens GA, Groeger J, et al. Global epidemiology of hepatitis B virus infection: new estimates of age-specific HBsAg seroprevalence and endemicity. Vaccine. 2012;30(12):2212–2219. doi:10.1016/j.vaccine.2011.12.116
10. Zuckerman AJ. Chapter 70: hepatitis Viruses. In: Baron S, editor. Medical Microbiology.
11. Locarnini S. Molecular virology of hepatitis B virus. Semin Liver Dis. 2004;24(Suppl 1):3–10. doi:10.1055/s-2004-828672
12. Levrero M, Zucman-Rossi J. Mechanisms of HBV-induced hepatocellular carcinoma. J Hepatol. 2016;64(1 Suppl):S84–S101. doi:10.1016/j.jhep.2016.02.021
13. Tan A, Koh S, Bertoletti A. Immune Response in Hepatitis B Virus Infection. Cold Spring Harb Perspect Med. 2015;5(8):a021428. doi:10.1101/cshperspect.a021428
14. Bengsch B, Chang KM. Evolution in Our Understanding of Hepatitis B Virus Virology and Immunology. Clin Liver Dis. 2016;20(4):629–644. doi:10.1016/j.cld.2016.06.001
15. Lampertico P, Agarwal K, Berg T; European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;67(2):370–398. doi:10.1016/j.jhep.2017.03.021
16. Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology. 2018;67(4):1560–1599. doi:10.1002/hep.29800
17. McMahon BJ, Alward WL, Hall DB, et al. Acute hepatitis B virus infection: relation of age to the clinical expression of disease and subsequent development of the carrier state. J Infect Dis. 1985;151(4):599–603. doi:10.1093/infdis/151.4.599
18. Edmunds WJ, Medley GF, Nokes DJ, et al. The influence of age on the development of the hepatitis B carrier state. Proc Biol Sci. 1993;253(1337):197–201. doi:10.1098/rspb.1993.0102
19. Hyams KC. Risks of chronicity following acute hepatitis B virus infection: a review. Clin Infect Dis. 1995;20(4):992–1000. doi:10.1093/clinids/20.4.992
20. Hadler SC, Judson FN, O’Malley PM, et al. Outcome of hepatitis B virus infection in homosexual men and its relation to prior human immunodeficiency virus infection. J Infect Dis. 1991;163(3):454–459. doi:10.1093/infdis/163.3.454
21. Bodsworth NJ, Cooper DA, Donovan B. The influence of human immunodeficiency virus type 1 infection on the development of the hepatitis B virus carrier state. J Infect Dis. 1991;163(5):1138–1140. doi:10.1093/infdis/163.5.1138
22. Sarin SK, Kumar M, Lau GK, et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: a 2015 update. Hepatol Int. 2016;10(1):1–98. doi:10.1007/s12072-015-9675-4
23. McMahon BJ. The natural history of chronic hepatitis B virus infection. Hepatology. 2009;49(5 Suppl):S45–55. doi:10.1002/hep.22898
24. Mason WS, Gill US, Litwin S, et al. HBV DNA Integration and Clonal Hepatocyte Expansion in Chronic Hepatitis B Patients Considered Immune Tolerant. Gastroenterology. 2016;151(5):986–998.e4. doi:10.1053/j.gastro.2016.07.012
25. Carrion AF, Martin P. Viral hepatitis in the elderly. Am J Gastroenterol. 2012;107(5):691–697. doi:10.1038/ajg.2012.7
26. Osawa M, Akuta N, Suzuki F, et al. Prognosis and predictors of hepatocellular carcinoma in elderly patients infected with hepatitis B virus. J Med Virol. 2017;89(12):2144–2148. doi:10.1002/jmv.24890
27. Voulgaris T, Papatheodoridi M, Lampertico P, et al. Clinical utility of hepatocellular carcinoma risk scores in chronic hepatitis B. Liver Int. 2020;40(3):484–495. doi:10.1111/liv.14334
28. Papatheodoridis G, Dalekos G, Sypsa V, et al. PAGE-B predicts the risk of developing hepatocellular carcinoma in Caucasians with chronic hepatitis B on 5-year antiviral therapy. J Hepatol. 2016;64(4):800–806. doi:10.1016/j.jhep.2015.11.035
29. Chang Y, Choe WH, Sinn DH, et al. Nucleos(t)ide Analogue Treatment for Patients With Hepatitis B Virus (HBV) e Antigen-Positive Chronic HBV Genotype C Infection: a Nationwide, Multicenter, Retrospective Study. J Infect Dis. 2017;216(11):1407–1414. doi:10.1093/infdis/jix506
30. Kim GA, Lim YS, Han S, et al. High risk of hepatocellular carcinoma and death in patients with immune-tolerant-phase chronic hepatitis B. Gut. 2018;67(5):945–952. doi:10.1136/gutjnl-2017-314904
31. Marcellin P, Gane E, Buti M, et al. Regression of cirrhosis during treatment with tenofovir disoproxil fumarate for chronic hepatitis B: a 5-year open-label follow-up study. Lancet. 2013;381(9865):468–475. doi:10.1016/S0140-6736(12)61425-1
32. Kim WR, Loomba R, Berg T, et al. Impact of long-term tenofovir disoproxil fumarate on incidence of hepatocellular carcinoma in patients with chronic hepatitis B. Cancer. 2015;121(20):3631–3638. doi:10.1002/cncr.29537
33. Cho H, Ahn H, Lee DH, et al. Entecavir and tenofovir reduce hepatitis B virus-related hepatocellular carcinoma recurrence more effectively than other antivirals. J Viral Hepat. 2018;25(6):707–717. doi:10.1111/jvh.12855
34. Sinn DH, Lee J, Goo J, et al. Hepatocellular carcinoma risk in chronic hepatitis B virus-infected compensated cirrhosis patients with low viral load. Hepatology. 2015;62(3):694–701. doi:10.1002/hep.27889
35. Jang JW, Choi JY, Kim YS, et al. Long-term effect of antiviral therapy on disease course after decompensation in patients with hepatitis B virus-related cirrhosis. Hepatology. 2015;61(6):1809–1820. doi:10.1002/hep.27723
36. Peng CY, Chien RN, Liaw YF. Hepatitis B virus-related decompensated liver cirrhosis: benefits of antiviral therapy. J Hepatol. 2012;57(2):442–450. doi:10.1016/j.jhep.2012.02.033
37. Yim HJ, Hwang SG. Options for the management of antiviral resistance during hepatitis B therapy: reflections on battles over a decade. Clin Mol Hepatol. 2013;19(3):195–209. doi:10.3350/cmh.2013.19.3.195
38. Su TH, Hu TH, Chen CY, et al. Four-year entecavir therapy reduces hepatocellular carcinoma, cirrhotic events and mortality in chronic hepatitis B patients. Liver Int. 2016;36(12):1755–1764. doi:10.1111/liv.13253
39. Petersen J, Heyne R, Mauss S, et al. Effectiveness and Safety of Tenofovir Disoproxil Fumarate in Chronic Hepatitis B: a 3-Year Prospective Field Practice Study in Germany. Dig Dis Sci. 2016;61(10):3061–3071. doi:10.1007/s10620-015-3960-x
40. Agarwal K, Brunetto M, Seto WK, et al. 96 weeks treatment of tenofovir alafenamide vs. tenofovir disoproxil fumarate for hepatitis B virus infection. J Hepatol. 2018;68(4):672–681. doi:10.1016/j.jhep.2017.11.039
41. Lampertico P, Viganò M, Di Costanzo GG, et al. Randomised study comparing 48 and 96 weeks peginterferon α-2a therapy in genotype D HBeAg-negative chronic hepatitis B. Gut. 2013;62(2):290–298. doi:10.1136/gutjnl-2011-301430
42. Chen X, Chen X, Chen W, et al. Extended peginterferon alfa-2a (Pegasys) therapy in Chinese patients with HBeAg-negative chronic hepatitis B. J Med Virol. 2014;86(10):1705–1713. doi:10.1002/jmv.24013
43. Kim GA, Lim YS, An J, et al. HBsAg seroclearance after nucleoside analogue therapy in patients with chronic hepatitis B: clinical outcomes and durability. Gut. 2014;63(8):1325–1332. doi:10.1136/gutjnl-2013-305517
44. Liu A, Le A, Zhang J, et al. Increasing co-morbidities in chronic hepatitis B patients: experience in primary care and referral practices during 2000-2015. Clin Transl Gastroenterol. 2018;9(3):141. doi:10.1038/s41424-018-0007-6
45. Nguyen MH, Lim JK, Burak Ozbay A, et al. Advancing Age and Comorbidity in a US Insured Population-Based Cohort of Patients With Chronic Hepatitis B. Hepatology. 2019;69(3):959–973. doi:10.1002/hep.30246
46. Wong GLH, Wong VWS, Yuen BWY, et al. An Aging Population of Chronic Hepatitis B With Increasing Comorbidities: a Territory-Wide Study From 2000 to 2017. Hepatology. 2020;71(2):444–455. doi:10.1002/hep.30833
47. Tseng CH, Hsu YC, Ho HJ, et al. Increasing Age and Nonliver Comorbidities in Patients with Chronic Hepatitis B in Taiwan: a Nationwide Population-Based Analysis. Dig Dis. 2021;39(3):266–274. doi:10.1159/000511585
48. Fabrizi F, Donato FM, Messa P. Association between hepatitis B virus and chronic kidney disease: a systematic review and meta-analysis. Ann Hepatol. 2017;16(1):21–47. doi:10.5604/16652681.1226813
49. Chen CH, Lin CL, Kao CH. Association Between Chronic Hepatitis B Virus Infection and Risk of Osteoporosis: a Nationwide Population-Based Study. Medicine. 2015;94(50):e2276. doi:10.1097/MD.0000000000002276
50. Lin CW, Huang XL, Liu HL, et al. Interactions of Hepatitis B Virus Infection with Nonalcoholic Fatty Liver Disease: possible Mechanisms and Clinical Impact. Dig Dis Sci. 2015;60(12):3513–3524. doi:10.1007/s10620-015-3772-z
51. Lampertico P, Chan HLY, Janssen HLA, et al. Review article: long-term safety of nucleoside and nucleotide analogues in HBV-monoinfected patients. Aliment Pharmacol Ther. 2016;44(1):16–34. doi:10.1111/apt.13659
52. Han Y, Zeng A, Liao H, et al. The efficacy and safety comparison between tenofovir and entecavir in treatment of chronic hepatitis B and HBV related cirrhosis: a systematic review and Meta-analysis. Int Immunopharmacol. 2017;42:168–175. doi:10.1016/j.intimp.2016.11.022
53. Law ST, Lee MK, Li KK, et al. Comparison of efficacy and renal safety of telbivudine and entecavir in treatment-naive elderly patients with chronic hepatitis B. Eur J Gastroenterol Hepatol. 2016;28(2):193–198. doi:10.1097/MEG.0000000000000519
54. Varbobitis I, Papatheodoridis GV. The assessment of hepatocellular carcinoma risk in patients with chronic hepatitis B under antiviral therapy. Clin Mol Hepatol. 2016;22(3):319–326. doi:10.3350/cmh.2016.0045
55. Papatheodoridis GV, Chan HLY, Hansen BE, et al. Risk of hepatocellular carcinoma in chronic hepatitis B: assessment and modification with current antiviral therapy. J Hepatol. 2015;62(4):956–967. doi:10.1016/j.jhep.2015.01.002
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.