")
Back to Journals » Breast Cancer: Targets and Therapy » Volume 16
HER2 Low Expression in Primary Male Breast Cancer
Authors Nobbe K, Erices-Leclercq M, Foerster F, Förster R, Baldus SE, Rudlowski C , Schröder L, Lubig S
Received 20 November 2023
Accepted for publication 27 February 2024
Published 28 March 2024 Volume 2024:16 Pages 141—148
DOI https://doi.org/10.2147/BCTT.S450682
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Pranela Rameshwar
Katleen Nobbe,1 Melanie Erices-Leclercq,1 Frank Foerster,2,3 Robert Förster,4 Stephan E Baldus,5 Christian Rudlowski,1,6 Lars Schröder,7 Sabine Lubig1
1Breast Unit, Lutheran Hospital Bergisch Gladbach, Bergisch Gladbach, Germany; 2Department of Economical Sciences, University of Applied Sciences, Zwickau, Germany; 3Outpatient Department of Gynaecological Oncology and Palliative Care, Chemnitz, Germany; 4Institute for Radiation Oncology, Cantonal Hospital Winterthur, Winterthur, Switzerland; 5Institute for Pathology, Cytology and Molecular Pathology, Bergisch Gladbach, Germany; 6Department of Gynecology, University Hospital Bonn, Bonn, Germany; 7Department of Gynaecology and Obstetrics, Ketteler Krankenhaus, Offenbach, Germany
Correspondence: Christian Rudlowski, Breast Unit, Lutheran Hospital Bergisch Gladbach, Ferrenbergstrasse 24, Bergisch Gladbach, 51465, Germany, Email [email protected]
Purpose: The introduction of HER2-targeting antibody drug conjugates (ADCs) offers new treatment options for female breast cancer patients (FBC) expressing low levels of HER2 (HER2 low). No evidence was found that HER2 low describes a new FBC subtype. There is a lack of studies determining the impact of HER2 low in male breast cancer (MBC). In this study, we evaluate the prevalence of HER2 low in primary MBC and correlate the results with patient characteristics.
Patients and Methods: In this study, histological specimens were obtained from 120 male patients diagnosed and treated for primary invasive breast cancer from 1995 to 2022 at Breast Cancer Units in Bergisch Gladbach, Chemnitz, and Zwickau, Germany. HER2 immunostaining and in situ hybridization were performed by central pathology and evaluated based on the ASCO/CAP guidelines. The correlation of expression of HER2 low with tumor biological characteristics and patient outcomes was investigated.
Results: Out of all cases, four patients (3.3%) showed HER2 positivity (3+), 39 (32.5%) patients were classified as HER2 low, 7 (5.8%) were HER2 2+ (no amplification), 32 (26.7%) were HER2 1+, and 77 (64.2%) were classified as HER2 zero. Out of 77 HER2 zero cases, 47 tumors (61.0%) showed incomplete staining, with < 10% of tumor cells classified as HER2 ultralow. No statistical correlation between HER2 low and tumor biological characteristics and patients’ survival was found.
Conclusion: Our findings show a notable, albeit lower, prevalence of HER2 low expression in primary MBC. However, tumors expressing HER2 low do not show specific tumor biological features to define a new breast cancer subtype in MBC. Our results suggest that a significant number of MBC patients could benefit from ADCs, as shown in FBC. Further studies are required to better understand HER2 low breast cancer, both generally and in MBC.
Keywords: male breast cancer, HER2 low, prognosis, survival
Introduction
Female breast cancer (FBC) and male breast cancer (MBC) share biological similarities, but significant differences regarding risk factors, prognosis, and response to therapy have been observed.1 MBC represents a more homogeneous tumor cohort with only minor differences in hormone receptor (HR) expression and HER2 distribution. Usually, MBC is highly HR positive and HER2 negative.2
HER2 is a transmembrane receptor tyrosine kinase encoded by the ERBB2 gene.3
It is a potent oncogene associated with a more aggressive tumor behavior.4 HER2 positivity is a therapeutic target for monoclonal antibody trastuzumab as well as for other anti-HER2 compounds.5 The introduction of targeted therapies was able to change treatment and prognosis dramatically.6 Until now HER2 classification followed a binary approach to distinguish between HER2 positive or negative: according to the American Society of Clinical Oncology and College of American Pathologists (ASCO/CAP), breast cancer is defined as HER2 positive by protein overexpression score 3+ with immunohistochemistry (IHC) and/or a IHC score 2+ with gene amplification in situ hybridization (ISH).7 Female as well as male patients who show HER2 positivity are recommended to be treated with antibodies. Patients who were categorized as HER2 negative were not treated with antibodies due to a lack of response.8
Recent studies shed light on reconsidering the spectrum of HER2 classification: in females more than 60% of HER2 negative breast tumors express low levels of HER2, defined as a score of 1+ by IHC or as an IHC score of 2+ and negative in ISH.7,9 The development of antibody drug conjugates (ADCs) targeting tumors with low levels of HER2, such as trastuzumab-deruxtecan (T-DXd), expand treatment options for HER2-expressing breast cancer.
Current clinical studies such as DESTINY-breast04 (D-b04) and DAISY trial presented promising data regarding treatment options for FBC expressing low levels of HER2.9–11 These studies focus on female patients. The D-b04 trial for metastatic FBC was able to show that patients with low levels of HER2 benefit from ADC therapy.10 In the ongoing DESTINY-breast06 (D-b06) study the efficacy of ADC T-DXd for tumors with very low levels of HER2 expression, so-called HER2 ultralow, was also tested.12 To assess this distinctive breast cancer subtype accurately might be challenging.
According to our knowledge there is no research available investigating the biological significance of HER2 low for primary MBC. Since the majority of MBC is HER2 negative there is a need to further investigate if there is a similar HER2 low distribution as in FBC. This could lead to a shift in pathological assessment as well as clinical treatment of MBC tumors.
In this study we aimed to describe the prevalence of HER2 low status in a cohort of primary MBC with emphasis on clinicopathologic features and clinical outcome.
Since the D-b06 trial is still proceeding we adapted their study design distinguishing HER2 low into subtypes HER2 low and HER2 ultralow to further investigate if there are new treatment options for these patients.
Materials and Methods
Patient Selection
In this multicenter retrospective study, histological specimens were obtained from 120 male patients who were diagnosed and treated for primary invasive breast cancer from 1995 to 2022 at Breast Cancer Units in Bergisch Gladbach, Chemnitz, and Zwickau, Germany. The patient data, histological findings, as well as treatment reports and follow-up data were collected with the approval of review boards from the hospital archives. The study was approved by the institutional local ethics committee (no.: 005/2005, University of Bonn, Germany) and in accordance with the declarations of Helsinki. Written informed consent was obtained from all patients.
Histopathological Analysis
Tumor specimens were fixed in formalin and embedded in paraffin. Immunohistological staining (IHC) was performed using an automatic immunostaining system (Ventana Benchmark GX, Roche Diagnostics, Mannheim, Germany) according to the manufacturer’s instructions.
All specimens were counterstained with hematoxylin. Pathohistological evaluation was performed within two weeks by two experienced physicians (S.E.B. and C.R.) after immune-histological staining.
Slides were microscopically reviewed. Histological carcinoma classification was recorded in accordance with current World Health Organization staging.13 Pathological staging was classified according to the International Union Against Cancer.14
HR status was evaluated using the Remmele and Stegner score,15 which is an immune reactivity score. For Ki67 immunostaining clone 30–9 (Roche Diagnostics) was used. The cut-off point of 13.5% for Ki67 was used referring to Erices-Leclercq et al.16
HER2 protein expression was determined with VENTANA anti-HER2/neu (4B5) Rabbit Monoclonal Primary Antibody (CE IVD, Roche Diagnostics). HER2 membrane staining intensity and pattern were analyzed based on ASCO/CAP approved criteria: 3+ immune staining was considered positive, and 2+ staining was categorized as equivocal. In this case HER2 positivity was defined by its gene amplification status (FISH) using standardized protocols.17 HER2 low was considered as a score 1+ and 2+ (FISH negative); 1+ was defined as an incomplete staining that was barely perceptible with >10% of tumor cells,and 2+ as weak to moderate complete membrane staining observed in >10% of tumor cells.
HER2 ultralow was defined by an incomplete staining with <10% of tumor cells. No staining was described as HER2 zero (Figure 1).
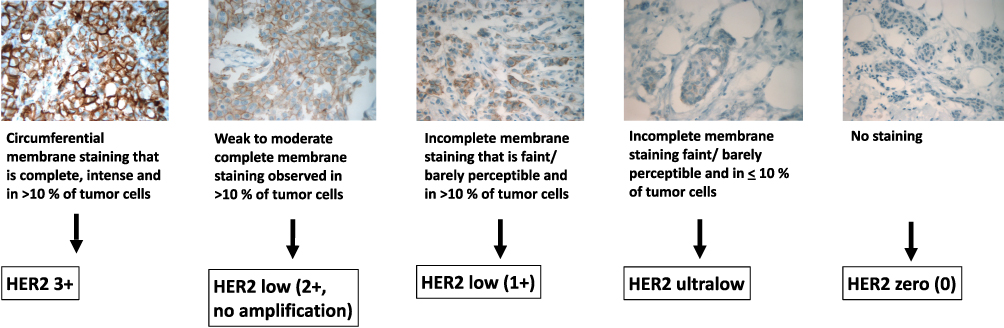 |
Figure 1 HER2-testing in primary male breast cancer. |
Statistical Analysis
The analysis of standard deviation, variance, and range are among the measures of dispersion and were evaluated. By calculating those parameters, we have ensured that our counted values correspond to a statistically correct homogeneous series of measurements. Overall survival (OS) benefits were calculated according to Kaplan–Meier curve (KMC).
We tested for significance using Spearman correlation as well as chi2 test and Fisher–Freeman–Halton exact test for small sample sizes to correlate histopathological features with our HER2 subgroups. All results were considered significant at p-values <0.05. All analyses were performed using the SPSS software package version 29 (SPSS Inc., Chicago, IL), and Microsoft® Excel® 2010, version 14 for Windows (Microsoft Corp., Redmond, WA).
Results
Patients’ age ranged from 34 to 89 years (median 66 years). Follow-up data were available for 109 patients. The median follow-up time was 59 months (range 1–207). The median overall survival (OS) was 97 months (range 1–207 months). Thirty-eight patients (35.8%) experienced relapse, and 38.3% (n = 46) of patients died.
Due to the retrospective characteristics of this study, data regarding treatment was incomplete. In 80.0% (n = 96) of cases patients underwent modified radical mastectomy. Breast-preserving surgery was carried out in 5.8% (n = 7) of patients, and 45.0% (n = 54) were treated adjuvantly with tamoxifen. Seven patients (5.8%) received aromatase inhibitors. Adjuvant chemotherapy was administered in 34 cases (28.3%).
Most tumors had intermediate differentiation (G2, 70.0%, n = 84); 7.5% (n = 9) were well (G1) and 22.5% (n = 27) poorly differentiated. A total of 43.3% (n = 35) of patients were diagnosed at tumor stage pT1, whereas 23.3% (n = 28) had stage pT2 and 3 patients (2.5%) stage pT3. Stage pT4 was found in 12.5% (n = 15); 36.7% (n = 44) of patients already had axillar lymph node metastases at the time of diagnosis.
In our cohort 119 (99.2%) tumors expressed estrogen receptors (ER), and 114 (95.0%) expressed progesterone receptors (PR). High Ki67 levels were found in 66 cases (55.0%).
A total of 120 tumors were available for HER2 expression analysis: 77 (64.2%) of cases were classified as HER2 negative, 39 (32.5%) as HER2 low, 7 (5.8%) were HER2 2+ (ISH negative), and 32 (26.7%) were HER2 1+. Four patients (3.3%) showed HER2 positivity (3+, ISH positive). Out of the 77 HER2 negative cases 47 tumors (39.2%) showed an incomplete staining with <10% of tumor cells, classified as HER2 ultralow (Figure 2). All the cases showing HER2 expression were HR positive. Regarding the immunohistochemical defined subtypes, 39.2% (n = 47) of cases were characterized as luminal A and 56.7% (n = 68) as luminal B type breast cancer. One patient was triple negative.
 |
Figure 2 HER2 expression in primary male breast cancer. Abbreviation: FISH, fluorescence-in-situ-hybridization. Notes: *FISH negative, **FISH positive. |
There was no correlation between histological markers and HER2 negative tumors, nor HER2 low/ultra-low tumors (Table 1). Among patients with tumor relapse, two patients showed HER2 overexpression (HER2 3+), 21 patients were HER2 low (HER2 1+), and 15 patients were classified as HER2 negative (HER2 ultralow in 5 and HER2 zero in 10 patients).
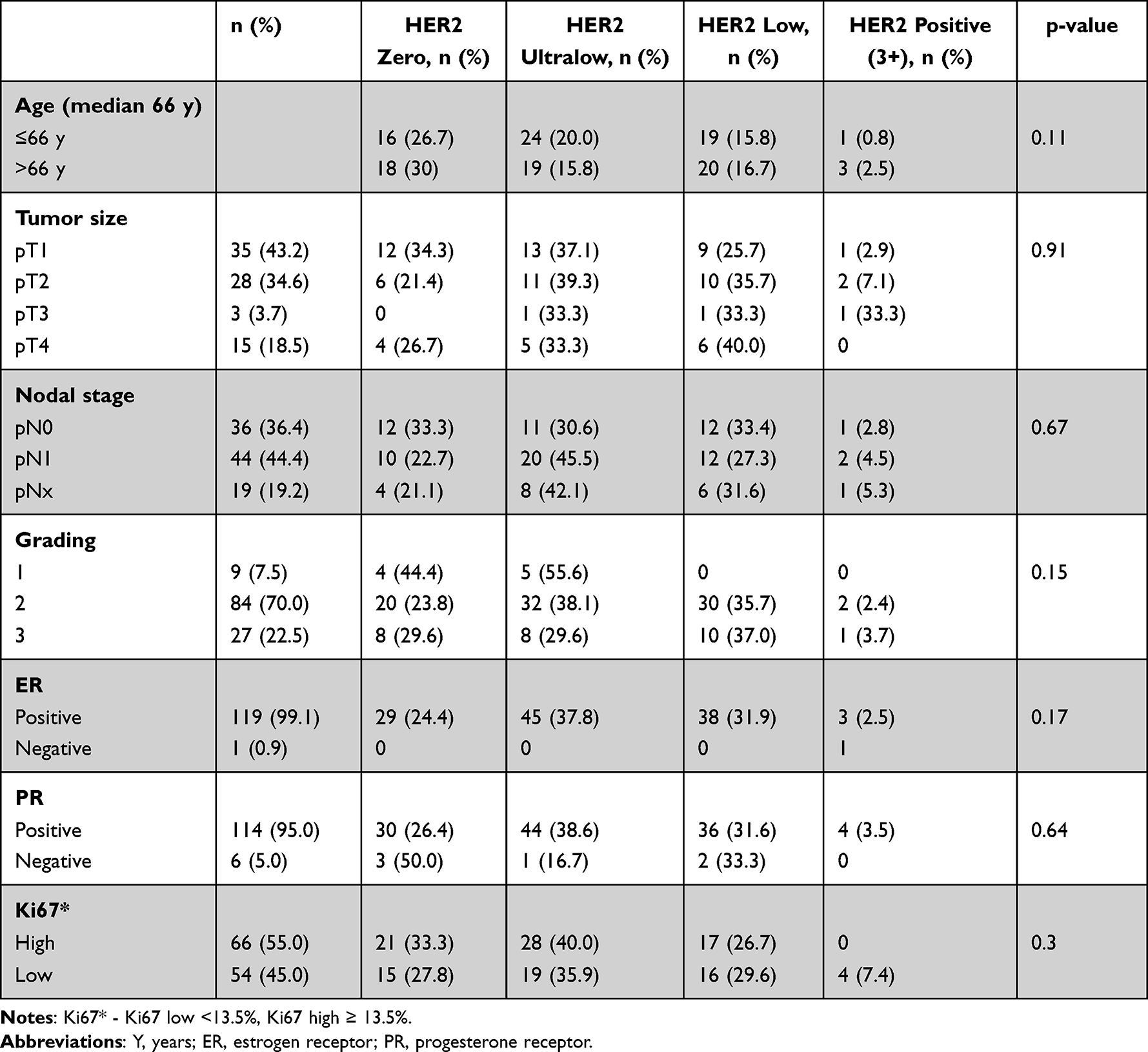 |
Table 1 Patient Characteristics Correlated with HER2 Expression in Primary Male Breast Cancer |
We calculated Kaplan–Meier curves (KMC) to determine disease-free survival (DFS) and overall survival (OS) for HER2 expression. There was no statistical significance regarding progression-free survival (PFS) and OS for HER2 zero and HER2 low. However, when comparing OS for HER2 zero, HER2 low, and HER2 ultralow, we were able to show a trend (p = 0.058) towards a survival benefit for patients with HER2 zero expression (Figure 3).
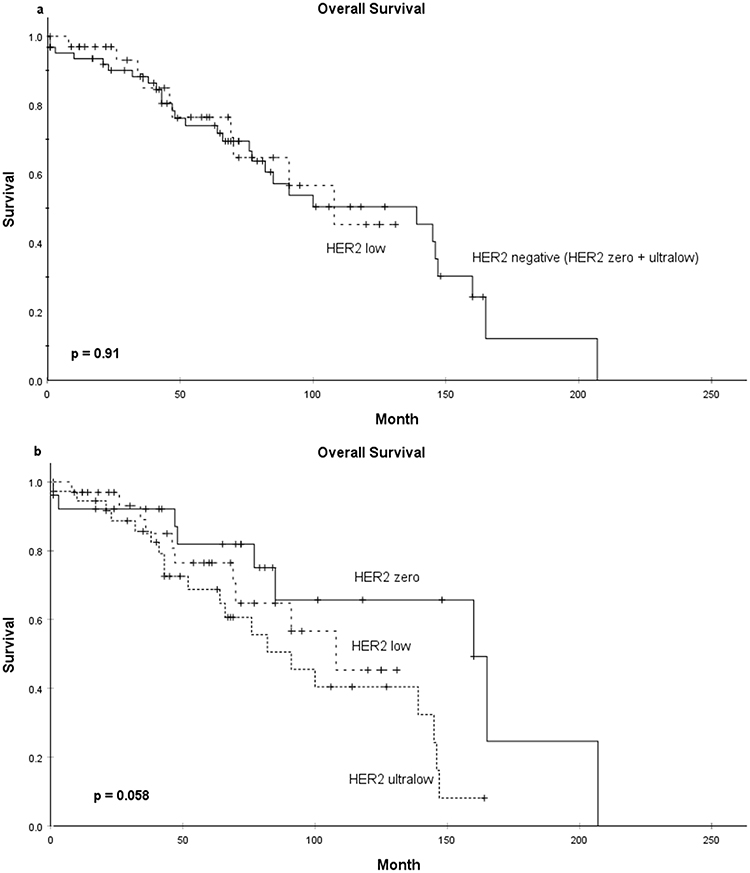 |
Figure 3 Kaplan–Meier curves for overall survival in primary male breast cancer. (a) Estimated survival calculated for HER2 low and HER2 negative tumors. (b) Estimated survival calculated for HER2 low, HER2 ultralow, and HER2 zero tumors. |
Discussion
In clinical practice treatment regimens for MBC patients are adapted from FBC guidelines. Prospective studies designed exclusively for primary MBC are rare. However, recently published prospective multicenter studies allowed male patients to participate. The recently published D-b04 trial included only two men out of 557 randomized patients, and only one male patient participated in the DAISY trial.10,11 Therefore, and due to its rare occurrence, it is of great value to base treatment decisions on male-specific tumor behavior.
Treating HER2 positive MBC patients with trastuzumab-containing regimens was practice-changing. Real-world data and case reports have shown evidence for this treatment option.18 Yet, no prospective trial was found in the literature giving evidence that HER2 positive MBC patients benefit from trastuzumab.
At the moment MBC is dichotomously categorized into HER2 negative or positive. In FBC approximately 60% of tumors show HER2 low expression.19,20 Promising study results for FBC offer new therapeutic regimens for patients showing low HER2 expression. It is clinically evident that activity of ADCs is independent of HER2 overexpression and amplification.21
The aim of this study was to evaluate if there is a similar distribution pattern of HER2 negative and HER2 low within this MBC cohort compared to females. In accordance with the literature our data demonstrate that MBC is dominated by luminal A and B subtype tumors.1,2,22 In our study HER2 positivity was less than 4%, which is in line with recently published data.23
In our cohort, 32.5% of cases show HER2 low expression, which is much lower compared to FBC.12 Out of the 64% HER2 negative tumors more than half showed at least a weak and incomplete but reproduceable HER2 staining classified as HER2 ultralow. These findings could have a significant clinical impact, since MBC patients showing low levels of HER2 expression might have access to new treatment options.
The clinical impact of this HER2 ultralow subclass is uncertain and therefore not established.24 The role of ADCs in this subgroup is being investigated in the ongoing D-b06 study including patients with HER2 IHC 0 but minimal expression (IHC score >0 but <1+).9,25
No statistical correlation between HER2 low and the established prognostic parameters or clinicopathological features was shown, which is in accordance with findings in MBC.20 Survival analyses revealed that HER2 low does not define a subgroup that has an impact on OS in MBC.
A limitation of our present study may be given by the fact that the data are based on a retrospective study with a limited sample size as well as incomplete follow-up data. It will be a future task to further investigate HER2 low and HER2 ultralow in MBC. It could be also of interest to shed light on survival analyses.
There is a risk that the IHC assay used in this study was suboptimal to detect low levels of protein expression and could therefore result in false-negative and/or false-positive test determination around the IHC 0/IHC 1+ threshold that would incorrectly influence our data.7 The recently published DAISY trial supports the assumption that IHC may not be the optimal method to define a boundary of HER2 expression to predict efficacy of treatment in patients with HER2 low FBC.11
To the best of our knowledge this is the first comprehensive study evaluating HER2 low and ultralow in primary MBC. Our data support the hypothesis that HER2 low defines no MBC-specific subgroup but is rather an important therapeutic target as recently established in metastatic FBC.10
Conclusion
Our findings illustrate a remarkable but lower prevalence of HER2 low disease in primary MBC compared to FBC. Further studies are required to better understand HER2 low breast cancer in general and for MBC.
Abbreviations
ADCs, antibody drug conjugates; FBC, female breast cancer; IHC, immunohistochemistry; FISH, fluorescence-in-situ-hybridization; MBC, male breast cancer; T-DXd, trastuzumab-deruxtecan.
Funding
This work was supported by the German Cancer Foundation Grant Number 70-3157. The authors declare that no other support was received during the preparation of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cardoso F, Bartlett JMS, Slaets L, et al. Characterization of male breast cancer: results of the EORTC 10085/TBCRC/BIG/NABCG International Male Breast Cancer Program. Ann Oncol. 2018;29(2):405–417. doi:10.1093/annonc/mdx651
2. Nilsson C, Johansson I, Ahlin C, et al. Molecular subtyping of male breast cancer using alternative definitions and its prognostic impact. Acta Oncol. 2013;52(1):102–109. doi:10.3109/0284186X.2012.711952
3. Slamon DJ, Clark GM, Wong SG, Levin WJ, Ullrich A, McGuire WL. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science. 1987;235(4785):177–182. doi:10.1126/science.3798106
4. Hamilton E, Shastry M, Shiller SM, Ren R. Targeting HER2 heterogeneity in breast cancer. Cancer Treat Rev. 2021;100:102286. doi:10.1016/j.ctrv.2021.102286
5. Marchio C, Annaratone L, Marques A, Casorzo L, Berrino E, Sapino A. Evolving concepts in HER2 evaluation in breast cancer: heterogeneity, HER2-low carcinomas and beyond. Semin Cancer Biol. 2021;72:123–135. doi:10.1016/j.semcancer.2020.02.016
6. Dieci MV, Miglietta F. HER2: a never ending story. Lancet Oncol. 2021;22(8):1051–1052. doi:10.1016/S1470-2045(21)00349-1
7. Wolff AC, Somerfield MR, Dowsett M, et al. Human epidermal growth factor receptor 2 testing in breast cancer: ASCO-College of American Pathologists Guideline Update. J Clin Oncol. 2023:JCO2202864. doi:10.1200/JCO.22.02864
8. Ponde N, Brandao M, El-Hachem G, Werbrouck E, Piccart M. Treatment of advanced HER2-positive breast cancer: 2018 and beyond. Cancer Treat Rev. 2018;67:10–20. doi:10.1016/j.ctrv.2018.04.016
9. Nicolo E, Boscolo Bielo L, Curigliano G, Tarantino P. The HER2-low revolution in breast oncology: steps forward and emerging challenges. Ther Adv Med Oncol. 2023;15:17588359231152842. doi:10.1177/17588359231152842
10. Modi S, Jacot W, Yamashita T, et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N Engl J Med. 2022;387(1):9–20. doi:10.1056/NEJMoa2203690
11. Mosele F, Deluche E, Lusque A, et al. Trastuzumab deruxtecan in metastatic breast cancer with variable HER2 expression: the Phase 2 DAISY trial. Nat Med. 2023;29(8):2110–2120. doi:10.1038/s41591-023-02478-2
12. Corti C, Giugliano F, Nicolo E, Tarantino P, Criscitiello C, Curigliano G. HER2-low breast cancer: a new subtype? Curr Treat Options Oncol. 2023;24(5):468–478. doi:10.1007/s11864-023-01068-1
13. Sinn HP, Helmchen B, Wittekind CH. TNM-Klassifikation beim Mammakarzinom: neuerungen und Anmerkungen zur 7. Auflage [TNM classification of breast cancer: changes and comments on the 7th edition]. Pathologe. 2010;31(5):361–366. German. doi:10.1007/s00292-010-1307-0
14. Wittekind C. Regionare Lymphknoten, Satelliten und TNM: werden wir besser? 7. Edition der UICC 2010 zur TNM-Klassifikation maligner Tumoren [Lymph nodes, tumour deposits, and TNM: are we getting better? 7th edition of UICC 2010 TNM classification of malignant tumors]. Strahlenther Onkol. 2012;188(2):191–192. German. doi:10.1007/s00066-011-0032-9
15. Remmele W, Stegner HE. Vorschlag zur einheitlichen Definition eines Immunreaktiven Score (IRS) fur den immunhistochemischen Ostrogenrezeptor-Nachweis (ER-ICA) im Mammakarzinomgewebe [Recommendation for uniform definition of an immunoreactive score (IRS) for immunohistochemical estrogen receptor detection (ER-ICA) in breast cancer tissue]. Pathologe. 1987;8(3):138–140. German.
16. Erices-Leclercq M, Lubig S, Forster F, et al. Prognostic relevance of Ki67 expression in primary male breast cancer: determination of cut-off points by different evaluation methods and statistical examinations. J Cancer Res Clin Oncol. 2022;148(2):441–447. doi:10.1007/s00432-021-03623-5
17. Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med. 2005;353(16):1659–1672. doi:10.1056/NEJMoa052306
18. Rudlowski C, Rath W, Becker AJ, Wiestler OD, Buttner R. Trastuzumab and breast cancer. N Engl J Med. 2001;345(13):997–998.
19. Tarantino P, Hamilton E, Tolaney SM, et al. HER2-low breast cancer: pathological and clinical landscape. J Clin Oncol. 2020;38(17):1951–1962. doi:10.1200/JCO.19.02488
20. Tarantino P, Jin Q, Tayob N, et al. Prognostic and biologic significance of ERBB2-low expression in early-stage breast cancer. JAMA Oncol. 2022;8(8):1177–1183. doi:10.1001/jamaoncol.2022.2286
21. Giugliano F, Curigliano G, Tarantino P. HER2-low expression in breast oncology: treatment implications in the smart chemotherapy era. Eur J Cancer Prev. 2023;32(2):149–154. doi:10.1097/CEJ.0000000000000781
22. Jylling AMB, Jensen V, Lelkaitis G, Christiansen P, Nielsen SS, Lautrup MD. Male breast cancer: clinicopathological characterization of a National Danish cohort 1980–2009. Breast Cancer. 2020;27(4):683–695. doi:10.1007/s12282-020-01066-3
23. Rudlowski C, Friedrichs N, Faridi A, et al. Her-2/neu gene amplification and protein expression in primary male breast cancer. Breast Cancer Res Treat. 2004;84(3):215–223. doi:10.1023/B:BREA.0000019953.92921.7e
24. Denkert C, Seither F, Schneeweiss A, et al. Clinical and molecular characteristics of HER2-low-positive breast cancer: pooled analysis of individual patient data from four prospective, neoadjuvant clinical trials. Lancet Oncol. 2021;22(8):1151–1161. doi:10.1016/S1470-2045(21)00301-6
25. Nicolo E, Tarantino P, Curigliano G. Biology and treatment of HER2-low breast cancer. Hematol Oncol Clin North Am. 2023;37(1):117–132. doi:10.1016/j.hoc.2022.08.013
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.