")
Back to Journals » Nature and Science of Sleep » Volume 16
Gender Differences in Prevalence of Sleepy Driving Among Young Drivers in Saudi Arabia
Authors Alqurashi YD , Alqarni AS, Albukhamsin FM, Alfaris AA, Alhassan BI, Ghazwani WK, Altammar AA, Aleid ME, Almutary H , Aldhahir AM , Alessy SA, Almusally R, Alsaid A, Mahmoud MI, Qutub HO, Sebastian T , Alghnam S, Polkey MI
Received 4 October 2023
Accepted for publication 5 January 2024
Published 1 February 2024 Volume 2024:16 Pages 53—62
DOI https://doi.org/10.2147/NSS.S439161
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Yousef D Alqurashi,1 Abdullah S Alqarni,1 Faisal Maher Albukhamsin,1 Abdullah Abdulaziz Alfaris,1 Bader Ibrahim Alhassan,1 Waleed Khalid Ghazwani,1 Abdulaziz Abdulrahman Altammar,1 Mutlaq Eid Aleid,1 Hayfa Almutary,2 Abdulelah M Aldhahir,3 Saleh A Alessy,4 Rayyan Almusally,5 Abir Alsaid,5 Mahmoud Ibrahim Mahmoud,5 Hatem Othman Qutub,5 Tunny Sebastian,6 Suliman Alghnam,7 Michael I Polkey8
1Respiratory Care Department, College of Applied Medical Sciences, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2Medical Surgical Nursing Department, King Abdulaziz University, Jeddah, Saudi Arabia; 3Respiratory Therapy Department, Faculty of Applied Medical Sciences, Jazan University, Jazan, Saudi Arabia; 4Department of Public Health, College of Health Sciences, Saudi Electronic University, Jeddah, Saudi Arabia; 5Internal Medicine Department, King Fahd Hospital of the University, Imam Abdulrahman Bin Faisal University, Khobar, Saudi Arabia; 6Clinical Nutrition Department, College of Applied Medical Sciences, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 7Population Health Section-King Abdullah International Medical Research Center (KAIMRC), King Saud Bin Abdulaziz University for Health Sciences (KSAU-HS), Riyadh, Saudi Arabia; 8Royal Brompton Hospital, Guy’s and St Thomas’ NHS Foundation Trust, London, UK
Correspondence: Yousef D Alqurashi, Respiratory Care Department, College of Applied Medical Sciences, Imam Abdulrahman Bin Faisal University, Dammam, 34221, Saudi Arabia, Email [email protected]
Introduction: Sleepy driving is associated with Motor Vehicles Accidents (MVAs). In Saudi Arabia, previous studies have addressed this association among men only. Therefore, the aim of this study was to compare the prevalence of sleepy driving and associated factors between genders.
Methods: In a cross-sectional study design, we offered a self-administered online questionnaire to 3272 participants from different regions of Saudi Arabia. The questionnaire included 46 questions covering sociodemographics, driving habits, sleeping habits, Epworth Sleepiness Scale, and Berlin questionnaire to assess the risk of sleep apnea. Univariable and multivariable logistic regression analyses were used to determine the significant factors associated with self-reported sleepy driving, defined as operating a motor vehicle while feeling sleepy in the preceding six months.
Results: Of the 3272 invitees, 2958 (90%) completed the questionnaire, of which 1414 (48%) were women. The prevalence of sleepy driving in the preceding six months was 42% (men: 50% and women 32%, p< 0.001). Specifically, participants reported the following: 12% had had to stop their vehicle due to sleepiness (men: 16.2% and women 7%, p< 0.001), 12.4% reported near-miss accidents (men: 16.2% and women: 8.2%, p< 0.001) and 4.2% reported an accident due to sleepiness (men: 4.3% and women: 4%, p=0.645). In multivariable analysis, being male, younger age, use of any type of medications, shift working, working more than 12 hours per day, driving duration of 3– 5 hours per day, driving experience of more than 2 years, excessive daytime sleepiness and risk of having obstructive sleep apnea were all associated with increased likelihood of falling asleep while driving in the preceding 6 months.
Conclusion: Sleepy driving and MVA are prevalent in both gender but was higher in men. Future public health initiatives should particularly focus on men, since men reported a greater likelihood of both sleep-related MVA and “near miss” events.
Keywords: sleepiness, driving, obstructive sleep apnea, OSA, gender differences
Introduction
Motor vehicle accidents (MVAs) are one of the leading causes of mortality globally; approximately 1.3 million people die each year because of MVA. These accidents cost countries more than 3% of their gross domestic product (GDP).1 In Saudi Arabia, MVA was the fifth most common cause of death in 2019. The death rate associated with MVA in Saudi Arabia is 28 per 100.000 population; this is above the world average (17.4 per 100.000 population), and even above the average of low-income countries (24.1 per 100.000 population).2 According to the Saudi Ministry of Health, there were 437,602 MVA in 2020; these MVA resulted in 4618 deaths and 25,561 injuries.3
Sleepy driving is thought to contribute to approximately 20% of all MVA types globally.4–8 Few studies have assessed whether the prevalence of sleepy driving differs by gender, which was confirmed by a recent systematic review and meta-analysis.9 Locally, a prior study conducted in Saudi Arabia demonstrated that sleepiness was a contributor to 11.6% of all MVAs.10 However, since women were not legally permitted to drive in Saudi Arabia until 2018, sleepy driving has hitherto mainly been assessed in men. However, in a population-based analysis, Al Shareef et al examined the association between excessive daytime sleepiness and falling asleep while driving and found that the male gender was the strongest predictor of drowsiness while driving.11 However, only 13% of his study participants were women. Furthermore, the association between obstructive sleep apnea (OSA) and sleepy driving has been well documented in the literature,5,12 but the role of gender in this association has not been studied.9
Therefore, the aim of this study was to assess the gender differences in prevalence of sleepy driving and associated factors, importantly factoring in the risk of having undiagnosed OSA, among both men and women in Saudi Arabia. We also aimed to investigate the practices used to counter sleepiness while driving in both genders.
Methodology
Study Subjects
This was a cross-sectional study conducted between February and June 2022. Data collectors from each of the provinces in Saudi Arabia were first identified. Then data collectors were asked to recruit, as much as possible, drivers of both genders from their provinces. Participants were invited to take part in the study through either emails or other social media invitations such as WhatsApp, Instagram, and Twitter, after the study purpose was explained. Participants were requested to complete a self-administered online questionnaire available in Arabic or English, and participants could complete either of them according to their preference. Exclusion criteria were an age <18 (the legal driving age) or >65 years old, a self-reported known diagnosis of a sleep disorder, or pregnancy.
The study was approved by the Research Ethic Committee (REC) of Imam Abdulrahman Bin Faisal University (IRB-UGS-2022-03-050). Consent to participate was obtained electronically before the participants were permitted to proceed to the study. The Helsinki principles were followed throughout the study.
Questionnaire
The questionnaire content was based on prior published studies.10,13–15 The questionnaire consisted of 46 organized multiple-choice questions, as listed below (see Figure S1). The time required to complete the questionnaire was approximately 10 minutes.
The following questions were included:
- Ten questions assessed participants’ demographic data.
- Two questions assessed participants’ work times and duration.
- One question assessed if the participant had been diagnosed with any sleep disorders.
- Twelve questions assessed participants’ sleep pattern and the usage of medications.
- Four questions assessed participants’ driving habits.
- Two questions assessed the presence and time of sleepy driving in the preceding six months.
- One question assessed if participant had to stop the car because of sleepiness.
- Three questions assessed the occurrence of sleep-related accidents, near-miss accidents, and any other causes of driving accidents. Accident types were classified as minor: defined as one or multiple scratches in the vehicle with injury not requiring medical attention or serious accident which led to hospitalization or death of either the driver or one of the passengers.
- Seven questions assessed the most frequently used techniques to counter sleepiness during driving, and the most effective way according to the drivers.
- Daytime sleepiness was assessed using the Epworth Sleepiness Scale (ESS).14
- Risk for obstructive sleep apnea was assessed using Berlin Questionnaire (BQ), all drivers included in the study were asked to complete the Berlin questionnaire (BQ). The presence of at least three symptom categories indicates a high likelihood of sleep disordered breathing.15
Sample Size Calculation
With an expected proportion of sleepy driving as 64.1%10 and absolute precision as 3%, the minimum required number of subjects for this study was 982, where Type 1 error is fixed as 5%. Formula used  , where p=0.641 and d=0.03. Hence, a sample size of a minimum of 1000 men and 1000 women was required for this study.
, where p=0.641 and d=0.03. Hence, a sample size of a minimum of 1000 men and 1000 women was required for this study.
Statistical Analysis
Continuous variables were summarized as mean ± standard deviation (SD) or median (IQR) according to the distribution of the data, while categorical variables were summarized using frequency and percentage (%). The Chi-square test was used to assess the significant association between categorical variables. In this study, we want to see the risk of occurrence of sleepy driving in male compared to female. Therefore, we used first univariable model to find the significance, then perform the multivariable model. Univariable and multivariable logistic regression analyses were used to assess significant factors associated with the outcome variable sleepy driving. Variable with p values <0.05 in univariable analysis were selected to design the most appropriate multivariable logistic regression model for each outcome variable. Adjusted odds ratios were presented with 95% confidence intervals (CIs). Variables included in the model after relevant statistical tests were gender, age, use of any type of medications, shift working, number of hours worked per day, driving duration per day, driving experience, excessive daytime sleepiness, and risk of having obstructive sleep apnea. A clustered bar plot was presented for the graphical representation of the results. Results were considered as statistically significant if P < 0.05. Data were analyzed using IBM SPSS Statistics 26 and StataSE 17.
Results
Out of 3272 who started the survey, 2958 (90%) participants completed it, of which 1414 (48%) were women, with no difference in completion rate between men and women. Seventy-five percent of the participants were 18–34 years old, presumably reflecting the recruitment strategy which relied on social media. The mean ESS score was 9.22 ± 4.3. The median (IQR) duration of driving per day of study participants was 3 hours (2–4 hours). Sleepy driving was mainly reported between the time of 1200 and 1600. Surprisingly, 867 (29.3%) of the surveyed drivers did not possess a driving license (11.5% men and 48.7% women).
Details of participants’ sociodemographic characteristics are presented in Table 1.
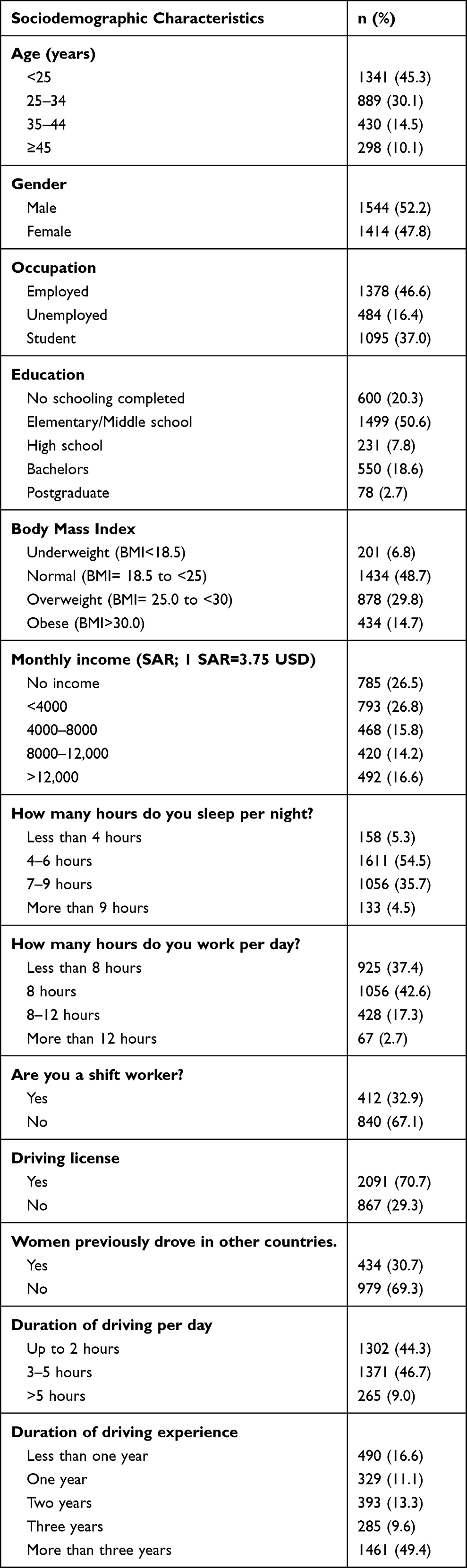 |
Table 1 Sociodemographic Characteristics of Study Participants (N=2958) |
Gender Difference in Prevalence of Sleepy Driving, Near-Miss Accidents, and Actual Accidents
The overall prevalence of sleepy driving in the preceding six months was 42% (men: 50% and women: 32%, p<0.001). In the preceding six months, participants reported the following: 12% they had to stop their vehicle due to sleepiness (men: 16.2% and women: 7%, p<0.001), 12.4% reported near-miss accidents (men: 16.2% and women: 8.2%, p<0.001) and 4.2% reported that they were in an actual vehicle accident caused by sleepiness (men: 4.3% and women: 4%, p=0.645). Most of these accidents were minor accidents (91.6%), compared to serious accidents (8.4%). The type of accident did not differ significantly between genders.
Univariable and Multivariable Analysis of Factors Associated with Sleepy Driving
In univariable analysis, younger age [OR 1.77 (95% CI 1.05–2.99); p=0.032)] Being a male [OR 2.1 (95% CI 1.81–2.44); p<0.001)], working 8 hours per day [OR 1.21 (95% CI 1.01–1.45); p<0.037)], driving duration of 3–5 hours per day [OR 1.76 (95% CI 1.50–2.05); p<0.001)], driving experience of more than 3 years [OR 4.51 (95% CI 3.52–5.79); p<0.001)], severe excessive daytime sleepiness [OR 1.78 (95% CI 1.35–2.36); p<0.001)], and high risk of obstructive sleep apnea [OR 2.12 (95% CI 1.73–2.59); p<0.001)] were all associated with sleepy driving in the preceding 6 months. There was no significant relationship between sleep duration and sleepy driving (p=0.357).
In multivariable analysis, younger age [OR 4.48 (95% CI 1.29–15.52); p=0.018)], being a male [OR 1.56 (95% CI 1.22–1.99); p<0.001)], using any type of medication [OR 1.61 (95% CI 1.21–2.13); p=0.001)], shift working [OR 1.64 (95% CI 1.26–2.13); p<0.001)] working more than 12 hours per day [OR 2.84 (95% CI 1.30–6.20); p<0.009)], driving duration of 3–5 hours per day [OR 1.31 (95% CI 1.02–1.69); p<0.035)], driving experience of more than 3 years [OR 4.51 (95% CI 3.52–5.79); p<0.001)], severe excessive daytime sleepiness [OR 1.64 (95% CI 1.03–2.61); p<0.036)], and high risk of obstructive sleep apnea, defined using the Berlin questionnaire [OR 2.37 (95% CI 1.73–3.25); p<0.001)] were all associated with sleepy driving in the preceding 6 months.
Table 2 shows binary logistic regression analyses of predictors for sleepy driving.
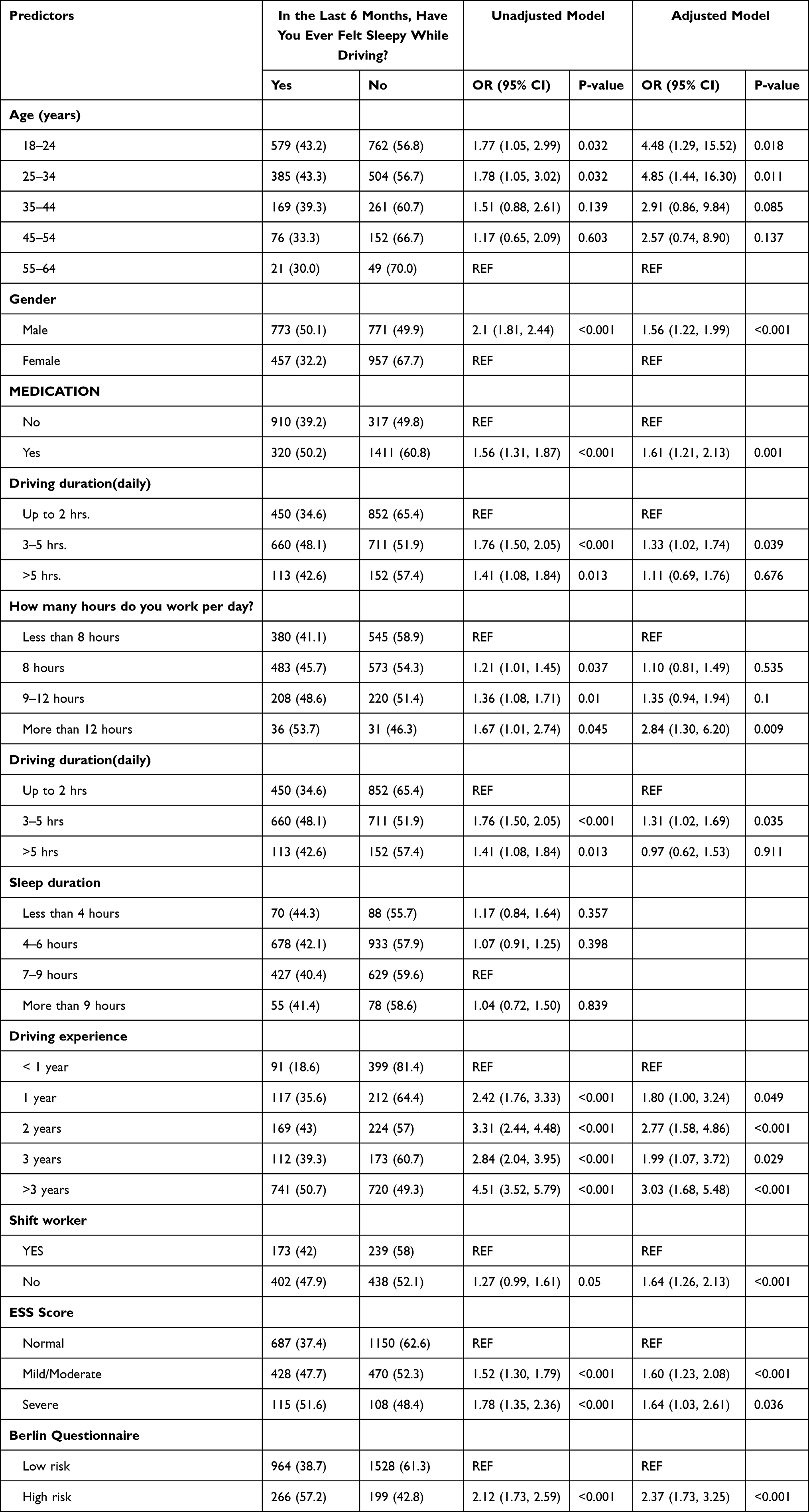 |
Table 2 Unadjusted and Adjusted Binary Logistic Regression Analyses of Predictors for Sleepy Driving |
Gender Differences of Association Between Risk of Sleep Apnea and Sleepy Driving
Using the Berlin questionnaire, 17% of men were judged at high risk of obstructive sleep apnea compared to 14% of women (p=0.018), with overall prevalence of 16%. The BQ determined risk of having obstructive sleep apnea was associated with an increased odds of being sleepy driving [OR 2.37 (95% CI 1.73–3.25); p<0.001)].
Figure 1 shows how participants countermeasure sleepiness while driving.
 |
Figure 1 Prevalence of countermeasure usage among men and women participants of the study. |
Discussion
Our data provide insight into gender differences of the prevalence of sleepy driving in Saudi Arabia. In line with prior work, sleepy driving was prevalent among both genders in Saudi Arabia but was higher in men than women. Male gender and positive responses to the Berlin questionnaire (indicating a high risk of obstructive sleep apnea) were strong predictors for sleepy driving.
Significance of the Findings
Our results revealed that the prevalence of sleepy driving was 50% among men and 32% among women, with overall prevalence of 42%. Two previous studies have assessed the prevalence of sleepy driving in Saudi Arabia in 2014 and 2021 and showed that the prevalence was 64%10 and 30%,6 respectively. These two studies report notable differences in prevalence compared to our findings, which can be explained by the methodology used, gender distribution and the sample size in each study. The prevalence in 2014 was conducted through interviews in hospitals, train stations, and waiting rooms of bus stations. It included men drivers only as women were not legally permitted to drive in Saudi Arabia before 2018. Likewise, the study by Alshareef in 2021 included only a small percentage of women drivers (13%). The sample size also varies somewhat between the two studies (1290 participants in 2014 vs 4708 participants in 2021). Despite these differences, a significant percentage of those sleepy drivers admits that they experienced actual accidents because of sleepiness (4%). This percentage might be underestimated due to recall bias or denial of accidents to avoid legal consequences; this requires further research.
Our results indicate that men are more likely to engage in sleepy driving than women. This is consistent with previous data in Saudi Arabia,6 gulf countries,16,17 Asian countries such as Australia,18 and 19 European countries.19 Furthermore, a large E-Survey of Road Users’ Attitudes reveal that self-declared fatigued driving rates are considerably higher for men drivers (24% to 28%) than for women drivers (15% to 21%) in Europe, North America and Africa.20 The reason behind this is still poorly understood, but one explanation may be that sleepiness, in general, is more common in men compared to women.21 Another explanation is that OSA is more prevalent in men compared to women, and this may justify these differences.
A diagnosis of Obstructive Sleep Apnea (OSA) is a major factor of experiencing sleepiness while driving.9 Consistent with previous findings, our study showed that positive responses to the Berlin questionnaire (indicating a high risk of obstructive sleep apnea) was associated with sleepy driving.22–24 The exact mechanism of sleepiness in patients with OSA is still under investigation. However, the combined effect of intermittent hypoxia and sleep fragmentation seems to be one of the convincing mechanisms.25 These lead to reduction of cognitive processing, reduced visual scanning ability, and microsleep, which all impact driving decision-making skills.26–28
There are many factors that can lead to sleepy driving such as age, sleep deprivation, medications, shift working and sleep disorders.8,29,30 Consistent with our findings, previous studies have shown that young drivers are more likely to engage in sleepy driving compared to older people. This might reflect a reduced perception of risk in young adults. In contrast to our findings, previous studies have shown that sleep deprivation was a main contributor to sleepy driving. Alabri et al 2018 showed that sleeping less than 6 hours per night was associated with sleepy driving in both men and women. Furthermore, it is estimated that 56,000 accidents in the United States each year were associated with sleep deprivation. However, other studies have shown that sleepy driving after sleep deprivation was not associated with excessive daytime sleepiness.31,32 Apart from sleep deprivation, there are number of factors that can lead to sleepy driving which include slow reaction time, reducing response accuracy, and attention deficit, all of which are of negative implications for safe driving.33
Our results also showed variable behavioral preferences toward countermeasures of sleepiness while driving; supportive of our overall conclusion every countermeasure was used more commonly by men than women. The method of choice in overcoming sleepiness while driving in our study was drinking coffee or tea, which previous studies have reported to be effective. A previous study demonstrated that one cup of caffeinated coffee (80 mg caffeine) enhances driving performance and lowers the driver’s sleepiness.34 Although listening to radio or music and opening the window to get air both were widely used, they appear to be ineffective to reduce sleepiness for extended time periods;35 moreover opening the window is not always feasible in Saudi Arabia. An alternative might be using the “LO” setting on the cars air-conditioning but this was not a question asked of participants. Few participants preferred to take a nap to overcome sleepiness while driving though it is the safest action as a countermeasure. According to Horne and Reyner, caffeine and napping considerably reduced subjective sleepiness, driving impairments, and EEG signs of drowsiness.36 There are other techniques that have proved to be effective to reduce sleepiness while driving. A previous study showed that in-car continuous exposure to blue light at nighttime reduces nocturnal drowsiness among sleepy drivers.37 However, the latter was not investigated in our study.
Critique of the Method
Our study contains several limitations. Cross-sectional studies are always prone to reporting bias, especially as this study assessed a sensitive topic such as driving behaviors which have legal consequences. However, as our findings did not largely deviate from previous studies, we assume that the risk of reporting bias was minimal. The high prevalence of respondents who admitted not having a driving license suggests that legal or privacy concerns were also not a significant issue for participants; however, it is a marker that the studied population may be atypical in some way.
Another limitation of our study was that we did not investigate the trip duration (short or long trip) nor road types (freeways, cities, and open roads). Different road types and trip duration can contribute differently to sleepiness while driving. Another limitation was that we did not ask specifically about the time when actual accidents occur as this seems to be associated with circadian rhythm variations. However, we did ask our participant about the times at which sleepy driving mainly occurred and we assume that accidents may occur at the same time as sleepy driving.
Nevertheless, this is the first study investigating the gender differences in sleepy driving in Saudi Arabia. Our findings extend previous findings that reported a high prevalence of sleepy driving and add to it the data around the countermeasures used against sleepiness among both genders. Future studies should investigate the cost analysis of sleepy driving and effectiveness of each countermeasure on overcoming sleepiness while driving.
Conclusion
Sleepiness while driving is widespread among drivers in Saudi Arabia. Factors associated with sleepy driving were risk of having obstructive sleep apnea, being a male, older age, employment, working 8 hours per day, driving duration of 3–5 hours per day, and driving experience of more than 3 years. Future public health initiatives should particularly focus on men with the aim of reducing gender imbalance in sleepy drivers.
Acknowledgment
The abstract of this paper was presented at the American Thoracic Society Conference 2023 as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in American Journal of Respiratory and Critical Care Medicine: Hyperlink: https://www.atsjournals.org/doi/abs/10.1164/ajrccm-conference.2023.207.1_MeetingAbstracts.A5845.
Disclosure
Dr Michael Polkey reports personal fees from Philips, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Saleem S. Risk assessment of road traffic accidents related to sleepiness during driving: a systematic review. East Mediterr Health J. 2022;28(9):695–700. doi:10.26719/emhj.22.055
2. World Health Organization. Regional Office for the Eastern M. Country Cooperation Strategy for WHO and Saudi Arabia 2012–2016. Cairo: World Health Organization. Regional Office for the Eastern Mediterranean; 2013.
3. Bioulac S, Micoulaud-Franchi J-A, Arnaud M, et al. Risk of motor vehicle accidents related to sleepiness at the wheel: a systematic review and meta-analysis. Sleep. 2017;40(10). doi:10.1093/sleep/zsx134
4. McNicholas WT. Sleepiness and Driving. Sleep Med Clin. 2019;14(4):491–498. doi:10.1016/j.jsmc.2019.08.006
5. Bonsignore MR, Randerath W, Schiza S, et al. European Respiratory Society statement on sleep apnoea, sleepiness and driving risk. Eur Respir J. 2020;57(2):2001272. doi:10.1183/13993003.01272-2020
6. AlShareef SM. Excessive daytime sleepiness and associations with sleep-related motor vehicle accidents: results from a nationwide survey. Sleep Breathing. 2020;25(3):1671–1676. doi:10.1007/s11325-020-02260-5
7. Nabi H, Guéguen A, Chiron M, Lafont S, Zins M, Lagarde E. Awareness of driving while sleepy and road traffic accidents: prospective study in GAZEL cohort. BMJ. 2006;333(7558):75. doi:10.1136/bmj.38863.638194.AE
8. Akerstedt T. Consensus statement: fatigue and accidents in transport operations. J Sleep Res. 2000;9(4):395. doi:10.1046/j.1365-2869.2000.00228.x
9. Luzzi V, Mazur M, Guaragna M, et al. Correlations of obstructive sleep apnea syndrome and daytime sleepiness with the risk of car accidents in adult working population: a systematic review and meta-analysis with a gender-based approach. J Clin Med. 2022;11(14):3971.
10. BaHammam AS, Alkhunizan MA, Lesloum RH, et al. Prevalence of sleep-related accidents among drivers in Saudi Arabia. Ann Thorac Med. 2014;9(4):236–241. doi:10.4103/1817-1737.140138
11. AlShareef SM. Excessive daytime sleepiness and associations with sleep-related motor vehicle accidents: results from a nationwide survey. Sleep Breath. 2021;25(3):1671–1676. doi:10.1007/s11325-020-02260-5
12. Thomas MJW, Gupta CC, Sprajcer M, et al. Fatigue and driving: an international review; 2021.
13. Sagaspe P, Taillard J, Bayon V, et al. Sleepiness, near-misses and driving accidents among a representative population of French drivers. J Sleep Res. 2010;19(4):578–584. doi:10.1111/j.1365-2869.2009.00818.x
14. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540–545. doi:10.1093/sleep/14.6.540
15. Netzer NC, Stoohs RA, Netzer CM, Clark K, Strohl KP. Using the Berlin Questionnaire to identify patients at risk for the sleep apnea syndrome. Ann Internal Med. 1999;131(7):485. doi:10.7326/0003-4819-131-7-199910050-00002
16. Al-Abri MA, Al-Adawi S, Al-Abri I, et al. Daytime sleepiness among young adult Omani car drivers. Sultan Qaboos Univ Med J. 2018;18(2):e143–e148. doi:10.18295/squmj.2018.18.02.004
17. Al-Houqani M, Eid HO, Abu-Zidan FM. Sleep-related collisions in United Arab Emirates. Accid Anal Prev. 2013;50:1052–1055. doi:10.1016/j.aap.2012.08.010
18. Obst P, Armstrong K, Smith S, Banks T. Age and gender comparisons of driving while sleepy: behaviours and risk perceptions. Transport Res Part F. 2011;14(6):539–542. doi:10.1016/j.trf.2011.06.005
19. Gonçalves M, Amici R, Lucas R, et al. Sleepiness at the wheel across Europe: a survey of 19 countries. J Sleep Res. 2015;24(3):242–253. doi:10.1111/jsr.12267
20. Goldenbeld C, Nikolaou D. Driver fatigue. ESRA2 thematic report Nr. 4. ESRA project (E-Survey of Road users’ Attitudes). The Hague, Netherlands Institute for Road safety Research SWOV; 2019.
21. Pérez-Carbonell L, Mignot E, Leschziner G, Dauvilliers Y. Understanding and approaching excessive daytime sleepiness. Lancet. 2022;400(10357):1033–1046. doi:10.1016/s0140-6736(22)01018-2
22. Lévy P, Kohler M, McNicholas WT, et al. Obstructive sleep apnoea syndrome. Nat Rev Dis Primers. 2015;1(1). doi:10.1038/nrdp.2015.15
23. Devita M, Montemurro S, Zangrossi A, et al. Cognitive and motor reaction times in obstructive sleep apnea syndrome: a study based on computerized measures. Brain Cognit. 2017;117:26–32. doi:10.1016/j.bandc.2017.07.002
24. George CFP. Sleep 5: driving and automobile crashes in patients with obstructive sleep apnoea/hypopnoea syndrome. Thorax. 2004;59(9):804–807. doi:10.1136/thx.2003.007187
25. Bucks RS, Olaithe M, Rosenzweig I, Morrell MJ. Reviewing the relationship between OSA and cognition: w here do we go from here? Respirology. 2017;22(7):1253–1261. doi:10.1111/resp.13140
26. Zhang X, Zhao X, Du H, Rong J. A study on the effects of fatigue driving and drunk driving on drivers’ physical characteristics. Traff Injury Prevent. 2014;15(8):801–808. doi:10.1080/15389588.2014.881996
27. Lucidi F, Russo PM, Mallia L, Devoto A, Lauriola M, Violani C. Sleep-related car crashes: risk perception and decision-making processes in young drivers. Accid Anal Prev. 2006;38(2):302–309. doi:10.1016/j.aap.2005.09.013
28. Thorpy M. International classification of sleep disorders. In: Sleep Disorders Medicine. Springer; 2017:475–484.
29. Daroff RB. The international classification of sleep disorders: diagnostic and coding manual. Neurology. 1991;41(1):160. doi:10.1212/wnl.41.1.160
30. Leibowitz SM, Lopes M-C, Andersen ML, Kushida CA. Sleep deprivation and sleepiness caused by sleep loss. Sleep Med Clin. 2006;1(1):31–45. doi:10.1016/j.jsmc.2005.11.010
31. Van Dongen HP, Maislin G, Mullington JM, Dinges DF. The cumulative cost of additional wakefulness: dose-response effects on neurobehavioral functions and sleep physiology from chronic sleep restriction and total sleep deprivation. Sleep. 2003;26(2):117–126. doi:10.1093/sleep/26.2.117
32. Cai AWT, Manousakis JE, Singh B, et al. On-road driving impairment following sleep deprivation differs according to age. Sci Rep. 2021;11(1):21561. doi:10.1038/s41598-021-99133-y
33. Lim J, Dinges DF. Sleep deprivation and vigilant attention. Ann N Y Acad Sci. 2008;1129(1):305–322. doi:10.1196/annals.1417.002
34. Mets MAJ, Baas D, van Boven I, Olivier B, Verster JC. Effects of coffee on driving performance during prolonged simulated highway driving. Psychopharmacology. 2012;222(2):337–342. doi:10.1007/s00213-012-2647-7
35. Schwarz JFA, Ingre M, Fors C, et al. In-car countermeasures open window and music revisited on the real road: popular but hardly effective against driver sleepiness. J Sleep Res. 2012;21(5):595–599. doi:10.1111/j.1365-2869.2012.01009.x
36. Horne JA, Reyner LA. Counteracting driver sleepiness: effects of napping, caffeine, and placebo. Psychophysiology. 1996;33(3):306–309. doi:10.1111/j.1469-8986.1996.tb00428.x
37. Taillard J, Capelli A, Sagaspe P, Anund A, Akerstedt T, Philip P. In-car nocturnal blue light exposure improves motorway driving: a randomized controlled trial. PLoS One. 2012;7(10):e46750. doi:10.1371/journal.pone.0046750
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.