")
Back to Journals » Orthopedic Research and Reviews » Volume 16
External Fixation as a Primary and Definitive Treatment for Complex Tibial Diaphyseal Fractures: An Underutilized and Efficacious Approach
Authors Albushtra A , Mohsen AH, Alnozaili KA, Ahmed F , Aljobahi YMAA , Mohammed F , Badheeb M
Received 20 November 2023
Accepted for publication 18 February 2024
Published 21 February 2024 Volume 2024:16 Pages 75—84
DOI https://doi.org/10.2147/ORR.S450774
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Ahmed Albushtra,1 Abdulsalam Hadi Mohsen,2 Khaled Ali Alnozaili,3 Faisal Ahmed,4 Younes Mohsen Ali Abdu Aljobahi,1 Fawaz Mohammed,1 Mohamed Badheeb5
1Department of Orthopedic, School of Medicine, Ibb University, Ibb, Yemen; 2Department of Orthopedic, School of Medicine, Aden University, Aden, Yemen; 3Department of Orthopedic, School of Medicine, 21 September University, Sana’a, Yemen; 4Department of Urology, School of Medicine, Ibb University, Ibb, Yemen; 5Department of Internal Medicine, Yale New Haven Health, Bridgeport Hospital, Bridgeport, CT, USA
Correspondence: Faisal Ahmed, Department of Urology, School of Medicine, Ibb University, Ibb, Yemen, Tel/Fax +967 4428950, Email [email protected]
Background: External fixation is one of the most often utilized treatment options for complicated tibial diaphyseal fractures (TDF). The purpose of this study was to assess the efficacy of unilateral external fixators as primary and definitive therapy for complex TDF in a resource-limited setting.
Materials and Methods: A retrospective study between June 2016 and March 2021 included 110 subjects with TDF who were treated with an external fixator as definitive fixation in hospitals affiliated with Ibb University. The patient’s demographic characteristics, complications, and outcomes were gathered and analyzed. Factors associated with pin site infection were also investigated.
Results: The mean age was 42.1 ± 10.1 years, with 92.7% being male. Rural residents accounted for 22.7%. Smoking and diabetes mellitus were present in 27.3% and 30.0%, respectively. General complications occurred in 12.0%, with pulmonary embolism being the most common at 4.5%. Orthopedic complications included pin-track infections in 27.3% (30) and osteomyelitis in 1.8% (2). Pin site infections required medical treatment in 21 cases and external fixator changes in five. Two cases each needed several debridements for osteomyelitis and soft tissue. Full union occurred in 79.1% (87) over 23.1 ± 3.2 weeks and final alignment in 97.3% (107) over 34.8 ± 4.8 weeks. Malunions occurred in 1.8% (2), and one case had hypertrophic nonunion. Factors like rural residency, smoking, diabetes, open fractures, worst fracture grade (Gustilo and Anderson type C), and general complications occurrence significantly correlated with pin site infection (all p-values < 0.05).
Conclusion: A unilateral external fixator as a primary and definitive treatment is a viable, simple, and effective option for TDF with a high success rate even in a resource-limited setting. In this study, residents in rural areas, smoking, diabetes, open fracture, worst fracture grade, and general complication occurrence were associated with pin site infection occurrence.
Keywords: external fixation, definitive treatment, tibial fractures, pin tract infection
Introduction
The tibial diaphysis represents one of the most frequently fractured long bones, influenced by the anatomical location that exposes it to a higher incidence of trauma, particularly from road traffic accidents.1 Such injuries often involve additional soft tissue or damage to the neurovascular bundle.2 Furthermore, there is an increased incidence of associated complications with tibial diaphyseal fractures (TDF), such as malunion, non-union, pin-track infections, and the consequent necessity for surgical re-intervention, emphasizing the importance for optimized initial therapeutic strategies.1
Despite the relatively high incidence of TDF, their management remains subject to debate. A spectrum of interventions is currently employed, including intramedullary nailing (IMN), plates and screws, external fixation, and others.3 While IMN has gained precedence as the preferred modality in the majority of TDF cases, its application is constrained in the context of complex fracture types (eg, type III), which necessitate adjunctive soft tissue reconstruction and neurovascular intervention, or when accompanied by multilevel fractures or compartment syndrome.4
External fixation was extensively used in the early twentieth century; however, it was reportedly less efficacious and associated with higher complication rates compared to IMN in several retrospective and prospective studies.5–8 These studies, however, are potentially limited by a high risk of biases, heterogeneity, and poor precision. Thus, it can be assumed that external fixation in TDF can be relatively underutilized, which can be influenced by its less favorable physical aesthetics and the associated psychological distress.9
Despite the significant burden of TDF within our national context, the application of this technique has not been extensively investigated, to our knowledge. Thus, we aimed to assess the outcome of unilateral external fixators in the definitive management of TDF within a resource-limited setting.
Materials and Methods
Study Design
This retrospective study included TDF that were managed within Ibb University-affiliated hospitals, within a time period of June 2016 to March 2021, including 111 cases that were managed with unilateral external fixators, with ethical approval obtained via the Ibb University’s ethics committee in adherence to the Declaration of Helsinki.
Inclusion Criteria
We included all patients with TDF (Gustilo and Anderson class I–III), and polytrauma patients with an Injury Severity Score (ISS) ≥16 who were managed in Ibb University-affiliated hospitals.
Exclusion Criteria
Patients older than 70 years, or the presence of any of the following; pathological fracture, concomitant vertebral, femoral, or intra-articular fractures, spinal cord injury, bone deficits, or if were treated initially in a prior healthcare facility that is not afflicted with Ibb University, were excluded from the study.
Preoperative Assessment
Initial preoperative evaluation included a primary survey aiming to stabilize cervical injuries, airway, and hemodynamics. Subsequent evaluation was focused on identifying skeletal injuries with any concomitant vascular, neurological, or soft tissue injuries, prioritizing managing immediately life-threatening injuries. TDF was typically evaluated with plain radiography, and involved limbs were immobilized in the form of above knee plaster of Paris posterior slab and limb elevation for all patients and the preparation for operation according to the indications. Typically, the surgical intervention if needed was performed within 8 hours, and the broad-spectrum antibiotics coverage was provided for all the operatively-managed patients.
Operative Techniques
All the cases were managed under general anesthesia. The initial operative approach included meticulous irrigation and debridement for any contaminated or necrotic soft tissue. The fractures and soft tissues were reduced manually under fluoroscopic guidance, and uniplanar AO-type external fixators (Hoffmann II External Fixation System, Stryker Corporation, Kalamazoo, Michigan, USA) were utilized. After drilling, at least three 5.0 mm cortical Schanz screws with radial preload were manually inserted with a T handle in each proximal and distal end of the tibia for external fixator application. If the fracture pattern permitted, attempts were made to avoid the cancellous area of the upper and lower ends of the tibia; otherwise, 6mm cancellous Schanz screws were used.
With the help of AO clamps, two connecting rods were connected to the Schanz screw after manual reduction while maintaining length, axial, and rotational alignment. More Schanz screws were fixed and connected to the rod with clamps on either end of the fracture if more stability was required. Axial loading was performed for simple transverse and short oblique fractures by unlocking the clamp pins’ pin to rod nuts and refixing it in bending stress towards the fracture for pins closer to the fracture and bending stress away from the fracture for far pins. Pins were subjected to bending stress in the opposite direction for comminuted fractures. More specific instructions on the structure and functioning principles of the ASC were mentioned in previous reports.10,11
Postoperative Care
Postoperatively, systemic antibiotics were continued for five days (Cefazolin I gr every 8 hours), dressings were done regularly, and the wound was left alone to heal, with secondary intention and dressings.
Depending on the patient’s pain tolerance, patients were encouraged to achieve knee and ankle range of motion (ROM). Axial dynamization and loading were individualized and began once the patient was painless when walking or could walk with minimal assistance. Weight-bearing was encouraged following dynamization. Patients were routinely monitored. Once the clinical or radiological union was achieved, ie, no pain or mobility at the fracture site and union in three cortices in anteroposterior and lateral views, the external fixator frame was removed, and the patient was placed in a patellar tendon bearing (PTB) cast for an additional six weeks to consolidate the union. The functional rehabilitation program was recommended for all patients in our rehabilitation units.
Data Collection
Age, gender, residency, mechanism of trauma, fracture score by AO/OTA Classification, open fracture score by Gustilo and Anderson’s classification (I, II & III),12 type of fracture (open or closed), comorbidities such as diabetes and current smoking history, time to union, final alignment, postoperative orthopedic complications including pin-site infection, osteomyelitis, and deep infection according to Checketts–Otterburn grading system [minor infection (CO 1–3) and major infection (CO 4–6)], nonunion, malunion, reoperations, and postoperative medical complications including deep venous thrombosis, pulmonary thromboembolism, and fat embolism.
Pin Site Infection Care and Management Strategy
For patients with pin site reactions, limiting activity, reducing weight bearing, and using oral antibiotics were recommended. If the symptoms persist or had a pin site infection, pin cultures were performed, followed by empiric antibiotics. Radiographs were collected for pin loosening in chronic infections, and antibiotics were administered based on culture findings. If radiographs do not show a half-pin loosening, the pin was removed from the frame and examined, and loose pins were promptly removed. After removing essential pins, patients were taken to the operating room for frame modification, debridement, and IV antibiotics if cellulitis was present. Patients with profound infections were monitored for osteomyelitis symptoms. Typically, removing the foreign body was enough to treat the infection, but magnetic resonance imaging (MRI) was acquired to determine the need for further debridement.
Definitions
Fracture Union
A duration of 6 months or less was considered a normal healing period. The extension of healing beyond 6 months but less than 8 months was considered delayed union, whereas non-union was defined as a lack of healing beyond 8 months. In regards to fracture alignment, the presence of varus or valgus misalignment of 50 degrees, anteroposterior misalignment of more than 100 degrees, or shortening of more than 1 inch were used to define malunion.
Pin-Track Infection and Deep Infection
Checketts–Otterburn system13 was used to grade pin-track infection, categorized into minors and major grades. Minor category, not necessitating surgical re-intervention, includes score 0: normal healthy appearance, score 1: discharge, score 2: Red, discharge, and score 3: Red, discharge. Major categories, generally precluding the use of external fixation, include score 4: Pin loose, score 5: Osteomyelitis in pin tract, and score 6: Osteomyelitis requiring curettage.
Main Outcome
Healing duration, union complications, and eventual alignment were identified as the primary end-point. While factors associated with pin-track infections were the secondary end-point outcomes of the study.
Statistical Analysis
IBM SPSS version 22 software (IBM Corp., Armonk, New York) was used for statistical analyses. For quantitative data, mean and standard deviation were utilized, whereas frequency and percentage were employed for qualitative variables. To examine the association between nominal and categorical variables with pin-site infections, the chi-square test was utilized. A p-value of 0.05 or less was judged statistically significant.
Results
In this study, 111 patients were diagnosed with complicated TDF, with one case having a pre-operative death secondary to pulmonary embolism. The average age of patients was 42.1 ± 10.1 years, ranging from 22 to 66 years. A significant proportion, 102 (92.7%), were male, and 25 (22.7%) originated from rural areas. Smoking history was present in 30 (27.3%) patients, while 33 (30.0%) had a history of diabetes mellitus. Further patients’ demographic details are elaborated in Table 1. The leading cause of TDF in this group was motor vehicle accidents, accounting for 81 (73.6%) cases. Open fractures were the most common type of TDF, noted in 92 (83.6%) cases. Based on the Gustilo and Anderson classification, type C fractures were the most prevalent, observed in 45 (48.9%) cases, followed by type B in 36 (39.1%) cases.
 |
Table 1 Patient Demographic Characteristics with Complicated Tibial Shaft Fractures |
All the patients were treated with a simple external fixator (Figure 1). Successful union was achieved in 87 (79.1%) patients, with an average healing period of 23.1 ± 3.2 weeks (range 18–32 weeks). This included 71 (64.5%) cases with normal healing and 34 (30.9%) with delayed union. Nonunion, indicating an absence of healing, was seen in 5 (4.5%) cases, while malunion occurred in 3 (2.7%) cases. Regarding orthopedic complications, there were 30 (27.3%) cases of pin-track infections and 2 (1.8%) of osteomyelitis. Pin site infections were medically treated in 21 cases, and 5 cases required reoperations for either nail or external fixator changes. Two cases with osteomyelitis needed multiple-bone debridements, and another two required multiple debridements of soft tissue, as detailed in Table 2. General complications were noted in 11 (12.0%) cases, including fat embolism (2 cases, 1.8%), pulmonary embolism (5 cases, 4.5%), and deep venous thrombosis (4 cases, 3.6%).
 |
Table 2 Postoperative Characteristics and Outcome |
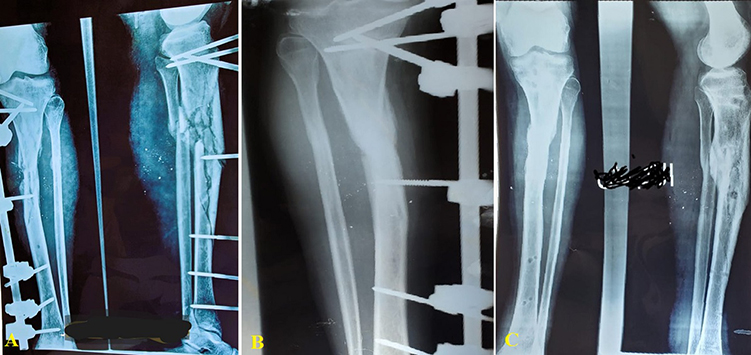 |
Figure 1 Open segmental tibial shaft fracture treated by external fixation method; (A) plain X-ray after injury (AP view and lateral views), (B) X-ray (AP view) 3 months after the injury, (C) X-ray (AP and lateral views) 6 months after the surgery. |
At the final follow-up, averaging 34.8 ± 4.8 weeks (range 29–44 weeks), proper alignment was achieved in 107 (97.3%) cases. There were 2 (1.8%) instances of malunion with tibial shortening and one case of hypertrophic nonunion with a shortening between 1.5 and 2 cm. In terms of knee and ankle joint movement and pain, there were no restrictions, and no patients reported pain at the final follow-up.
Factors Associated with Pin Track Infection
Rural residence, active smoking, history of diabetes mellitus, open fracture, worst grade of open fracture according to Gustilo and Anderson (type C), and general complication occurrence were associated with pin track infection and were statistically significant (Table 3).
 |
Table 3 Factors Associated with Pin-Track Infections |
Discussion
In this study, we evaluate the effectiveness of unilateral external fixators as the primary and definitive treatment for complex TDF in resource-limited settings. Additionally, we explore factors associated with pin tract infections. To our knowledge, this is the first study to use unilateral external fixation as the sole treatment for complex tibial fractures in Yemen. Similar recent published reports were mentioned by Beltsios et al in Greece,1 and in Pakistan by Makhdoom et al.14
The management of complicated TDF presents significant clinical challenges. The inconsistency in treatment guidelines, combined with the heightened risk of severe complications leading to functional impairment in predominantly young patients, further complicates TDF management. Various treatments, including IMN, external fixation, open reduction internal fixation (ORIF), minimally invasive plate osteosynthesis (MIPO), and even non-operative methods, have been explored for TDF management.3 Nonetheless, there is no consensus on treatment preference, which is often influenced by factors such as surgeon experience, device availability, and patient costs.3 External fixation, traditionally a common method for TDF management, is favored for its affordability, relatively simpler application, and fewer iatrogenic complications. However, postoperative complications, including pin-tract infections, instability, and unsuitability for osteoporotic bones, have led many physicians to favor IMN.15 This perspective was corroborated by a clinical trial conducted by Holbrook et al, which encompassed 60 patients, and demonstrated that IMN was non-inferior to external fixation for treating TDF, excluding grade III injuries.8 Subsequently, IMN was posited as superior to external fixation in analogous clinical contexts, as evidenced by a trial involving 174 patients.7 More recently, a meta-analysis by Giovannini et al6 illustrated more favorable outcomes in terms of infection rates with IMN compared to external fixation, even when considering patients with complex TDF (ie, class III).5 However, it is crucial to note that the latter study’s evidence is characterized by low or very low confidence, marked incoherence, and a high risk of bias.
While IMN is often considered a safer alternative for the management of complicated TDF, with soft tissue injuries, it has been shown to be associated with an elevated risk for septic pin-track infection and nonunion.16,17 Subsequently, delayed reamed IMN was advocated, under the presumption that earlier nailing is associated with increased complications, particularly in complicated TDF.17,18 Furthermore, reamed nailing, purported to offer greater stability, received support from a meta-analysis conducted by Bhandari et al, which demonstrated superior outcomes and lower failure rates with reamed IMN.19 These findings, however, have been a subject of debate due to concerns over high levels of bias and methodological flaws. A subsequent randomized clinical trial, involving 1319 patients with TDF, suggested a potential advantage of reamed IMN for closed TDF. However, it failed to establish a significant difference in outcomes for open TDF.20 This conclusion was further echoed in a later meta-analysis by Xue et al.21
Conversely, external fixation can represent a suitable approach in specific settings, particularly when availability, cost, or emergent intervention is taken into consideration, as shown by Cardozo et al.22 This study also underscored the advantages of IMN as an initial treatment strategy in cases where delayed internal osteosynthesis is anticipated. However, in low-income countries, the practical application of this strategy is frequently constrained by factors like the higher costs associated with re-operation, loss of follow-up, and the limited availability of health facilities capable of providing such interventions.15 Furthermore, it has been shown that external fixation can yield satisfactory outcomes even without transitioning to internal osteosynthesis.22 In fact, a study by Giannoudis noted an increased incidence of infections following the conversion from external fixation to internal osteosynthesis in cases of open TDF.4 Consequently, external fixation is recommended as a definitive treatment option, as it eliminates the necessity for a second surgical procedure, thereby indirectly reducing patient burdens associated with awaiting surgery and avoiding the risks linked to subsequent operations and anesthesia.1,15 Further reinforcing this perspective, a prospective study in Guinea found external fixation to be a suitable, safe, and effective method for managing various types of TDF, particularly lower-grade fractures.23
In this study, the full union was achieved in 87 (79.1%) patients, within a mean duration of 23.1 ± 3.2 weeks (ranging from 18 to 32 weeks). This finding is closely aligned with an Indian study, which documented a union rate of 87.7% within an average of 22.4 weeks (ranging from 15 to 29 weeks), suggesting that both studies likely involved comparable patient and environmental factors.15 Overall, there were 34 (30.9%) delayed unions 5 (4.5%) nonunions, and 3 (2.7%) malunion, in our study. Notably, we had an overall higher delayed union rate compared to prior reports, for instance, Jain et al15 reported delayed union at about 19%, compared to 21% in a prospective study by Holbrook et al8 while Beltsios et al reported as low as 9.5%.1 Nevertheless, we observed a lower union and malunion comparatively.8,24 These discrepancies could be attributed to the variability in clinical settings, duration of follow-up, and, most crucially, the characteristics of the patients and the incidence of TDF in each respective study.
While our study did not examine IMN, there is a lack of consistency in IMN complication rates compared to external fixation. Allegedly, IMN complications are purported to be less frequent than external fixation; however, this assertion warrants cautious interpretation. For instance, Lin et al25 reported a lower incidence of malunion with IMN (2%) versus external fixation (15%). However, these findings must be carefully considered, as the IMN group had approximately 2.5 times more patients than the external fixation group. Additionally, higher rates of comminution and open fractures were observed in the external fixation group. The relatively higher percentage of complications in these studies may suggest potential issues with patient selection and an increased risk of bias.
In our study, the incidence of pin site infection was 27.3%, which is higher than the 22.8% reported in the series by Jain et al15 but lower than the 59.1% noted by Abalo et al.26 Most of these infections (20 cases) were minor, classified as either grade 1, 2, or 3 according to the Checketts-Otterburn classification system, and were successfully treated with antibiotics. Only 10 cases (9.1%) experienced major infections, as defined by the Otta classification for pin site infection, necessitating pin revision due to loosening in five instances. Two cases involved osteomyelitis requiring multiple debridements of bone, and another two necessitated several soft tissue debridements. The relatively low incidence of major pin site infections in our study is attributed to meticulous pin insertion techniques, a limited follow-up period, preloading, and adequate care and dressing of the pin site. It is important to note that pin site infection rates can vary significantly across different regions, largely influenced by surgical techniques, staff proficiency, and the cleanliness standards of operating theaters.
Regarding the fracture type, reported infection rates range from 0 to 6% in closed tibia fractures and 12–65% in open tibia fractures.27 Similarly, our result showed that pin-site infection was common in open tibial shaft fractures and was a predictor for pin-site infection. A study of 68 closed tibial shaft fractures treated with an anterior unilateral external fixator over five years found that pin tract drainage and infection were common, leading to 61 secondary operations during healing. All fractures healed within 22 weeks, with three refractures. Functional results were excellent in 41%, good in 46%, and acceptable in 13% at follow-up. The poor results are probably due to weight-bearing being too high in these patients relative to the mechanical stability provided by the external fixator system.24
In this study, residents in the rural area, currently smoking, history of diabetes mellitus, open fracture type, worst grade of open fracture according to Gustilo and Anderson (type C), and general complication occurrence were associated with pin site infections and were statistically significant. These findings, generally, affirm the previously reported observations. For instance, smoking has been associated with overall poor healing, a higher risk of prolonged healing time, nonunion, and pin site infections28 — findings that have been extensively reported in prior studies, according to the authors. Counterintuitively, a meta-analysis by Fridberg et al found no correlation between pin-site infection and factors such as smoking, age, or body mass index.29 However, it did note a heightened risk of pin-site infections among patients with poorly controlled diabetes. Previous studies have also identified the time to definitive fixation, time to soft tissue closure, and wound contamination as factors associated with osteomyelitis.30 On the other hand, Penn-Barwell et al observed no significant relationship between the severity of injury, the mechanism of injury, the use of an external fixator, the necessity for vascularized tissue transfer, smoking status, and subsequent infection, except for bone loss, which was significantly linked to subsequent infection.31 Most consistently, the higher Gustilo-Anderson classification, particularly class C, has been consistently identified as the most robust predictor of pin site infections and osteomyelitis.30
In another study, Biz et al studied the long-term outcomes and complications of Ilizarov bone transport in 72 patients with isolated tibial fractures (with bone defects or tibial deformities). They found a cumulative rate of 55.6% during the first 36 months and 66.7% at 180 months. They concluded that Ilizarov bone transport is effective for definitive treatment, with most complications occurring within the first 3 years.32 These observations have been echoed in other studies as well.33,34 Overall, predicting outcomes for TDF requires the consideration of multiple confounding factors, including the nature and mechanics of the fracture, as well as intra-operative complications such as blood loss and the surgical approach utilized. To enhance our understanding, further prospective studies are imperative.
Study Limitations
This study was constrained by several limitations, including its retrospective design, which inherently lacked control and randomization. This approach is prone to selection bias and attrition due to loss of follow-up, potentially skewing the results. Furthermore, the small sample size diminishes the statistical power and validity of the conclusions drawn. The assessment of secondary outcomes was also limited, lacking adjustments for critical external factors such as pin care, the pin-bone interface of the external fixator, and the number of pins used in each fracture. Also, we do not have information on the requirement for adjunct treatments (such as soft tissue covering) or plastic surgery involvement in wound care, which can influence the infection rate. This omission could lead to an incomplete understanding of the factors influencing treatment outcomes.
Conclusion
A unilateral external fixator a primary and definitive treatment is a viable, simple, and effective option for complicated tibia shaft fractures with a high success rate even in a resource-limited setting. In this study, residents in rural areas, currently smoking, history of diabetes mellitus, open fracture, worst grade of open fracture according to Gustilo and Anderson (type C), and general complication occurrence were associated with pin site infection occurrence.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The Ibb University’s ethics committee approved the study protocol and all patients provided informed consent before enrolment and the study was complies with the Declaration of Helsinki.
Consent for Publication
All authors reviewed the manuscript and approved its submission.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Beltsios M, Savvidou O, Kovanis J, Alexandropoulos P, Papagelopoulos P. External fixation as a primary and definitive treatment for tibial diaphyseal fractures. Strategies Trauma Limb Reconstr. 2009;4(2):81–87. doi:10.1007/s11751-009-0062-3
2. Penn-Barwell JG, Bennett PM, Fries CA, Kendrew JM, Midwinter MJ, Rickard RF. Severe open tibial fractures in combat trauma: management and preliminary outcomes. Bone Joint J. 2013;95-b(1):101–105. doi:10.1302/0301-620X.95B1.30580
3. French B, Tornetta P. High-energy tibial shaft fractures. Orthop Clin North Am. 2002;33(1):211–230, ix. doi:10.1016/S0030-5898(03)00081-6
4. Giannoudis PV, Papakostidis C, Roberts C. A review of the management of open fractures of the tibia and femur. J Bone Joint Surg Br. 2006;88(3):281–289. doi:10.1302/0301-620X.88B3.16465
5. Foote CJ, Guyatt GH, Vignesh KN, et al. Which surgical treatment for open tibial shaft fractures results in the fewest reoperations? A network meta-analysis. Clin Orthop Relat Res. 2015;473(7):2179–2192. doi:10.1007/s11999-015-4224-y
6. Giovannini F, de Palma L, Panfighi A, Marinelli M. Intramedullary nailing versus external fixation in Gustilo type III open tibial shaft fractures: a meta-analysis of randomised controlled trials. Strategies Trauma Limb Reconstr. 2016;11(1):1–4. doi:10.1007/s11751-016-0245-7
7. Henley MB, Chapman JR, Agel J, Harvey EJ, Whorton AM, Swiontkowski MF. Treatment of type II, IIIA, and IIIB open fractures of the tibial shaft: a prospective comparison of unreamed interlocking intramedullary nails and half-pin external fixators. J Orthop Trauma. 1998;12(1):1–7. doi:10.1097/00005131-199801000-00001
8. Holbrook JL, Swiontkowski MF, Sanders R. Treatment of open fractures of the tibial shaft: ender nailing versus external fixation. A randomized, prospective comparison. J Bone Joint Surg Am. 1989;71(8):1231–1238. doi:10.2106/00004623-198971080-00017
9. Gasser B, Tiefenboeck TM, Boesmueller S, Kivaranovic D, Bukaty A, Platzer P. Damage control surgery - experiences from a level I trauma center. BMC Musculoskelet Disord. 2017;18(1):391. doi:10.1186/s12891-017-1751-6
10. Hao ZC, Xia Y, Wu JH, Zhang YT, Xu SG. Application of a Ni-Ti arched shape-memory connector in unstable lateral malleolus fractures: a retrospective study. Injury. 2019;50(2):551–557. doi:10.1016/j.injury.2018.10.037
11. Hao ZC, Xia Y, Xia DM, Zhang YT, Xu SG. Treatment of open tibial diaphyseal fractures by external fixation combined with limited internal fixation versus simple external fixation: a retrospective cohort study. BMC Musculoskelet Disord. 2019;20(1):311. doi:10.1186/s12891-019-2679-9
12. Thakore RV, Francois EL, Nwosu SK, et al. The Gustilo-Anderson classification system as predictor of nonunion and infection in open tibia fractures. Eur J Trauma Emerg Surg. 2017;43(5):651–656. doi:10.1007/s00068-016-0725-y
13. Checketts RG, MacEachem AG, Otterbum M. Pin track infection and the principles of pin site care. In: De Bastiani G, Apley AG, Goldberg A, editors. Orthofix External Fixation in Trauma and Orthopaedics. London: Springer London; 2000:97–103.
14. Makhdoom AU, Shaikh BJ, Baloch RA, Malah HR, Tunio ZH, Jokhio MF. Management of segmental fracture of tibia treated by Ilizarov external fixation. J Ayub Med Coll Abbottabad. 2020;32(3):291–294.
15. Jain S, Patel P, Gupta S. External fixator as a definitive treatment for tibial diaphyseal fractures. Orthopaedic J M P Chapter. 2020;26(1):34–39.
16. Alhammoud A, Maaz B, Alhaneedi GA, Alnouri M. External fixation for primary and definitive management of open long bone fractures: the Syrian war experience. Int Orthop. 2019;43(12):2661–2670. doi:10.1007/s00264-019-04314-0
17. Wang X, Wang B, Hou X, Cheng X, Zhang T. Unilateral external fixator combined with lateral auxiliary frame for ultimate treatment of tibia and fibula shaft fractures with poor soft tissue conditions. Biomed Res Int. 2022;2022:9990744. doi:10.1155/2022/9990744
18. McMahon SE, Little ZE, Smith TO, Trompeter A, Hing CB. The management of segmental tibial shaft fractures: a systematic review. Injury. 2016;47(3):568–573. doi:10.1016/j.injury.2015.11.022
19. Bhandari M, Guyatt GH, Tong D, Adili A, Shaughnessy SG. Reamed versus nonreamed intramedullary nailing of lower extremity long bone fractures: a systematic overview and meta-analysis. J Orthop Trauma. 2000;14(1):2–9. doi:10.1097/00005131-200001000-00002
20. Bhandari M, Guyatt G, Tornetta P, et al. Randomized trial of reamed and unreamed intramedullary nailing of tibial shaft fractures. J Bone Joint Surg Am. 2008;90(12):2567–2578. doi:10.2106/JBJS.G.01694
21. Xue D, Zheng Q, Li H, Qian S, Zhang B, Pan Z. Reamed and unreamed intramedullary nailing for the treatment of open and closed tibial fractures: a subgroup analysis of randomised trials. Int Orthop. 2010;34(8):1307–1313. doi:10.1007/s00264-009-0895-x
22. Cardozo RT, Silva LG, Bragante LA, Rocha MA. Treatment of fractures of the tibial diaphysis using external fixator compared with locked intramedullary nails. Rev Bras Ortop. 2013;48(2):137–144. doi:10.1016/j.rbo.2012.09.002
23. Keita D, de l’Escalopier N, Lamah L, et al. Tibia fracture management in low-resource settings using the external fixation and traction device of the Guinean military health service. Orthop Traumatol. 2022;108:103377.
24. Emami A, Mjöberg B, Karlström G, Larsson S. Treatment of closed tibial shaft fractures with unilateral external fixation. Injury. 1995;26(5):299–303. doi:10.1016/0020-1383(95)00037-A
25. Lin L, Liu Y, Lin C, et al. Comparison of three fixation methods in treatment of tibial fracture in adolescents. ANZ J Surg. 2018;88(6):E480–E485. doi:10.1111/ans.14258
26. Abalo A, Tomta K, Walla A, Ayouba G, Dossim A. Incidence and risk factors for pin tract infection in external fixation of fractures. Nigerian J Orthop Trauma. 2010;9(1).
27. Smith EJ, Kuang X, Pandarinath R. Comparing hospital outcomes between open and closed tibia fractures treated with intramedullary fixation. Injury. 2017;48(7):1609–1612. doi:10.1016/j.injury.2017.03.038
28. Sanjay N, Shanthappa AH. Effect of smoking on the healing of tibial shaft fractures in a rural Indian population. Cureus. 2022;14(14):e23018. doi:10.7759/cureus.23018
29. Kold S, Fridberg M, Bue M, Rölfing J. Host factors and risk of pin site infection in external fixation: a systematic review examining age, body mass index, smoking, and comorbidities including diabetes. J Limb Lengthen Reconstr. 2022;8(3):S3–S15. doi:10.4103/jllr.jllr_32_21
30. Zhang J, Lu V, Zhou AK, Stevenson A, Thahir A, Krkovic M. Predictors for infection severity for open tibial fractures: major trauma centre perspective. Arch Orthop Trauma Surg. 2023;143(11):6579–6587. doi:10.1007/s00402-023-04956-1
31. Penn-Barwell JG, Bennett PM, Mortiboy DE, Fries CA, Groom AF, Sargeant ID. Factors influencing infection in 10 years of battlefield open tibia fractures. Strategies Trauma Limb Reconstr. 2016;11(1):13–18. doi:10.1007/s11751-016-0250-x
32. Biz C, Crimì A, Fantoni I, Vigo M, Iacobellis C, Ruggieri P. Functional outcome and complications after treatment of comminuted tibial fractures or deformities using Ilizarov bone transport: a single-center study at 15- to 30-year follow-up. Arch Orthop Trauma Surg. 2021;141(11):1825–1833. doi:10.1007/s00402-020-03562-9
33. Olasinde AA, Jones GE. Predictive factors for pin sites infection in external fixation of open tibia fractures. J Musculoskelet Surg Res. 2023;1–7(4):271–277.
34. Matos MA, Lima LG, de Oliveira LA. Predisposing factors for early infection in patients with open fractures and proposal for a risk score. J Orthop Traumatol. 2015;16(3):195–201. doi:10.1007/s10195-015-0345-z
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.