")
Back to Journals » Breast Cancer: Targets and Therapy » Volume 13
Effectiveness of Psycho-Education Intervention Programme on Coping Strategies Among Jordanian Women Diagnosed with Breast Cancer: A Randomised Controlled Trial
Authors Younis M, Norsa'adah B , Othman A
Received 29 December 2020
Accepted for publication 19 March 2021
Published 11 May 2021 Volume 2021:13 Pages 285—297
DOI https://doi.org/10.2147/BCTT.S299584
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Murad Younis,1– 3 Bachok Norsa’adah,1 Azizah Othman4
1Unit of Biostatistics & Research Methodology, School of Medical Sciences, Universiti Sains Malaysia, Kota Bharu, 16150, Kelantan, Malaysia; 2Assistant Medical Science Department, Community College, University of Tabuk, Tabuk, Kingdom of Saudi Arabia; 3Radiation Oncology Department, Al-Bashir Hospital, 261 Amman, The Hashemite Kingdom of Jordan; 4Department of Pediatrics, School of Medical Sciences, Universiti Sains Malaysia, Kota Bharu, 16150, Kota Bharu, Kelantan, Malaysia
Correspondence: Murad Younis; Bachok Norsa’adah
Unit of Biostatistics & Research Methodology, School of Medical Sciences, Universiti Sains Malaysia, Kubang Kerian, Kota Bharu, 16150, Kelantan, Malaysia
Email [email protected]; [email protected]
Objective: This study aimed to assess the effectiveness of a psycho-education intervention programme in improving the coping strategies of Jordanian breast cancer patients.
Methods: A double-blinded randomised control trial involving 200 participants between the ages of 20 to 65 years old breast cancer patients was performed. Apart from those who refused participation, patients with chronic diseases and extreme baseline depression scores were also excluded. The control group received standard care twice a week from the social welfare services team facilitator compared to the intervention group that received additional psycho-education intervention programme (PEIP). The coping strategies were measured using the Brief-COPE inventory consisting of 28 items. It was administered on the second and 12th week of trial. The primary end point was compared between pre- and post-intervention. The effect of the intervention between groups, time, and covariates was measured using the generalised linear mixed model (GLMM) analysis.
Results: The mean (SD) of adaptive coping score among the intervention group increased from 5.63 (1.3) at baseline to 6.42 (1.3) at post-intervention. The mean avoidant coping score was 3.87 (1.1) at baseline but reduced to 3.69 (0.8) post-intervention. GLMM showed that women who received the intervention reported significantly higher usage of the adaptive coping strategies after attending the programme (B=0.921, p < 0.001).
Conclusion: PEIP significantly improved knowledge of breast cancer patients. Thus, this programme may be considered as a part of the healthcare services in Jordan towards improving the adaptive coping strategies among breast cancer patients, which may point towards the potential for these services to increase adaptive coping strategies among patients in Jordan.
Implications for Public Health: PEIP may be considered as psychosocial intervention in public health and healthcare setting to address rising concerns on quality of care among breast cancer patients.
Keywords: randomised controlled trial, health education, breast cancer, adaptive coping, avoidant coping, psycho-education intervention programme
Introduction
Breast cancer is one of the most frequently diagnosed cancers among women.1 The World Health Organization (WHO) reported that that breast cancer is accountable for approximately 30% of all cancers among women.2 It is also ranked as the fifth-highest cause of cancer-related deaths. Therefore, breast cancer is considered a global public health concern in both developed and developing countries.3,4 Furthermore, the cancer survival rate in developing countries is lower than that in developed countries. The lower survival rates can be caused by insufficient early detection programmes, thus resulting in delayed diagnosis at advanced stages.3 Locally, breast cancer is the third most common cause of cancer mortality among Jordanian women after lung and colorectal cancers.5 Hence, early detection of breast cancer is of vital importance. Unfortunately, breast cancer patients in Jordan do not have easy access to adequate cancer care due to the shortage of oncology-trained healthcare professionals. An imbalance in the physician–patient ratio in Jordan may also lead to insufficient counselling time for patients.6,7 As a result, it may result in communication failure and poor awareness of the patients’ concerns.8,9
A diagnosis of breast cancer is a stressful event that can challenge a woman’s basic values, beliefs, goals, life functions besides threatening her sense of identity. On one hand, the patients face unmet needs at the time of diagnosis and they often have the urge to speak with someone experienced to obtain the necessary information to overcome the disease.2 On the other hand, physicians usually need to see a large number of patients in the clinics daily, putting them at a point of burnout apart from limiting the consultation time spent with the patients. Particularly, the information that is given to patients often does not meet their needs at different phases of the disease trajectory.10,11 Therefore, it is necessary to instill effective coping strategies that can improve the psychological adaptation and quality of life of the patients.
Coping is defined as a method for patients to adapt to challenges and overcome their negative experiences.12 Psycho-educational intervention is also vital to improve wellbeing and reduce psychological distress such as cancer-related depression.13 A few interventions have been recommended to provide psycho-education and to facilitate experience-sharing in helping these patients.10,11 However, the majority of the studies focused on stress management during treatment or survival, and only a few targeted patients at the time of diagnosis when patients are most stress-prone.14
Furthermore, there is a scarcity of research to determine the effectiveness of the psycho-educational intervention programme (PEIP) to enhance coping strategies among women with breast cancer in Jordan. A cross-sectional study recommended further assessment of the impact of psychological and lifestyle influences on the prognosis of Jordanian breast cancer patients with appropriate coping strategies.15 Similarly, a meta-analysis from the Middle East and Arabic countries also amplified the urgency of investigating the effectiveness of a psycho-educational intervention in improving the coping strategies among breast cancer patients.13 This meta-analysis reported that the psycho-educational intervention was helpful for breast cancer patients to improve coping strategies. Our randomised controlled trial (RCT) study aimed to develop and examine the effectiveness of a PEIP for breast cancer patients in Jordan.
Methods
Ethics
Ethical approval was obtained to carry out from the research from the Ethics Committee for Research Involving Human Subjects of the Universiti Sains Malaysia (USM) No: (USM/JEPeM/18080386). Permission was also obtained from the Ethics Committee for Research involving human subjects, Jordanian Ministry of Health (JMOH) (development/plans/5085), correspondence: 05/07/2018. All participants provided informed consent, and this trial was conducted in accordance with the Declaration of Helsinki. The trial retrospectively registered with Australian New Zealand Clinical Trials Registry (ANZCTR) with the trial number of ACTRN12619000095167.
Study Design and Participants
This research was a double-blind parallel-group RCT guided by the CONSORT Statement.16 The blinding was applied to the data collectors to reduce ascertainment bias in the outcome. The study involved a total of 200 breast cancer patients who had received treatment at the Al-Bashir Hospital from January to March 2019. Patients with histologically confirmed metastatic breast cancer and those who did not consent to participate were not included in this research. Participants were recruited from the oncology clinics and wards through telephone calls. The randomisation of the control and the interventional groups was performed using the randomised block design (RBD). The allocation was performed through six blocks that consisted of four patients each (AABB, ABAB, ABBA, BAAB, BABA, BBAA) by the primary investigator (Figure 1).
 |
Figure 1 CONSORT diagram. |
Study Tools
Participants who met the eligibility criteria for the trial completed a questionnaire that captured baseline socio-demographic and clinical characteristics. The interventional outcome was assessed using Hospital Anxiety and Depression (HADS), European Organization for Research and Treatment of Cancer (EORTC), and Brief Coping Orientation to Problems Experienced (Brief-COPE) inventory.17–19 The HADS questionnaire consists of seven items to measure patients’ anxiety and depression state. Each item is scored from zero to three. Patients with a total subscale score of more than eight of the possible 21 are deemed to have experienced anxiety or depression. The magnitude of anxiety and depression is categorised as mild,8–10 moderate,11–14 and severe.15–21 The patient’s quality of life (QOL) was measured using EORTC QLQ-C30 and QLQ-BR23. The EORTC QLQ-C30 is a cancer-specific quality of life questionnaire consisting of 30 items. It is mainly used to measure the patient’s global health, functional, and symptom status on different scales. Meanwhile, EORTC QLQ-BR23 is a breast cancer-specific QOL questionnaire. It consists of 23 items that measure the patient’s appearance, sexual functions, and systemic therapy side effects. Each item was scored on a Likert scale ranging from “1 = Not at all” to “4 = Very much”, except for global status items with scores ranging from “1 = Very poor” to “7 = Excellent”. The total score is transformed to a linear scale of 0–100. A higher score represents higher functional wellbeing, symptoms, and QOL. Lastly, the patient’s coping strategy was evaluated using the Brief-COPE inventory. The higher scores for adaptive coping are better and the higher scores for avoidant coping are worse. This instrument measures 14 factors on a Likert scale, of which six are avoidant and eight are adaptive strategies corresponding to patients’ feelings and experience of cancer-related stressful events. The scoring ranges from 1 = “I have not been doing this at all” to 4 = “I have been doing this a lot”.
All the questionnaires are available in the Arabic language except for the Brief-COPE inventory. This questionnaire was translated into the Arabic language to overcome the linguistic problem while maintaining cultural relevance. Two independent translators performed the translation by applying forward and backward translation methods.20 Also, two psychologists examined the content and face validity of the pre-translated questionnaire. The pre-final questionnaire was subjected to pilot testing involving 10% of the sample size to obtain their appraisals for the appropriateness of the translation. Any discrepancies in the concepts of the translated questionnaire were resolved via discussion with a group of expert panel.21 The internal consistency of the translated Arabic questionnaire was comparable with the original questionnaire (Cronbach’s alpha, 0.85).
Participants in the control group received twice-weekly standard care by the social welfare services facilitators. Meanwhile, the intervention group received additional care in the form of PEIP. An expert committee was constituted to examine and edit the content for the psycho-educational materials used in PEIP. The six members of the expert committee consisted of clinical psychologists, oncologists, and public health specialists. The final version of the amended PEIP materials was given to the intervention group.
Psycho-Education Modules
The initial phase of the trial included the planning of study tools that took place between January and June 2019. The PEIP training module was prepared through a discussion with stakeholders and an expert committee based on the available scientific literature and patients’ suggestions. The final draft of the modules was presented to the physicians, nurses, and study participants. Following that, a pilot testing of the study tools was conducted alongside a semi-structured interview among 27 breast cancer patients to identify their perceived problems, disease knowledge, and expectations of the healthcare providers. It also aimed to identify the best coping strategy that the patients can adapt to achieve a good QOL to prevent psychological distress. The PEIP training module was finalised in the evaluation phase as per the recommendation by the reviewers. Finally, the expert panel validated the content of the final version of PEIP training modules (Table 1).
 |
Table 1 Tabular Illustration of Breast Cancer Psycho-Educational Intervention Modules Programme by Construct and Contents |
Measurements
The baseline socio-demographic and clinical characteristics questionnaire, the Hospital Anxiety and Depression Scale (HADS) questionnaire, and the Brief-COPE questionnaire were administered as face-to-face interviews. The questionnaires were administered by trained female nurses to minimise interviewer biases. In addition, the Brief-COPE questionnaire was re-administered at the second and twelfth week of follow-up. The study participants were followed up with giving reminder through phone calls and text messages via WhatsApp group of patients.
The participants in the intervention group attended a two-day session of PEIP interventional modules. Two modules were conducted during the first day and the remaining three modules, in the second-day session. Each module was allocated approximately two hours of face-to-face interaction. A trained clinical oncology consultant facilitated the intervention module. Each module emphasised health message about breast cancer such as the relevant facts, lifestyles or habits, problem-solving skills, interpersonal relationships, and experience-sharing. The calming technique was offered by a voluntary psychiatric therapist nurse while a breast cancer survivor offered the experience-sharing support sessions. The participants in the control group, they received a standard non-specific intervention that offered multiple services to support the mental wellbeing of cancer patients through spiritual support and calming technique. This service was facilitated by the social welfare officers for approximately 15 to 20 minutes twice a week for cancer patients with different prognosis in the group. A booklet that contained five health messages was given to all participants in both groups intervention and control group.
Statistical Analysis
All analyses were performed with the Statistical Package for the Social Sciences (SPSS) software version 24. The internal consistency of the Arabic version of Brief-COPE was determined through reliability analysis based on Cronbach’s alpha value. Descriptive statistics were reported whereby mean (M) and standard deviation (SD) were used to describe continuous variables while categorical variables were described with frequency (n) and percentages (%).
The difference in the baseline characteristics between the control and interventional groups was determined with the Independent t-test and Chi-square (χ2) test. Non-linear Categorical Principal Components Analysis (CATPCA) was used to calculate the Socioeconomic Index (SEI) with the dimension reduction technique. The CATPCA reduced the observed variables (women’s socioeconomic and educational level) to a composite index score of uncorrelated principal components.
Next, the Generalised Linear Mixed Models (GLMM) was performed to evaluate the effects of the intervention adjusted for confounding variables. A randomised wait-list controlled repeated measures (pre, post, and follow-up) were applied. Also, the interaction effect (time × intervention) was evaluated to measure the changes in the outcome variables between pretest and posttest as well as between pretest and follow-up. Independent variables for the preliminary main-effect model were determined based on the lowest Akaike Corrected Information Criterion (ACIC) and Bayesian Information Criterion (BIC), followed by variable selection using forward and backward stepwise procedure. The final model was selected based on the simplicity of the model that best described the association between the dependent variable (adaptive, avoidant) and other independent variables and outcomes. The dependent score was measured in three repeated measures (T1, T2, and T3). The model fitness was assessed with the diagnostic digital root information criteria. A statistically significant difference was considered at p-value ≤ 0.05.
Results
In total, 365 patients with breast cancer were screened for initial eligibility. Of these, 120 patients did not fulfill the inclusion criteria and 40 patients did not agree to participate. Thus, they were excluded from the study. Another five patients declined later on and only 200 patients remained in the study. All eligible participants were randomly allocated to the control and interventional groups.
Socio-Demographic and Clinical Characteristics at Baseline
The variability of baseline demographic and clinical characteristics between the control and interventional groups was evaluated to minimise bias and confounding in the trial (Table 2). The mean age of the participants in the control group was higher than that of the interventional group. There were no statistical or clinical differences between the two groups. The family history did not have any significant association between the interventional and control groups.
 |  | 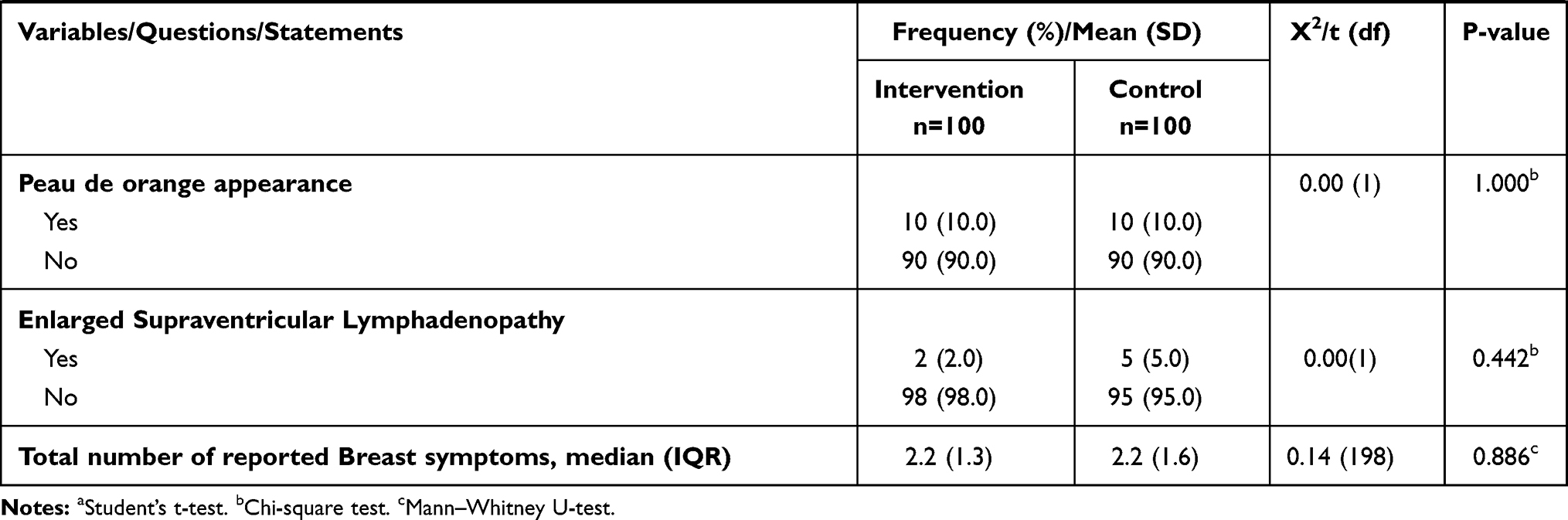 |
Table 2 Baseline Socio-Demographic and Clinical Characteristics of Participation |
Baseline Brief-COPE Score
There was no significant difference at baseline adaptive coping score [t(198)=0.13, p=0.901] between the control group (M=5.7, SD=1.3) and interventional group (M=5.6, SD=1.3). Similarly, no statistically significant difference was observed between the avoidant coping score observed between the control (M=3.7, SD=1.0) and (M=3.9, SD=1.1), [t(198)=0.85, p=0.339].
Effectiveness of the Intervention: Adaptive Coping
Table 3 provides the GLMM Repeated Measure analysis findings for the adaptive coping score of breast cancer patients. The model showed that the mean adaptive coping score was significantly higher across all the follow-up time points among the interventional group than the control group (B=0.921, 95% CI=0.58, 1.27, p<0.001). The PEIP intervention programme helped to increase the adaptive coping skills of the participants. The interaction of adaptive coping score between follow-up time and in the interventional group indicated significantly lower mean score at baseline when compared to the third month (B=−0.949, 95% CI=−1.38,-0.51 p<0.001). The model also suggested that patients with depression showed an inverse relationship with the adaptive coping score (B=−0.148, 95% CI=−0.17,-0.13, p<0.001). Meanwhile, patients with better socio-economic Index (SEI) demonstrated significantly greater adaptive coping scores compared with those with lower SEI (B=0.204, 95% CI=0.07, 0.34, p=0.003). All other covariates that were not significantly related to the adaptive coping scores were omitted from the model.
 |
Table 3 Effects of Psycho-Education Intervention Program on Adaptive Coping Strategy Scores Among Participation |
The model was fit throughout the data well as evidenced by a significantly low value of Information Criteria Indexes (AIC=1840.9 and BIC=1857.9). A low value of Information Criteria Indexes implied a good fit between the data and the predicted values of coping compared to an empty model with no predictors. Lastly, a post hoc pairwise comparison between the patients in the two groups at each time point was performed using the Independent t-test series. The result indicated that the participants in the control group had a significantly lower mean score of adaptive coping at the second week compared to those in the intervention group [Mean difference=−1.12, t(592)=7.38, p<0.001]. Furthermore, a similar result was found during three-month follow-up time point [Mean difference=−1.85, t(592)=9.061, p<0.001].
Effectiveness of the Intervention: Avoidant Coping
The GLMM Repeated Measure Model on perceived avoidant coping is shown in Table 4. Similar to adaptive coping, only covariates of avoidant coping that fit into the model were retained. As evidenced by the information criteria indexes, the goodness of fit of the model was significantly lower than an empty model with no predictors (AIC=1560.789, BIC= 1573.884). Regardless of the study groups, participants tended to have a lower avoidant coping score with increasing age (B=−0.018, 95% CI=−3.39, -.0.028 p=0.001). Study participants with a higher anxiety score also exhibited better avoidance coping strategies (B=−0.047, 95% CI=0.025, 0.068 p<0.001). There was a significant relationship between avoidance coping and cancer stages of participants in which participants showed higher avoidance scores as the disease progressed.
 |
Table 4 Effects of Psycho-Education Intervention Program on Avoidant Coping Strategy Scores Among Participation |
Furthermore, the interaction between follow-up time and the study groups suggested that the participants in the intervention group had significantly better avoidant coping strategies in the second follow-up compared to the third follow-up (B=−0.282, 95% CI=0.016, 0.547 p=0.038). The post hoc pairwise comparison test showed that the mean avoidant coping score was significantly higher at the second follow-up among participants in the control group compared to the interventional group [Mean difference=−0.51, t(590)=4.2, p<0.001].
Discussion
The baseline comparison test was performed within the randomised groups to ensure homogeneity between the control and intervention groups. Baseline homogeneity can limit the risk of bias and ensures post-intervention comparability between the two groups.22 From this study, the coping strategies of the cancer patients were observed to decline as the duration of cancer treatment increased. In the early stages of the diagnosis, the patients might still feel positive when coping with their newly diagnosed condition. However, their positivity would gradually wane off after receiving a few sessions of treatment. A recent study also stressed that cancer patients have a high tendency to feel lonely as they go through their cancer journey, thus affecting their abilities to cope with their lives.23
Additionally, the current study findings demonstrated that with each follow-up, the adaptive coping scores of the participants in the control group gradually decreased. A previous study by McKierbab et al echoed the steady drop in the mean adaptive coping score among the control group.24 Therefore, it is vital to provide constant emotional support to encourage breast cancer patients to cope with the disease. PEIP is one of the frequently used strategies to provide emotional support for patients.25 This programme helps patients to cope with their stressful health conditions by providing new knowledge and coping strategies related to breast cancer.26 These coping strategies incorporated in the interventional programme assist them to overcome negative emotions. The study results reflected the effectiveness of PEIP among the study participants. The mean adaptive coping score among participants in the intervention group showed a steady increase from baseline to the third month of follow-up compared to the control group. Previous literature also highlighted PEIP’s benefits in improving patients’ self-awareness of emotional and psychological handling, all of which might influence their coping strategy.23
Furthermore, the GLMM model used in this study also highlighted that the adaptive coping strategy was highly influenced by the depression score and the socioeconomic index of the patients. Patients with a lower depression score and higher socioeconomic index were significantly better at adaptive coping. The study finding correlated with Christie et al in which patients with lower incomes perceived more psychological stress than patients with stable incomes.27 Patients with a stable psychological state were better at coping with stress and they tended to face the problems rather than avoiding them. Additionally, the ability of a patient to positively adapt to their health condition was also highly influenced by economic stability.28 The socio-economic index used in this current study included socio-demographic status such as the participants’ education level, an important covariant in determining the coping strategy of a patient. Patients with higher educational backgrounds are more accepting and better at coping with their current health conditions.28 In this study, over 90% of the patients in the intervention group had at least attended secondary high schools. Hence, this finding was aligned with the Fogel (2004) study, which highlighted a significant relationship between educational level and adaptive coping strategies.
Meanwhile, the average avoidant coping score increased in the second week of intervention compared to the baseline score. In contrast, the avoidant coping score declined in the third month of follow-up. As outlined in the previous study, the diagnosis and treatment of breast cancer contributed not only to physical stress but also social and psychological stress.29 The motivation to cope with the disease often deteriorates as the patients experience an extended period of post-cancer diagnosis. Physical changes during treatment such as hair loss may also contribute to avoidance coping than adaptive coping strategies.29
Lastly, the GLMM analysis in this study highlighted that age was an important covariant to measure the coping strategy of the patient. Furthermore, age influenced the selection of the type of coping strategies among patients. Younger patients showed a higher tendency to practise avoidant coping strategies than the older patients.30 The model also demonstrated that avoidance coping could be influenced by anxiety. A higher anxiety score resulted in an increased practice of avoidant coping. The findings echoed an earlier study that reported on how psychological distress may lead to negative coping strategies.24
Strengths and Limitations
To the best of our knowledge, this was the first RCT that examined the effects of PEIP among breast cancer patients. However, there are a few limitations to the results of this study. Firstly, the PEIP was performed among a heterogeneous Jordanian population. Thus, the results cannot be generalised to other populations since the trans-cultural validity was limited only to the Jordanian population. Furthermore, several sensitive questions were left unresponded by the participants. As a result, these missing data might cause certain biases and compromised the precision of the result. Nevertheless, the missing values were addressed using the hot-deck imputation method. Apart from that, the inability to maintain an absolute controlled environment is another limitation of the RCT since there might be other external factors that could have caused response bias. Lastly, another drawback of the model was its failure to account for environmental and cultural factors, both of which are essential in predicting and explaining the patients’ behaviours.
Implications for Public Health
The added value of the present study included its potential contribution to the evaluative research on PEIP through the design, implementation, and assessment of a group counselling by breast cancer survivors for patients as well as the results obtained from the Generalised Linear Mixed Model (GLMM) analysis. The contributions of the trial can be applied in a theoretical, methodological, or pragmatic sense. From a theoretical perspective, this RCT fills a gap in the international psychological literature on the dimensions of psycho-education interventional in career development and construction. This study also allows for the development of adaptive and avoidant coping strategies among women diagnosed with breast cancer. In addition, the trial suggests that various stakeholders including nurses, public health leaders, policymakers, and healthcare institutions can reconsider the benefit of PEIP for breast cancer patients. Lastly, this study finding can guide healthcare policies by specifying and prioritising the appropriate services so that adequate and cost-effective programmes can be delivered to Jordanian breast cancer patients.
Conclusion
The PEIP trial in Jordan was found to be beneficial for breast cancer patients, thus further studies are warranted. The program successfully induced a positive coping strategy among the participants in the intervention group. A more precise plan needs to be taken to improve patient’s depression state by offering them better socio-economic security for better adoption of positive coping.
Data Sharing Statement
The data sharing statement indicating that individual participant data (IPD) are not available due to confidentiality issues and participant consent.
Acknowledgment
The authors wished to thank the participation of Universiti Sains Malaysia in this study. This article is based on Murad Younis’s doctoral dissertation that was submitted to the Universiti Sains Malaysia. Portions of this research were presented at the King Salman Armed Forces Hospital Northwestern Region Updates in Psychiatry Conference and the 1st MSD Forum of Health Education, Tabuk, Saudi Arabia 2020.
Funding
The research was supported partly by the Bridging Grant (304.PPSP, 6316342) from the Universiti Sains Malaysia.
Disclosure
Mr Murad Younis report a patent BREAST CANCER. HELPING WOMEN TO COPE BETTER licensed to CRLY00017416. The authors declare no other conflicts of interest.
References
1. Steponaviciene L, Briediene R, Vanseviciute R, Smailyte G. Trends in breast Cancer incidence and stage distribution before and during the introduction of the mammography screening programme in Lithuania. Cancer Control. 2019;26(1):1073274818821096. doi:10.1177/1073274818821096
2. DeSantis CE, Ma J, Gaudet MM, et al. Breast cancer statistics, 2019. CA Cancer J Clin. 2019;69(6):438–451. doi:10.3322/caac.21583
3. Rivera-Franco MM, Leon-Rodriguez E. Delays in breast cancer detection and treatment in developing countries. Breast Cancer Basic Clin Res. 2018;12:1178223417752677. doi:10.1177/1178223417752677
4. Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–E86. doi:10.1002/ijc.29210
5. Information and Research [Internet]. Non-communicable diseases directorate; 2017. Available from: http://www.moh.gov.jo/Echobusv3.0/SystemAssets/2d0cc71d-d935-4d6f-a72c-73d60cd0a16c.pdf.
6. National Research Council. Meeting psychosocial needs of women with breast cancer. National Academies Press; 2004.
7. King Hussien Cancer Foundation. Jordan breast cancer programme; 2009. Available from: http://khcfusa.org/khcfusaorg/BENEFICIARY/KHCF/JordanBreastCancerProgrammeJBCP/tabid/116/Default.asx.
8. Martino G, Catalano A, Agostino RM, et al. Quality of life and psychological functioning in postmenopausal women undergoing aromatase inhibitor treatment for early breast cancer. PLoS One. 2020;15(3):e0230681. doi:10.1371/journal.pone.0230681
9. Parker PA, Aaron J, Baile WF. Breast cancer: unique communication challenges and strategies to address them. Breast J. 2009;15(1):69–75. doi:10.1111/j.1524-4741.2008.00673.x
10. Harrison JD, Young JM, Price MA, Butow PN, Solomon MJ. What are the unmet supportive care needs of people with cancer? A systematic review. Supportive Care Cancer. 2009;17(8):1117–1128. doi:10.1007/s00520-009-0615-5
11. Park BW, Hwang SY. Unmet needs of breast cancer patients relative to survival duration. Yonsei Med J. 2012;53(1):118–125. doi:10.3349/ymj.2012.53.1.118
12. Zastrow C, Kirst-Ashman K. Understanding human behavior and the social environment. Brooks. Coles, United States: CA; 2013.
13. Younis MAR, Othman A, Norsa’adah B. Psychoeducational intervention programme for women with breast cancer: a systematic review and meta-analysis. Med Sci. 2020;24(104):2110–2118.
14. Di Giuseppe M, Di Silvestre A, Lo Sterzo R, Hitchcott P, Gemignani A, Conversano C. Qualitative and quantitative analysis of the defensive profile in breast cancer women: a pilot study. Health Psychol Open. 2019;Jun(1):2055102919854667.
15. Younis MAR, Norsa’adah B, Othman A, Shaqarin Y, Alqudah H, Shamoun S. Psychological distress impact and associated factors among Jordanian women diagnosed with breast cancer. Med Sci. 2020;24(104):2610–2619.
16. Hopewell S, Boutron I, Moher D. CONSORT and Its Extensions for Reporting Clinical Trials. Principles Pract Clin Trials. 2020;1–15.
17. Fayers P, Aaronson NK, Bjordal K, Sullivan M. EORTC QLQ–C30 scoring manual: European Organisation for Research and Treatment of Cancer; 1995.
18. Carver CS, Scheier MF, Weintraub J, Psychology S. Assessing coping strategies: a theoretically based approach. Journal of Personality and Social Psychology. 1989;56(2):267.
19. Snaith RP. The hospital anxiety and depression scale. Health Qual Life Outcomes. 2003;1(1):29. doi:10.1186/1477-7525-1-29
20. Brislin RW. Back-translation for cross-cultural research. J Cross Cult Psychol. 1970;1(3):185–216. doi:10.1177/135910457000100301
21. Chen HY, Boore JR. Translation and back‐translation in qualitative nursing research: methodological review. J Clin Nurs. 2010;19(1‐2):234–239. doi:10.1111/j.1365-2702.2009.02896.x
22. Corbett MS, Higgins JP, Woolacott NF. Assessing baseline imbalance in randomised trials: implications for the Cochrane risk of bias tool. Res Synth Methods. 2014;5(1):79–85. doi:10.1002/jrsm.1090
23. Cipolletta S, Simonato C, Faccio E. The effectiveness of psychoeducational support groups for women with breast cancer and their caregivers: a mixed methods study.Frontiers In Psychology 2019;10:288.
24. McKiernan A, Steggles S, Guerin S, Carr A. A controlled trial of group cognitive behavior therapy for Irish breast cancer patients. J Psychosoc Oncol. 2010;28(2):143–156. doi:10.1080/07347330903570511
25. Ram S, Narayanasamy R, Barua A. Effectiveness of group psycho-education on well-being and depression among breast cancer survivors of Melaka, Malaysia. Indian J Palliat Care. 2013;19(1):34. doi:10.4103/0973-1075.110234
26. Biegańska J, Pihut M. Psychoeducation programme on strategies for coping with stress in patients with temporomandibular joint dysfunction. Biomed Res Int. 2014;2014. doi:10.1155/2014/678169
27. Christie KM, Meyerowitz BE, Maly RC. Depression and sexual adjustment following breast cancer in low‐income Hispanic and non‐Hispanic White women. Psycho‐Oncology. 2010;19(10):1069–1077. doi:10.1002/pon.1661
28. Fogel J. Internet breast health information use and coping among women with breast cancer. CyberPsychol Behav. 2004;7(1):59–63. doi:10.1089/109493104322820129
29. Boatemaa Benson R, Cobbold B, Opoku Boamah E, Akuoko CP, Boateng D. Challenges, coping strategies, and social support among breast cancer patients in Ghana. Adv Public Health. 2020;2020.
30. Gruhn MA, Compas BE. Effects of maltreatment on coping and emotion regulation in childhood and adolescence: a meta-analytic review. Child Abuse Negl. 2020;103:104446. doi:10.1016/j.chiabu.2020.104446
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.