")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
Effect of Multi-Month Dispensing on Viral Suppression for Newly Enrolled Adolescents and Adults in Northern Nigeria
Authors Semo BW , Ezeokafor NA, Oyawola B, Mugo C
Received 29 July 2023
Accepted for publication 15 October 2023
Published 16 November 2023 Volume 2023:15 Pages 697—704
DOI https://doi.org/10.2147/HIV.S432976
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Bazghina-Werq Semo,1,* Nnenna A Ezeokafor,2,3,* Babatunde Oyawola,3 Cyrus Mugo4
1Global Health Division, Chemonics International, Washington, DC, USA; 2Maryland Global Initiative Cooperation, University of Maryland, Abuja, Nigeria; 3Global Health Division, Chemonics International, Abuja, Nigeria; 4Department of Research and Programs, Kenyatta National Hospital, Nairobi, Kenya
*These authors contributed equally to this work
Correspondence: Bazghina-Werq Semo, Global Health Division, Chemonics International, 1275 New Jersey Avenue, Washington, DC, 20003, USA, Email [email protected]
Purpose: We evaluated the effect of multi-month dispensing (MMD) on viral suppression among newly enrolled adolescents and adults with HIV in 11 northern Nigerian states.
Patients and Methods: We conducted a retrospective analysis of longitudinal data from 75 health facilities. We abstracted electronic medical records for patients ≥ 10 years, initiated on ART April 1, 2019 – June 30, 2021, and with a 6- or 12-month viral load (VL) result. We categorized participants in the MMD group to see if they received antiretroviral treatment (ART) for ≥ 84 days at any visit within 6 months of ART initiation. We consider cut-offs for viral suppression at 50 copies/mL. The period when the VL was performed was classified as pre-COVID-19 (before April 1, 2020) or during the COVID-19 pandemic. We estimated relative risks (RR) by comparing the unsuppressed proportion of those on MMD to those not on MMD, adjusted for age, gender, and COVID-19 period.
Results: Overall, 19,859 participant records were abstracted. Median age was 33 years, 64% were female, 91% were started on a dolutegravir (DTG)-based regimen, and 65% were on MMD. Overall, 15,259 (77%) participants were followed for ≥ 6 months, 4136 (27%) had a VL at 6 months and 3640 (24%) had a VL at 12 months after ART initiation. A slightly higher proportion of patients on MMD had undetectable VL levels at 6 months (65% vs 58%) and 12 months (66% vs 62%). In the adjusted analysis, we found no significant differences in undetectable VL at 6 months and 12 months between newly enrolled patients on MMD and those not on MMD. Those on Protease inhibitor-based regimen had 54% lower likelihood of undetectable VL compared to those on DTG-based regimen.
Conclusion: MMD does not result in poorer viral suppression among newly enrolled patients.
Keywords: HIV, differentiated service delivery, PLHIV, Nigeria
Introduction
Globally 39 million people were living with HIV (PLHIV) in 2022, 86% knew their HIV status, 89% of HIV positive people were on antiretroviral (ARV) treatment, and 92% of PLHIV on treatment had achieved viral suppression.1,2 As the number of PLHIV on treatment increases in high HIV burden countries, it has become necessary to scale up differentiated service delivery models that are client-centered and reduce the burden on national health systems. In 2016, the World Health Organization (WHO) recommended 3–6 monthly ARV refills also known as multi-month dispensing (MMD) for stable PLHIV (on treatment for a minimum of 1 year, no opportunistic infections and adverse reactions to treatment, not pregnant or breastfeeding, and virally suppressed based on two consecutive viral load (VL) measurements).3 By early 2020, the rollout of MMD among stable patients grew from 49% to 72% in 21 PEPFAR-supported countries4,5 with high levels of demonstrable viral suppression in sub-Saharan Africa.5–7 In 2020, at the start of the Coronavirus disease 2019 (COVID-19) pandemic, WHO further reiterated its call for the implementation of MMD, appealing to global leaders to maintain essential HIV services during the COVID-19 pandemic and beyond and to ensure adequate supplies of drugs.4
In 2021, Nigeria ranked fourth in the world with an estimated 1.9 million PLHIV.8 By the end of 2021, Nigeria had achieved 98–96-89 of the global 95–95–95 UNAIDS targets.9 The 2020 Nigerian guidelines for HIV prevention, treatment, and care by the National AIDS and STDs Control Program recommend MMD as a care package for stable clients who have achieved viral suppression and have spent over 6 months in care.10
In March 2020, the COVID-19 pandemic led to lockdowns and movement restrictions.5,11 To mitigate treatment interruptions, Nigeria adopted some innovative approaches and rapidly scaled up MMD among most treatment naïve and experienced PLHIV.10,12,13 Similar MMD practices were adopted by sub-Saharan African countries to avoid treatment interruptions, reduce the burden on health systems, and protect PLHIV and health providers from acquiring COVID-19 5,14 As a result, by the end of 2020, MMD coverage rates increased up to four-fold in some countries.5 In Nigeria, MMD coverage grew from 54% to 94% within the same period.15
The Strategic HIV/AIDS and TB Response Program Task Orders 1 and 3 (SHARP TO1 and TO3) are two-year projects funded by the US Agency for International Development (USAID) and implemented by Chemonics International to support HIV care and treatment services in 11 states and approximately 200 facilities in northern Nigeria. By March 2022, both projects had enrolled over 170,000 PLHIV on treatment, 93% of whom were receiving ARV treatment through MMD.
We conducted this study to assess the effect of MMD on viral suppression among newly enrolled and treatment naïve PLHIV in northern Nigeria.
Materials and Methods
Study Design and Procedures
This was a retrospective analysis of longitudinal patient records (clinic, pharmacy, and laboratory) for adolescents and adults (ages ≥10 years) newly enrolled in antiretroviral therapy (ART) from April 1, 2019 – June 30, 2021. The patients were receiving care in 75 facilities across 11 states in northern Nigeria (Adamawa, Bauchi, Borno, Jigawa, Kano, Kebbi, Kwara, Niger, Sokoto, Yobe, and Zamfara), We abstracted data for this study from the electronic medical records in the national Lafiya Management Information System.16
Measures and Definition of Variables
VL: As per Nigerian HIV care guidelines, patients receive VL measures 6 and 12 months after ART initiation, and at least yearly thereafter.10,17 Delays in VL sample collection and results processing were common in sub-Saharan African settings, especially during the COVID-19 pandemic.18–20 For this analysis, we selected the first VL measure on record for each patient done between 5 and 9 months after ART initiation as the 6-month VL, and the first VL done between 9 and 15 months after ART initiation as the 12-month VL. VL results were classified as unsuppressed (>1000 copies/mL), suppressed (<1000 copies/mL), detectable (>50 copies/mL), or undetectable (<50 copies/mL).10,17
MMD group: This consisted of participants who received ART for ≥84 days during any ART refill visit within the first 6 months after ART initiation. We created a sub-category of participants who received ART for ≥84 days in the same period more than once.
The ART regimen recorded at the time of initiating treatment was classified as one of the following:
- Dolutegravir (DTG) based
- Non-nucleoside reverse transcriptase inhibitor (NNRTI)-based for those on efavirenz or nevirapine
- Protease inhibitor (PI)-based for those on lopinavir or atazanavir
- Other for those not in any of the three drug categories.
Lastly, we included a variable we named COVID-19 period to identify whether a patient started ART before April 1, 2020 (pre-COVID-19 pandemic), or after April 1, 2020 (during COVID-19).
Analysis
We used descriptive measures (counts, proportions, medians, and interquartile ranges (IQR) to summarize the sociodemographic and HIV-related data and generalized linear models to determine their association with viral suppression at 6 and 12 months for all participants, and for participants on MMD.
The primary analyses determined the effect of MMD on undetectable viral load (VL<50 copies/mL) 6 months after initiating ART, and 12 months after initiating ART. Secondary analyses determined the effect of MMD on viral suppression (VL<1000 copies/mL) 6 months after initiating ART, and 12 months after initiating ART. In each analysis, we included only records of participants with complete data. For each analysis, we used generalized linear models (family = binomial (link=log)) and included bivariate and multivariate analysis. In the latter, we adjusted for age, gender, ART regimen, and COVID-19 period. We report relative risks (RR) from bivariate analyses and adjusted relative risks (aRR) from multivariate analyses. The 95% confidence intervals (95% CI) for the aRR, and p-values were computed using bootstrapping (1000 bootstrap samples from the full sample) to account for clustering of participants by facility. Additionally, we ran a sensitivity analysis comparing PLHIV with more than one MMD refill with PLHIV with one or no MMD refills to determine differences in achieving undetectable VL among the groups. All analyses were completed using R (Version 4.0.3, Foundation for Statistical Computing, Vienna, Austria) and R studio (Integrated Development Environment for R. RStudio, 2022, PBC, Boston, MA).
Ethical Considerations
We received Institutional Review Board (IRB) approvals from the National Health Research Ethics Committee of Nigeria (NHREC Approval Number NHREC/01/01/2007-28/06/2021) and the University of Maryland Baltimore Institutional Review Board (HP-00097414). Individual consent, including parental consent for minors, for the abstraction of patient medical records was waived since no patient identifying information was collected. Unique patient identifiers and names were excluded from the datasets shared with the research team by the program data teams. The handling of the data was done in accordance with the ethical principles in the Declaration of Helsinki for handling human subjects, materials, and data in research. The de-identified data were stored in a secure cloud repository with access restricted to only authorized study investigators. The data managers who did the data extraction are not co-authors of this paper.
Results
We abstracted pharmacy records for 19,859 newly enrolled adolescents and adults living with HIV. Majority (64%) of the participants were female, 91% were started on DTG-based regimen, 65% received ART refills to last ≥84 days (MMD) within the first 6 months, and 30% of PLHIV received greater than one MMD refill over the 6-month period. The median age of all the participants was 33 years (interquartile range [IQR]: 26–40). Of 19,859 participants, 15,259 (77%) were followed up for 6 months or more. Of 15,259 participants, 4136 (27%) had a VL 6 months after ART initiation, while 3640 (24%) had a VL 12 months after ART initiation. While there were no major differences between participants with a 6- or 12-month VL in the overall sample in terms of age, gender, and MMD, only 34% and 16% of those with a 6- and 12-month VL, respectively, were enrolled during the COVID-19 pandemic, compared to 53% in the overall sample, and a slightly lower proportion were on DTG (maximum difference of 7%) (Tables 1 and 2).
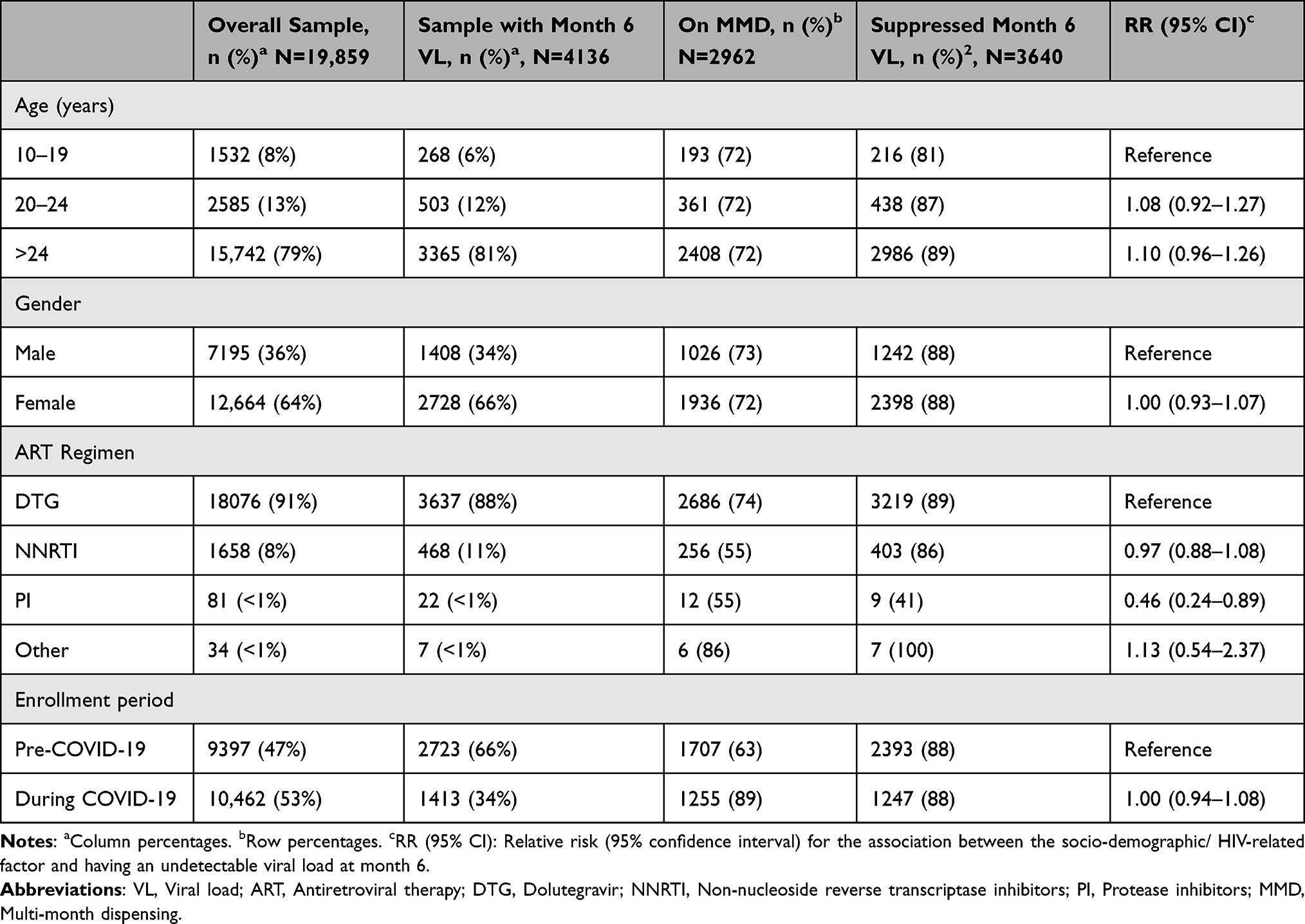 |
Table 1 Characteristics of Participants Newly Initiated on Antiretroviral Therapy and Viral Load Measures at 6 Months |
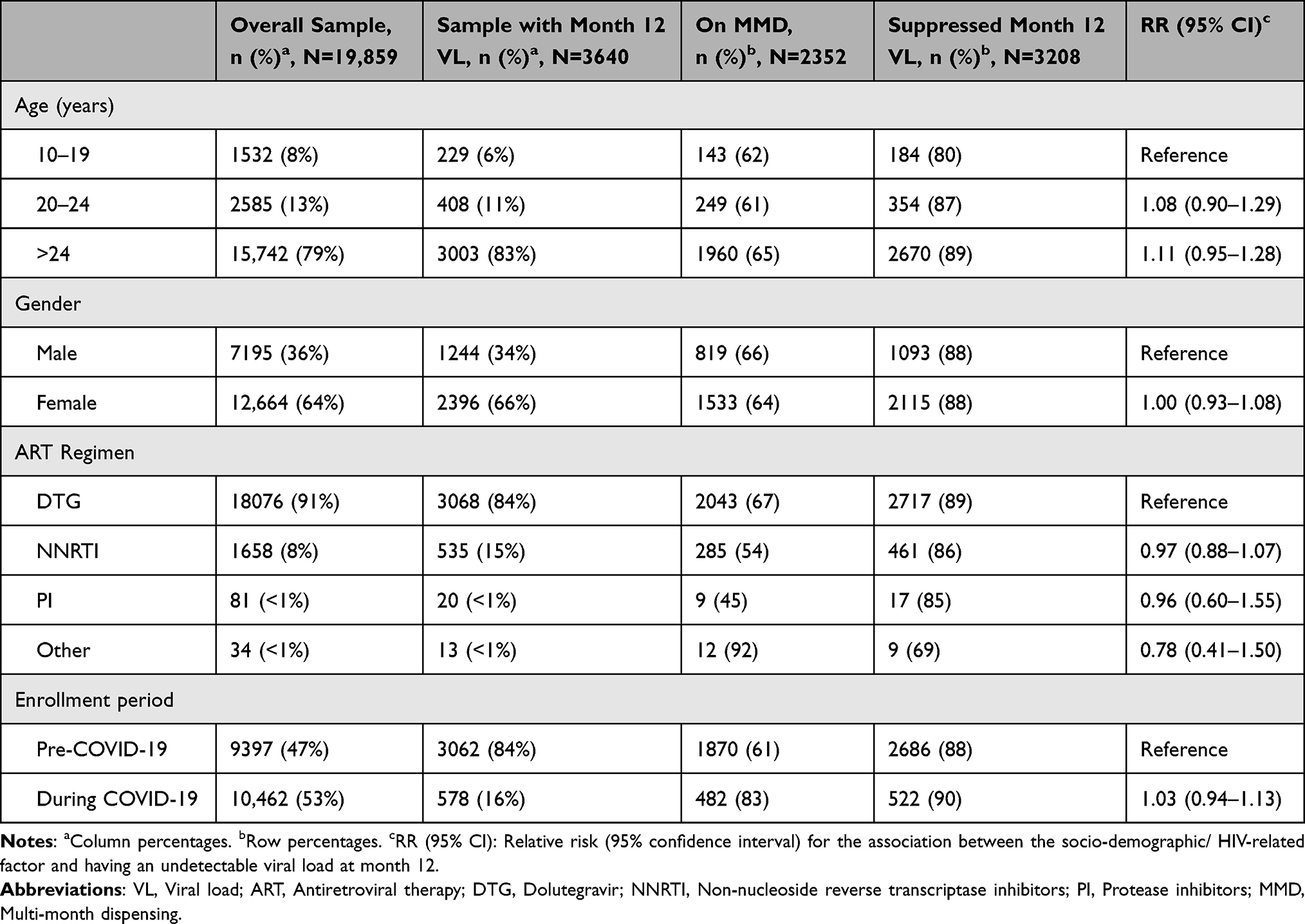 |
Table 2 Characteristics of Participants Newly Initiated on Antiretroviral Therapy and Viral Load Measures at Month 12 |
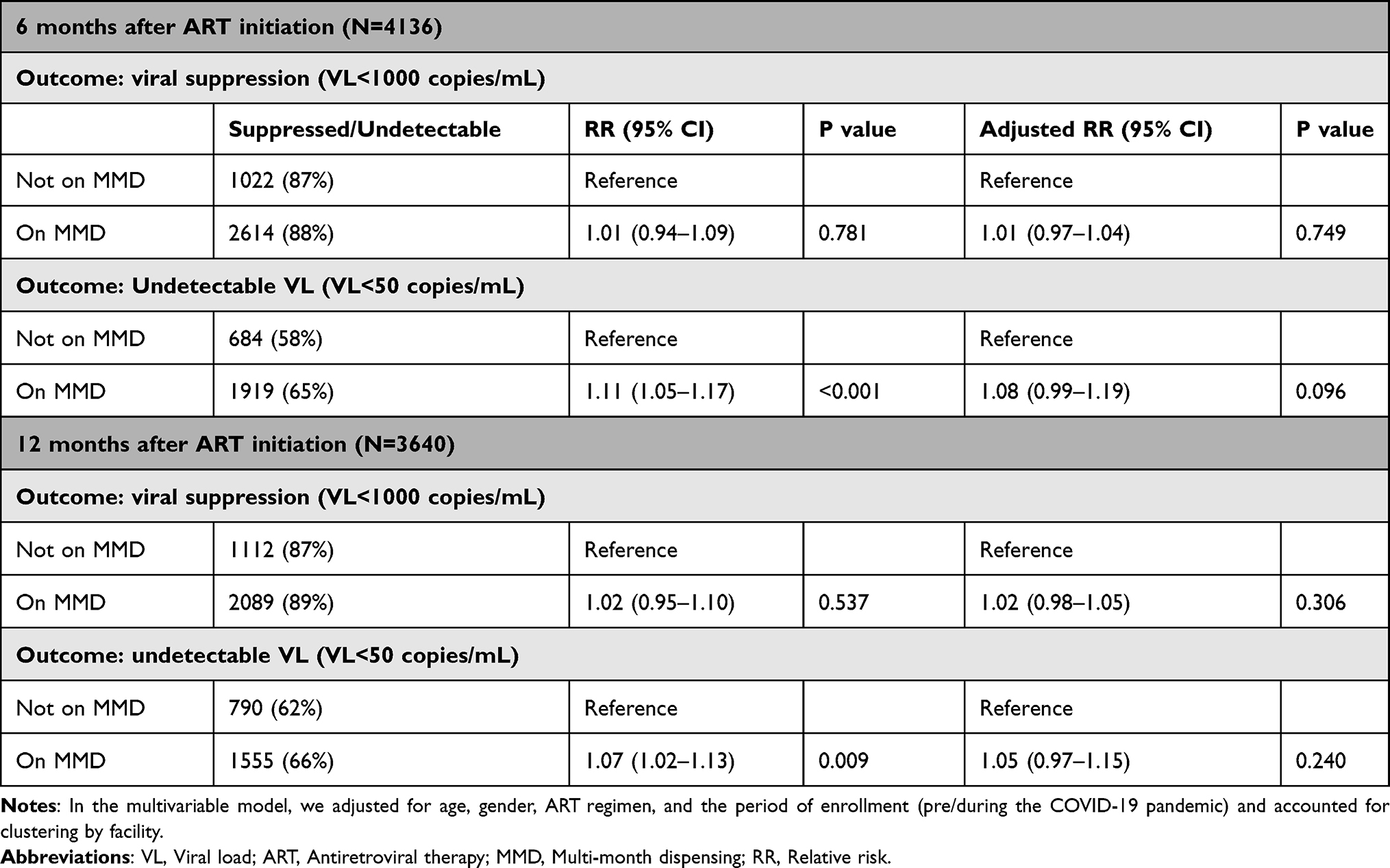 |
Table 3 Effect of Multi-Month Dispensing on Viral Loads at 6 Months and 12 Months After Initiation of Antiretroviral Therapy |
Of 4136 PLHIV with a 6-month VL result, 3640 (88%) were virally suppressed (<1000 copies/mL), while 2606 (63%) had undetectable VL results (<50 copies/mL) and 2962 (72%) were on MMD. Of the 3640 PLHIVS with a 12-month VL result, 3208 (88%) were virally suppressed and 2350 (65%) had undetectable VL results; 2352 (65%) were on MMD. A slightly higher proportion of patients on MMD were virally suppressed 6 months after ART initiation compared to those not on MMD (88% vs 87%), with the difference being higher in undetectable VL levels (65% vs 58%). Similarly, among PLHIVs with a 12-month VL result, those on MMD had higher viral suppression (89% vs 87%) and undetectable VL results (66% vs 62%). ART regimen was associated with viral suppression at 6 months among PLHIV on MMD. Those on PI-based regimen had 54% lower likelihood of viral suppression at 6 months compared to those on DTG-based regimen (RR: 0.46 [95% CI: 0.24–0.89]). No other factors were associated with viral suppression for the full sample (Table 1), and among those on MMD (Supplementary Table 1). We found no significant differences in viral suppression or undetectable VL results at 6 months (aRR: 1.01 [95% CI: 0.97–1.04], and aRR: 1.08 [95% CI: 0.99–1.19] respectively); and at 12 months (aRR: 1.02 [95% CI: 0.98–1.05], and aRR: 1.05 [95% CI: 0.97–1.15]) (Table 3) between newly enrolled patients on MMD and not on MMD, respectively. We found similar results [no significant differences in viral suppression or undetectable VL results at 6 months (aRR: 1.01 [95% CI: 0.98–1.04], 0.602, and aRR: 1.02 [95% CI: 0.96–1.10], p=0.477, respectively); and at 12 months (aRR: 1.03 [95% CI: 0.99–1.06], p=0.053, and aRR: 1.07 [95% CI: 0.98–1.16], p=0.110)] from the analysis comparing PLHIV who had more than one MMD refill with those who had one or no MMD refills.
Discussion
This study demonstrates MMD of ART is feasible and does not result in poorer treatment outcomes among adolescents and adults newly enrolled in HIV care. However, despite more than 90% of participants having been initiated on DTG-based regimen, over one-third of patients did not attain an undetectable VL at 6 and 12 months, while approximately 10% of PLHIV did not achieve VL suppression below the 1000 copies/mL level. The uptake of VL testing at 6 and 12 months after ART initiation was low, with over 70% of the eligible participants missing VL testing, likely due to the logistical barriers experienced in many settings during the COVID-19 pandemic.13 However, we noted that a slightly higher number of patients were initiated on ART during the pandemic, demonstrating the resilience of the program in ensuring HIV testing and treatment services were accessible.
Two-thirds of patients received MMD of ART within the first 6 months of treatment initiation. Notably, this practice existed in the year preceding the COVID-19 pandemic with 63% of newly initiated ART patients receiving their medications through MMD within the first 6 months. This finding demonstrates that providers in Nigeria had embraced MMD before COVID-19, contrary to local treatment guidelines. This is likely to have been informed by studies from other countries that showed it was a feasible strategy for HIV care and treatment.21–23
In 2020, MMD was rapidly scaled up among PLHIV in Nigeria to improve access and mitigate treatment interruptions, due to the COVID-19 pandemic. Despite beliefs from the HIV community that MMD could adversely affect treatment outcomes among newly initiated ART patients,24,25 we found that patients on MMD were more likely to achieve undetectable VL at 6 and 12 months comparable to patients who were not on MMD and similar to previous studies among treatment-experienced and stable patients.26 Our study also showed that the number of MMD refills does not have an effect on viral suppression. The benefits of MMD for HIV programs such as decongesting clinics and reducing the cost of care for patients21 can be extended to the care of newly enrolled PLHIV without fear of poorer treatment outcomes. Our results align with evidence from recent studies that show MMD is feasible among newly diagnosed patients.27
We assessed the effect of other key factors on VL suppression and undetectable VL levels among newly diagnosed PLHIV. Due to better tolerability, we expected PLHIV on DTG to maintain better VL suppression rates than patients on PIs at 6 and 12 months.28,29 Overall, patients initiated on PI-based regimen had a lower likelihood of VL suppression compared to those on DTG at 6 months. However, we did not observe a lower likelihood of VL suppression for patients on PI-based regimen at 12 months. The early advantages of DTG including more rapid declines in VL have been established in previous studies. Moreover, when conducting further analysis for PLHIV on MMD, we were not able to observe the advantages of being on DTG-based regimen even at 6 months, likely due to the smaller sample size and a lack of power to detect small differences.
The high DTG (>90%) coverage in 2021 speaks to how successful Nigeria has been in transitioning PLHIV to a more effective ART that is well tolerated, easy to take, less toxic and has a higher barrier to resistance.11 Unlike previous studies among ART-experienced PLHIV, factors like lower age (especially adolescent stage)30,31 and male gender were not associated with a lower likelihood of viral suppression.32–34
The study population was heavily skewed towards adults (79%), which reflects the population of PLHIV in Nigeria.35,36 High levels of missing VL results were a concern, however there were no major differences between the overall PLHIV population and patients with a VL in terms of the variable, suggesting this might have been random. In our study, we used routine clinical data to abstract a limited number of variables and were unable to identify the full range of possible factors that could influence viral suppression including social factors like stigma and mental health.37,38
Conclusion
In this study, we found similar treatment outcomes between newly diagnosed patients on multi-month dispensing and PLHIV not on MMD within the first 6 months after initiating ART. The findings from our study suggest that MMD can be adopted and promoted for new PLHIV on ART without concern that patients will experience poorer outcomes.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. The global health observatory. Available from: https://www.who.int/data/gho/data/themes/hiv-aids.
2. UNAIDS. Global HIV & AIDS statistics — fact sheet. Available from: https://www.unaids.org/en/resources/fact-sheet.
3. World Health Organization. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: recommendations for a public health approach; 2016. Available from: https://www.who.int/publications/i/item/9789241549684.
4. World AIDS Day 2020. WHO calls for global solidarity to maintain HIV services. Available from: https://www.who.int/news/item/30-11-2020-world-aids-day-2020-who-calls-for-global-solidarity-to-maintain-hiv-services.
5. Bailey LE, Siberry GK, Agaba P, Douglas M, Clinkscales JR, Godfrey C. The impact of COVID-19 on multi-month dispensing (MMD) policies for antiretroviral therapy (ART) and MMD uptake in 21 PEPFAR-supported countries: a multi-country analysis. J Int AIDS Soc. 2021;24(Suppl 6). doi:10.1002/jia2.25794
6. Traub AM, Ifafore-Calfee T, Phelps BR. Multimonth dispensing of antiretroviral therapy protects the most vulnerable from 2 pandemics at Once. Glob Heal Sci Pract. 2020;8(2):176–177. doi:10.9745/GHSP-D-20-00160
7. Lopes J, Grimwood A, Ngorima-Mabhena N, et al. Out-of-facility multimonth dispensing of antiretroviral treatment: a pooled analysis using individual patient data from cluster-randomized trials in Southern Africa. J Acquir Immune Defic Syndr. 2021;88(5):477–486. doi:10.1097/QAI.0000000000002797
8. World Health Organization. 2021 Annual report: making people healthier 2021; 2021:1–12. Available from: https://www.afro.who.int/countries/nigeria/publication/nigeria-country-office-2021-annual-report.
9. NASCP. 2021 Annual Report HIV / AIDS health sector response in Nigeria; Natl AIDS, Viral Hepatitis and STI Control Program; 2021:45.
10. National HIV Treatment Guideline; 2020. Available from: https://nascp.gov.ng/resources/get_resource_doc/17.
11. Odukoya OO, Adejimi AA, Isikekpei B, Jim CS, Osibogun A, Ogunsola FT. Epidemiological trends of coronavirus disease 2019 in Nigeria: from 1 to 10,000. Niger Postgrad Med J. 2020;27(4):271–279. doi:10.4103/npmj.npmj_233_20
12. HRH Organization PAH. Guidelines for the implementation of multi-month dispensing of antiretrovirals; 2020. Available from: https://iris.paho.org/bitstream/handle/10665.2/52949/PAHOCDEHSSCOVID-19200037_eng.pdf?sequence=5.
13. World Health Organization. Disruption in HIV, Hepatitis and STI services due to COVID-19 Global HIV, Hepatitis and STI Programmes Global COVID − 19 status – case counts. World Health Organization; 2020:22. Available from: https://www.who.int/hiv/data/HHS_Service_Disruption_Slides_July_2020.pdf?ua=1.
14. Golin R, Godfrey C, Firth J, et al. PEPFAR’s response to the convergence of the HIV and COVID-19 pandemics in Sub-Saharan Africa. J Int AIDS Soc. 2020;23(8):1–5. doi:10.1002/jia2.25587
15. Nigeria Country Operational Plan (COP). 2021 strategic direction summary; 2021:19. Available from: https://www.state.gov/wp-content/uploads/2021/09/Nigeria_SDS_Final-Public_Aug-11-2021.pdf.
16. Olukunle O. Assessing innovative ICT for health information system in African rural communities. Geo Infor Manag. 2009;1(1):69–93.
17. Federal Ministry of Health N. National AIDS and STI’s control programme, federal ministry of health: national guidelines for HIV prevention treatment and care. 2016. Available from: https://www.prepwatch.org/wp-content/uploads/2017/08/nigeria_national_guidelines_2016.pdf.
18. Kalua T, Egger M, Jahn A, Chimpandule T, Kolola R, Anderegg N. HIV suppression was maintained during the COVID-19 pandemic in Malawi: a program-level cohort study. J Clin Epidemiol. 2022;150:116–125. doi:10.1016/j.jclinepi.2022.06.019
19. Lagat H, Sharma M, Kariithi E, et al. Impact of the COVID-19 pandemic on HIV testing and assisted partner notification services, Western Kenya. AIDS Behav. 2020;24(11):3010–3013. doi:10.1007/s10461-020-02938-7
20. Lecher SL, Naluguza M, Mwangi C, et al. Notes from the field: impact of the COVID-19 response on scale-up of HIV viral load testing - PEPFAR-Supported Countries, January-June 2020. MMWR Morb Mortal Wkly Rep. 2021;70(21):794–795. doi:10.15585/mmwr.mm7021a3
21. Traub AM, Ifafore-Calfee T, Frymus D, Phelps BR. Multimonth dispensing of antiretroviral therapy for HIV. Lancet HIV. 2020;7(7):e457–e458. doi:10.1016/S2352-3018(20)30169-7
22. Fatti G, Ngorima-Mabhena N, Mothibi E, et al. Outcomes of Three- versus six-monthly dispensing of antiretroviral treatment (ART) for Stable HIV patients in community ART refill groups: a cluster-randomized trial in Zimbabwe. J Acquir Immune Defic Syndr. 2020;84(2):162–72. doi:10.1097/QAI.0000000000002333
23. Tukei BB, Fatti G, Tiam A, et al. Twelve-month outcomes of community-based differentiated models of multimonth dispensing of ART among stable HIV-infected adults in Lesotho: a cluster-randomized noninferiority trial. J Acquir Immune Defic Syndr. 2020;85(3):280–91. doi:10.1097/QAI.0000000000002439
24. Mantell JE, Zech JM, Masvawure TB, et al. Implementing six multi-month dispensing of antiretroviral therapy in Ethiopia: perspectives of clients and healthcare workers. BMC Health Serv Res. 2023;23(1):563. doi:10.1186/s12913-023-09549-7
25. Hubbard J, Phiri K, Moucheraud C, et al. A qualitative assessment of provider and client experiences with 3- and 6-month dispensing intervals of antiretroviral therapy in Malawi. Glob Heal Sci Pract. 2020;8(1):18–27. doi:10.9745/GHSP-D-19-00286
26. Hagey JM, Li X, Barr-Walker J, et al. Differentiated HIV care in sub-Saharan Africa: a scoping review to inform antiretroviral therapy provision for stable HIV-infected individuals in Kenya. AIDS Care. 2018;30(12):1477–1487. doi:10.1080/09540121.2018.1500995
27. Fatti G, Ngorima-Mabhena N, Tiam A, et al. Community-based differentiated service delivery models incorporating multi-month dispensing of antiretroviral treatment for newly stable people living with HIV receiving single annual clinical visits: a pooled analysis of two cluster-randomized trials in Southern Africa. J Int AIDS Soc. 2021;24:S6.
28. Nickel K, Halfpenny NJA, Snedecor SJ, Punekar YS. Comparative efficacy, safety and durability of dolutegravir relative to common core agents in treatment-naïve patients infected with HIV-1: an update on a systematic review and network meta-analysis. BMC Infect Dis. 2021;21(1):222. doi:10.1186/s12879-021-05850-0
29. McCormack PL. Dolutegravir: a review of its use in the management of HIV-1 infection in adolescents and adults. Drugs. 2014;74(11):1241–1252. doi:10.1007/s40265-014-0256-y
30. Mujugira A, Celum C, Tappero JW, Ronald A, Mugo N, Baeten JM. Younger age predicts failure to achieve viral suppression and virologic rebound among HIV-1-infected persons in serodiscordant partnerships. AIDS Res Hum Retroviruses. 2016;32(2):148–154. doi:10.1089/aid.2015.0296
31. Hess KL, Hall HI. HIV viral suppression, 37 states and the district of columbia, 2014. J Community Health. 2018;43(2):338–347. doi:10.1007/s10900-017-0427-3
32. Regan M, Muhihi A, Nagu T, et al. Depression and viral suppression among adults living with HIV in Tanzania. AIDS Behav. 2021;25(10):3097–3105. doi:10.1007/s10461-021-03187-y
33. Njuguna I, Neary J, Mburu C, et al. Clinic-level and individual-level factors that influence HIV viral suppression in adolescents and young adults: a national survey in Kenya. AIDS. 2020;34(7):1065–1074. doi:10.1097/QAD.0000000000002538
34. Andronescu L, Zulu PM, Jackson SS, Hachaambwa L, Claassen CW, Stafford KA. The association between gender and HIV viral suppression on third-line therapy in Zambia: a retrospective cohort study. Int J STD AIDS. 2019;30(5):453–459. doi:10.1177/0956462418817645
35. Awofala AA, Ogundele OE. HIV epidemiology in Nigeria. Saudi J Biol Sci. 2018;25(4):697–703. doi:10.1016/j.sjbs.2016.03.006
36. Aids G. Country progress report: Nigeria; 2020:14. Available from: https://www.unaids.org/sites/default/files/country/documents/NGA_2020_countryreport.pdf.
37. Mugo C, Kohler P, Kumar M, et al. Effect of HIV stigma on depressive symptoms, treatment adherence, and viral suppression among youth with HIV. AIDS. 2023;37(5):813–821. doi:10.1097/QAD.0000000000003473
38. Bhardwaj A, Comins CA, Guddera V, et al. Prevalence of depression, syndemic factors and their impact on viral suppression among female sex workers living with HIV in eThekwini, South Africa. BMC Women's Health. 2023;23(1):232. doi:10.1186/s12905-023-02392-2
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.