")
Back to Journals » Clinical and Experimental Gastroenterology » Volume 16
Dumping Syndrome: Pragmatic Treatment Options and Experimental Approaches for Improving Clinical Outcomes
Authors Masclee GM , Masclee AA
Received 15 June 2023
Accepted for publication 22 October 2023
Published 6 November 2023 Volume 2023:16 Pages 197—211
DOI https://doi.org/10.2147/CEG.S392265
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vipul Yagnik
Gwen MC Masclee,1 Ad AM Masclee2,3
1Department of Gastroenterology and Hepatology, Amsterdam University Medical Center, Amsterdam, the Netherlands; 2Department of Gastroenterology and Hepatology, Maastricht University Medical Center +, Maastricht, the Netherlands; 3NUTRIM, School of Nutrition and Translational Research in Metabolism, Maastricht University, Maastricht, the Netherlands
Correspondence: Gwen MC Masclee, Department of Gastroenterology and Hepatology, Amsterdam University Medical Center, Meibergdreef 9, Amsterdam, 1105 AZ, the Netherlands, Tel +3120 4440613, Email [email protected]
Abstract: Dumping syndrome is a common complication after esophageal, gastric and bariatric surgery and has a significant negative impact on the quality of life of patients. This narrative review describes the clinical syndrome, pathophysiology, diagnosis and reports on standard and pragmatic therapeutical treatment options in order to improve the clinical outcome of patients with dumping syndrome. Dumping syndrome consists of early and late dumping symptoms and can be diagnosed using clinical parameters with the help of the Sigstad’s score, questionnaires or by provocative testing. The prevalence of dumping syndrome varies depending on the employed definition of dumping syndrome. Overall, dumping syndrome is more frequent nowadays due to increasing numbers of upper gastrointestinal and bariatric surgeries being performed. First treatment step includes dietary adjustment and dietary supplements, which are often sufficient to manage symptoms for the majority of patients. Next step of therapy includes acarbose, which is effective for late dumping symptoms, but the use is limited due to side effects. Somatostatin analogues are indicated after these two steps have failed. Somatostatin analogues are very effective for controlling early and late dumping, also in the long term. Glucagon like peptide-1 receptor agonists, endoscopic and surgical (re)interventions are reported as treatment options for refractory dumping syndrome; however, their use is not recommended in clinical practice due to the limited evidence on and uncertainty of outcomes. These alternatives should be considered only as last resort options in patients with otherwise refractory and invalidating dumping syndrome.
Keywords: dumping syndrome, early and late dumping, somatostatin analogues, octreotide, bariatric surgery, upper gastrointestinal surgery
Introduction
The first descriptions of postprandial symptoms and rapid emptying of the stomach after surgical gastroenterostomy date from 1907 to 1913 and report the occurrence of symptoms as unfavorable after-effects of the surgery.1,2 The term “dumping” was introduced seven years later. in 1920, when rapid barium gastric emptying was first documented in patients with typical postprandial symptoms.3,4 Since the description of this syndrome, there has been an increase in reporting of dumping syndrome due to increased awareness and an increase in the number of upper gastrointestinal surgeries consisting of oncologic, bariatric (Roux-en-Y gastric bypass [RYGB] or sleeve gastrectomy) and anti-reflux surgeries being performed. There is still debate about the definition and diagnosis of dumping syndrome, hampering interpretation and aggregation of results from scientific studies. Clinical symptoms are divided into early dumping symptoms (within an hour after a meal) and late dumping symptoms, typically occurring 1–3 hours postprandially. Although we have learned a lot in terms of pathophysiology and treatment options, there are still several knowledge gaps that should be identified before we can optimize treatment. This is particularly relevant for patients with dumping syndrome in whom initial treatment options such as diet and drug therapy with somatostatin analogues do not sufficiently improve symptoms. The aim of the current narrative review is to describe dumping syndrome and guide clinicians, dieticians and other medical caregivers in terms of diagnosis and treatment options.
Methods
Relevant studies for this narrative review were identified by a PubMed search using search terms including dumping syndrome. Articles published up to 31 January 2023 and written in the English language were reviewed and selected. Additionally, reference lists from the original articles were reviewed for other relevant studies in order to be as complete as possible in the current review. As there is limited availability of evidence of high-quality studies on diagnosis and treatment of dumping syndrome, one should note that this review comprises evidence and suggestions from the consensus guideline5 on dumping syndrome published in 2020 and data from the most recent literature. In the consensus guideline, level of evidence is graded and given per questioned item.6 In this narrative review we provide the level of evidence (Supplementary Table 1) for each item that is discussed.
Clinical Features of Dumping Syndrome
The clinical picture of dumping syndrome consists of two subtypes: early and late dumping, based on the timing at which symptoms appear postprandially and on their underlying pathophysiology. About 70% of patients with dumping syndrome have early dumping without late dumping and 30% present with combined early and late dumping. A small minority of patients suffer from late dumping only. Early dumping occurs in the first hour after meal ingestion and late dumping occurs one to three hours postprandially. Early dumping symptoms are divided into abdominal and systemic symptoms. Abdominal symptoms consist of borborygmi, fullness, abdominal distension, pain, nausea and diarrhea. Systemic (vasomotor) symptoms consist of palpitations, desire to lie or sit down, feeling of warmth, sweating, flushing, dizziness, fatigue and exhaustion. Early dumping is the result of rapid nutrient delivery into the small intestine. Symptoms of late dumping syndrome are primarily the manifestations of reactive (neuro)hypoglycemia, as indicated by fatigue, weakness, confusion, hunger, syncope, and loss of consciousness, and autonomic and/or adrenergic reactivity, as indicated by perspiration, palpitations, tremors and irritability. Dumping symptoms typically develop after ingestion of food. Patients are free of symptoms in the fasting state. Meals and liquid foods rich in rapidly absorbable carbohydrates (usually simple sugars with a high glycemic index) rather than meals rich in complex carbohydrates are not well tolerated. The severity of complaints may vary from mild to severe. Dumping symptoms are often debilitating and emotionally distressing, and are associated with a substantial reduction in quality of life and subsequently may lead to considerable weight loss as a result of the patient avoiding food intake.5,7–9
Pathophysiology of Dumping Syndrome
Upper gastrointestinal (GI) surgery can reduce gastric volume, remove the barrier function of the pylorus, or affect gastric motor function via vagal denervation. All these factors may lead to more rapid delivery of food into the small bowel. The hyperosmolar small bowel chyme may cause a fluid shift from the vascular compartment to the intestinal lumen, resulting in hypotension and occasionally even syncope. The fluid shift may cause bowel distension and generate abdominal symptoms such as fullness, borborygmus, abdominal distension, cramping, pain and diarrhea. The occurrence of this fluid shift has previously been confirmed by a rise in hematocrit level in the first hour after meal ingestion or during dumping provocation tests.10,11 Consequently, as compensation, a drop in atrial natriuretic peptide secretion may occur.12 Volume shifts are not the only mechanism of early dumping as adequate intravenous fluid substitution is not effective in preventing symptoms of early dumping.13 A second mechanism involved is the enhanced release of various gastrointestinal hormones resulting in (1) stimulation of gastrointestinal motility and secretion, and (2) enhanced release of vasoactive agents affecting both abdominal and systemic blood flow and vasomotor function. Much attention has been given in the past decades to incretin hormones such as glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic peptide (GIP), both being gut peptides released from the more proximal small bowel and known to stimulate insulin secretion after a hyperglycemic spike resulting in reactive hypoglycemia.14–16 Postprandial hypoglycemia (PPH) occurs more often after bariatric surgery.5,17,18 A recent study that used continuous glucose monitoring (CGM) found a prevalence of PPH after bariatric surgery of up to 50% in patients who had undergone Roux-en-Y gastric bypass (RYGB) or vertical sleeve gastrectomy.19 The terms PPH and late dumping are used interchangeably. Some authors, however, differentiate the two conditions because of differences in the time of onset after surgery: dumping developing shortly after surgery (weeks), while hypoglycemia typically manifests at a later stage, months or sometimes years after bariatric surgery.20 In our experience, this is also the case with late dumping symptoms. Most importantly, the pathophysiology of dumping and PPH is identical21 and, in our opinion, PPH should be seen and treated as a late dumping manifestation.
Epidemiology of Dumping Syndrome
The reported incidence and prevalence of dumping syndrome varies widely and depends on (1) which definition and diagnostic criteria are used, and (2) the type and extent of surgery performed. It is estimated that dumping symptoms are present in around 20% of patients with vagotomy with pyloroplasty, up to 40% of patients after RYGB or sleeve gastrectomy, and have been reported in up to 50% of patients after esophagectomy (Table 1). The cause of dumping syndrome has shifted from post-upper GI surgery for benign gastric or duodenal ulcer disease to the majority of dumping syndrome being due to post-bariatric surgery and upper gastrointestinal oncologic surgery nowadays. As a larger number of patients are undergoing sleeve gastrectomy or RYGB for bariatric purposes, it is important for clinicians to recognize and treat dumping syndrome as it results in a reduced health-related quality of life for patients.8
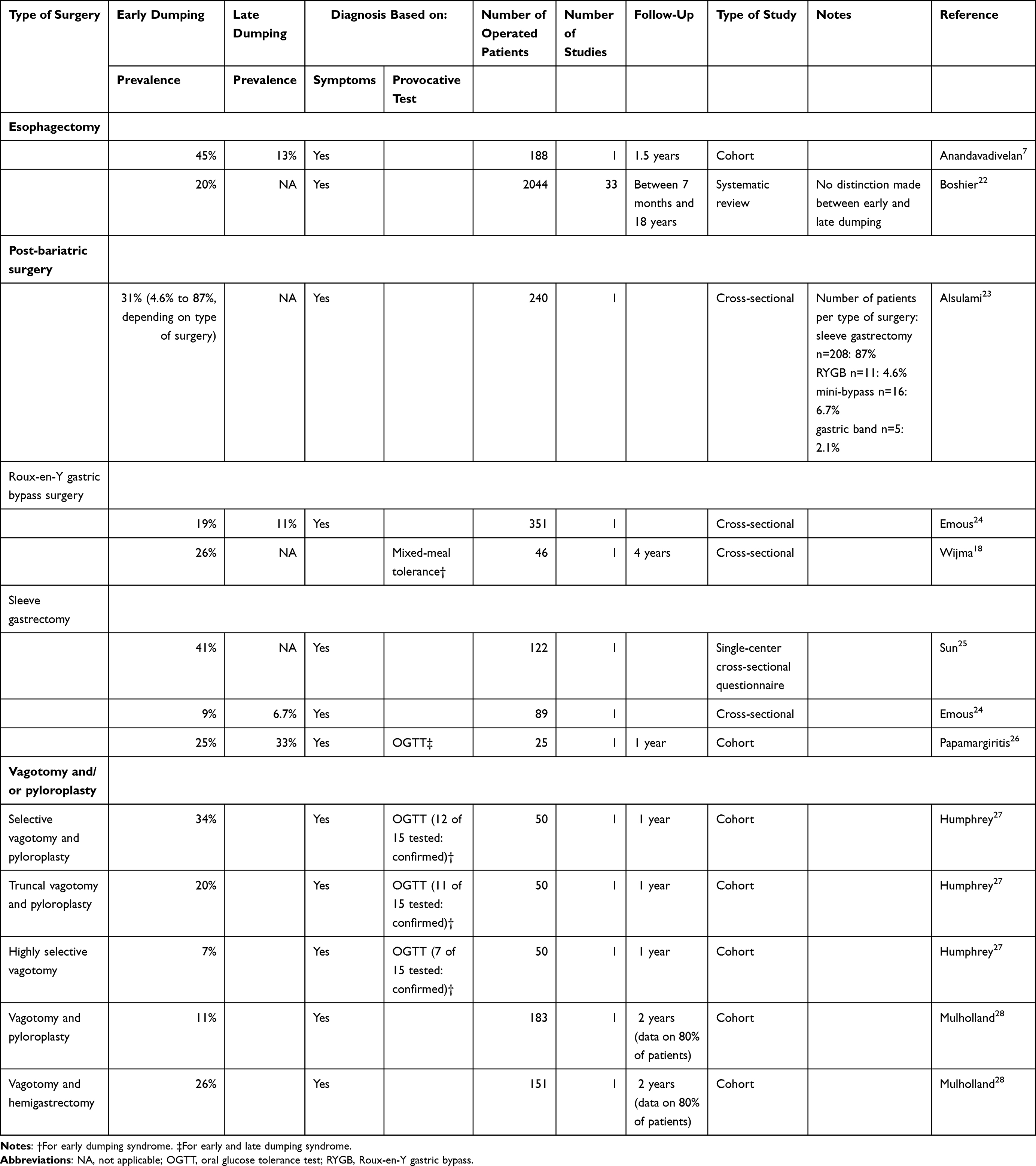 |
Table 1 Prevalence of Dumping Syndrome After Surgery |
Prevalence Based on Self-Reported Symptoms
When looking at the incidence and prevalence of dumping symptoms, widely varying occurrence of dumping symptoms has been reported in several studies, including systematic reviews (Table 1).22 Reported incidence and prevalence of dumping symptoms depend on whether symptoms are self-reported or based on the Sigstad’s diagnostic scoring system (Table 2). However, it is likely that underreporting of reactive hypoglycemia is likely in published case series. Early studies report on the presence of dumping symptoms in 11% of patients after vagotomy and pyloroplasty and 26% of patients after vagotomy and after vagotomy and hemigastrectomy for surgical treatment of duodenal ulcers.28 Early dumping symptoms are encountered in up to 45% of patients and late dumping symptoms in up to 13% of patients after esophagectomy.7 A systematic review reports on the presence of dumping symptoms in up to 78% of patients after esophagectomy.22 Post-gastrectomy (distal gastrectomy with Billroth I or Roux-en-Y reconstruction, proximal/total/pylorus preserving gastrectomy), self-reported symptoms of early dumping syndrome occur in around 67% of patients and of late dumping syndrome in 38% of patients after surgery for gastric cancer.29 With regard to post-bariatric surgery, presence of dumping symptoms differs per type of surgery performed. When RYGB and sleeve gastrectomy are combined, 31% of patients report experiencing dumping symptoms.23 For sleeve gastrectomy, the highest reported estimate of early dumping symptoms is 41%,25 whereas it is 26% after RYGB.18 The presence of late dumping symptoms was reported less frequently: in 11% of patients after RYGB and in 6.7% of patients after sleeve gastrectomy.24 Notably, late dumping symptoms appeared to occur more often in patients with revisional RYGB after an initial gastric band procedure compared to primary RYGB, perhaps because it is easier to damage the vagal nerve fibers during a second intervention (revisional RYGB) in the case of prior adhesions after gastric banding.24 When late dumping symptoms are present they are nearly always preceded by early dumping symptoms, whereas early dumping symptoms may occur separately.30
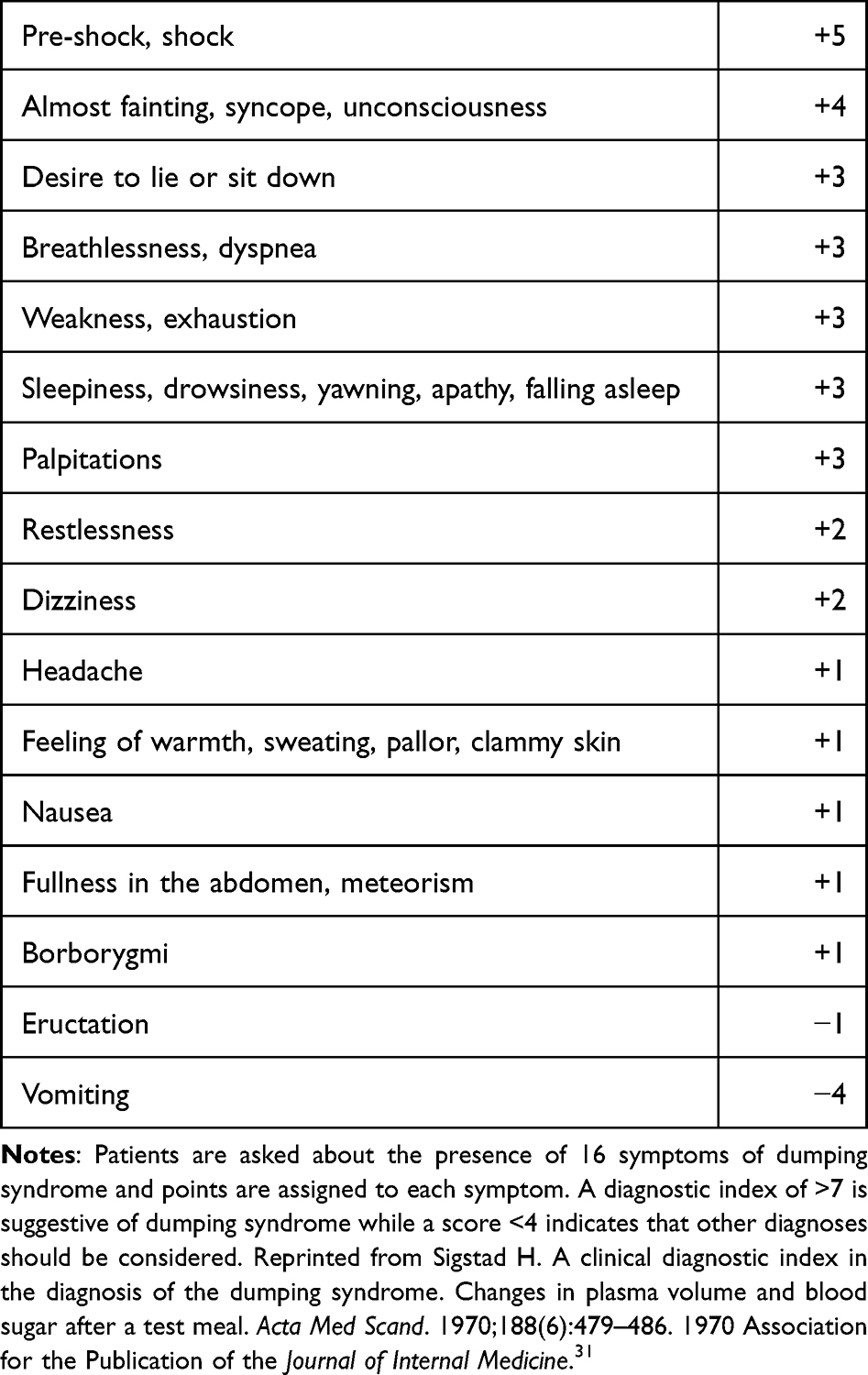 |
Table 2 Sigstad’s Diagnostic Index for the Diagnosis of Dumping Syndrome |
Dumping syndrome is also seen after anti-reflux surgery, such as Nissen fundoplication, but is mainly reported to occur in children.32–34 Potential causes for dumping syndrome after fundoplication include vagal nerve damage and impaired postprandial fundic accommodation. Vagal damage may occur in up to 20% of patients after anti-reflux surgery but dumping syndrome occurring after anti-reflux surgery is rare.35
In recent years, pyloric intervention (pyloroplasty or pyloromyotomy) has been introduced as a therapy for refractory gastroparesis. It remains unclear whether these procedures increase the risk of dumping syndrome. Even when taking earlier studies27,28 into account, with a varying presence of dumping after different degrees of vagotomy with or without pyloroplasty, uncertainty remains whether it is the vagotomy or pyloroplasty that causes dumping symptoms. In a recent study on the safety of gastric per oral endoscopic myotomy (G-POEM) in 217 patients with refractory gastroparesis, three patients were reported to have developed dumping symptoms after G-POEM however, this is without confirmation by provocative testing.36
Prevalence Based on Provocative Testing
Presence of dumping syndrome one year after surgery as assessed by a provocation test with oral hypertonic glucose ingestion is higher in patients who underwent selective vagotomy and pyloroplasty (80%; 12 of 15 tested patients) or truncal vagotomy and pyloroplasty (73%; 11 of 15 tested patients) as compared to a highly selective vagotomy (47%; 7 of 15 tested patients) (Table 1).27 Strikingly, this early study showed that clinical incidence of early dumping symptoms was much lower than when based on provocative testing: 34% after selective vagotomy and pyloroplasty, 20% after truncal vagotomy and pyloroplasty, and 7% after highly selective vagotomy.27 Provocative testing by a mixed-meal tolerance test showed that early dumping symptoms were present in 26% of patients (n=12) four years after RYGB.18 An increase in complaints of dumping symptoms after a mixed-meal test was seen in 46% of RYGB patients (22 out of 47 patients in total).21 Patients often develop late dumping syndrome after a longer post-operative period compared to early dumping symptoms. This is shown in a study including patients after RYGB who underwent an oral glucose tolerance test: the prevalence of late dumping syndrome was highest at the latest follow-up at 12 months (33%, n=4) as compared to 6 weeks or 6 months after surgery.26
In general, the prevalence of dumping symptoms is increasing over time as more upper gastrointestinal (GI) and bariatric surgical procedures are being performed. One should consider that patients have often changed eating patterns to reduce dumping symptoms prior to seeking medical advice. This hampers interpretation of the above-mentioned studies and estimates, as provocative testing is not uniformly or routinely performed.
Diagnosis of Dumping Syndrome
When is Testing Indicated?
Dumping syndrome should be suspected based on the concurrent presentation of typical systemic and abdominal symptoms in patients who have undergone upper GI or bariatric surgery. Unfortunately, in daily clinical practice a diagnosis of dumping syndrome is frequently missed and appropriate initiation of effective treatment is therefore delayed. In patients suspected of dumping syndrome, diagnosis can be established using symptom-based scores or questionnaires and provocation tests, with scoring of both symptoms and objective parameters. In every patient after bariatric surgery, upper GI oncologic surgery or anti-reflux surgery who presents with combined typical systemic and abdominal postprandial symptoms, dumping syndrome should be suspected.
Which Test Should Be Performed for Confirmation of Diagnosis?
In 1970, the Sigstad’s score was introduced to aid diagnosis of dumping by assigning points to each of 16 typical dumping symptoms (Table 2).31 The total sum of points is used to calculate a diagnostic index. A score of >7 is suggestive of dumping syndrome; a score of <4 indicates that other diagnoses should be considered. The Sigstad’s score was developed in the era of peptic ulcer surgery. It should be taken into account that the diagnostic accuracy of the Sigstad’s score has not been established in patients after bariatric surgery or upper GI oncological surgery. The dumping severity score developed by Arts et al37 is mainly used as an index of severity and was not designed for diagnostic purposes. The Dumping Symptom Rating Scale is a questionnaire that takes into account nine symptoms addressing early dumping syndrome.38 This scale has been validated in a large patient cohort.38 Unfortunately, responsiveness to therapy has not yet been evaluated.
Scores and questionnaires may prove helpful but the cornerstone of a clinical diagnosis of dumping is clinical awareness, patient medical history and a detailed investigation of typical postprandial symptoms. The occurrence of these typical systemic and abdominal postprandial symptoms in patients after bariatric or upper GI (oncological) surgery should make physicians suspect the presence of dumping syndrome. The Sigstad’s score has diagnostic value and both Sigstad’s and Arts scores may help to quantify the severity and impact of dumping symptoms. Dumping provocation tests may help to confirm the diagnosis in cases where dumping syndrome is uncertain or should be distinguished from other postprandially occurring disorders.
In its original report, Sigstad’s diagnostic questionnaire test was proposed to be combined with an oral glucose tolerance test (OGTT) in the diagnostic work-up of dumping.31 In addition to symptoms, objective signs such as a higher pulse rate and an increase in hematocrit were also used as indicators of hypovolemia. Later, hypoglycemia was added as a marker for late dumping. For diagnostic purposes the OGTT is still the preferred dumping provocation test. This test usually involves the ingestion of 50 or 75 grams of glucose in an aqueous solution. Blood concentrations of glucose, hematocrit level, pulse rate and blood pressure are measured at 15–30-minute intervals for up to 3 hours after the ingestion of the glucose solution. The test is considered positive for early dumping if early dumping symptoms are provoked and these symptoms are associated with an early increase in hematocrit level of more than 3% and/or by an episode of increased pulse rate by more than 10 beats per minute.10,11 For the diagnosis of late dumping after OGTT, symptoms of late dumping should be provoked in combination with a glycaemia below 3.3 mmol/L, usually occurring between 90 and 180 minutes after glucose ingestion.39–41 In other studies a cut-off level of 2.8 mmol/L was preferred, but at this level diagnostic sensitivity to late dumping is lower. In a recent international consensus report, a cut-off of 2.8 mmol/L was selected as definition of late dumping.5 In the past we have validated the dumping provocation test by defining cut-off values for hematocrit, pulse rate increase and late hypoglycemia (at 3.0 mmol/L) between dumping patients, healthy controls and asymptomatic patients after upper GI surgery.42 Dumping provocation using meals rich in rapidly absorbable carbohydrates appears more attractive since this is a greater physiological stimulus. However, this provocation test is less well standardized.5 For more than 30 years we used the OGTT dumping provocation test in cases where we doubted the diagnosis. It is important that the test is well standardized, that the patient is in a resting state and medical staff are familiar with the occurrence and management of symptomatic hypoglycemia. Several authors indicate that a beneficial response to octreotide (OCT) subcutaneous (s.c.) during provocation tests is important additional evidence for the diagnosis of dumping syndrome. Gastric emptying is a key mechanism in dumping syndrome; however, gastric emptying tests have low sensitivity and specificity for dumping syndrome and are therefore not recommended for diagnosis.5
Treatment Options
Therapy for dumping syndrome mainly relies on dietary and lifestyle adjustments. A schematic illustration of the treatment steps can be seen in Figure 1.
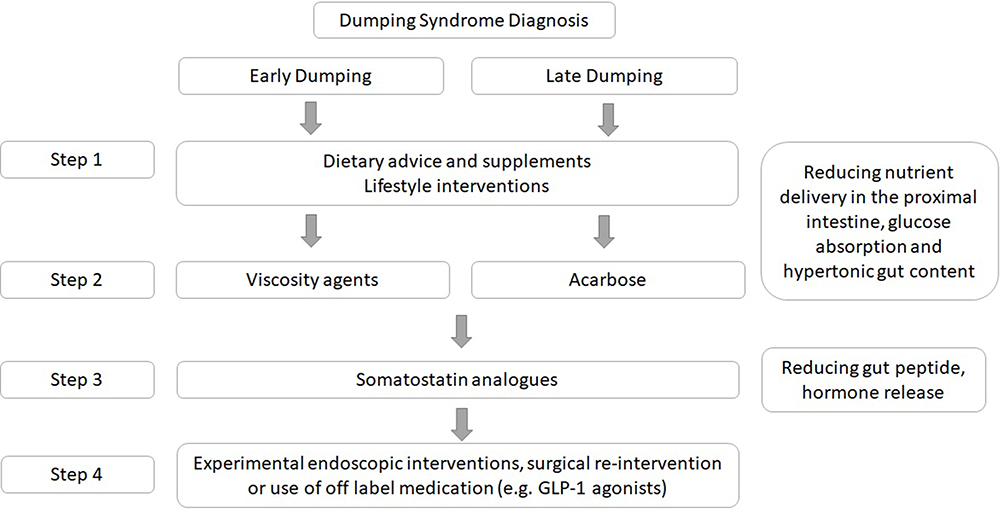 |
Figure 1 Stepwise approach for management of dumping syndrome. |
Diet
The first step in the management of dumping syndrome consists of dietary modifications. This step is essential and usually effective in patients with mild to moderate dumping symptoms. Patients with moderate to severe dumping usually avoid large meals and meals rich in rapidly absorbable carbohydrates to control symptoms. In post-bariatric patients and patients after oncologic surgery the occurrence of dumping syndrome is a risk factor for malnutrition. Nutritional support is essential and should include smaller and more frequent meals. Patients are advised to consume a diet high in fiber and rich in proteins, the latter to ensure sufficient caloric intake. Rapidly absorbable carbohydrates should be eliminated from the diet and dietary advice with education about the glycemic index of different foods is essential and requires referral to a dietician. It is advised to refrain from intake of fluids for at least 30 minutes after meals in order to delay gastrointestinal transit.5,43
In case of insufficient control of dumping symptoms with dietary measures, use of dietary supplements should be considered. Supplements such as guar gum, pectin and glucomannan increase chyme viscosity, delay gastrointestinal transport and reduce gut peptide release, thus contributing to better control of dumping symptoms and glucose homeostasis.5 Despite proven efficacy for managing dumping symptoms, the palatability, tolerability and patient acceptance of dietary supplements that increase chyme viscosity are poor. Behavioral interventions are indicated when aversion changes in eating patterns have occurred due to the invalidating postprandial discomfort caused by dumping.20 Ketogenic diets are increasingly popular nowadays for several indications such as diabetes mellitus and epilepsia. In this diet, carbohydrate intake is severely restricted and may result in a disruption of normal glucose homeostatic mechanisms. Hypoglycemic episodes have been described in people consuming ketogenic diets but without the classical symptoms of hypoglycemia.44 More information is needed on the long-term effects of this diet in general. Given the additional risk of hypoglycemia, ketogenic diets should not be advised for patients with dumping syndrome.
Acarbose
Acarbose is an alpha glycosidase hydrolase inhibitor that is taken before a meal (50 to 100 mg 3 times daily) to delay the conversion of oligosaccharides to monosaccharides in the small bowel that results in attenuated post-prandial hyperglycemia. It was widely used initially for the treatment of non-insulin-dependent diabetes mellitus. Its first use in dumping syndrome dates from the 1980s, when small-scale studies pointed to improvement in symptoms in patients with dumping syndrome, improvement in oral glucose tolerance test results, reduction of gastrointestinal hormone release and reduction in the incidence of hypoglycemia. Its use in daily clinical practice is limited due to side effects resulting from bacterial fermentation of unabsorbed carbohydrates in the colon leading to bloating, diarrhea and flatulence.45–47 Published studies have described acarbose improving late dumping symptoms while its effect on early dumping symptoms is only limited.
Somatostatin Analogues
Somatostatin (SST) is a brain–gut peptide that exerts its effects by interacting with specific receptors that belong to the family of G-protein coupled receptors. Five SST receptor subtypes have been identified (SSTR1-SSTR5). While all five subtypes are expressed in human tissue, the predominant subtypes in endocrine tissue are SSTR2 and SSTR5. SST inhibits the secretion of growth hormone, prolactin and various gastrointestinal peptides. SST also inhibits gastric, exocrine and endocrine pancreatic secretions and reduces intestinal blood flow. On one hand, it modulates gastrointestinal motility by inhibiting gallbladder motility, delaying gastric emptying (late phase) and intestinal transit time while, on the other hand, stimulating phase III of the migrating motor complex in the small intestine.
Octreotide (OCT) is a synthetic analogue of SST with pronounced gastrointestinal inhibitory effects including the inhibition of secretion of incretin hormones and insulin. OCT has an elimination half-life of 100–110 minutes. Since the 1980s octreotide has been registered for use in endocrine disorders, but not for dumping syndrome: the use of octreotide for dumping syndrome is still off-label. Several studies have clearly demonstrated the efficacy of repeated daily injections of OCT in preventing or significantly reducing symptoms of early and late dumping.10,37,48–54 It is generally agreed that OCT is the preferred treatment option for dumping symptoms in patients refractory to dietary measures and dietary supplements. Octreotide is already effective at doses of 25–50 microgram s.c. Based on frequency of dumping symptoms, it can be administered 1–3 times daily, 15–30 minutes before meal intake or upon patient’s preference or depending on intended caloric (carbohydrate) intake. Side effects such as steatorrhea, nausea and painful injection sites may occur. We have previously shown that, despite high efficacy, many patients discontinue short-acting OCT therapy because of pain at the injection site and the need for repeated daily s.c. injections.49,55
After an initial positive response to short-acting somatostatin analogues lasting from several weeks to months, patients can be converted to long-acting somatostatin analogues providing equal symptomatic benefit.5,9 Patients prefer long-acting formulations primarily because of the lower number of injections required: once every four weeks intramuscular instead of 1–3 times s.c. daily. Compared to short-acting SST, the long-acting SST analogues appear to be more effective in increasing body weight and improving quality of life.9 Dumping symptoms are reduced by 50%, and this efficacy remains present in long-term users both with short-acting and long-acting somatostatin analogues. Nevertheless, during a long-term follow-up (mean 55 months) in 34 patients with dumping syndrome, over 50% discontinued octreotide therapy because of side effects or insufficient symptomatic response.55 Body weight continued to increase during long-term octreotide therapy despite more pronounced steatorrhea.
Both Arts et al37 and Didden et al55 reported that, in patients with the most severe dumping symptoms, better symptom control was obtained with short-acting octreotide three times a day than with long-acting octreotide administered monthly. After a dose of 50 µg s.c. of short-acting octreotide, peak plasma concentrations are reached around 2–3 ng/mL within one hour, thereafter declining to zero within several hours, while with monthly 20 mg octreotide long-acting release (LAR), steady state concentrations of 1.2–1.5 ng/mL are reached.56 To prevent or reduce dumping symptoms high serum concentrations are needed but only in the first 1–2 postprandial hours.
Considerations to remember when prescribing somatostatin analogues to patients are that (1) gallbladder motility is diminished and up to 30% of patients develop gallbladder stones,55,57 and (2) inhibition of pancreatic enzyme secretion and of fat malassimilation/malabsorption may occur, resulting in steatorrhea.55,58 Didden et al55 found that steatorrhea was significantly higher during short-acting compared to long-acting somatostatin analogues.
With respect to long-acting somatostatin analogues, several formulations are on the market: depot long-acting octreotide, pasireotide and lanreotide. For lanreotide, a randomized placebo-controlled trial was in favor of the efficacy of lanreotide autogel on early dumping symptoms but not for late dumping symptoms.59 Pasireotide, a newer long-acting SST analogue, appeared to be equally effective in the prevention of hypoglycemia but treatment-related hyperglycemia was more frequently reported in patients receiving pasireotide treatment.60,61 Pasireotide has a higher binding affinity for the SSTR5 and similar affinity for the SSTR2 when compared to octreotide. Large-scale placebo-controlled studies or studies comparing the efficacy of long-acting SST analogues in dumping syndrome are lacking.
New Perspectives in Medical Interventions
Given that the pathophysiology of dumping syndrome is partly due to glucagon-like peptide-1 (GLP-1; a gut-derived incretin hormone secreted by the L cells mainly found in the ileum that stimulate insulin secretion from the pancreatic β cells), it was suggested that antagonizing the action of GLP-1 may lead to a reduction in postprandial hypoglycemic events.16 Although the exact mechanism remains unclear, we know from studies on glucagon-like peptide-1 receptor agonists (GLP-1RAs) in type 2 diabetes mellitus patients that GLP-1RAs delay gastric emptying, reduce postprandial hyperglycemia, promote insulin secretion, reduce β-cell workload and intestinal glucose absorption, and delay nutrient transit through the small intestine. GLP-1RAs avoid a postprandial peak in insulin release by mimicking native GLP-1 and blocking the GLP-1 receptor (as they are resistant to dipeptidyl peptidase-4 breakdown) and therefore may reduce hyperinsulinemic hypoglycemia episodes after bariatric surgery, as was recently analyzed in a systematic review.16 Successful use of GLP-1RAs has also been described in individual cases: a patient with postsurgical late dumping syndrome symptoms after Toupet fundoplication (liraglutide)14 and a patient after distal gastrectomy (beinaglutide)15 by reducing symptomatic postprandial hyperinsulinemic hypoglycemic events. The use of GLP-1RAs was not discussed in the clinical consensus guideline5 and is currently not advised for routine clinical care in dumping syndrome.
Sodium-glucose cotransporter inhibitors (SGLTi) are a new class of drugs that play an increasingly important role in the treatment of type 2 and possibly also type 1 diabetes mellitus. Studies have shown that SGLTi reduce carbohydrate absorption by inhibiting SGLT and thus decreasing the postprandial insulin spike, thereby potentially preventing PPH. Indeed, in a small-scale study with 21 patients, the SGLT-1 inhibitor canagliflozin reduced over 85% of the hypoglycemic episodes in patients with severe postprandial hypoglycemia.62 This class of drugs deserves further evaluation in patients with severe dumping syndrome, especially late dumping. In case reports, the efficacy of diazoxide and calcium channel blockers was demonstrated in patients with postprandial hypoglycemia by reducing the severity of hypoglycemia via a reduction in postprandial insulin secretion.63
Surgical Re-Intervention
After conservative steps have failed to manage symptoms of dumping syndrome, continuous enteral feeding or surgical interventions can be considered.17 Continuous enteral feeding by a jejunostomy or tube in the remnant stomach avoids symptoms triggered by meals but is invasive, associated with complications and has therefore a limited place in the management of dumping syndrome.64 Depending on the initial type of surgery, several interventional procedures have been proposed and described:17 pouch restriction, bypass reversal, interposed jejunal loops and even pancreatic resection.65–67 Surgical re-intervention after RYGB can be technically challenging, first, as a result of altered anatomy and, second, because of adhesions, resulting in a higher number of adverse events and vagal nerve damage.24 When surgical re-intervention (after RYGB or sleeve gastrectomy) including reversal to normal anatomy is considered, one should verify whether the symptoms will improve if a feeding tube is placed through the remnant stomach or bypasses the small bowel prior to reconnecting the gastric pouch to the remnant stomach. The consensus guideline on dumping syndrome, however, recommends a restrictive approach to surgical re-intervention, first, because the long-term outcome of re-intervention is unclear and, second, the optimal procedure has not yet been established.5 Up-to-date studies on surgical re-intervention are relatively small, have short follow-up periods, are not consistent in terms of diagnosis of dumping syndrome, and do not include a control arm. Therefore, conservative methods should be preferred in the case of dumping syndrome whilst also taking into account spontaneous improvement of symptoms and gradual adaptation over time.
New Developments in Surgical and Endoscopic Intervention
A variety of surgical and endoscopic procedures to address refractory dumping syndrome have been reported in the literature. Currently, these procedures are certainly not considered as standard because of technical and methodological challenges and wide variation in symptomatic response outcomes. Additionally, in these studies the definition and diagnosis of dumping syndrome employed vary considerably and include patients who are poorly characterized. Furthermore, data on the natural course of dumping syndrome are lacking, eg whether patients improve over time remains unclear. From clinical experience, we have learned that the severity of dumping symptoms may gradually diminish over time. However, in a small proportion of patients debilitating symptoms remain present, despite combined dietary and medical interventions. Taking into account the limitations described above, a few newly-developed therapeutic techniques are described below.
Targets of endoscopic or surgical interventions may include the delay of gastric emptying. After RYGB surgery, endoscopic therapy may help to reduce the diameter of a dilated or incompetent gastrojejunal anastomosis in order to delay gastric pouch emptying. In the literature, this procedure is referred to as transoral outlet reduction (TORe),68–70 or endoscopic gastrojejunostomy revision (EGJR), or revision of the gastrojejunal anastomosis (GJA).71–74 A systematic review to evaluate the effects of this technique included 6 studies, of which only 1 was prospective while the others were retrospective reports.71 Technical and clinical success was reported in 98% and 89% of patients, respectively, with a re-intervention rate of 11.5%, taking into account that different devices were used for revision of the gastrojejunal anastomosis.71 A recent retrospective study with two years of follow-up after gastrojejunal anastomosis reduction reported that, among 58 patients with dumping syndrome, the symptoms and Sigstad’s score improved in 69% (n=40 out of 58) of patients and in 57% (n=20 out of 35) a complete resolution of Sigstad’s score.73 Notably, in that study follow-up at 2 years was only complete in 64% of patients. An alternative method to reduce the pyloric diameter is by use of argon plasma coagulation (APC) on the anterior and apical surface of the pylorus and by using hemoclips. This has been described in one female patient with dumping syndrome after sleeve gastrectomy.75
Despite endoscopic reduction of the gastrojejunostomy being reported as a relatively safe procedure, this technique requires further clinical prospective evaluation. It is important that well-designed studies include patients prospectively and evaluate dumping diagnosis and efficacy according to a structured protocol before its use is considered in routine clinical practice.
One case report described a modified duodenal switch with pyloric restoration and shortening of bowel length after RYGB improving subjective intractable dumping syndrome symptoms.76
Apart from a possible target of therapy as a delay in gastric pouch emptying, slowing the esophageal passage of food to the gastric pouch is also reported to be a target for intervention in dumping syndrome.77 A case report on a modified Nissen fundoplication after RYGB – by creating a cuff around the esophageal–gastric junction with the fundus of the remnant stomach – showed clinical success in managing dumping syndrome symptoms in one female patient. As the follow-up was rather short, the occurrence of late complications after surgery, such as dysphagia, esophageal stasis or recurrent symptoms remains unclear.77
Use of the above-mentioned experimental surgical and endoscopic techniques has resulted in impressive success rates in otherwise therapy-refractory patients. These techniques are currently certainly not ready for implementation in daily clinical practice.5
Conclusions
In recent decades, the face (clinical presentation) of dumping syndrome has not changed. Dumping is still related to a postoperative state of the upper gastrointestinal tract with an accelerated nutrient delivery. Over the last 40 to 50 years, the indications for upper GI surgery have shifted from benign ulcer disease to oncological causes and severe obesity (bariatric surgery). Clinicians’ awareness of the typical symptoms of early and late dumping is crucial. The occurrence of dumping symptoms within a typical fixed timeframe after meal ingestion combined with objective signs of hypovolemia for early dumping (0–60 minutes postprandially) and symptomatic hypoglycemia (60–180 minutes postprandially) confirm the diagnosis. Provocation tests have additional value in diagnosis of dumping syndrome. There is limited evidence of high quality treatment options. Diet and therapy with short-acting and long-acting somatostatin analogues are effective in most patients. The second step of therapy includes dietary supplements (viscosity agents) or acarbose, which is effective for late dumping symptoms; however, their use is limited due to side effects. Long-term compliance with therapy involving somatostatin analogues should be improved. Here, the use of patient reported outcome measures and shared decision making is essential. On-demand incidental therapy with low doses of subcutaneous octreotide is an alternative to continuous use somatostatin analogues, for instance when patients go out for dinner or attend social events. Medical interventions with GLP-1 receptor agonists and possibly also SGLT-inhibitors, continuous enteral nutrition, endoscopic and surgical (re)interventions are reported as treatment options for refractory dumping syndrome. However, their routine use is not recommended in clinical practice due to limited evidence and uncertainty of outcomes. These alternatives should be considered only as last-resort options in patients with otherwise refractory and invalidating dumping syndrome.
Abbreviations
APC, Argon Plasma Coagulation; CGM, Continuous Glucose Monitoring; EGJR, Endoscopic Gastrojejunostomy Revision; GI, Gastrointestinal; GIP, Glucose-dependent Insulinotropic Peptide; GJA, Gastrojejunal Anastomosis; GLP-1, Glucagon-like Peptide-1; GLP-1RA, Glucagon-like Peptide-1 Receptor Agonist; G-POEM, Gastric Per Oral Endoscopic Myotomy; LAR, Long Acting Release; OCT, Octreotide; OGTT, Oral Glucose Tolerance Test; PPH, Postprandial Hypoglycemia; RYGB, Roux-en-Y Gastric Bypass; s.c., Subcutaneous; SGLTi, Sodium-Glucose co-Transporter inhibitors; SST, Somatostatin; TORe, Transoral Outlet Reduction.
Disclosure
Professor Ad AM Masclee reports grants from the Dutch Cancer Society and Pentax GMBH outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Hertz AF. The Cause and Treatment of Certain Unfavorable After-effects of Gastro-enterostomy. Ann Surg. 1913;58(4):466–472. doi:10.1097/00000658-191310000-00004
2. Denehau D. Les suites medicales eloigneés de la gasteroenterostomie au cours d’ulcer de stomach et de ses complications. Syndrome de dyspeptique secondaire a la gastroenterostomie. Paris: These pour le doctorat en médécine; 1907.
3. Andrews EW. “Dumping stomach” and other results of gastrojejunostomy: operative cure by disconnecting old stoma. Surg Clin. 1920;4:883.
4. Mix CL. Dumping stomach following gastrojejunostomy. Surg Clin North Am. 1922;2:617–622.
5. Scarpellini E, Arts J, Karamanolis G, et al. International consensus on the diagnosis and management of dumping syndrome. Nat Rev Endocrinol. 2020;16(8):448–466. doi:10.1038/s41574-020-0357-5
6. Guyatt G, Oxman AD, Akl EA, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383–394. doi:10.1016/j.jclinepi.2010.04.026
7. Anandavadivelan P, Wikman A, Malberg K, et al. Prevalence and intensity of dumping symptoms and their association with health-related quality of life following surgery for oesophageal cancer. Clin Nutr. 2021;40(3):1233–1240. doi:10.1016/j.clnu.2020.08.005
8. Klevebro F, Boshier PR, Savva KV, et al. Severe Dumping Symptoms Are Uncommon Following Transthoracic Esophagectomy But Significantly Decrease Health-Related Quality of Life in Long-Term, Disease-Free Survivors. J Gastrointest Surg. 2021;25(8):1941–1947. doi:10.1007/s11605-020-04670-y
9. Penning C, Vecht J, Masclee AAM. Efficacy of depot long-acting release octreotide therapy in severe dumping syndrome. Aliment Pharmacol Ther. 2005;22(10):963–969. doi:10.1111/j.1365-2036.2005.02681.x
10. Hopman WP, Wolberink RG, Lamers CB, Van Tongeren JH. Treatment of the dumping syndrome with the somatostatin analogue SMS 201-995. Ann Surg. 1988;207(2):155–159. doi:10.1097/00000658-198802000-00007
11. Vecht J, Masclee AA, Lamers CB. The dumping syndrome. Current insights into pathophysiology, diagnosis and treatment. Scand J Gastroenterol Suppl. 1997;223:21–27.
12. Tulassay Z, Tulassay T, Gupta R, Rascher W. Atrial natriuretic peptide in dumping syndrome. Digestion. 1993;54(1):44–47. doi:10.1159/000201010
13. Johnson LP, Sloop RD, Jesseph JE. Etiologic significance of the early symptomatic phase in the dumping syndrome. Ann Surg. 1962;156(2):173–179. doi:10.1097/00000658-196208000-00002
14. Chiappetta S, Stier C. A case report: liraglutide as a novel treatment option in late dumping syndrome. Medicine. 2017;96(12):e6348. doi:10.1097/MD.0000000000006348
15. Ding B, Hu Y, Yuan L, Yan RN, Ma JH. Effectiveness of beinaglutide in a patient with late dumping syndrome after gastrectomy: a case report. Medicine. 2021;100(21):e26086. doi:10.1097/MD.0000000000026086
16. Llewellyn DC, Logan Ellis H, Aylwin SJB, et al. The efficacy of GLP-1RAs for the management of postprandial hypoglycemia following bariatric surgery: a systematic review. Obesity. 2023;31(1):20–30. doi:10.1002/oby.23600
17. van Beek AP, Emous M, Laville M, Tack J. Dumping syndrome after esophageal, gastric or bariatric surgery: pathophysiology, diagnosis, and management. Obes Rev. 2017;18(1):68–85. doi:10.1111/obr.12467
18. Wijma RB, Emous M, van den Broek M, Laskewitz A, Kobold ACM, van Beek AP. Prevalence and pathophysiology of early dumping in patients after primary Roux-en-Y gastric bypass during a mixed-meal tolerance test. Surg Obes Relat Dis. 2019;15(1):73–81. doi:10.1016/j.soard.2018.10.004
19. Lupoli R, Lembo E, Ciciola P, Schiavo L, Pilone V, Capaldo B. Continuous glucose monitoring in subjects undergoing bariatric surgery: diurnal and nocturnal glycemic patterns. Nutr Metab Cardiovasc Dis. 2020;30(11):1954–1960. doi:10.1016/j.numecd.2020.06.029
20. Bettini S, Belligoli A, Fabris R, Busetto L. Diet approach before and after bariatric surgery. Rev Endocr Metab Disord. 2020;21(3):297–306. doi:10.1007/s11154-020-09571-8
21. van Furth AM, de Heide LJM, Emous M, Veeger N, van Beek AP. Dumping Syndrome and Postbariatric Hypoglycemia: supporting Evidence for a Common Etiology. Surgery Obesity Related Dis. 2021;17(11):1912–1918. doi:10.1016/j.soard.2021.05.020
22. Boshier PR, Huddy JR, Zaninotto G, Hanna GB. Dumping syndrome after esophagectomy: a systematic review of the literature. Dis Esophagus. 2017;30(1):1–9. doi:10.1111/dote.12488
23. Alsulami I, Fathaldin A, Alghamdi T, et al. Prevalence of Dumping Syndrome and Its Determinants Among Post-Bariatric Surgery Adult Patients at King Fahad General Hospital, Jeddah, 2019-2020. Cureus. 2022;14(12):e32630. doi:10.7759/cureus.32630
24. Emous M, Wolffenbuttel BHR, van Dijk G, Totté E, van Beek AP. Long-term self-reported symptom prevalence of early and late dumping in a patient population after sleeve gastrectomy, primary, and revisional gastric bypass surgery. Surg Obes Relat Dis. 2018;14(8):1173–1181. doi:10.1016/j.soard.2018.04.011
25. Sun W, Zhang Y, Shen Q, Zhang W, Yao Q, Yang Y. Prevalence and risk factors for symptoms suggestive of hypoglycemia and early dumping syndrome after sleeve gastrectomy. Surg Obes Relat Dis. 2019;15(9):1439–1446. doi:10.1016/j.soard.2019.06.026
26. Papamargaritis D, Koukoulis G, Sioka E, et al. Dumping Symptoms and Incidence of Hypoglycaemia After Provocation Test at 6 and 12 Months After Laparoscopic Sleeve Gastrectomy. Obes Surg. 2012;22(10):1600–1606. doi:10.1007/s11695-012-0711-3
27. Humphrey CS, Johnston D, Walker BE, Pulvertaft CN, Goligher JC. Incidence of dumping after truncal and selective vagotomy with pyloroplasty and highly selective vagotomy without drainage procedure. Br Med J. 1972;3(5830):785–788. doi:10.1136/bmj.3.5830.785
28. Mulholland M, Morrow C, Dunn DH, Schwartz ML, Humphrey EW. Surgical treatment of duodenal ulcer: a prospective randomized study. Arch Surg. 1982;117(4):393–397. doi:10.1001/archsurg.1982.01380280001001
29. Mine S, Sano T, Tsutsumi K, et al. Large-scale investigation into dumping syndrome after gastrectomy for gastric cancer. J Am Coll Surg. 2010;211(5):628–636. doi:10.1016/j.jamcollsurg.2010.07.003
30. Ahmad A, Kornrich DB, Krasner H, et al. Prevalence of Dumping Syndrome After Laparoscopic Sleeve Gastrectomy and Comparison with Laparoscopic Roux-en-Y Gastric Bypass. Obes Surg. 2019;29(5):1506–1513. doi:10.1007/s11695-018-03699-y
31. Sigstad H. A clinical diagnostic index in the diagnosis of the dumping syndrome. Changes in plasma volume and blood sugar after a test meal. Acta Med Scand. 1970;188(6):479–486. doi:10.1111/j.0954-6820.1970.tb08072.x
32. Villet R, Boureau M, Hayat P, Weisgerber G. Dumping syndrome, a serious complication of Nissen’s opération a report of four cases (author’s transl). Chir Pediatr. 1978;19(4):269–273.
33. Zaloga GP, Chernow B. Postprandial hypoglycemia after Nissen fundoplication for reflux esophagitis. Gastroenterology. 1983;84(4):840–842. doi:10.1016/0016-5085(83)90155-5
34. Kreckler S, Dowson H, Willson P. Dumping syndrome as a complication of laparoscopic Nissen fundoplication in an adult. Jsls. 2006;10(1):94–96.
35. van Rijn S, Rinsma NF, van Herwaarden-Lindeboom MY, et al. Effect of Vagus Nerve Integrity on Short and Long-Term Efficacy of Antireflux Surgery. Am J Gastroenterol. 2016;111(4):508–515. doi:10.1038/ajg.2016.42
36. Baret F, Jacques J, Pioche M, et al. Evaluation of the safety profile of endoscopic pyloromyotomy by G-POEM: a French multicenter study. Therap Adv Gastroenterol. 2022;15:17562848221122472. doi:10.1177/17562848221122472
37. Arts J, Caenepeel P, Bisschops R, et al. Efficacy of the long-acting repeatable formulation of the somatostatin analogue octreotide in postoperative dumping. Clin Gastroenterol Hepatol. 2009;7(4):432–437. doi:10.1016/j.cgh.2008.11.025
38. Laurenius A, Olbers T, Näslund I, Karlsson J. Dumping syndrome following gastric bypass: validation of the dumping symptom rating scale. Obes Surg. 2013;23(6):740–755. doi:10.1007/s11695-012-0856-0
39. Emous M, Ubels FL, van Beek AP. Diagnostic tools for post-gastric bypass hypoglycaemia. Obes Rev. 2015;16(10):843–856. doi:10.1111/obr.12307
40. Calabria AC, Gallagher PR, Simmons R, Blinman T, De León DD. Postoperative surveillance and detection of postprandial hypoglycemia after fundoplasty in children. J Pediatr. 2011;159(4):597–601.e1. doi:10.1016/j.jpeds.2011.03.049
41. Roslin MS, Oren JH, Polan BN, Damani T, Brauner R, Shah PC. Abnormal glucose tolerance testing after gastric bypass. Surg Obes Relat Dis. 2013;9(1):26–31. doi:10.1016/j.soard.2011.11.023
42. van der Kleij FG, Vecht J, Lamers CB, Masclee AA. Diagnostic value of dumping provocation in patients after gastric surgery. Scand J Gastroenterol. 1996;31(12):1162–1166. doi:10.3109/00365529609036905
43. Vavricka SR, Greuter T. Gastroparesis and Dumping Syndrome: current Concepts and Management. J Clin Med. 2019;8(8):56.
44. Spoke C, Malaeb S. A Case of Hypoglycemia Associated With the Ketogenic Diet and Alcohol Use. J Endocr Soc. 2020;4(6):bvaa045. doi:10.1210/jendso/bvaa045
45. Ng DD, Ferry RJ Jr, Kelly A, Weinzimer SA, Stanley CA, Katz LE. Acarbose treatment of postprandial hypoglycemia in children after Nissen fundoplication. J Pediatr. 2001;139(6):877–879. doi:10.1067/mpd.2001.119169
46. Hasegawa T, Yoneda M, Nakamura K, et al. Long-term effect of alpha-glucosidase inhibitor on late dumping syndrome. J Gastroenterol Hepatol. 1998;13(12):1201–1206.
47. Speth PA, Jansen JB, Lamers CB. Effect of acarbose, pectin, a combination of acarbose with pectin, and placebo on postprandial reactive hypoglycaemia after gastric surgery. Gut. 1983;24(9):798–802. doi:10.1136/gut.24.9.798
48. Primrose JN, Johnston D. Somatostatin analogue SMS 201-995 (octreotide) as a possible solution to the dumping syndrome after gastrectomy or vagotomy. Br J Surg. 1989;76(2):140–144. doi:10.1002/bjs.1800760212
49. Vecht J, Lamers CB, Masclee AA. Long-term results of octreotide-therapy in severe dumping syndrome. Clin Endocrinol (Oxf). 1999;51(5):619–624. doi:10.1046/j.1365-2265.1999.00819.x
50. Tulassay Z, Tulassay T, Gupta R, Cierny G. Long acting somatostatin analogue in dumping syndrome. Br J Surg. 1989;76(12):1294–1295. doi:10.1002/bjs.1800761223
51. Geer RJ, Richards WO, O’Dorisio TM, et al. Efficacy of octreotide acetate in treatment of severe postgastrectomy dumping syndrome. Ann Surg. 1990;212(6):678–687. doi:10.1097/00000658-199012000-00005
52. Richards WO, Geer R, O’Dorisio TM, et al. Octreotide acetate induces fasting small bowel motility in patients with dumping syndrome. J Surg Res. 1990;49(6):483–487. doi:10.1016/0022-4804(90)90172-X
53. Gray JL, Debas HT, Mulvihill SJ. Control of dumping symptoms by somatostatin analogue in patients after gastric surgery. Arch Surg. 1991;126(10):1231–1235. doi:10.1001/archsurg.1991.01410340073010
54. Hasler WL, Soudah HC, Owyang C. Mechanisms by which octreotide ameliorates symptoms in the dumping syndrome. J Pharmacol Exp Ther. 1996;277(3):1359–1365.
55. Didden P, Penning C, Masclee AAM. Octreotide therapy in dumping syndrome: analysis of long-term results. Aliment Pharmacol Ther. 2006;24(9):1367–1375. doi:10.1111/j.1365-2036.2006.03124.x
56. Chanson P, Timsit J, Harris AG. Clinical pharmacokinetics of octreotide. Therapeutic applications in patients with pituitary tumours. Clin Pharmacokinet. 1993;25(5):375–391. doi:10.2165/00003088-199325050-00004
57. Dowling RH, Hussaini SH, Murphy GM, Wass JA. Gallstones during octreotide therapy. Digestion. 1993;54(Suppl 1):107–120. doi:10.1159/000201088
58. Witt K, Pedersen NT. The Long-Acting Somatostatin Analogue SMS 201-995 Causes Malabsorption. Scand J Gastroenterol. 1989;24(10):1248–1252. doi:10.3109/00365528909090795
59. Wauters L, Arts J, Caenepeel P, et al. Efficacy and safety of lanreotide in postoperative dumping syndrome: a Phase II randomised and placebo-controlled study. United Eur Gastroenterol J. 2019;7(8):1064–1072. doi:10.1177/2050640619862166
60. Deloose E, Bisschops R, Holvoet L, et al. A pilot study of the effects of the somatostatin analog pasireotide in postoperative dumping syndrome. Neurogastroenterol Motil. 2014;26(6):803–809. doi:10.1111/nmo.12333
61. Tack J, Aberle J, Arts J, et al. Safety and efficacy of pasireotide in dumping syndrome-results from a Phase 2, multicentre study. Aliment Pharmacol Ther. 2018;47(12):1661–1672. doi:10.1111/apt.14664
62. Ciudin A, Sánchez M, Hernandez I, et al. Canagliflozin: a New Therapeutic Option in Patients That Present Postprandial Hyperinsulinemic Hypoglycemia after Roux-en-Y Gastric Bypass: a Pilot Study. Obes Facts. 2021;14(3):291–297. doi:10.1159/000515598
63. Gonzalez-Gonzalez A, Delgado M, Fraga-Fuentes MD. Use of diazoxide in management of severe postprandial hypoglycemia in patient after Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2013;9(1):e18–9. doi:10.1016/j.soard.2011.05.010
64. McLaughlin T, Peck M, Holst J, Deacon C. Reversible hyperinsulinemic hypoglycemia after gastric bypass: a consequence of altered nutrient delivery. J Clin Endocrinol Metab. 2010;95(4):1851–1855. doi:10.1210/jc.2009-1628
65. Mala T. Postprandial hyperinsulinemic hypoglycemia after gastric bypass surgical treatment. Surg Obes Relat Dis. 2014;10(6):1220–1225. doi:10.1016/j.soard.2014.01.010
66. Xu Q, Zou X, You L, et al. Surgical Treatment for Postprandial Hypoglycemia After Roux-en-Y Gastric Bypass: a Literature Review. Obes Surg. 2021;31(4):1801–1809. doi:10.1007/s11695-021-05251-x
67. Vanderveen KA, Grant CS, Thompson GB, et al. Outcomes and quality of life after partial pancreatectomy for noninsulinoma pancreatogenous hypoglycemia from diffuse islet cell disease. Surgery. 2010;148(6):1237–1245. doi:10.1016/j.surg.2010.09.027
68. Matteo MV, Gallo C, Pontecorvi V, et al. Weight Recidivism and Dumping Syndrome after Roux-En-Y Gastric Bypass: exploring the Therapeutic Role of Transoral Outlet Reduction. J Pers Med. 2022;12(10). doi:10.3390/jpm12101664.
69. Relly R, Mati S, Aviv CN, Fishman S. Endoscopic trans-oral outlet reduction after bariatric surgery is safe and effective for dumping syndrome. Surg Endosc. 2021;35(12):6846–6852. doi:10.1007/s00464-020-08190-3
70. Hakiza L, Sartoretto A, Burgmann K, et al. Transoral Outlet Reduction (TORe) for the Treatment of Weight Regain and Dumping Syndrome after Roux-en-Y Gastric Bypass. Medicina. 2023;59(1). doi:10.3390/medicina59010125.
71. Bazarbashi AN, Dolan RD, McCarty TR, Jirapinyo P, Thompson CC. Endoscopic revision of gastrojejunal anastomosis for the treatment of dumping syndrome in patients with Roux-en-Y gastric bypass: a systematic review and meta-analysis. Surg Endosc. 2022;36(6):4099–4107. doi:10.1007/s00464-021-08731-4
72. Petchers A, Walker A, Bertram C, Feustel P, Singh TP, Zaman J. Evaluation of endoscopic gastrojejunostomy revision after Roux-en-Y gastric bypass for treatment of dumping syndrome. Gastrointest Endosc. 2022;96(4):639–644. doi:10.1016/j.gie.2022.04.1306
73. Pontecorvi V, Matteo MV, Bove V, et al. Long-term Outcomes of Transoral Outlet Reduction (TORe) for Dumping Syndrome and Weight Regain After Roux-en-Y Gastric Bypass. Obes Surg. 2023;33(4):1032–1039. doi:10.1007/s11695-023-06466-w
74. Tsai C, Steffen R, Kessler U, Merki H, Zehetner J. Short-term outcomes of endoscopic gastro-jejunal revisions for treatment of dumping syndrome after Roux-En-Y gastric bypass. Surg Endosc. 2020;34(8):3626–3632. doi:10.1007/s00464-019-07137-7
75. Yavuz A, Akan K, Ulaşoğlu C, Tuncer İ, Çolak Y. An Alternative Method for Treating Dumping Syndrome Using Hemoclips. Cureus. 2021;13(5):e14869. doi:10.7759/cureus.14869
76. Huang CK, Wang MY, Hsin MC, Chang PC. Conversion to modified duodenal switch for relieving intractable dumping syndrome and constipation after laparoscopic Roux-en-Y gastric bypass. Obes Surg. 2015;25(5):946. doi:10.1007/s11695-015-1607-9
77. Maurissen J, Yercovich N, Van Aelst P, Dillemans B. Modified Nissen Fundoplication for Late Dumping Syndrome After Roux-en-Y Gastric Bypass. Obes Surg. 2021;31(5):2353–2355. doi:10.1007/s11695-021-05310-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.