")
Back to Journals » Pragmatic and Observational Research » Volume 15
Drug Repurposing in Crohn’s Disease Using Danish Real-World Data
Authors Shakibfar S, Allin KH, Jess T, Barbieri MA, Battini V, Simoncic E, Kirchgesner J, Ulven T , Sessa M
Received 8 December 2023
Accepted for publication 8 February 2024
Published 21 February 2024 Volume 2024:15 Pages 17—29
DOI https://doi.org/10.2147/POR.S444569
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor David Price
Saeed Shakibfar,1 Kristine H Allin,2 Tine Jess,2 Maria Antonietta Barbieri,1,3 Vera Battini,1,4 Eva Simoncic,1 Julien Kirchgesner,5 Trond Ulven,1,* Maurizio Sessa1,*
1Department of Drug Design and Pharmacology, University of Copenhagen, Copenhagen, Denmark; 2Center for Molecular Prediction of Inflammatory Bowel Disease (PREDICT), Department of Clinical Medicine, Aalborg University, Copenhagen, Denmark; 3Department of Clinical and Experimental Medicine, University of Messina, Messina, Italy; 4Pharmacovigilance & Clinical Research, International Centre for Pesticides and Health Risk Prevention, Department of Biomedical and Clinical Sciences (DIBIC), ASST Fatebenefratelli-Sacco University Hospital, Università Degli Studi Di Milano, Milan, Italy; 5Department of Gastroenterology, INSERM, Institut Pierre Louis d’Epidémiologie Et de Santé Publique, AP-HP, Hôpital Saint-Antoine, Sorbonne Université, Paris, France
*These authors contributed equally to this work
Correspondence: Saeed Shakibfar, Department of Drug Design and Pharmacology, University of Copenhagen, Copenhagen, Denmark, Email [email protected]
Aim: Drug repurposing, utilizing electronic healthcare records (EHRs), offers a promising alternative by repurposing existing drugs for new therapeutic indications, especially for patients lacking effective therapies. Intestinal fibrosis, a severe complication of Crohn’s disease (CD), poses significant challenges, increasing morbidity and mortality without available pharmacological treatments. This article focuses on identifying medications associated with an elevated or reduced risk of fibrosis in CD patients through a population-wide real-world data and artificial intelligence (AI) approach.
Methods: Patients aged 65 or older with a diagnosis of CD from 1996 to 2019 in the Danish EHRs were followed for up to 24 years. The primary outcome was the need of specific surgical procedures, namely proctocolectomy with ileostomy and ileocecal resection as proxies of intestinal fibrosis. The study explored drugs linked to an increased or reduced risk of the study outcome through machine-learning driven survival analysis.
Results: Among the 9179 CD patients, 1029 (11.2%) underwent surgery, primarily men (58.5%), with a mean age of 76 years, 10 drugs were linked to an elevated risk of surgery for proctocolectomy with ileostomy and ileocecal resection. In contrast, 10 drugs were associated with a reduced risk of undergoing surgery for these conditions.
Conclusion: This study focuses on repurposing existing drugs to prevent surgery related to intestinal fibrosis in CD patients, using Danish EHRs and advanced statistical methods. The findings offer valuable insights into potential treatments for this condition, addressing a critical unmet medical need. Further research and clinical trials are warranted to validate the effectiveness of these repurposed drugs in preventing surgery related to intestinal fibrosis in CD patients.
Keywords: Crohn’s disease, drug repurposing, inflammatory bowel disease, intestinal fibrosis, machine-learning, real-world data
Introduction
Traditional drug development processes are widely recognized for their sluggishness and high costs.1,2 This sluggishness in drug development translates into prolonged periods before new drugs reach the pharmaceutical market, leaving patients with limited treatment options.1,2 In contrast, the steep expenses associated with drug development often mean that only those drug candidates deemed promising from the outset proceed to further stages. Currently, there are numerous diseases for which we lack effective pharmacological treatments.3 To expedite the development of therapies for these conditions, it is imperative to explore alternative avenues beyond conventional drug discovery methods, such as high-throughput screening of chemical compounds or approaches used for biologics and vaccines. One of the most promising alternatives, diverging from the conventional drug discovery route, is the repurposing of drugs using electronic healthcare records (EHRs). Drug repurposing involves harnessing existing drugs for indications other than their original intended use. This approach boasts several advantages, notably the already-established knowledge regarding their safety, pharmacokinetics, and pharmacodynamics. With the advent of big data, we now have the capacity to scrutinize thousands of pharmaceuticals already approved for use in the market for potential repurposing. While numerous studies have ventured into this domain, a considerable proportion either lacked epidemiological and clinical rationale or failed to incorporate state-of-the-art technologies.1
After conducting a thorough review of the scientific literature (Supplementary Material 1), to the best of our knowledge, drug repurposing using EHRs remains uncharted territory within the realm of inflammatory bowel diseases (IBDs) and, more specifically, in the context of intestinal fibrosis. Fibrosis, or scarring, is defined by an accumulation of excess extracellular components. It is essentially the formation of scar tissue that occurs because of inappropriate healing. Currently, there is no option to prevent intestinal fibrosis from developing, and there are very few treatments available. Patients who develop fibrosis typically have very poor outcomes, such as resections of sections of the intestinal tract. Among IBDs, Crohn’s disease (CD) has the highest incidence of developing intestinal fibrosis.3,4 Intestinal fibrosis occurs in a third of patients with CD and is associated with higher mortality and morbidity. Extensive intestinal fibrosis can cause a blockage in the bowel, leading to surgery as the only available treatment option at present. No pharmacological treatments are approved for intestinal fibrosis in CD.5,6 Therefore, this study aims to take advantage of extensive Danish real-world data (eg, EHRs and administrative databases) to identify existing drugs that could be repurposed to prevent the development the surgery related to intestinal fibrosis in patients with CD.
Materials and Methods
Data Source
Danish administrative and EHR databases were used as real-world data sources. These databases have a rich history of use in epidemiological research, as evidenced by numerous prior studies.7–9 Sociodemographic information on Denmark’s residents, including details such as age, gender, immigration, emigration, and more, was sourced from the Danish Civil Registration System.10 Data concerning hospitalizations, surgery and medical procedures, and redeemed medications from territorial pharmacies were obtained from the Danish National Patient Register11 and the Danish National Prescription Registry,12 respectively. Lastly, the date of death was obtained from the Danish Register of Causes of Death.13 These registers contained sufficient information to virtually trace the entire medical history of individuals included in the study population.
Study Design
Study Population
The study population consisted of all individuals aged 65 with a diagnosis of CD in Denmark during the period from 01/01/1996 to 01/01/2019. Individuals were considered to have CD if they received a hospital diagnosis with one of the following International Classification of Diseases 10th Revision, (ICD-10): K50. The Positive Predictive Value (PPV) of a single CD diagnosis in the Danish National Prescription Registry is 82% (95% Confidence Interval, 95% CI: 81%-83%).14 Baseline characteristics of the study population were presented as the mean age, the proportion of individuals of female sex, and the year of inclusion in the study population.
Follow-Up
The study population was followed for up to 24 years from the date of the initial CD diagnosis. This observation continued until the occurrence of the study outcome (ie, surgeries related to intestinal fibrosis), with censoring applied at the time of death or at the end of the data coverage.
Study Outcome
The study outcome was the need of specific surgical procedures, namely proctocolectomy with ileostomy and ileocecal resection following the Nordic Medico-Statistical Committee (NOMESCO) codes: KJFH40, KJFH20, KJFH21, KJFB20 and KJFB21).15 It is important to note that in Danish registries, the availability of reliable proxies for intestinal fibrosis is limited. As a result, we have chosen to utilize these surgical interventions as proxies for severe CD, including cases that may eventually develop fibrosis. While these proxies may not provide a comprehensive picture of intestinal fibrosis, they serve as valuable indicators of disease severity within the constraints of the available data. Of note, we assessed how many individuals had been diagnosed with an intestinal stricture (ICD-10 codes: K56.5–7; K62.4; K31.5) prior to the aforementioned surgeries.
Drugs Associated with an Increased Risk of the Study Outcome
In the first part of this study, we investigated treatments associated with an increased risk of developing the study outcome in individuals with CD. Within the study population, we identified individuals who had encountered the study outcome and conducted risk-set matching by choosing five individuals with CD matched for age and sex on the day of surgery (referred to as the index date). This matching process was performed among those individuals who, at the time of matching, had not experienced mortality, migration, or the study outcome. Adherence to these drugs was assessed using the Medication Possession Rate (MPR).
The potential drug candidates were selected during the year prior IBD diagnosis and their impact was assessed from CD diagnosis to outcome occurrence or end of follow-up. A single covariate assessment window was employed to generate the high-dimensional sets of variables aimed at identifying redeemed prescriptions that individuals were exposed to within 365 days before the first diagnosis of CD (ie, Covariate Assessment Window). Anatomical Therapeutic Chemical Classification codes (ATC codes) were systematically arranged based on their prevalence. Prevalence, in this context, indicates the proportion of individuals with a specific code recorded at least once during the covariate assessment window. The n most prevalent codes were selected as potential empirical covariates, considering the entire latest version of the ATC code for each medication. For the top n most prevalent ATC codes, we assessed how frequently each code was recorded for individual patients during the covariate assessment window. To represent this data, we created three binary variables for each code: (1) whether the code occurred once (no/yes), (2) whether the code occurred more times than the median number of occurrences, and (3) whether the code occurred more times than the 75th percentile number of occurrences. If a code exceeded the 75th percentile in terms of occurrence frequency, all three recurrence variables held a true value. In our data structure, this resulted in ATC codes, multiplied by n (the most prevalent codes within each data dimension), and further multiplied by 3 to account for the three recurrence variables (code occurred once, exceeded median occurrences, exceeded 75th percentile occurrences). This comprehensive approach led to a total of 3n covariates, in addition to sociodemographic characteristics, such as age and sex.
Given the high dimensionality of the analytical dataset, we performed features filtering based on variance. We systematically screened the entire list of features and removed variables that exhibited 99% identical values across individuals in the study population. The purpose of this filter is to eliminate features that primarily consist of noise and, therefore, have very little variation.16
For each individual exposed to the drug, at the time of their first use of the drug in the covariate assessment window (ie, index date), either individually or for all ATC codes that were not filtered, we employed risk-set matching to identify controls who were not exposed to the drug under investigation. Each individual exposed and not exposed to the drug under investigation was followed for 24 years from the index date up to the study outcome, censoring at the time of death or the end of the follow-up period. Crude and adjusted survival analysis were conducted to estimate the hazard ratio (HR) and generate cumulative hazard plots for the outcome using Cox regression. The adjusted HR was computed while adjusting for the High-Dimensional Propensity Score (HDPS) computed at the index date.17 The HDPS was computed using information on hospital admissions, redeemed prescriptions other than the drug under investigation, and surgical/non-surgical procedures. Proportionality of hazard was assessed using scaled Schoenfeld residuals.18
From the list of drugs associated with an increased risk of the study outcome, we performed a case-by-case analysis. This analysis involved a plenary discussion within the research team (MS, KA, AB, JK) to evaluate those associated with a heightened risk of protopathic bias.19 Only the drugs that were not excluded during the team discussion underwent further assessment using time-dependent approaches.
Specifically, to accommodate variations in covariates during the follow-up period, we applied Inverse Probability of Treatment Weighting (IPTW) and Inverse Probability of Censoring Weighting (IPCW) in conjunction with Marginal Structural Models (MSM). IPTW and IPCW were calculated using the HDPS at the end of each calendar year from the index date. Crude and adjusted risk differences between individuals exposed and those not exposed to the investigational drug were computed using MSM both with and without IPTW and IPCW, respectively.
Drugs That May Delay/Reduce the Risk of the Study Outcome
In the second part of this study, we investigated treatments associated with a reduced risk of the study outcome in individuals with CD.
We identified individuals in the study population who had experienced the study outcome. We then assessed all prescriptions redeemed by individuals included in the study population at community pharmacies in the year before their initial CD diagnosis. Adherence to these drugs was assessed using the MPR.
Subsequently, we examined the time interval from the initial diagnosis of CD to the development of the study outcome. By employing LASSO regression as a regularization technique, we identified drugs associated with a prolonged duration from the onset of CD to the study outcome. Our underlying assumption was that a drug administered from the beginning of CD, if it had a beneficial effect on slowing down the progression of intestinal fibrosis necessitating the study outcome, would result in an extended duration free from the need for this type of surgery. The purpose of this drug exposure was to potentially delay the progression toward the eventual outcome among individuals at risk of its development.
After we retrieved the list of drugs associated with a prolonged duration from the onset of CD to the study outcome, we used the entire population to identify those individuals exposed and not exposed to drugs in the aforementioned list. For each drug, we computed a high-dimensional set and filtered variables using variance with the same procedure explained in section 2.2.4.
Each individual exposed and not exposed to the drug under investigation were followed for 24 years from the index date, up to the study outcome, and censored at the time of death or the end of the follow-up period. Crude and adjusted survival analysis were used to estimate the HR and plotted the cumulative hazard for the outcome using a Cox regression. The adjusted HR was computed while adjusting for the HDPS calculated at the index date.17 The HDPS was computed using information on hospital admission, redeemed prescriptions other than the drug under investigation, and surgical/non-surgical procedures. The proportionality of hazard was checked using scaled Schoenfeld residuals.18
To account for variations in covariates during the follow-up period, we employed IPTW and IPCW in conjunction with MSM. IPTW and IPCW were calculated using the HDPS at the end of each calendar year from the index date. Crude and adjusted risk differences between those exposed and not exposed to the investigational drug were computed using MSM both with and without IPTW and IPCW, respectively.
The objective of this analysis was to explore whether administering a drug from the onset of CD influenced the development of the study outcome.
Sensitivity Analysis
A sensitivity analysis was conducted for drugs that may delay or reduce the risk of the study outcome using a more specific outcome definition. Specifically, we included only individuals who underwent ileocecal resection, identified by the NOMESCO codes KJFB20 and KJFB21 for intestinal stricture with code K50 listed as the main cause of surgery. The ultimate aim of this analysis was to further confirm drugs that demonstrated a protective effect for the study outcome using this narrower outcome definition.
Ethics
In Denmark, every patient record/information is pseudonymized before analysis, eliminating the need for informed consent or ethical approval in registry-based studies. The University of Copenhagen, where the analysis occurred, and Statistics Denmark (project number 707278) hold utilization data approval from the Regional Capital Area Data Protection Agency.
Results
Sociodemographic Characteristics
In total, 1029 individuals out of 9179 CD patients had the study outcome during the study period (11.2%) of which 476 (46.3%) had a diagnosis of intestinal stricture. The mean age (±SD) of individuals who underwent surgery for fibrosis was 76 (±7) years, whereas for individuals who did not undergo surgery for fibrosis, it was 78 (±8) years. The gender distribution was 41.5% women 58.5% men.
In Supplementary Material 2, we present several key visualizations to enhance our study’s methodology and findings. This includes a boxplot depicting the propensity score’s changes over time, calculated at the start of each year during the follow-up period. Additionally, we provide a graphical representation of the cumulative hazard for the study’s outcome, showing how the risk evolves over time. Finally, we offer a propensity score density comparison for individuals exposed to the drug under investigation at the date of first exposure to the drug under investigation versus those who were not exposed.
Drugs Associated with an Increased Risk of the Study Outcome
Altogether, 2440 features were created, and after filtering by variance, 32 of them were retained. These 32 features were related to drugs associated with an increased risk of the study outcome, and their HRs and incidence rates are provided in Figure 1.
 |
Figure 1 Hazard ratio of drugs associated with an increased risk of the study outcome. |
In total, 22 out of 32 drugs (69%) were associated with an increased risk of the study outcome due to protopathic bias. These drugs include azathioprine, hydroxocobalamin, metoclopramide, potassium chloride, proton pump inhibitors (pantoprazole, lansoprazole, omeprazole, and esomeprazole), IBD therapeutics (azathioprine, mesalazine, sulfasalazine), corticosteroids (betamethasone, hydrocortisone butyrate), antimicrobial agents (amoxicillin, metronidazole, ciprofloxacin, chloramphenicol, pivmecillinam, roxithromycin, and sulfamethizole), and analgesics (tramadol, codeine, and paracetamol).
In all, 10 out of 32 drugs (31%) were associated with an increased risk of the study outcome. These drugs include indomethacin, enalapril, bendroflumethiazide and potassium, furosemide, zolpidem, zopiclone, oxazepam, diazepam, citalopram, and estradiol. This association was further confirmed in time-dependent analyses (Figure 2).
 |
Figure 2 Risk difference of drugs associated with an increased risk of the study outcome. |
In Supplementary Material 3 we provided the median MPR of the 10 drugs confirmed in time-dependent analyses.
Drugs Associated with a Delayed/Preventive Risk of the Study Outcome
A total of 1174 features were generated one year before the onset of CD in intestinal fibrosis cases. After filtering with LASSO using log(λ) = 4.5, 16 features were retained to achieve optimal feature selection (Figure 3). In Figure 3, we demonstrated that by monitoring how the Mean-Squared Error (MSE) changes with the number of variables included in the LASSO model, we could identify the point at which adding more variables did not significantly improve the model’s predictive performance. This finding indicates the optimal number of variables needed to achieve a balance between model parsimony and predictive accuracy.
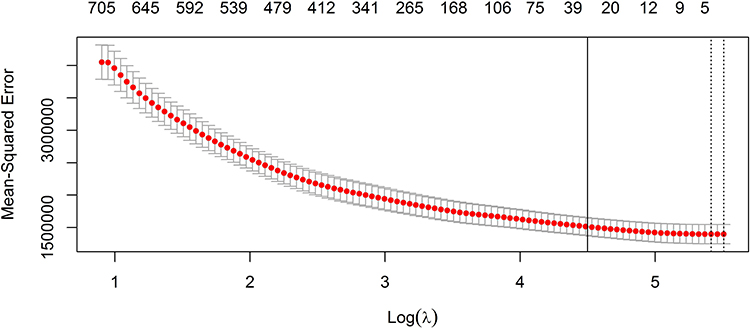 |
Figure 3 Lasso regression for variable selection prolonging time interval from CD to the study outcome. Log(λ) = 4.5 was chosen to get the optimal number of features. |
These 16 features were linked to drugs that prolonged the time interval from the initial diagnosis of CD and the study outcome. When we compared individuals exposed to these drugs with those not exposed, we observed a reduced risk of the study outcome. The results of the survival analyses are presented in Figure 4. In Figure 4, we presented a list of drugs that exhibited a statistically significant HR below 1, indicating a reduced risk of the study outcome. These drugs include erythromycin, metformin, levocabastine, fexofenadine, levothyroxine, glucosamine, fluticasone, clopidogrel, tolterodine, glyceryl trinitrate, isosorbide, decusate sodium, quetiapine, montelukast, disulfiram, and epinephrine.
 |
Figure 4 Hazard ratio of drugs associated with a prolonged time interval from the initial diagnosis of CD to the study outcome. |
Only 10 of these associations were subsequently confirmed in time-dependent analyses, (Figure 5). In Figure 5, we displayed a list of drugs demonstrating a risk difference below 1 in our time-dependent analyses, signifying a reduced risk of the study outcome. These drugs comprised fexofenadine, fluticasone, levocabastine, decusate sodium, quetiapine, montelukast, levothyroxine, disulfiram, epinephrine, and tolterodine.
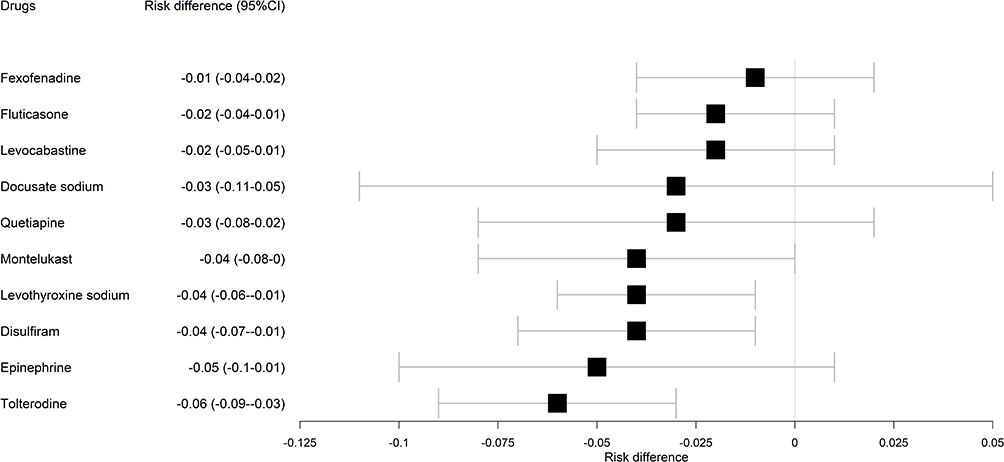 |
Figure 5 Risk difference of drugs associated with an increased time interval from CD diagnosis date to the study outcome date. |
In Supplementary Material 3 we provided the median MPR of the 10 drugs confirmed in time-dependent analyses.
Sensitivity Analysis
Due to the lack of statistical power, in the sensitivity analysis, we confirmed four drugs with a prolonged time to the outcome, specifically fluticasone, glucosamine, glyceryl nitrate, and clopidogrel (Supplementary Material 4).
Discussion
The findings from this study provided valuable insights into the relationship between drug exposure and the occurrence of surgery related to intestinal fibrosis in patients with CD. The study observed a cohort of 9179 CD patients, among whom 1029 individuals (11.2%) underwent surgery related to intestinal fibrosis during the study period. Intestinal fibrosis is a process characterized by the excessive deposition of fibrous tissue in the walls of the intestine. This fibrosis can lead to complications such as strictures, which are abnormal narrowing of the intestinal passage. In the context of CD, intestinal fibrosis is often associated with chronic inflammation and can contribute to the need for surgical intervention.20 The connection between intestinal fibrosis and our surgery outcomes lies in the impact of fibrosis on the structure and function of the intestine. When fibrosis occurs, it can lead to the formation of strictures or scar tissue, causing a narrowing of the intestinal lumen. This narrowing can obstruct the normal flow of contents through the intestine, leading to symptoms such as abdominal pain, bloating, and changes in bowel habits, necessitating surgery.21,22
The study aimed to investigate the impact of various drugs on the risk of the study outcome. A total of 32 drug-related features were identified as potential contributors to this outcome. Interestingly, 22 out of these 32 drugs (69%) were associated with an increased risk of the study outcome due to protopathic bias. It is important to consider the concept of protopathic bias, which implies that these drugs might have been prescribed to patients due to early symptoms of CD that eventually led to the study outcome. This highlighted the need for cautious interpretation of the causal relationship between these drugs and surgery. The implicated drugs encompassed a wide spectrum of medications, some of which are approved for the treatment of CD itself, such as azathioprine, mesalazine, sulfasalazine, and corticosteroids.23 Additionally, several drugs used to manage CD-related complications, including proton pump inhibitors for gastrointestinal ulcers, hydroxocobalamin for vitamin B12 deficiency, potassium supplements for malabsorption-related issues, and antimicrobial agents for conditions like fistulas or abscesses, were linked to an increased risk of the study outcome. For instance, metronidazole, an antibiotic, is sometimes employed in CD treatment, especially when complications like fistulas or abscesses occur.24 CD patients may also experience electrolyte imbalances, such as hypokalemia, due to factors like diarrhea or nutrient malabsorption. Healthcare providers may recommend potassium supplementation, which may include potassium chloride, to address these deficiencies.25 The interplay between these drugs and CD, as well as their impact on the progression of the disease and the subsequent need for surgical intervention, highlighted the complexity of CD management and the importance of a nuanced approach when selecting and prescribing medications for affected individuals. Prior research indicated that steroid therapy during the initial treatment of CD and the presence of deep ulcers in the intestinal tract were factors predictive of the development of intestinal strictures in CD patients.26
Conversely, 10 out of the 32 drugs (31%) were identified as having an increased association with the study outcome without the influence of protopathic bias. This suggested that these medications might have genuinely posed a risk to patients with CD, warranting further investigation and careful evaluation. Time-dependent analyses reinforced and validated this association, underscoring the significance of these findings. This strengthened the credibility of the study, highlighting that certain drugs do indeed play a role in the surgical outcomes for CD patients. One of the notable drugs in this category was indomethacin, a cyclooxygenase inhibitor, which has been found to potentially exacerbate fibrosis by interfering with the anti-fibrotic effects of cyclooxygenase 2.27 Depression is a common issue in patients with IBD, affecting approximately 21.2% of individuals with IBD and increasing to 34.7% among those with active disease. It’s crucial to recognize that depression is not merely an emotional concern but has significant implications for disease management and outcomes. It is associated with heightened disease activity, reduced quality of life, and can predict the future risk of relapses, the need for surgery, and hospitalization.28–31 Additionally, over 75% of individuals with active IBD, including CD, experience sleep disturbances. Research has shown that sleep disturbances were predictive of symptom flares.32,33 Drugs like zolpidem, zopiclone, citalopram, diazepam, and oxazepam are often prescribed for conditions related to depression, anxiety, and sleep disorders. Their inclusion in this context is noteworthy, as it may potentially reflect severity of IBD and hence would be expected to associate with later surgery quality, as measured by the Pittsburgh Sleep Quality Index, in relation to the likelihood of surgery or hospitalization among CD patients. This study also revealed increased usage of benzodiazepines and psychiatric medications in these cases, signifying a potential overlap between the treatment of anxiety and sleep disorders. The association with psychiatric medication use further suggested a potential burden of mood disorders associated with poor sleep quality in the CD population, possibly contributing to the risk of surgery.34 Furthermore, another study indicated that patients with CD exposed to antidepressants had an increased risk of CD-related surgery, underlining the complexity of these relationships within the realm of CD management and the impact of medication choices on surgical outcomes, including intestinal fibrosis.35 However, it is unclear if the observed associations have to be considered related to the disease or their treatments.
Regarding enalapril, the results are highly controversial. The renin-angiotensin system (RAS) is traditionally associated with cardiovascular and renal functions. However, emerging research has shown that components of the RAS, including angiotensin-converting enzyme (ACE) and renin, are also found in the small and large intestines. In the context of IBD, there is evidence to suggest that ACE is present at higher concentrations within the inflamed tissues of the intestine. This observation indicates that the RAS, with its various components, could be involved in the pathogenesis of inflammation and fibrosis within the intestinal tissue of individuals with IBD.36 Nevertheless, the role of specific medications like ACE inhibitors (such as enalapril) in this context is not fully understood. In several studies the likelihood of intestinal resection was significantly lower with the use of ACE inhibitors.37,38 However, in patients with CD, there were no significant differences in operations before or during ACE inhibitors use.37 More research is needed to determine the implications and potential therapeutic approaches related to the RAS in IBD.
Some diuretics, such as furosemide and bendroflumethiazide, have the potential to influence the activity of thiopurine S-methyltransferase, an enzyme involved in the metabolism of thiopurines like azathioprine and 6-mercaptopurine, both primarily used to treat CD.39–41 This interaction could affect the effectiveness of CD treatment, potentially leading to a drug-drug interaction and impacting the progression of the disease, particularly in the context of intestinal fibrosis. However, the clinical significance of this effect is not entirely clear.
The use of oral contraceptives, which includes estradiol, was associated with an increased risk of CD42,43 as well as an elevated risk of requiring surgery.44 This risk seemed to be linked to the consistent and long-term use of these medications, particularly when they were used together.44
The application of LASSO feature selection resulted in the identification of 16 features that were linked to drugs associated with prolonged intervals between the initial diagnosis of CD and the study outcome. Remarkably, exposure to these drugs was associated with a reduced risk of surgery, suggesting that some drugs might offer a protective effect against the need for the study outcome in CD patients. Based on our current knowledge, no existing study definitively demonstrated the ability of these drugs to prevent the development of intestinal fibrosis. Nevertheless, the potential use of these medications in the treatment of CD could not be ruled out, because they might have the potential to delay the onset of complications such as intestinal obstruction frequently associated with fibrosis, by effectively controlling inflammation. Among these drugs, metformin held promise for potential benefits in the context of IBD, including CD. Its anti-inflammatory and antioxidant properties, along with its ability to enhance gut barrier integrity in both cellular and animal models of IBD, make it a compelling candidate. Furthermore, metformin’s capacity to restore gut microbiota in mice with colitis led to a reduction in intestinal inflammation.45 Moreover, oral glucosamine demonstrated anti-inflammatory effects in an experimental model of IBD.46 This suggested that glucosamine could potentially serve as a new functional food for individuals with IBD and may help in managing stricturing disease.47
Considering clopidogrel, it potentially inhibits the inflammatory factors in IBD and alleviates IBD symptoms. Earlier research indicated that clopidogrel enhanced the inhibition of platelet activation, platelet-leukocyte interaction, and P-selectin expression on CD40 lymphocytes through P2Y12 receptor inhibition, which might contribute to the resolution of IBD symptoms.48
The time-dependent analysis confirmed that ten drugs could have prevented surgery related to intestinal fibrosis in CD patients. Among them, fluticasone, a corticosteroid medication used to reduce inflammation, is often inhaled to treat conditions such as asthma and chronic obstructive pulmonary disease. In the context of CD, fluticasone could be employed to manage inflammation and alleviate CD-related symptoms.49–51
Moreover, montelukast, a leukotriene receptor antagonist used for treatment of asthma and allergy, was found associated to prevent colitis induced by rectal administration of acetic acid. This experimental model simulated a form of IBD, and the results suggested that montelukast effectively reduced the resulting inflammation. The observed effect seemed to have been, at least partially, linked to its modulation of the nitric oxide-cGMP-KATP channel pathway.52
Other drugs that could prevent fibrosis were antihistamines. Histamine serves as a vital mediator in allergic diseases and IBD. It can be released by mast cells, which play a key role in regulating inflammatory responses. When histamine is released, it can lead to a range of symptoms, including itching, swelling, redness, and increased mucus production. These symptoms could occur in IBD, contributing to inflammation in the gastrointestinal tract. Fexofenadine and levocabastine, histamine H1 receptor antagonists, and could have been explored as potential treatments to mitigate the histamine-induced inflammatory response and alleviate symptoms associated with these conditions.53–55
Considering disulfiram, although there was some research suggesting that disulfiram might play a role in reducing oxidative stress and lipid peroxidation in colonic tissues, especially in the context of colitis in animal models, its potential use in CD has not been extensively explored or firmly established. Disulfiram appeared to influence the reduction of malondialdehyde levels in the colonic tissues of rats with colitis.56,57 This reduction might be linked to disulfiram’s function as an inhibitor of acetaldehyde dehydrogenase.58
The sensitivity analysis further confirmed and strengthened our findings regarding the association of clopidogrel, glucosamine, fluticasone, and glyceryl trinitrate with a reduced risk of the study outcome. Since the definition of the study outcome only included surgery, specifically associated with the development of intestinal fibrosis, these results should be prioritized when deciding on future directions. Of particular interest is fluticasone, as it was also confirmed in the time-dependent analysis.
Strengths and Limitations
The results of this study provided important insights into the relationship between drug exposure and the likelihood of the study outcome for surgery related to intestinal fibrosis in patients diagnosed with CD. This information shed light on which medications might have a meaningful impact on the need for surgery in these patients. One of the main strengths is that the study included a substantial cohort of 9179 CD patients, which enhances the reliability and generalizability of the findings. The Danish National Patient Registry is typically highly valid, with nearly complete registration of IBD diagnosis for both UC and CD.59,60 The study investigated the impact of a wide range of drugs on the risk of the study outcome, providing a comprehensive assessment of medication effects in CD management. Moreover, the identification of drugs that were associated with a reduced risk of surgery, potentially offering a protective effect against the study outcome in CD patients, information could have important clinical implications.
However, it’s essential to recognize and consider certain limitations of this study. In this study, we included 42 (4.1%) out of 1029 individuals who underwent proctocolectomy. Previous studies have suggested a connection between proctocolectomy and the further development of intestinal fibrosis, particularly in the context of certain diseases such as CD.61–63 However, at the time of the surgery, these individuals had not yet developed intestinal fibrosis.
Therefore, there is a potential risk of misclassification of the outcome. These limitations included the potential influence of confounding variables, which could have affected the accuracy of the findings. Additionally, it’s important to note that this study had a retrospective design and might not have accounted for all variables or changes over time. Furthermore, even though the implicated drugs encompassed a broad spectrum, including those approved for CD treatment and drugs used for managing CD-related complications, no data were available for drugs used in the hospital context, such as biologics and biosimilars, which are widely used in CD treatment. Another limitation is the lack of information concerning the disease location and extent of intestinal fibrosis. Since the National Patient Registry is not considered a valid tool for assessing the Montreal classification,64 it was not possible to include the effect of IBD phenotype on the risk of fibrosis. Finally, the study is also limited by the lack of information regarding smoking habits, diet, and family history of CRC. To reinforce the significance and practical application of these findings, further research is needed. This additional research has the potential to strengthen our understanding of the relationship between drug exposures and the surgical outcomes of CD patients with intestinal fibrosis. Ultimately, this ongoing investigation could play a crucial role in shaping and improving treatment strategies and clinical decision-making for individuals with CD.
While our study identifies potential repurposed drugs for CD, it’s essential to recognize the preliminary nature of our findings and limitations in immediate clinical applicability. The need for additional research and robust clinical trials is crucial to validate the effectiveness and safety of these drugs. Our study represents an initial step, and while promising, comprehensive clinical validation is necessary before these repurposed drugs can be confidently recommended for widespread use. Viewed as a stimulus for further investigation, our findings underscore the importance of ongoing research to elucidate the therapeutic potential and limitations of the identified drugs.
Finally, the study’s use of observational data from Danish registers introduces potential biases and limitations in the analysis and interpretation of results. Care should be taken to consider the inherent constraints associated with relying on secondary data sources for repurposing studies.
Conclusion
The findings from this study provided valuable insights into the role of drug exposures in the study outcome among patients with CD and surgery related to intestinal fibrosis. These insights gain significance in the context of personalized medicine for CD patients. Tailoring treatment plans based on individual factors such as age, gender, and medication history could play a pivotal role in optimizing CD management and potentially reducing the need for surgical interventions.
Furthermore, these findings underscored the ongoing importance of assessing the impact of medications on the progression and treatment of CD. Nevertheless, it is vital to emphasize the need for further research, as only through this iterative process of investigation and validation can we aspire to refine strategies for CD management and potentially reduce the reliance on surgical procedures, ultimately enhancing the quality of life for those facing this challenging condition.
Data Sharing Statement
Data are stored on secure servers on Statistics Denmark and cannot be shared according to Statistics Denmark regulations. Access to Statistics Denmark servers and the associated data can be granted by Statistics Denmark upon adequate permissions.
Acknowledgments
VB is enrolled in the PhD in Experimental and Clinical Pharmacological Sciences, Università degli Studi di Milano, which supports her fellowship.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The manuscript received funding from Novo Nordisk Foundation, grant NNF21OC0069019.
Disclosure
Dr Tine Jess reports personal fees from Ferring, outside the submitted work. Dr Julien Kirchgesner reports personal fees from Janssen, personal fees from Abbvie, personal fees from Pfizer, personal fees from Galapagos, personal fees from Takeda, personal fees from Tillots, personal fees from Amgen, personal fees from Lilly, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Pushpakom S, Iorio F, Eyers PA, et al. Drug repurposing: progress, challenges and recommendations. Nat Rev Drug Discov. 2019;18(1):41–58. doi:10.1038/nrd.2018.168
2. Scannell JW, Blanckley A, Boldon H, Warrington B. Diagnosing the decline in pharmaceutical R&D efficiency. Nat Rev Drug Discov. 2012;11(3):191–200. doi:10.1038/nrd3681
3. Zanello G, Chan CH, Pearce DA, Group IrdW. Recommendations from the IRDiRC Working Group on methodologies to assess the impact of diagnoses and therapies on rare disease patients. Orphanet J Rare Dis. 2022;17(1):181. doi:10.1186/s13023-022-02337-2
4. Lin SN, Mao R, Qian C, et al. Development of antifibrotic therapy for stricturing Crohn’s disease: lessons from randomized trials in other fibrotic diseases. Physiol Rev. 2022;102(2):605–652. doi:10.1152/physrev.00005.2021
5. Ismail MS, Charabaty A. Management of Crohn’s stricture: medical, endoscopic and surgical therapies. Frontline Gastroenterol. 2022;13(6):524–530. doi:10.1136/flgastro-2021-101827
6. Alastruey CL, Murcia XA, Comas ME. The role of stents in the treatment of Crohn’s disease strictures. Endosc Int Open. 2016;4(03):E301–E308. doi:10.1055/s-0042-101786
7. Sessa M, Mascolo A, Andersen MP, et al. Effect of chronic kidney diseases on mortality among digoxin users treated for non-valvular atrial fibrillation: a nationwide register-based retrospective cohort study. PLoS One. 2016;11(7):e0160337. doi:10.1371/journal.pone.0160337
8. Hagengaard L, Søgaard P, Espersen M, et al. Association between serum potassium levels and short-term mortality in patients with atrial fibrillation or flutter co-treated with diuretics and rate-or rhythm-controlling drugs. Eur Heart J. 2020;6(3):137–144. doi:10.1093/ehjcvp/pvz024
9. Sessa M, Khan AR, Liang D, Andersen M, Kulahci M. Artificial intelligence in pharmacoepidemiology: a systematic review. Part 1—overview of knowledge discovery techniques in artificial intelligence. Front Pharmacol. 2020;11:1028. doi:10.3389/fphar.2020.01028
10. Schmidt M, Pedersen L, Sørensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. doi:10.1007/s10654-014-9930-3
11. Lynge E, Sandegaard JL, Rebolj M. The Danish national patient register. Scand J Public Health. 2011;39(7_suppl):30–33. doi:10.1177/1403494811401482
12. Kildemoes HW, Sørensen HT, Hallas J. The Danish national prescription registry. Scand J Public Health Suppl. 2011;39(7_suppl):38–41. doi:10.1177/1403494810394717
13. Helweg-Larsen K. The Danish register of causes of death. Scand J Public Health. 2011;39(7_suppl):26–29. doi:10.1177/1403494811399958
14. Albaek Jacobsen H, Jess T, Larsen L. Validity of inflammatory bowel disease diagnoses in the Danish National Patient Registry: a population-based study from the North Denmark region. Clin Epidemiol. 2022;1099–1109. doi:10.2147/CLEP.S378003
15. Agrawal M, Ebert AC, Poulsen G, et al. Early ileocecal resection for Crohn’s disease is associated with improved long-term outcomes compared to anti-tumor necrosis factor therapy: a population-based cohort study. Gastroenterology. 2023;165(4):976–985.e3. doi:10.1053/j.gastro.2023.05.051
16. Kuhn M, Johnson K. Applied Predictive Modeling. Vol. 26. Springer; 2013.
17. Schneeweiss S, Rassen JA, Glynn RJ, Avorn J, Mogun H, Brookhart MA. High-dimensional propensity score adjustment in studies of treatment effects using health care claims data. Epidemiology. 2009;20(4):512. doi:10.1097/EDE.0b013e3181a663cc
18. Xue X, Xie X, Gunter M, et al. Testing the proportional hazards assumption in case-cohort analysis. BMC Med Res Methodol. 2013;13(1):1–10. doi:10.1186/1471-2288-13-88
19. Horwitz RI, Feinstein AR. The problem of “protopathic bias” in case-control studies. Am J Med. 1980;68(2):255–258. doi:10.1016/0002-9343(80)90363-0
20. Wang Y, Huang B, Jin T, Ocansey DKW, Jiang J, Mao F. Intestinal Fibrosis in Inflammatory Bowel Disease and the Prospects of Mesenchymal Stem Cell Therapy. Front Immunol. 2022;13:835005. doi:10.3389/FIMMU.2022.835005/BIBTEX
21. Iwata K, Mikami Y, Kato M, Yahagi N, Kanai T. Pathogenesis and management of gastrointestinal inflammation and fibrosis: from inflammatory bowel diseases to endoscopic surgery. Inflamm Regen. 2021;41(1):1–8. doi:10.1186/S41232-021-00174-7/FIGURES/2
22. Rieder F. Managing Intestinal Fibrosis in Patients With Inflammatory Bowel Disease. Gastroenterol Hepatol. 2018;14(2):120.
23. Sado A, Kalla R, Campbell S. Conventional and Future Therapies for Crohn’s Disease. OBM Hepatol Gastroenterol. 2019;3(3):1–19. doi:10.21926/obm.hg.1903032
24. Scribano ML, Prantera C. Use of antibiotics in the treatment of Crohn’s disease. World J Gastroenterol. 2013;19(5):648. doi:10.3748/wjg.v19.i5.648
25. Barkas F, Liberopoulos E, Kei A, Elisaf M. Electrolyte and acid-base disorders in inflammatory bowel disease. Ann Gastroenterol. 2013;26(1):23.
26. Rieder F, Fiocchi C, Rogler G. Mechanisms, management, and treatment of fibrosis in patients with inflammatory bowel diseases. Gastroenterology. 2017;152(2):340–350. doi:10.1053/j.gastro.2016.09.047
27. Klopcic B, Appelbee A, Raye W, et al. Indomethacin and retinoic acid modify mouse intestinal inflammation and fibrosis: a role for SPARC. Dig Dis Sci. 2008;53(6):1553–1563. doi:10.1007/s10620-007-0068-y
28. Kuźnicki P, Kempiński R, Neubauer K. The emerging role of mood disorders in inflammatory bowel diseases. Adv Clin Exp Med. 2020;29(12):1505–1510. doi:10.17219/acem/127676
29. Gao X, Tang Y, Lei N, et al. Symptoms of anxiety/depression is associated with more aggressive inflammatory bowel disease. Sci Rep. 2021;11(1):1440. doi:10.1038/s41598-021-81213-8
30. Mikocka-Walus A, Knowles SR, Keefer L, Graff L. Controversies revisited: a systematic review of the comorbidity of depression and anxiety with inflammatory bowel diseases. Inflamm Bowel Dis. 2016;22(3):752–762. doi:10.1097/MIB.0000000000000620
31. Kochar B, Barnes EL, Long MD, et al. Depression is associated with more aggressive inflammatory bowel disease. Am J Gastroenterol. 2018;113(1):80. doi:10.1038/ajg.2017.423
32. Uemura R, Fujiwara Y, Iwakura N, et al. Sleep disturbances in Japanese patients with inflammatory bowel disease and their impact on disease flare. Springerplus. 2016;5(1):1–8. doi:10.1186/s40064-016-3408-6
33. Ananthakrishnan AN, Long MD, Martin CF, Sandler RS, Kappelman MD. Sleep disturbance and risk of active disease in patients with Crohn’s disease and ulcerative colitis. Clin Gastroenterol Hepatol. 2013;11(8):965–971. doi:10.1016/j.cgh.2013.01.021
34. Sofia MA, Lipowska AM, Zmeter N, Perez E, Kavitt R, Rubin DT. Poor sleep quality in Crohn’s disease is associated with disease activity and risk for hospitalization or surgery. Inflamm Bowel Dis. 2020;26(8):1251–1259. doi:10.1093/ibd/izz258
35. Kristensen MS, Kjærulff TM, Ersbøll AK, Green A, Hallas J, Thygesen LC. The influence of antidepressants on the disease course among patients with Crohn’s disease and ulcerative colitis—a Danish nationwide register–based Cohort Study. Inflamm Bowel Dis. 2019;25(5):886–893. doi:10.1093/ibd/izy367
36. Salmenkari H, Korpela R, Vapaatalo H. Renin–angiotensin system in intestinal inflammation—Angiotensin inhibitors to treat inflammatory bowel diseases? Basic Clin Pharmacol Toxicol. 2021;129(3):161–172. doi:10.1111/bcpt.13624
37. Jacobs JD, Wagner T, Gulotta G, et al. Impact of angiotensin II signaling blockade on clinical outcomes in patients with inflammatory bowel disease. Dig Dis Sci. 2019;64(7):1938–1944. doi:10.1007/s10620-019-5474-4
38. Fairbrass KM, Hoshen D, Gracie DJ, Ford AC. Effect of ACE inhibitors and angiotensin II receptor blockers on disease outcomes in inflammatory bowel disease. Gut. 2021;70(1):218–219. doi:10.1136/gutjnl-2020-321186
39. Cohn HM, Dave M, Loftus JEV. Understanding the cautions and contraindications of immunomodulator and biologic therapies for use in inflammatory bowel disease. Inflamm Bowel Dis. 2017;23(8):1301–1315. doi:10.1097/MIB.0000000000001199
40. Lysaa RA, Giverhaug T, Libæk Wold H, Aarbakke J. Inhibition of human thiopurine methyltransferase by furosemide, bendroflumethiazide and trichlormethiazide. Eur J Clin Pharmacol. 1996;49(5):393–396. doi:10.1007/BF00203784
41. Xin HW, Fischer C, Schwab M, Klotz U. Thiopurine S-methyltransferase as a target for drug interactions. Eur J Clin Pharmacol. 2005;61(5–6):395–398. doi:10.1007/s00228-005-0950-5
42. Khalili H, Higuchi LM, Ananthakrishnan AN, et al. Oral contraceptives, reproductive factors and risk of inflammatory bowel disease. Gut. 2013;62(8):1153–1159. doi:10.1136/gutjnl-2012-302362
43. Pasvol TJ, Bloom S, Segal AW, Rait G, Horsfall L. Use of contraceptives and risk of inflammatory bowel disease: a nested case–control study. Aliment Pharmacol Ther. 2022;55(3):318–326. doi:10.1111/apt.16647
44. Khalili H, Granath F, Smedby KE, et al. Association between long-term oral contraceptive use and risk of Crohn’s disease complications in a nationwide study. Gastroenterology. 2016;150(7):1561–1567. doi:10.1053/j.gastro.2016.02.041
45. Wanchaitanawong W, Thinrungroj N, Chattipakorn SC, Chattipakorn N, Shinlapawittayatorn K. Repurposing metformin as a potential treatment for inflammatory bowel disease: evidence from cell to the clinic. Int Immunopharmacol. 2022;112:109230. doi:10.1016/j.intimp.2022.109230
46. Azuma K, Osaki T, Kurozumi S, et al. Anti-inflammatory effects of orally administered glucosamine oligomer in an experimental model of inflammatory bowel disease. Carbohydr Polym. 2015;115:448–456. doi:10.1016/j.carbpol.2014.09.012
47. Salvatore S, Heuschkel R, Tomlin S, et al. A pilot study of N‐acetyl glucosamine, a nutritional substrate for glycosaminoglycan synthesis, in paediatric chronic inflammatory bowel disease. Aliment Pharmacol Ther. 2000;14(12):1567–1579. doi:10.1046/j.1365-2036.2000.00883.x
48. Patel SH, Rachchh MA, Jadav PD. Evaluation of anti-inflammatory effect of anti-platelet agent-clopidogrel in experimentally induced inflammatory bowel disease. Indian J Pharmacol. 2012;44(6):744. doi:10.4103/0253-7613.103278
49. Ibrahim SH, Smyrk TC, Faubion WA. Treatment of isolated gastric Crohn’s disease with inhaled corticosteroids. Case Rep Gastroenterol. 2008;2(3):363–368. doi:10.1159/000158543
50. de Kaski MC, Peters AM, Lavender JP, Hodgson HJ. Fluticasone propionate in Crohn’s disease. Gut. 1991;32(6):657–661. doi:10.1136/gut.32.6.657
51. Prantera C, Marconi S. Glucocorticosteroids in the treatment of inflammatory bowel disease and approaches to minimizing systemic activity. Therap Adv Gastroenterol. 2013;6(2):137–156. doi:10.1177/1756283X12473675
52. Ghorbanzadeh B, Behmanesh MA, Mahmoudinejad R, Zamaniyan M, Ekhtiar S, Paridar Y. The effect of montelukast, a leukotriene receptor antagonist, on the acetic acid-induced model of colitis in rats: involvement of NO-cGMP-KATP channels pathway. Front Pharmacol. 2022;13:1011141. doi:10.3389/fphar.2022.1011141
53. Xie H, He SH. Roles of histamine and its receptors in allergic and inflammatory bowel diseases. World J Gastroenterol. 2005;11(19):2851. doi:10.3748/wjg.v11.i19.2851
54. Zhao X, Liu R, Chen Y, Hettinghouse A, Liu C. Cytosolic Phospholipase A2 Is Required for Fexofenadine’s Therapeutic Effects against Inflammatory Bowel Disease in Mice. Int J Mol Sci. 2021;22(20):11155. doi:10.3390/ijms222011155
55. Dvornikova KA, Platonova ON, Bystrova EY. Inflammatory Bowel Disease: crosstalk between Histamine, Immunity, and Disease. Int J Mol Sci. 2023;24(12):9937.
56. Chi F, Zhang G, Ren N, et al. The anti-alcoholism drug disulfiram effectively ameliorates ulcerative colitis through suppressing oxidative stresses-associated pyroptotic cell death and cellular inflammation in colonic cells. Int Immunopharmacol. 2022;111:109117. doi:10.1016/j.intimp.2022.109117
57. Zhou W, Zhang H, Huang L, et al. Disulfiram with Cu2+ alleviates dextran sulfate sodium-induced ulcerative colitis in mice. Theranostics. 2023;13(9):2879. doi:10.7150/thno.81571
58. Guo W, Chen S, Li C, Xu J, Wang L. Application of disulfiram and its metabolites in treatment of inflammatory disorders. Front Pharmacol. 2022;12:795078. doi:10.3389/fphar.2021.795078
59. Fonager K, Sørensen HT, Rasmussen SN, Møller-Petersen J, Vyberg M. Assessment of the diagnoses of Crohn’s disease and ulcerative colitis in a Danish hospital information system. Scand J Gastroenterol. 1996;31(2):154–159. doi:10.3109/00365529609031980
60. Schmidt M, Schmidt SAJ, Sandegaard JL, Ehrenstein V, Pedersen L, Sørensen HT. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;449–490. doi:10.2147/CLEP.S91125
61. Kissane J, Neutze JA, Singh H. Bowel Obstruction. In: Radiology Fundamentals. Springer International Publishing; 2020:187–193. doi:10.1007/978-3-030-22173-7_28
62. Mizushima T, Kameyama H, Watanabe K, et al. Risk factors of small bowel obstruction following total proctocolectomy and ileal pouch anal anastomosis with diverting loop‐ileostomy for ulcerative colitis. Ann Gastroenterol Surg. 2017;1(2):122–128. doi:10.1002/ags3.12017
63. Dolejs S, Kennedy G, Heise CP. Small Bowel Obstruction Following Restorative Proctocolectomy: affected by a Laparoscopic Approach? J Surg Res. 2011;170(2):202–208. doi:10.1016/j.jss.2011.03.004
64. Lo B, Vind I, Vester-Andersen MK, Burisch J. Validation of ulcerative colitis and Crohn’s disease and their phenotypes in the Danish National Patient Registry using a population-based cohort. Scand J Gastroenterol. 2020;55(10):1171–1175. doi:10.1080/00365521.2020.1807598
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.