")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
Does the Healthy China 2030 Policy Improve People’s Health? Empirical Evidence Based on the Difference-in-Differences Approach
Authors Ning C , Pei H , Huang Y , Li S , Shao Y
Received 10 September 2023
Accepted for publication 20 December 2023
Published 6 January 2024 Volume 2024:17 Pages 65—77
DOI https://doi.org/10.2147/RMHP.S439581
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Chuanlin Ning,1 Huacheng Pei,2 Youjia Huang,1 Sichen Li,1 Yiling Shao1
1School of Media and Communication, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 2School of Finance, Shanghai University of Finance and Economics, Shanghai, People’s Republic of China
Correspondence: Yiling Shao, School of Media and Communication, Shanghai Jiao Tong University, No. 800, Dongchuan Road, Minhang District, Shanghai, 200240, People’s Republic of China, Email [email protected]
Background: The Healthy China 2030 (HC2030) policy is currently recognized as China’s most significant and influential national health policy. However, despite its implementation in 2016, the policy’s impact has yet to be comprehensively evaluated, particularly in relation to its effectiveness in enhancing population health and promoting public health equity.
Methods: We utilized the Difference-in-Differences (DiD) method to evaluate the impact of the HC2030. Our analysis utilized a panel dataset derived from five longitudinal surveys conducted by the China Family Panel Studies (CFPS).
Results: The implementation of HC2030 has improved the overall health status of residents, particularly in urban areas and the western and eastern regions. Mechanistic analysis has further unveiled that the policy’s beneficial impact on health outcomes is attributed to a rise in physical activity frequency and the betterment of mental health. Additionally, female, married, and medically insured individuals have demonstrated a significant positive impact of the policy on their health outcomes.
Conclusion: Although the HC2030 appears to have effectively improved overall population health, it needs to promote equity in public health adequately. The study suggests adjustments are needed to address the unequal distribution of health outcomes between urban and rural areas and among different regions.
Keywords: health China 2030, health policy, policy evaluation, health equity, health communication, public health
Introduction
Since the founding of the People’s Republic of China, the country has achieved remarkable progress in economic development. However, industrialization, urbanization, population aging, changes in disease spectrums, ecological environment, and lifestyle have brought a series of new challenges to maintaining and promoting health.1 In this context, the Chinese government is attempting to address the increasingly severe public health problems by issuing a set of public health policies, including the most important one, Healthy China 2030 (HC2030).2 HC2030, announced on October 25, 2016, by the Communist Party of China Central Committee and the State Council, is the first medium-to-long-term strategic policy for health at the national level in China and a localization of the Sustainable Development Goals of the United Nation.3 In addition to developing the domestic healthcare system and medical services, the policy shifts the focus from passive “medical treatment” to proactive “disease prevention”. Three years later, the vision was put into action with the launch of the Healthy China Initiative 2019–2030. The initiative includes 15 major actions (Figure 1), guiding the populace to enhance health literacy in their daily lives, emphasizing the cultivation of healthy lifestyle habits, and refining associated infrastructure. It is the most significant leadership policy in public health governance in China which aims to comprehensively solve major health issues over the national strategic timeframe.4 In particular, against the backdrop of the disparities in basic health services and health levels among urban and rural areas, regions, and population groups,5,6 the plan aims to achieve universal health coverage and promote social equity.1 However, the current impact and effectiveness of this policy on public health have yet to be fully understood. Sanderson argued that evidence-based policy evaluation has two aims: the first is to evaluate accountability of the government, and the second is to suggest improvement.7 As HC2030 has been operated for seven years, analyzing its efficacy at the current stage would provide valuable insights into both past and future outcomes. Particularly, China has challenging financial burden for medical services, which requires to setting a realistic goal based on evidences.8
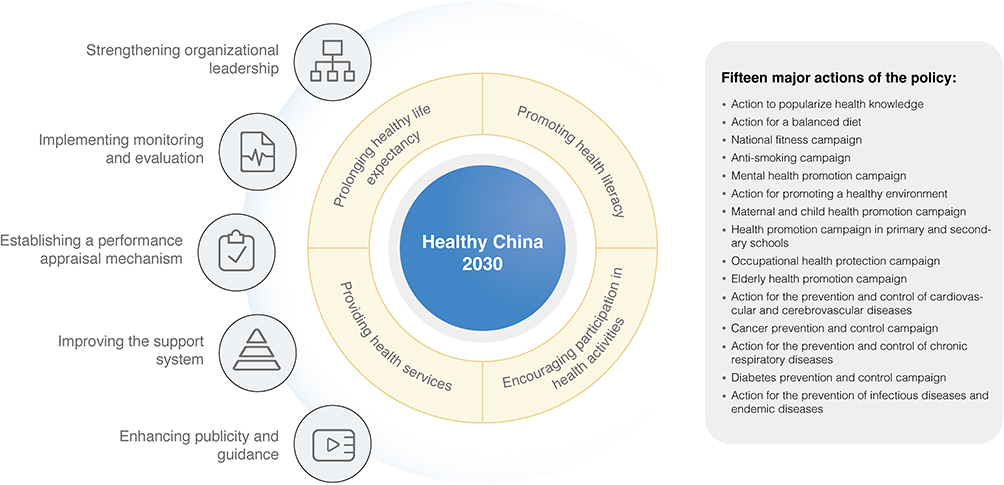 |
Figure 1 The Healthy China Initiative 2019–2030. |
Scholars have examined the HC2030 policy from various aspects. By analyzing the current gaps in the health care system reform, Li and Fu praised that the HC2030 is heading a right direction by focusing not only disease care but the general health care.9 However, Dong et al analyzed the health conditions of Chinese adolescents and found discrepancies between the set goal and the status quo in terms of poor vision, obesity and daily physical activity.10 Similarly, Wang et al predicted that obesity is becoming an alarming issue in China and post challenges to the policy.11 From the perceptual perspective, Wu et al found that most respondents in their survey reported poor awareness regarding the policy.12 Zhang et al also reported biased understandings among the public towards the initiative practice for health concept proposed by HC2030.13 Still, most studies above did not analyze the effect of the policy, rather they focus on the disparities between the current trend of public health and the HC2030 goal. In this regard, our study aims to analyze the effect of policy implementation on residents’ perceived health status through a natural experiment.
Specifically, we propose that physical activity and mental health condition may serve as the underlying mechanisms for this effect. The existing literature has well-established the impact of physical activity14 and mental health levels15 on overall health conditions. Given that both physical and mental health are two integral aspects of HC2030 directly related to residents’ overall health status,16 the study aims to investigate which aspect the policy has more effectively addressed.
We are particularly interested in testing whether the HC2030 implementation has mitigated regional and demographical inequality issues. Existing literature has documented the inequalities between geographic areas and demographic groups in China. Rural and urban divides, as well as east, central, and west regional divides, are two critical divides to unpack China’s geographic-based inequalities.17 While evidence suggests a narrowing gap in basic health services18 and maternal and child health outcomes19 between urban and rural areas, extensive literature has outlined persisting disparities in the effectiveness of health insurance,20 underlying diseases among the elderly,21 healthy aging,22 and health human resources.23
Regional inequalities are also prominent. Owing to gaps in GDP and health care resources/services, provinces in western and middle China scored lower than those in the eastern China particularly in terms of maternal and child health and infectious diseases.6 The premature mortality rate of the four main non-communicable diseases is much more severe in less developed regions of China than in developed cities like Shanghai and Beijing.24
Demographic factors, such as health insurance coverage, gender, and marital status, contribute to health outcome disparities as well. These dimensions were chosen for their intrinsic differences and relevance to health outcomes: medical insurance as a choice reflecting health-related behavior, gender as an innate characteristic, and marital status as a significant aspect of adult identity.
While China has achieved near-universal health insurance coverage, over 4% of the population remains uncovered.25 A noticeable trend involves individuals discontinuing insurance in recent years due to increasing insurance fees.26 Health insurance in China does produce positive outcomes, including preventive care usage, outpatient services, or hospitalization, although the benefits are somewhat limited in certain aspects.27,28 Given that the HC2030 focuses on disease prevention other than medical treatment, it would be meaningful to study whether individuals without health insurance exhibit more health activities and have health conditions comparable to those with coverage.
Gender represents another prominent and complex factor. On one hand, males have higher excess death rate than females, attributed to factors such as susceptibility to diseases like TB and HIV/AIDS, drinking- and smoking-related illnesses, and suicide.20 On the other hand, the experience of and access to healthcare is generally biased against women.29 Girls face discrimination in accessing healthcare; only upon entering child-bearing age do they receive preferable treatment compared to men.30 Research by Song and Bian revealed that male patients incur higher expenditures and longer hospitalization durations than females.31 Exploring whether the HC2030 policy could alleviate the gender health gap is a subject of interest.
There is relatively little evidence from China regarding the impact of marriage on health outcomes. In study involving older adults, marriage has been associated with generally more positive outcomes concerning both physical and mental health.32 However, within the broader population, self-rated health conditions vary significantly by marital status only among rural populations rather than urban populations.33 Despite the diverse mechanisms behind marriage effects, mental health and daily physical activities are one of the key factors. It is reasonable to propose that by promoting mental and physical health awareness among residents, HC2030 could potentially narrow the gap between the health outcomes of single and married populations.
Finally, considering the more pronounced demographical health inequalities in less developed regions, the study aims to compare the effect of HC2030 on these disparities across geographical areas. In addition to the previously discussed variations in marriage effects between urban and rural populations, evidence indicates that gender health inequalities against women are more severe in less developed and/or rural areas.34 Furthermore, disparities exist in health insurance policies across provinces and rural-urban areas. The integration of the Urban and Rural Medical Insurance System was not implemented uniformly nationwide but was initially tested in provinces like Shanghai, Zhejiang, Tianjin, etc., before extending to other regions.35 This sequential approach may contribute to disparities across geographical areas. While evidence suggests that the integration efforts have reduced the health insurance gap and addressed unmet healthcare needs in rural areas,36 it remains unclear whether health outcomes have improved among under-covered rural residents.
Overall, there are both encouraging and discouraging portrayal in the literature regarding the attainment of health equity goals set by HC2030. However, few studies have specifically examined the impact of HC2030 implementation on individuals from diverse geographic areas and demographics. The current study aims to fill this gap.
Materials and Methods
The dataset used in this study was sourced from the China Family Panel Studies (CFPS, official website: https://www.isss.pku.edu.cn/cfps/). CFPS is a large-scale biennial social survey implemented by the Institute of Social Science Survey (ISSS) of Peking University, aiming to reflect China’s social, economic, demographic, educational, and health changes by tracking and collecting data at three levels: individual, household, and community, and to provide a database for academic research and public policy analysis. In China, several micro-survey databases exist, yet the CFPS stands out for its continuity — the capacity to track changes in the same participants over nearly a decade. This feature forms the foundation for constructing individual-year panel data. We accessed raw data from the CFPS’s official website, encompassing five surveys spanning from 2012 to 2020, and engaged in a series of processing steps. Firstly, we filtered out the minor-age group, focusing exclusively on adult respondents. To effectively analyze changes in individual health pre-policy and post-policy implementation, we omitted records that included only pre-policy or post-policy data. Lastly, we excluded cases with missing key variables for data accuracy and validity. After implementing these criteria, we compiled a robust dataset of 117,751 valid samples for our analysis.
The Difference in Differences (DiD) method is widely adopted in empirical research to evaluate the impacts of policies.37 Its approach is notably more intuitive than other methodologies, beginning with the observation of pre- and post-policy changes in those affected by the policy, and similarly in those unaffected. This method’s essence lies in comparing the difference between these two sets of changes to gauge the policy’s effect. Typically, the standard DiD method includes four key elements: the event causing the change (shock event), the group experiencing the policy (treatment group), the group not influenced by the policy (control group), and the relevant time frame. These elements are encapsulated as two dimensions in the regression model, with one dimension being a dummy variable signifying policy impact on individuals, and the other indicating the time relative to policy implementation.
However, the challenge arises when dealing with a national-level health policy that affects everyone, eliminating the distinction between treatment and control groups. Addressing this, our study adheres to the core principles of DiD, discerning differences in our observed sample along two dimensions. The first dimension controls for unobservable time trends, while the second captures the varying impacts of the policy along urban-rural lines. Specifically, we compare the health changes of urban residents before and after policy implementation against those in rural residents during the same timeframe. Urban samples are coded as 1 (Treat=1), and rural samples as 0 (Treat=0). We use “Post” as a proxy variable for policy implementation, with pre-policy data from 2012, 2014, and 2016 coded as Post=0, and post-policy data from 2018 and 2020 as Post=1. Our analysis hinges on the interaction term Treat*Post as the independent variable, with the dependent variable being the respondents’ perceived health level (Health). Health status was gauged through the question, “How do you perceive your overall health?”, rated on a five-point scale from “very unhealthy” to “very healthy”, where higher scores denote better health. Regarding the definition of our variables and the descriptive statistics of the variables, please refer to Table 1 and Table 2. Additionally, we included controls for individual characteristics (Controls) in our model (1), and  ,
,  ,
,  ,
,  denote individual fixed effects, year fixed effects, provincial fixed effects, and error term, respectively.
denote individual fixed effects, year fixed effects, provincial fixed effects, and error term, respectively.

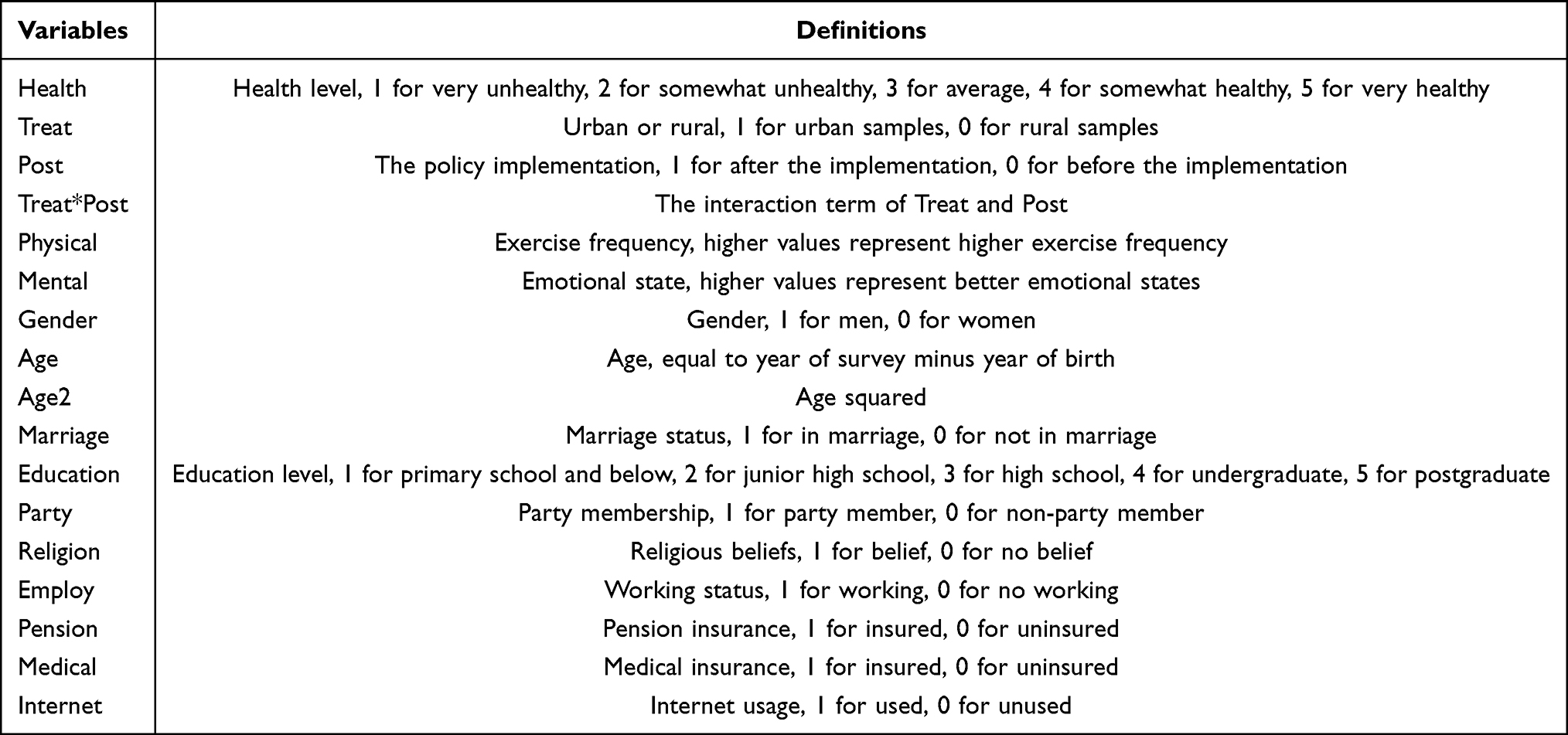 |
Table 1 Variable Definition |
 |
Table 2 Descriptive Statistics |
In our research, we delved into the mechanisms through which the policy implementation influences people’s health, focusing on both physical and mental aspects. To gauge the physical impact (Physical), we used a question about exercise frequency. Higher values in this metric signify increased frequency of exercise, reflecting better physical health. For the mental aspect (Mental), we relied on a question about emotional states, with higher values indicating more positive emotional states.
Our method for testing mediating effects is a two-step approach. Initially, we employed model (2) to explore the influence of the policy on physical or mental states. In this model, the dependent variable, Mechanism, alternates between representing Physical or Mental states, depending on the focus of the analysis. The independent variable in this model is Treat*Post, capturing the interaction between the group and the post-policy period.
Subsequently, we integrated the findings from model (2) into model (3), which expands on model (1) by including the control variable Mechanism. This step is crucial as it allows us to assess the indirect effects of the policy through changes in physical and mental health. By adding the Mechanism variable, we aim to understand how physical and mental health mediate the relationship between policy implementation and overall health outcomes. In model (3), the dependent variable remains the perceived health level (Health), all other control variables and fixed effects are consistent with those used in model (1).


In our final phase of analysis, we sought to uncover the diverse effects of policy implementation on health across different segments of the population: gender, marital status, and medical insurance coverage. We introduced interaction terms in model (4), effectively combining each of these three variables (“Var” denotes Gender, Marriage, and Medical, respectively) with the Treat*Post variable. The rest of the model (4) maintains consistency with model (1) in terms of other control variables and fixed effects. This method enables us to individually and comparatively assess how the policy’s impact is modulated by these factors.

Results
According to the DiD models, there has been a noteworthy enhancement in the health status of the Chinese population subsequent to the implementation of the HC2030 policy. However, there exist noticeable discrepancies in the effect of policy implementation on the health status of urban and rural residents, as evidenced by the findings presented in Table 3. With the inclusion of additional control variables, the regression coefficients of Treat*Post display a statistically significant positive effect (0.0333–0.0794) at the 1% level, indicating that the health level of urban residents surpasses that of their rural counterparts after the implementation of the policy.
 |
Table 3 Basic Results |
Subsequently, we analyzed the disparities in the impact of policy implementation on health levels among the three primary economic regions of China. Specifically, we divided all the samples in this paper into three sub-samples based on economic regions: east, center and west, and then tested them separately using model (1), and the results are shown in Table 4. Figure S1 in the Supplementary Data provides the division of the economic regions. The regression coefficients of Treat*Post reveal a considerably positive effect (0.0568) at the 1% level in the western zone (Column 3), a significantly positive effect (0.0391) at the 5% level in the eastern zone (Column 1), and an insignificant effect in the central zone (Column 2). This implies that the highest increase in health levels after policy implementation is most noticeable in the western zone, followed by the eastern zone, with no discernible change observed in the central zone.
 |
Table 4 Heterogeneity Analysis on Three Economic Regions |
We analyzed the pathways through which policy implementation affects health outcomes, as presented in Table 5. Column 1 shows that the variable Treat*Post is significantly and positively associated with Physical at the 1% level, column 2 shows that the coefficients for Treat*Post and Physical are both significantly positive, indicating that the implementation of HC2030 has increased the frequency of physical exercise among residents and consequently improved their health. Additionally, column 3 shows that the variable Treat*Post is significantly and positively associated with Mental at the 1% level, column 4 shows that the coefficients for Treat*Post and Mental are both significantly positive, indicating that the implementation of HC2030 has improved the mental well-being of residents and thus contributed to people’s health improvement. In summary, Physical and Mental have a mediating role, HC2030 has enhanced the health of individuals through the improvement of both their physical and mental states.
 |
Table 5 Mediating Effects of Physical and Mental |
We conducted an analysis of the effect of policy implementation on health levels based on individual characteristics, and the results are presented in Table 6. Column 1 shows that the regression coefficient for Treat*Post*Gender is significantly negative (−0.0298) at the 5% level, indicating that the positive effect of policy implementation on the health level of residents is more pronounced among women compared to men. Column 2 shows that the regression coefficient for Treat*Post*Marriage is significantly positive (0.0529) at the 1% level, suggesting that the positive effect of policy implementation on the health level of residents is more evident among married individuals compared to those who are not married. Lastly, column 3 shows that the regression coefficient for Treat*Post*Medical is positive (0.0451) at the 1% level, demonstrating that the positive effect of policy implementation on the health level of residents is more substantial among people with medical insurance compared to those without medical insurance. In summary, Gender, Marriage and Medical have a moderating role. The results indicate that the characteristics of being married and having medical insurance can enhance the positive impact of the HC2030 policy on people’s health while being male can weaken this positive impact.
 |
Table 6 Moderating Effects of Individual Characteristics |
Discussion
The primary objective of this study was to assess the impact of the HC2030 policy in China. Previous research on HC2030 has focused on three areas: a) providing a macro-level analysis of its social significance, b) investigating its effects on specific populations, such as adolescents, and c) analyzing the disparities between the policy’s objectives and current trends. Synthesizing the empirical findings, this research indicates that the implementation of HC2030 has resulted in improved physical and mental health among residents. However, variations were observed in the effects of policy implementation across different geographical areas, regions, and individual characteristics. Overall, these findings contribute to the existing body of research by offering a targeted examination of the specific impacts of HC2030 on residents’ health.
The major finding of the study is that public health progresses with the HC2030 while challenges remain. The finding of a positive effect for HC2030 is broadly consistent with previous studies that it empowers population health and wellbeing.38 Mobilizing Substantial political and financial resources is the main contributor to the improvement in the quality of health.39 Indeed, the Chinese government has increased its support for health during these years.40 This conclusion follows from several evidences. First, at the national level, the State Council, the National Development and Reform Commission, the National Health Commission, and many other departments have issued policies to support and regulate the development of the health industry, involving the reform of the medical and health care system, the development of the health service industry, and the regulation of the safety of food and health products. Second, provinces and municipalities have also issued plans for the construction of local medical and healthcare systems in the context of the Fourteenth Five-Year Plan and the Outline of the HC2030. To name only a few, Beijing, Shanghai, and Guangdong have all put forward master plans from the perspectives of people’s health level, healthy living, health services and protection, and a healthy environment. Third, the government actively promotes multi-industry interactions centered on the health industry, including the integration and development of health with pension, tourism, the Internet, fitness and leisure, and food. One example is the Development Planning for a New Generation of Artificial Intelligence in 2017 proposes to promote the application of AI treatment and the construction of intelligent healthcare. Our research provides evidence supporting the positive effects of these measures, which collectively demonstrate the Chinese government’s commitment to enhancing the nation’s health and well-being.
Identifying the unequal distribution of health outcomes across geographical areas has significant practical implications. Several potential explanations have been considered. Firstly, the equity-efficiency trade-off is a crucial aspect of policy implementation.41 The HC2030 prioritizes attention to western and impoverished areas, focusing on regions that are most likely to benefit from interventions. This may partially account for the superior performance of the West compared to the Center, as the western zone faces more challenging circumstances. Consequently, the policies are more likely to yield positive results in these areas. Furthermore, the HC2030 emphasizes that achieving a healthy China is a collective responsibility and endeavors to enhance individual health knowledge through various means. However, Chinese urban residents tend to have higher levels of education than their rural counterparts, which leads to better health knowledge and behaviors among urban residents. While “fairness and equity” is a fundamental principle of HC2030, there remains a pressing need to fully promote equity in public health.
Lastly, this study expands on previous research by examining additional socio-demographic variables such as gender, marital status, and medical insurance status. Previous studies have shown that females face disadvantages in accessing healthcare, although they interact with the healthcare system more frequently than males, possibly due to women assuming a greater responsibility for their own health and the well-being of their families.42 Our research findings indicate that the HC2030 policy has a stronger effect on improving health outcomes for women, suggesting a narrowing of the gender gap. Scholars have also demonstrated that married individuals tend to enjoy better health and longer life expectancy compared to those who have never been married, divorced, or widowed.43 In our study, we found that the positive impact of policy implementation on residents’ health levels is more pronounced among married individuals than among unmarried individuals. Similarly, individuals with medical insurance are likely to prioritize their health more than those without coverage. This observation highlights the necessity of strengthening medical insurance in disadvantaged regions or populations within China, and supports the continued promotion and universal coverage of the national health insurance policy.
Pursuing health equity means working to eliminate health disparities.44 In total, the HC2030 has not fully succeeded in promoting health equity. In the long term, this could result in new imbalances in population health, which goes against the original intentions of the policy. Health equity cannot focus only on isolated health issues. Rather, it must address the larger issue of equity and fairness in social arrangements, including economic distribution, by focusing on the role of health in human life and freedom.45 Thus, governments, industries, and individuals should make efforts to promote health equity. Firstly, governments prioritize promoting China’s economic development as a primary objective. In terms of policy implementation, it is crucial to make further adjustments to address existing inconsistencies. This includes refining the scope and strength of implementation,46 as well as accurately measuring health indicators.2 Additionally, comprehensive interventions such as health literacy promotion, encouraging balanced diets, and promoting physical fitness for all are essential. These interventions aim to guide individuals in developing healthy behaviors and lifestyles. Furthermore, it is important to ensure equitable access to systematic and continuous healthcare services throughout the entire life cycle. Addressing key health issues and the factors that influence them at different stages of life, including infancy, adolescence, adulthood, and old age, is integral to this approach. Secondly, industries must engage in cross-sectoral collaboration. Sectors such as education, environment, food, medicine, and sports need to work together. For instance, addressing the challenge of providing nutritious meals to children in western regions requires the combined efforts of multiple sectors, including schools, food suppliers, the healthcare sector, and food safety regulatory bodies. Thirdly, individuals play a crucial role in improving health literacy and adopting healthy lifestyles. It is essential for residents to acquire health information through educational institutions, literature, and media sources, covering topics such as disease prevention, treatment, and food safety. Only by fostering a climate of community-wide collaboration can effective promotion of health equity be achieved.
Limitations of This Study
This study has several limitations that should be acknowledged. Firstly, the dataset utilized in this study relied on subjective reports from individuals rather than objective health indicators such as data obtained from physical examinations. Consequently, there may be some discrepancies between the reported health status and the actual health conditions of the participants. Secondly, public health is a multifaceted issue influenced by numerous factors, including environmental pollution, which were not taken into account in the present research. Therefore, the findings may not fully capture the broader context of public health determinants. Thirdly, future studies would benefit from incorporating additional empirical evidence and providing more detailed explanations regarding health inequities. These additions would enhance the comprehensiveness and depth of understanding in evaluating the effects of the HC2030 policy on residents’ health.
Conclusion
Despite the aforementioned limitations, this study presents valuable insights into the evaluation of China’s HC2030 policy in terms of population health using the Difference-in-Differences (DiD) method. The findings indicate that the implementation of HC2030 appears to have led to improved health outcomes among residents. Furthermore, the policy has demonstrated a significant impact on urban areas as well as the western and eastern regions of China. Mechanism analysis revealed that HC2030 has enhanced public health by promoting increased physical exercise and improving the psychological well-being of residents. Additionally, individual characteristics have been identified as moderating factors, with females, married individuals, and those with health insurance experiencing more pronounced positive health effects from the policy. These findings highlight the importance of promoting equity in the implementation of HC2030, while acknowledging the need for further research to assess its long-term effects.
Ethical Statement
Ethical approval was issued by the Peking University Biomedical Ethics Review Committee (IRB00001052-14010), and all respondents signed an informed consent form before the study was initiated. The study was conducted in accordance with the regulations and ethics followed in compliance with the Declaration of Helsinki.
Acknowledgement
We would like to express our gratitude to the anonymous reviewers for their valuable feedback on the paper, which greatly contributed to its improvement in quality. We would also like to extend our appreciation to the editor for their guidance and support throughout the publication process. Their expertise and input were instrumental in shaping the final version of the paper.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revised or critically reviewed the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No external financial support was received for this study.
Disclosure
The authors declare no potential financial and non-financial competing interests in this work.
References
1. Xinhua News Agency. The central committee of the communist party of china and the state council issued the ‘Healthy China 2030’ Planning Outline; 2016. Available from: http://www.gov.cn/zhengce/2016-10/25/content_5124174.htm.
2. Tan X, Zhang Y, Shao H. Healthy China 2030, a breakthrough for improving health. Glob Health Promot. 2019;26(4):96–99. doi:10.1177/1757975917743533
3. Dai J, Menhas R. Sustainable development goals, sports and physical activity: the localization of health-related sustainable development goals through sports in China: a narrative review. Risk Manag Healthca Policy. 2020;13:1419–1430. doi:10.2147/RMHP.S257844
4. Chen P, Li F, Harmer P. Healthy China 2030: moving from blueprint to action with a new focus on public health. Lancet Public Health. 2019;4(9):e447. doi:10.1016/S2468-2667(19)30160-4
5. Sun J, Lyu S, Zhao R. Socioeconomic inequality in health outcomes among the elderly: evidence from a cross-sectional study in China. Risk Manag Healthca Policy. 2020;13:397–407. doi:10.2147/RMHP.S248019
6. Fang P, Dong S, Xiao J, Liu C, Feng X, Wang Y. Regional inequality in health and its determinants: evidence from China. Health Policy. 2010;94(1):14–25. doi:10.1016/j.healthpol.2009.08.002
7. Sanderson I. Evaluation, policy learning and evidence‐based policy making. Public Adm. 2002;80(1):1–22. doi:10.1111/1467-9299.00292
8. Fu W, Zhao S, Zhang Y, Chai P, Goss J. Research in health policy making in China: out-of-pocket payments in Healthy China 2030. BMJ. 2018;360:k234. doi:10.1136/bmj.k234
9. Li L, Fu H. China’s health care system reform: progress and prospects. Int J Health Plann Manage. 2017;32(3):240–253. doi:10.1002/hpm.2424
10. Dong B, Zou Z, Song Y, et al. Adolescent health and healthy China 2030: a review. J Adolesc Health. 2020;67(5):S24–S31. doi:10.1016/j.jadohealth.2020.07.023
11. Wang Y, Zhao L, Gao L, Pan A, Xue H. Health policy and public health implications of obesity in China. Lancet Diabetes Endocrinol. 2021;9(7):446–461. doi:10.1016/S2213-8587(21)00118-2
12. Wu Q, Chen B, Zhu J. Insights from COVID-19: reflecting on the promotion of long-term health policies in China. Int J Environ Res Public Health. 2023;20(4):2889. doi:10.3390/ijerph20042889
13. Zhang Y, Zhou M, Jiang M, Zhang X, Wang X, Wang B. Awareness of initiative practice for health in the Chinese population: a questionnaire survey based on a network platform. World J Clin Cases. 2022;10(16):5241. doi:10.12998/wjcc.v10.i16.5241
14. Warburton DE, Nicol CW, Bredin SS. Health benefits of physical activity: the evidence. CMAJ. 2006;174(6):801–809. doi:10.1503/cmaj.051351
15. Salovey P, Rothman AJ, Detweiler JB, Steward WT. Emotional states and physical health. Am Psychol. 2000;55(1):110. doi:10.1037/0003-066X.55.1.110
16. Penedo FJ, Dahn JR. Exercise and well-being: a review of mental and physical health benefits associated with physical activity. Curr Opin Psychiatry. 2005;18(2):189–193. doi:10.1097/00001504-200503000-00013
17. Wan G. Understanding regional poverty and inequality trends in China: methodological issues and empirical findings. Rev Income Wealth. 2007;53(1):25–34. doi:10.1111/j.1475-4991.2007.00216.x
18. Cao F, Xi Y, Zheng C, Bai T, Sun Q. How efficient are basic public health services between Urban and Rural in Shandong Province, China? A data envelopment analysis and panel tobit regression approach. Risk Manag Healthca Policy. 2022;15:727–738. doi:10.2147/RMHP.S354758
19. Li Y, Zhang Y, Fang S, et al. Analysis of inequality in maternal and child health outcomes and mortality from 2000 to 2013 in China. Int J Equity Health. 2017;16(1):1–11.
20. Chen S, Guo L, Wang Z, et al. Current situation and progress toward the 2030 health-related sustainable development goals in China: a systematic analysis. PLoS Med. 2019;2019:1.
21. Qin VM, McPake B, Raban MZ, et al. Rural and urban differences in health system performance among older Chinese adults: cross-sectional analysis of a national sample. BMC Health Serv Res. 2020;20:1–14. doi:10.1186/s12913-020-05194-6
22. Li H, Zeng Y, Gan L, et al. Urban-rural disparities in the healthy ageing trajectory in China: a population-based study. BMC Public Health. 2022;22(1):1–13. doi:10.1186/s12889-022-13757-x
23. Wu J, Yang Y. Inequality trends in the demographic and geographic distribution of health care professionals in China: data from 2002 to 2016. Int J Health Plann Manage. 2019;34(1):e487–e508. doi:10.1002/hpm.2664
24. Zeng X, Li Y, Liu S, et al. Subnational analysis of probability of premature mortality caused by four main non-communicable diseases in China during 1990–2015 and “Health China 2030” reduction target. Zhonghua Yu Fang Yi Xue Za Zhi. 2017;51(3):209–214. doi:10.3760/cma.j.issn.0253-9624.2017.03.004
25. National Healthcare Security Administration. 2022 national statistical report on the development of healthcare security undertakings; 2023. Available from: http://www.nhsa.gov.cn/art/2023/7/10/art_7_10995.html.
26. Sohu. Behind the withdrawal of 25 million people from medical insurance: premiums increased 37 times in 20 years - medical insurance bureau reveals reasons and trends; 2023. Available from: https://www.sohu.com/a/731385257_121333743.
27. Li X, Zhang W. The impacts of health insurance on health care utilization among the older people in China. Soc Sci Med. 2013;85:59–65. doi:10.1016/j.socscimed.2013.02.037
28. He H, Nolen PJ. The effect of health insurance reform: evidence from China. Chin Econ Rev. 2019;53:168–179.
29. World Health Organization. Gender and health. Available from: https://www.who.int/health-topics/gender#tab=tab_1.
30. Gao M, Yao Y. Gender gaps in access to health care in rural China. Econ Dev Cult Change. 2006;55(1):87–107. doi:10.1086/505720
31. Song Y, Bian Y. Gender differences in the use of health care in China: cross-sectional analysis. Int J Equity Health. 2014;13:1–6.
32. Williams L, Zhang R, Packard KC. Factors affecting the physical and mental health of older adults in China: the importance of marital status, child proximity, and gender. SSM Popul Health. 2017;3:20–36. doi:10.1016/j.ssmph.2016.11.005
33. Hu LC. Marital status and self-rated health in China: a longitudinal analysis. Popul Res Policy Rev. 2021;40(3):499–531. doi:10.1007/s11113-020-09593-9
34. Chen L, Standing H. Gender equity in transitional China’s healthcare policy reforms. Fem Econ. 2007;13(3–4):189–212. doi:10.1080/13545700701439473
35. The Paper. More than 10 provinces have explicitly merged urban and rural medical insurance, with variations in payment and reimbursement policies; 2016. Available from: https://www.thepaper.cn/newsDetail_forward_1485524.
36. Zhou S, Huang T, Li A, Wang Z. Does universal health insurance coverage reduce unmet healthcare needs in China? Evidence from the national health service survey. Int J Equity Health. 2021;20(1):1–17. doi:10.1186/s12939-021-01385-7
37. Wing C, Simon K, Bello-Gomez RA. Designing difference in difference studies: best practices for public health policy research. Annu Rev Public Health. 2018;39:453–469. doi:10.1146/annurev-publhealth-040617-013507
38. Bao Y, Meng S, Sun Y, Jie S, Lu L. Healthy China Action plan empowers child and adolescent health and wellbeing. Lancet Public Health. 2019;4(9):E448. doi:10.1016/S2468-2667(19)30164-1
39. Meng Q, Mills A, Wang L, Han Q. What can we learn from China’s health system reform? BMJ. 2019;365:1.
40. Yip W, Fu H, Chen A, et al. 10 years of health-care reform in China: progress and gaps in universal health coverage. Lancet. 2019;394(10204):1192–1204. doi:10.1016/S0140-6736(19)32136-1
41. Paolucci F, Mentzakis E, Defechereux T, Niessen LW. Equity and efficiency preferences of health policy makers in China—a stated preference analysis. Health Policy Plan. 2015;30(8):1059–1066. doi:10.1093/heapol/czu123
42. Wallen J, Waitzkin H, Stoeckle J. Physician stereotypes about female health and illness: a study of patient’s sex and the informative process during medical interviews. Women Health. 1979;4(2):135–146. doi:10.1300/J013v04n02_03
43. Lawrence EM, Rogers RG, Zajacova A, Wadsworth T. Marital happiness, marital status, health, and longevity. J Happiness Stud. 2019;20(5):1539–1561. doi:10.1007/s10902-018-0009-9
44. Braveman P. Health disparities and health equity: concepts and measurement. Annu Rev Public Health. 2006;27:167–194. doi:10.1146/annurev.publhealth.27.021405.102103
45. Tang S, Meng Q, Chen L, Bekedam H, Evans T, Whitehead M et al. Tackling the challenges to health equity in China. Lancet. 2008;372(9648):1493–1501. doi:10.1016/S0140-6736(08)61364-1
46. Mohan G, Longo A, Kee F. Evaluation of the health impact of an urban regeneration policy: neighbourhood Renewal in Northern Ireland. J Epidemiol Community Health. 2017;71(9):919–927. doi:10.1136/jech-2017-209087
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.