")
Back to Journals » Orthopedic Research and Reviews » Volume 16
Cruciate-Retaining Total Knee Arthroplasty versus Unicompartmental Knee Arthroplasty in Medial Compartmental Osteoarthritis: A Propensity Score-Matched Analysis of Early Postoperative Recovery
Authors Laoruengthana A , Reosanguanwong K, Rattanaprichavej P, Sahasoonthorn K, Santisathaporn N, Pongpirul K
Received 7 November 2023
Accepted for publication 19 March 2024
Published 10 April 2024 Volume 2024:16 Pages 103—110
DOI https://doi.org/10.2147/ORR.S444547
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Clark Hung
Artit Laoruengthana,1 Kongpob Reosanguanwong,1 Piti Rattanaprichavej,1 Kamonnop Sahasoonthorn,1 Nopparat Santisathaporn,1 Krit Pongpirul2,3
1Department of Orthopaedics, Faculty of Medicine, Naresuan University, Phitsanulok, Thailand; 2Department of Preventive and Social Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 3Department of International Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD, USA
Correspondence: Kongpob Reosanguanwong, Department of Orthopaedics, Faculty of Medicine, Naresuan University, Phitsanulok, Thailand, Email [email protected]
Background: Cruciate-retaining (CR) total knee arthroplasty (TKA) may provide better physiological knee kinematics, proprioception, and quadricep recovery than posterior-stabilized (PS) TKA. Therefore, we hypothesized that CR TKA with multimodal pain control may provide comparable postoperative pain and recovery as unicompartmental knee arthroplasty (UKA).
Methods: This study included patients with isolated medial compartment knee osteoarthritis who underwent CR TKA and UKA. TKA and UKA patients were propensity score-matched with age and body mass index (BMI) and compared using visual analog scales (VAS) for pain scores, total amount of morphine use (TMU), knee flexion angle, straight leg raise (SLR), independent ambulation, length of hospital stay (LOS), and costs during hospitalization.
Results: After propensity score matching, 46 patients were included in the TKA and UKA groups, respectively, with no differences in demographic data. VAS at 6– 72 h and TMU at 48 h after surgery were comparable between the groups. The knee flexion angle in the UKA group was significantly higher at 24 h (60.0° vs 46.6°; p< 0.001) and 48 h (76.9° vs 69.1°; p = 0.021) than that in the TKA group. The SLR in the UKA group was significantly higher than that in the TKA group at 24– 72 h. The UKA group ambulated significantly earlier (1.56 vs 2.13 days; p< 0.001), had shorter LOS (3.68 vs 4.28 days; p< 0.004) and incurred 12.43% lower costs when compared to the TKA group.
Conclusion: Patients who underwent CR TKA with multimodal pain management did not experience more postoperative pain or morphine use than those who underwent UKA. However, UKA patients seem to experienced faster recovery and shorter LOS than CR-TKA patients during the early postoperative course. Accordingly, UKA may be considered instead of TKA for patients who are good candidates for UKA and require expedited recovery.
Keywords: total knee arthroplasty, cruciate-retaining, unicompartmental knee arthroplasty, postoperative pain, recovery
Introduction
Osteoarthritis (OA) is the most common degenerative joint disease, characterized by painful swelling and permanent damage to joints. Inflammation of the infrapatellar fat pad and synovial membrane within the knee may play a central role in OA pain, potentially leading to peripheral and central sensitization in knee osteoarthritis (KOA).1 With the increasing prevalence of OA, the number of knee arthroplasties performed is increasing, particularly in younger patients.2 For late-stage medial compartmental knee OA, total knee arthroplasty (TKA) and unicompartmental knee arthroplasty (UKA) are effective surgical procedures for improving patient function and health-related quality of life.3
However, there is an ongoing debate on whether TKA or UKA is a better option for patients with medial compartmental OA of the knee. UKA has gained interest from both surgeons and patients because of its many potential advantages over TKA, including reduced surgical trauma, preservation of bone stock and both cruciate ligaments, less blood loss, and fewer complications.4 However, UKA has been reported in national registries to be associated with a higher rate of revision and inferior survival than TKA.5,6 For instance, the National Joint Registry (NJR) of England, Wales, and Northern Ireland reported that UKA had a 3.2 times higher revision rate than TKA.6 Furthermore, concerning regard to strict patient selection criteria, ideal bearing design, and judicious use of advanced technology cause numerous arthroplasty surgeons hesitate to use this procedure. Thus, many surgeons opt for TKA for patients with medial compartmental OA as their standard practice.
Nevertheless, approximately 20% of patients remain dissatisfied with the results of TKA,7 and high post-TKA pain levels in the perioperative phase can result in persistent postsurgical pain.8 Moreover, inadequate pain control after TKA may increase the risk of perioperative complications such as lung atelectasis, venous thromboembolism and cardiac stress, and can affect functional outcomes at 2-year follow-up.9,10 Posterior cruciate ligament (PCL) preservation for TKA has been considered to provide more physiologic knee kinematics, better proprioception, and better quadricep recovery than posterior-stabilized (PS) TKA.11–13 Cruciate-retaining (CR) prostheses also require less bone resection, resulting in less blood loss than PS prosthesis.14 Additionally, enhanced recovery after surgery (ERAS) protocols which comprises multimodal, multidisciplinary, evidence-based strategies is commonly incorporated into modern perioperative care.15 ERAS protocol has been shown to be an effective strategy for reducing surgical stress and postoperative pain, facilitating early mobilization and recovery, reducing the length of hospital stay (LOS), and improving patient satisfaction after TKA.16 Thus, we hypothesized that patients who undergo less constrained, CR TKA may exhibit comparable recovery in the early postoperative course to those who undergoing UKA.
Recently, a multicenter matched-pair analysis comparing postoperative pain between UKA and TKA in the first 24 h revealed that UKA patients had significantly lower pain scores and required fewer opioids than TKA patients.17 UKA is also associated with shorter LOS, better functional outcomes, and lower costs than TKA.18,19 However, the results from these studies were not specific to the type of TKA design, and the pre- and post-operative care protocols were not controlled. To our knowledge, only a limited number of studies have directly compared the outcomes of CR TKA and UKA during the acute postoperative phase. Hence, the purpose of this study was to compare postoperative pain intensity, analgesic consumption, and recovery between CR TKA and UKA, both employing multimodal pain control, in patients undergoing surgery in similar environments.
Materials and Methods
This study included consecutive patients with isolated medial compartment knee osteoarthritis who underwent unilateral UKA and CR TKA between January 2018 and April 2021. Our indications for UKA were functionally intact anterior and posterior cruciate ligaments, normal lateral compartment, cartilage degeneration in the patellofemoral compartment not greater than grade 3 according to the Outerbridge classification,20 flexion arc ≥ 90°, flexion deformity ≤ 5°, varus deformity ≤ 10°, and body mass index (BMI) < 30. Patients that cannot fulfill these prerequisites would receive CR TKA instead. Patients who had been diagnosed with secondary osteoarthritis, prior knee infection, or previous surgery around the operated knee were excluded from the study. The study protocol was approved by the Institutional Review Board (IRB).
All procedures were performed under spinal anesthesia with bupivacaine (0.5% Marcaine, AstraZeneca, Sweden). Premedication with gabapentin (Gabapentin GPO, GPO, Thailand) and anxiolytic drugs (0.5 mg Tranavan, Polipharm, Thailand) was administered to all patients on the night before surgery. The preemptive adductor canal block (ACB) was individually performed according to the anesthesiologist’s preference for TKA or UKA. Prophylactic antibiotics were administered, the affected leg was prepped using a sterile technique, and the tourniquet was inflated to 250 mm Hg before making a skin incision. All surgical procedures were performed by a single experienced surgeon.
For UKA, the medial parapatellar approach involved a 2 cm incision in the quadriceps tendon. After arthrotomy, infrapatellar fat pad was partially resected. Proximal tibial resection was performed using an extramedullary guide to cut the medial tibial plateau perpendicular to the anatomical tibial axis. Distal femoral resection was performed parallel to the tibial cutting plane using the spacer-block technique. The flexion/extension gap was measured using a gap-checking device that matched the spacer-block thickness. A cemented fixed-bearing UKA prosthesis (Sigma, DePuy Synthes, USA) was implanted with bone cement.
For CR TKA, a midline skin incision of approximately 10 cm was made to perform the medial parapatellar approach. Then infrapatellar fat pad was partially resected, the anterior cruciate ligaments were excised, an extramedullary cutting guide was placed on the tibia, and the proximal tibia was resected perpendicular to the mechanical axis. The distal femoral cut was prepared using an intramedullary guide, and the anterior–posterior femoral cut was completed using the anterior referencing technique. Soft tissue balancing, including medial collateral ligament release and PCL recession, was occasionally performed to achieve an appropriate flexion and extension gap, and the pilot hole in the femoral medullary canal was occluded using a bone plug. Fixed-bearing (FB), CR knee prostheses (PFC Sigma, DePuy Synthes, Warsaw, IN, USA) were implanted with bone cement, and the patella was routinely resurfaced in all cases.
For both groups, periarticular anesthetic injection (PAI) was performed using a cocktail mixture consisting of 20 mL of 0.5% bupivacaine (0.5% Marcaine, AstraZeneca, Sweden) and 30 mg of ketorolac (Ketolac 1 mL, SiuGuan, Taiwan), which was diluted with 0.9% Normal Saline to a total volume of 75 mL. Tranexamic acid (15 mg/kg) was poured into the knee joint before arthrotomy closure. A vacuum drain was placed in the TKA group for 24 h, whereas no drain was applied in the UKA group. The arthrotomy was closed, a compressive dressing was applied, and the tourniquet was deflated.
Identical multimodal pain control was applied in all patients during the postoperative course. Intravenous patient-controlled analgesia (PCA) was used to inject an on-demand bolus of 0.5 mg of morphine sulfate (10 mg/mL Morphine sulfate injection, M&H manufacturing, Thailand) with a 5-minute lockout period, and the amount of morphine consumption was recorded during the first 48 h. During the first 48 h after surgery, intravenous (IV) injection of 30 mg of ketorolac was administered intravenously every 8 h. After 48 h, the PCA and intravenous catheters were discarded. Acetaminophen (500 mg) was administered orally three times daily and naproxen (250 mg) was administered orally twice daily. An additional 2 mg of intravenous morphine was also given every 4–6 h as needed for moderate to severe pain throughout hospitalization. Chemoprophylaxis for venous thromboembolism (VTE) was administered to all patients after the drain was removed, using low-molecular-weight heparin (Clexane, Sanofi-Aventis, France) in the first 48 h and combined with bridging warfarin. Active ankle pumping was encouraged immediately after surgery, and a continuous passive motion (CPM) device (Artromot-K1, Freiburg, Germany) was used on the day after surgery. Early ambulation with gait aids was promoted as tolerated.
The outcomes of this study aim to compare 10 cm visual analog scale (VAS) for pain intensity at rest and the total amount of morphine use (TMU) during the first 48 h, the knee flexion angle measured by a continuous passive motion device while the patient was lying in the supine position and the foot and leg strapped in neutral position, the straight leg raise (SLR) measured by a long-arm universal goniometer, independent ambulation after the index surgery, the incidence of postoperative nausea and vomiting (PONV), LOS, costs during hospitalization, and any other acute complications experienced during hospitalization. All outcome data were prospectively gathered on a regular basis at specific time point (6,12, 18, 24, 48 and 72 h after the surgery) by a group of independent assessors.
Statistical Analysis
Propensity score-matched analysis was used to reduce the potential confounding effects of the observed covariates in both patient groups. The matching method used was the nearest neighbor algorithm, which matched each participant from the study and control groups based on their closest propensity score. The confounding adjustments included age and BMI. All measured characteristics and outcomes were summarized using descriptive statistics, including the frequency, mean, and standard deviation. The normality of data was assessed with Shapiro–Wilk and Kolmogorov–Smirnov test. All outcomes were compared between groups using an independent t-test for continuous variables and the Chi-square or Fisher’s exact test for categorical variables. For non-normally distributed data, the median and range are shown, and the Mann–Whitney U-test was applied to compare the differences between groups. After propensity matching, the sample size of 46 patients had an 83.6% power to detect a difference of 1.5 in VAS score for pain intensity, with an SD of 2.5, alpha error of 5%, and 84.3% power to detect significant differences in LOS. Stata/MP software (version 15.0; StataCorp LP, College Station, TX, USA) was used for all statistical analyses. Statistical significance was defined as p<0.05.
Results
Sixty-two patients who underwent UKA and 71 who underwent CR TKA were enrolled in this study. After propensity score matching, there were 46 patients in the TKA group and 46 in the UKA group, with no differences in age, BMI, sex, ASA classification, preoperative VAS, ROM, Hb, or anesthetic type between the two groups. Demographic data of the participants before and after matching are presented in Table 1.
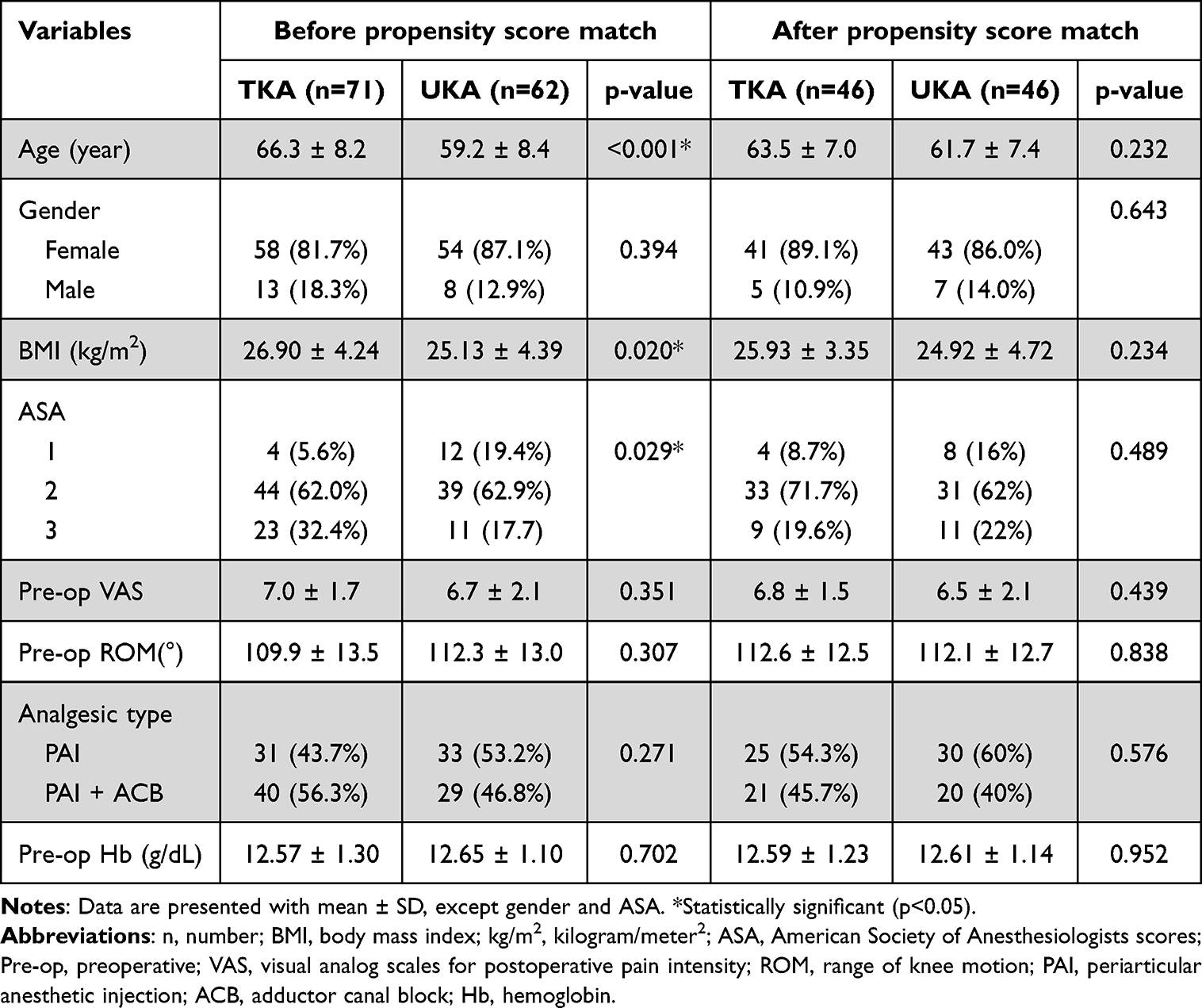 |
Table 1 Demographic Data and Preoperative Characteristics of the TKA and UKA Groups Before and After Propensity Score Matching |
All outcome measures are shown in Table 2. The UKA group had a significantly shorter operative time (defined as skin incision to skin closure) than did the TKA group. There was no difference between the TKA and UKA groups in terms of VAS at 6–72 h, TMU at 24 and 48 h after surgery, or incidence of PONV in the first 24 h after surgery.
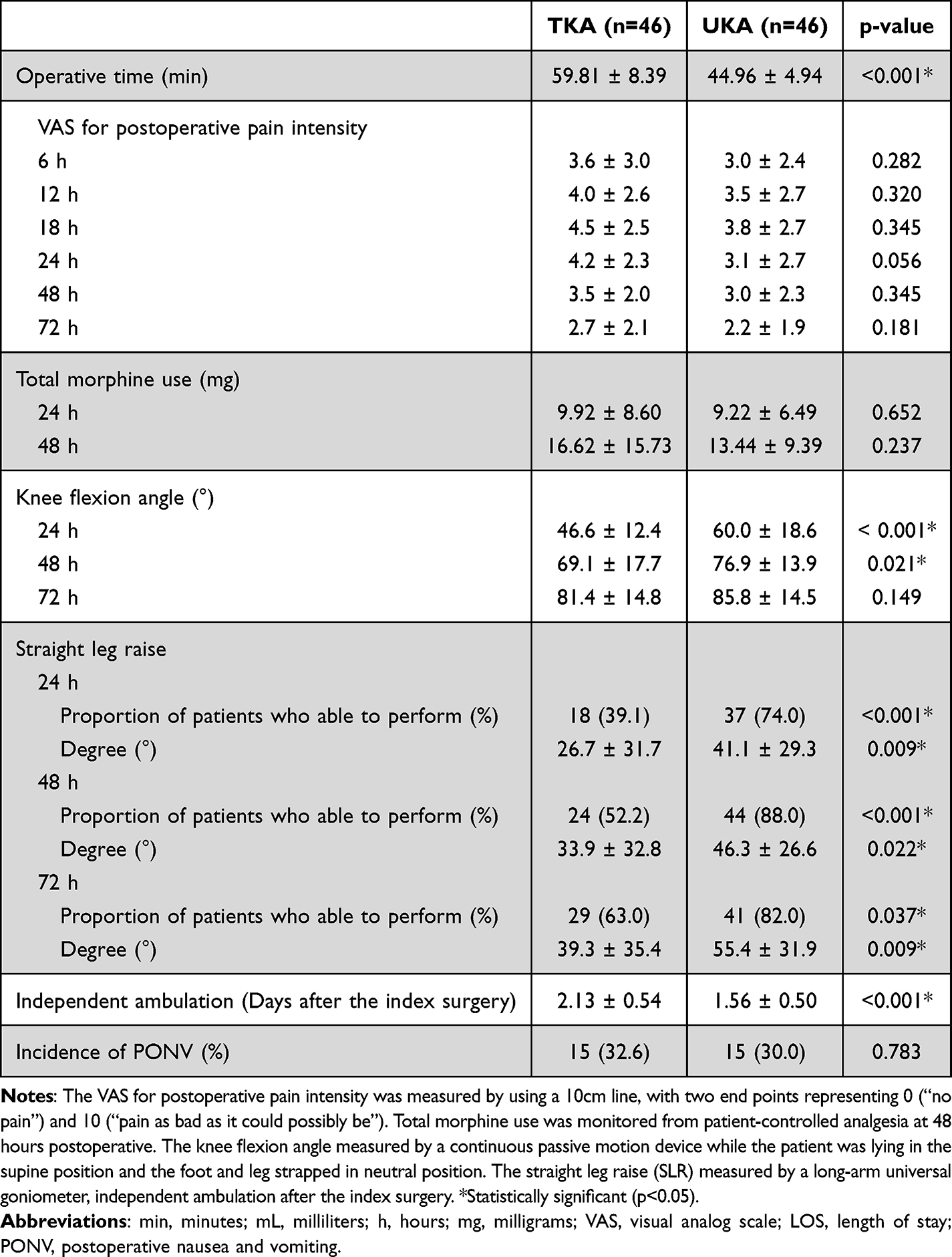 |
Table 2 Peri and Post-Operative Outcomes of the TKA and UKA Groups After Propensity Score Matching |
However, the UKA group showed significantly better knee flexion during the first 48 h than the TKA group. Moreover, significantly more patients in the UKA group could perform the straight leg raise (SLR) than those in the TKA group, and they achieved a higher average degree. Patients in the UKA group could ambulate independently with gait aids earlier than those in the TKA group (p<0.01). The UKA group had a significantly shorter LOS than the TKA group (Figure 1).
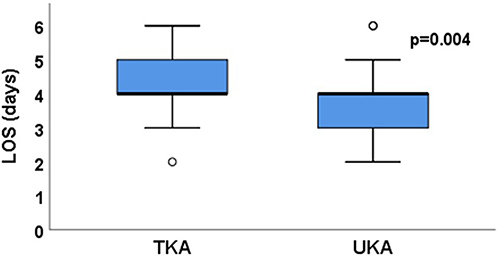 |
Figure 1 LOS demonstrated by Box-Whisker plot. There was a significant difference between groups (p =0.004). Abbreviations: LOS, Length of stay; TKA, Total knee arthroplasty, (UKA) Unicompartmental knee arthroplasty. |
No acute complications, including hemodynamic instability, infection, venous thromboembolism, or falls were observed in either group. At discharge, patients in the UKA group had incurred costs that were 12.43% lower than those in the TKA group (p<0.01).
Discussion
A range of knee prosthesis designs have been used to alleviate pain and improve function in patients with end-stage medial compartmental OA. However, the most preferred prosthesis remains controversial. Regarding postsurgical pain, approximately 50% of patients report being dissatisfied with the perioperative experience of post-TKA pain.8 Thus, post-TKA pain and speed of recovery are still issues of concern to patients, particularly those who have limited social support.7,8,10 A recent large-scale multicenter study and national registry demonstrated that TKA (non-specific design) is associated with higher pain levels, longer LOS, and lower recovery in the early postoperative course than is the case for UKA.17–19 Despite this, we found no difference in pain scores and TMU between patients with medial compartmental OA who underwent CR TKA or UKA. The efficacy of the multimodal pain approach and surgical technique for CR TKA, which is associated with less bony excision, less blood loss, and less constraint than PS TKA, may be an explanation. Currently, multiple analgesic pathways consisting of pre-emptive analgesia, peripheral nerve block, periarticular anesthetic infiltration, and specific systemic medication are principles that enhance recovery after surgery.21 Our multimodal pain regimen for TKA, which comprises PAI with bupivacaine and ketorolac, pre-emptive ACB, and intra-articular tranexamic acid, was developed based on the results of our previous studies to mitigate post-TKA pain.22,23
Nonetheless, in the present study, the UKA group still had a significantly better knee flexion angle and SLR and could independently ambulate earlier than the CR TKA group during the acute postoperative phase. Moreover, our UKA group required a shorter operative time and LOS, which made the procedure 12.43% less costly than TKA. In accordance, a recent prospective randomized multicenter trial that compared UKA and CR TKA showed that the UKA group experienced a faster recovery time than the TKA group, as determined by the Oxford Knee Score (OKS) and Knee Injury and Osteoarthritis Score (KOOS) at 2 and 12 months postoperatively.24 Strickland et al25 demonstrated that UKA resulted in a 2–3 times faster recovery period than TKA, according to the Oxford Arthroplasty Early Recovery Score (OARS) in the first 6 weeks post-surgery. Recently, a systematic review demonstrated that the average time for patients to return to work following UKA was 5.4 weeks (range 1–32 weeks), and > 80% of patients were able to work the same or longer hours or undertake more physically demanding tasks post-surgery.26 Thus, these findings may support the use of UKA in patients with medial compartmental OA who have limited social support and need to accelerate postoperative recovery.
Another subject of debate is whether superior recovery following UKA in the early postoperative course affects outcomes at long-term follow-up.18,27 Although recent prospective randomized multicenter trial showed no differences in patient-reported outcomes, including OKS and KOOS, between UKA and TKA at 2 years post-surgery,18 many previous studies showed that better postoperative range of knee motion and SLR were associated with shorter length of stay, superior patient-reported outcomes, and better patient satisfaction post-surgery.27–31 Kennedy et al27 found that UKA patients had better OKS in all age groups and had better outcomes in the median 10-year follow-up. In some studies, confounding variables were minimized by comparing the outcomes of UKA and TKA in the same patients. According to a study by Pongcharoen et al30 at mean follow-up of 48 months, patients show that the UKA limb feels nearer to their normal knee when they report a significantly higher JFS and KOOS than do those receiving a TKA limb. Gait analysis in 16 patients who had received one TKA and one UKA knee on the contralateral side also showed that the UKA was the preferred knee and nearer to the normal knee when compared to the TKA limb.31
Furthermore, surgeons and patients might consider the costs of procedures. Although revision rates for UKA were significantly higher than TKA at 5 and 10 years postoperatively, the cumulative mean healthcare costs for patients who underwent UKA were significantly lower than those who underwent TKA, up to 10 years post-surgery.32 In addition, the Total or Partial Knee Arthroplasty Trial (TOPKAT),33 a multicenter, pragmatic randomized controlled trial comparing the cost-effectiveness of UKA and TKA, demonstrated that UKA resulted in fewer complications and was significantly more effective and less expensive than TKA during the 5 years of follow-up.
However, our study had some limitations. First, this study had a retrospective design, which may have introduced confounding factors. The patients in the UKA group in our study were younger and had a lower ASA score and lower BMI than those in the TKA group. Thus, we conducted propensity score matching, and subsequently found no demographic difference between the UKA and TKA groups. However, propensity score matching does not guarantee an exact match for all individuals. Although the current expanded indication for medial UKA was applied in our study, patients undergoing CR TKA must have at least one factor not fulfilled for UKA, such as preoperative pain severity due to the patellofemoral compartment and the degree of preoperative lower limb deformity, which could affect the clinical evaluation. Second, our study can only represent early postoperative results without specific knee score assessment; prolonged follow-up in this patient cohort would be beneficial to demonstrate the differences in clinical outcomes between the groups. Third, we did not determine the amount of opioids that patients might generally use before surgery. Finally, the variability in healthcare systems among countries may have a significant impact on patient recovery and costs.
Conclusion
Patients who underwent CR TKA with multimodal pain management did not experience more postoperative pain or morphine use than those who underwent UKA. However, UKA patients seem to experienced faster recovery and shorter LOS than CR TKA patients during the early postoperative course. Accordingly, UKA may be considered instead of TKA for patients who are good candidates for UKA and require expedited recovery.
Ethics Approval and Informed Consent
Ethical clearance was obtained from the Institutional Review Board of the Naresuan University (IRB number P3-0015/2563 with protocol number 112/2020). Participants for the research will be selected based on predefined criteria. Before collecting the data, describe the details regarding the research data, explaining how the data collected in this research will be used for research purposes, and provide details about the research itself. Those who are selected to participate in the research must agree to participate and sign personally. The study was carried out in compliance with the International guidelines for human research protection as Declaration of Helsinki, The Belmont Report, CIOMS guideline and International Conference on Harmonization in Good Clinical Practice (ICH-GCP).
Acknowledgments
The authors gratefully acknowledge Bhuwad Chinwatanawongwan, MD; Pawin Sudbanthad, MD; Sasawat Ratanapises, MD; Passakorn Teekaweerakit, MD; Parin Samapath, MD; and Wasee Lertkajornsin for their technical assistance; and Ms. Dollapas Punpanich for her expertise with statistical analysis. We thank Mr. Roy I. Morien of the Naresuan University Graduate School for his assistance in editing the English expression and grammar in this document.
Funding
This study was performed with no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Belluzzi E, Stocco E, Pozzuoli A, et al. Contribution of infrapatellar fat pad and synovial membrane to knee osteoarthritis pain. Biomed Res Int. 2019;2019:6390182. doi:10.1155/2019/6390182
2. Singh JA, Yu S, Chen L, Cleveland JD. Rates of total joint replacement in the United States: future projections to 2020–2040 using the national inpatient sample. J Rheumatol. 2019;46(9):1134–1140. PMID: 30988126. doi:10.3899/jrheum.170990
3. Rönn K, Reischl N, Gautier E, Jacobi M. Current surgical treatment of knee osteoarthritis. Arthritis. 2011;2011:454873. PMID: 22046517; PMCID: PMC3200113. doi:10.1155/2011/454873
4. Schwab PE, Lavand’homme P, Yombi JC, Thienpont E. Lower blood loss after unicompartmental than total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2015;23(12):3494–3500. PMID: 25063489. doi:10.1007/s00167-014-3188-x
5. Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR). Hip, knee & shoulder arthroplasty: 2020 annual report, Adelaide; AOA, 2020: 1–474.
6. Porter M, Borroff M, Gregg P National joint registry for England 10th annual report. Wales and Northern Ireland; 2013.
7. Hirschmann MT, Testa E, Amsler F, Friederich NF. The unhappy total knee arthroplasty (TKA) patient: higher WOMAC and lower KSS in depressed patients prior and after TKA. Knee Surg Sports Traumatol Arthrosc. 2013;21(10):2405–2411. PMID: 23358576. doi:10.1007/s00167-013-2409-z
8. Grosu I, Lavand’homme P, Thienpont E. Pain after knee arthroplasty: an unresolved issue. Knee Surg Sports Traumatol Arthrosc. 2014;22(8):1744–1758.
9. American Society of Anesthesiologists Task Force on Acute Pain Management. Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of anesthesiologists task force on acute pain management, Anesthesiology. 2012;116(2):248–273. PMID: 22227789. doi:10.1097/ALN.0b013e31823c1030
10. Lakra A, Murtaugh T, Shah RP, Cooper HJ, Geller JA. Early postoperative pain predicts 2-year functional outcomes following knee arthroplasty. J Knee Surg. 2020;33(11):1132–1139. PMID: 31269524. doi:10.1055/s-0039-1692650
11. Andriacchi TP, Galante JO. Retention of the posterior cruciate in total knee arthroplasty. J Arthroplasty. 1988;3:S13–9. PMID: 3199135. doi:10.1016/s0883-5403(88)80003-2
12. Dorr LD, Ochsner JL, Gronley J, Perry J. Functional comparison of posterior cruciate-retained versus cruciate-sacrificed total knee arthroplasty. Clin Orthop Relat Res. 1988;236:36–43. PMID: 3180584.
13. Warren PJ, Olanlokun TK, Cobb AG, Bentley G. Proprioception after knee arthroplasty. The influence of prosthetic design. Clin Orthop Relat Res. 1993;297:182–187. PMID: 8242929.
14. Mähringer-Kunz A, Efe T, Fuchs-Winkelmann S, Schüttler KF, Paletta JR, Heyse TJ. Bleeding in TKA: posterior stabilized vs. cruciate retaining. Arch Orthop Trauma Surg. 2015;135(6):867–870. PMID: 25917192. doi:10.1007/s00402-015-2209-7
15. Moningi S, Patki A, Padhy N, Ramachandran G. Enhanced recovery after surgery: an anesthesiologist’s perspective. J Anaesthesiol Clin Pharmacol. 2019;35(Suppl 1):S5–S13. doi:10.4103/joacp.JOACP_238_16
16. Gaffney CJ, Pelt CE, Gililland JM, Peters CL. Perioperative pain management in hip and knee arthroplasty. Orthop Clin North Am. 2017;48(4):407–419. PMID: 28870302. doi:10.1016/j.ocl.2017.05.001
17. Leiss F, Götz JS, Maderbacher G, et al. Pain management of unicompartmental (UKA) vs. total knee arthroplasty (TKA) based on a matched pair analysis of 4144 cases. Sci Rep. 2020;10(1):17660. PMID: 33077754; PMCID: PMC7572421. doi:10.1038/s41598-020-74986-x
18. Wilson HA, Middleton R, Abram SGF, et al. Patient relevant outcomes of unicompartmental versus total knee replacement: systematic review and meta-analysis. BMJ. 2019;364:l352. doi:10.1136/bmj.l352
19. Mohammad HR, Judge A, Murray DW. A matched comparison of the patient-reported outcome measures of 38,716 total and unicompartmental knee replacements: an analysis of linked data from the National Joint Registry of England, Northern Ireland and Isle of Man and England’s National PROM collection programme. Acta Orthop. 2021;92(6):701–708. PMID: 34309481; PMCID: PMC8635544. doi:10.1080/17453674.2021.1956744
20. Outerbridge RE. The etiology of chondromalacia patellae. J Bone Joint Surg Br. 1961;43-B(4):752–757. doi:10.1302/0301-620X.43B4.752
21. Franzoni S, Rossi SMP, Cassinadri A, Sangaletti R, Benazzo F. Perioperative pain management in total knee arthroplasty: a narrative review of current multimodal analgesia protocols. Appl. Sci. 2023;13:3798. doi:10.3390/app13063798
22. Laoruengthana A, Rattanaprichavej P, Mahatthanatrakul A, Tantimethanon T, Lohitnavy M, Pongpirul K. Periarticular Injection of ketorolac augmenting intravenous administration of ketorolac for postoperative pain control: a randomized controlled trial in simultaneous bilateral total knee arthroplasty. J Knee Surg. 2022;35(8):868–873. PMID: 33231281. doi:10.1055/s-0040-1721088
23. Laoruengthana A, Rattanaprichavej P, Rasamimongkol S, Galassi M, Weerakul S, Pongpirul K. Intra-articular tranexamic acid mitigates blood loss and morphine use after total knee arthroplasty. a randomized controlled trial. J Arthroplasty. 2019;34(5):877–881. PMID: 30755381. doi:10.1016/j.arth.2019.01.030
24. Knifsund J, Niinimaki T, Nurmi H, et al. Functional results of total-knee arthroplasty versus medial unicompartmental arthroplasty: two-year results of a randomised, assessor-blinded multicentre trial. BMJ Open. 2021;11(6):e046731. PMID: 34162649; PMCID: PMC8231055. doi:10.1136/bmjopen-2020-046731
25. Strickland LH, Rahman A, Jenkinson C, Pandit HG, Murray DW. Early recovery following total and unicompartmental knee arthroplasty assessed using novel patient-reported measures. J Arthroplasty. 2021;36(10):3413–3420. PMID: 34120796. doi:10.1016/j.arth.2021.05.025
26. Ng HJH, Loke WJ, James Liang Hao W. Return to work after medial unicompartmental knee arthroplasty: a systematic review. Knee. 2021;30:254–266. PMID: 33975066. doi:10.1016/j.knee.2021.04.015
27. Kennedy JA, Mohammad HR, Mellon SJ, Dodd CAF, Murray DW. Age stratified, matched comparison of unicompartmental and total knee replacement. Knee. 2020;27(5):1332–1342. PMID: 33010745. doi:10.1016/j.knee.2020.06.004
28. Devers BN, Conditt MA, Jamieson ML, Driscoll MD, Noble PC, Parsley BS. Does greater knee flexion increase patient function and satisfaction after total knee arthroplasty? J Arthroplasty. 2011;26(2):178–186. PMID: 20413247. doi:10.1016/j.arth.2010.02.008
29. Suh J, Liow MHL, Pua YH, et al. Early postoperative straight leg raise is associated with shorter length of stay after unilateral total knee arthroplasty. J Orthop Surg. 2021;29(1):23094990211002294. PMID: 33779408. doi:10.1177/23094990211002294
30. Pongcharoen B, Timjang J. The outcomes of mobile bearing unicompartmental knee arthroplasty and total knee arthroplasty on anteromedial osteoarthritis of the knee in the same patient. Arch Orthop Trauma Surg. 2020;140(11):1783–1790. PMID: 32710343. doi:10.1007/s00402-020-03527-y
31. Wiik AV, Nathwani D, Akhtar A, Al-Obaidi B, Strachan R, Cobb JP. The unicompartmental knee is the preferred side in individuals with both a unicompartmental and total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2020;28(10):3193–3199. PMID: 31781799; PMCID: PMC7511463. doi:10.1007/s00167-019-05814-7
32. Burnett Iii RA, Yang J, Courtney PM, Terhune EB, Hannon CP, Della Valle CJ. Costs of unicompartmental compared with total knee arthroplasty: a matched cohort study over ten years. Bone Joint J. 2021;103-B(6 Supple A):23–31. PMID: 34053283. doi:10.1302/0301-620X.103B6.BJJ-2020-2259.R1
33. Beard DJ, Davies LJ, Cook JA, et al.; TOPKAT Study Group. The clinical and cost-effectiveness of total versus partial knee replacement in patients with medial compartment osteoarthritis (TOPKAT): 5-year outcomes of a randomised controlled trial. Lancet. 2019;394(10200):746–756. PMID: 31326135; PMCID: PMC6727069. doi:10.1016/S0140-6736(19)31281-4
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.