")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 19
Correlation Between Diaphragmatic Excursion and Exercise Tolerance Improvement Following Pulmonary Rehabilitation in Patients with Chronic Obstructive Pulmonary Disease-Obstructive Sleep Apnea Overlap Syndrome
Authors Shen H , Xu Y, Zhang Y, Ren L, Chen R
Received 4 October 2023
Accepted for publication 26 December 2023
Published 9 January 2024 Volume 2024:19 Pages 63—75
DOI https://doi.org/10.2147/COPD.S437698
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Min Zhang
Honghua Shen,1,2 Yiming Xu,2 Yin Zhang,2 Lei Ren,2 Rui Chen1
1Department of Respiratory Medicine, the Second Affiliated Hospital of Soochow University, Suzhou, 215004, People’s Republic of China; 2Department of Respiratory Rehabilitation, the Fourth Rehabilitation Hospital of Shanghai, Shanghai, 200040, People’s Republic of China
Correspondence: Rui Chen, Department of Respiratory Medicine, the Second Affiliated Hospital of Soochow University, Suzhou, 215004, People’s Republic of China, Email [email protected]
Purpose: We assess the predictive value of diaphragm excursion (DE) in enhancing exercise tolerance following pulmonary rehabilitation (PR) among patients with COPD-OSA overlap syndrome.
Material and Methods: This prospective cohort study enrolled 63 patients diagnosed with COPD-OSA overlap syndrome who actively participated in a PR program from January 2021 to May 2023. Among these, 58 patients successfully completed the 20-week PR program, with exercise tolerance assessed through the measurement of six-minute walk distance (6MWD), and DE evaluated by ultrasonography. The responder to PR in terms of exercise ability was defined as a patient who showed an increase of > 30m in 6MWD. The cutoff value for predicting PR response based on DE was determined using receiver operating characteristic (ROC) curves.
Results: Following the PR program, significant improvements were observed in mMRC, 6MWD, DE during deep breathing, and diaphragm thickness fraction (DTF). Of the participants, 33 patients (57%) were classified as responders, while 25 patients (43%) were considered non-responders. Baseline values of FEV1% predicted, 6MWD, DE during deep breathing, DTF, and PaO2 exhibited a significant elevation in responders as compared to non-responders. The changes of 6MWD were positively associated with the baseline values of DTF and DE during deep breathing, FEV1% predicted and PaO2, while negatively correlated with baseline value of mMRC. The predictive performance in terms of the area under the ROC curve for determining responder’s DTF was found to be 0.769, accompanied by a sensitivity of 85% and specificity of 68%, using a cutoff value at 17.26%. Moreover, it was observed that DE during deep breathing could predict the area under the ROC curve for responders to be 0.753, with a sensitivity of 91% and specificity of 56% at a cutoff value of 3.61cm.
Conclusion: Diaphragm excursion serves as a valuable predictor for determining the enhancement of exercise tolerance following PR in patients with COPD-OSA overlap syndrome.
Trial Registration: ChiCTR1800020257, www.chictr.org.cn/index.aspx.
Keywords: pulmonary rehabilitation, COPD-OSA overlap syndrome, diaphragm excursion, diaphragm thickness fraction, six-minute walk distance
Background
Overlap syndrome1 denotes the coexistence of Chronic Obstructive Pulmonary Disease (COPD) and Obstructive Sleep Apnea (OSA), which is anticipated to manifest in approximately 0.5% of adults aged over 40 years, and is associated with substantial morbidity and mortality.2 In China, the prevalence of coexisting COPD with OSA was determined to be 66.0% based on Apnea-Hypopnea Index (AHI) of ≥5 events/h, with 23% exhibiting an AHI ≥ 15 events/h.3 COPD is a prevalent and preventable condition characterized by persistent airflow limitation that exhibits limited reversibility.4 The occurrence of OSA is characterized by recurrent upper airway closure during sleep and is frequently observed in individuals with COPD. The overlap syndrome presents poorer outcomes than OSA or COPD alone, and its management differs from that of either condition. Therefore, the identification of concurrent OSA in individuals diagnosed with COPD gives significant clinical ramifications.
The overlap syndrome exerts a more profound detrimental impact on the quality of life in individuals with COPD, leading to reduced daily activity attributed to dyspnea. The coexistence of COPD and OSA leads to more severe nocturnal hypoxemia and hypercapnia effects than either condition alone, due to their similar pathophysiological effects, particularly in terms of hypoxia and systemic inflammation.5–7 Additionally, overlap syndrome is associated with a decrease in daytime oxygen saturation and quality of life scores, as well as an increase in the frequency of acute exacerbations, comorbidities, and economic burden linked to COPD.8,9
Although there is limited literature on rehabilitation interventions for OSA, there is substantial evidence supporting pulmonary rehabilitation (PR) as the standard of care for patients with COPD.10 The implementation of PR has been documented to enhance dyspnoea, exercise capacity, and quality of life among patients diagnosed with COPD.11 Studies by Boutou et al12 and Costi et al13 demonstrated that patients with better exercise capacity and health-related quality of life likelihood of successfully completing PR. Conversely, van Ranst et al reported inconclusive findings, indicating that status and extensive utilization of health-care services may encounter challenges in effectively completing PR.14
Despite a more unfavorable prognosis, there is a critical need for clinical attention to rehabilitation, and objective evaluation of therapeutic effects is necessary for individuals with COPD-OSA overlap syndrome. Currently, there is no universally accepted standardized approach for accessing diaphragm excursion in patients with overlap syndrome both pre- and post-PR. Although computed tomography (CT) and dynamic magnetic resonance imaging (MRI) have been used in previous studies to measure diaphragm movement, the utilization of these methodologies incurs substantial expenses and exposes individuals to heightened levels of radiation.15–17 In contrast, ultrasound (US) imaging, a cost-effective and widely available technique devoid of ionizing radiation risks, is not commonly used to assess diaphragm dysfunction associated with COPD-OSA overlap syndrome. Relevant investigations have been conducted to explore the thickness and motion of the diaphragm in individuals with COPD, and similar studies on diaphragm using ultrasonography have been conducted.18,19 Given the pivotal role of dynamic lung hyperinflation (DLH) in the pathogenesis of dyspnea and impaired exercise capacity among patients with COPD, employing objective measures that accurately reflect the extent of DLH could facilitate the identification of individuals who are likely to respond favorably to PR. Shiraishi et al20 reported that ultrasonography can effectively predict the improvement in exercise tolerance after PR in patients with COPD by measuring the maximum level of DE. However, there is a lack of previous investigation on the US characteristics of the diaphragm for COPD-OSA overlap syndrome. Therefore, it is crucial to accurately identify patients who are more likely to derive greater benefits from a PR program, especially for these patients. The primary objective of this study is to elucidate the role of diaphragmatic excursions in predicting the enhancement in exercise tolerance following PR in individuals with COPD-OSA overlap syndrome.
Methods
Materials and Methods
Study Design and Subjects
This present study is a prospective cohort study with a parallel group design and a 20-week follow-up period. It was conducted at the Department of Respiratory Rehabilitation, The Fourth Rehabilitation Hospital of Shanghai, China, from January 2021 to May 2023, following the principles of good clinical practice.
The study was granted approval by the Ethics Committee of The Fourth Rehabilitation Hospital of Shanghai (SP202002), and written informed consent was obtained from all participants.
The inclusion criteria with both COPD and OSA were defined as follows:
- The diagnosis of stable COPD is established by integrating clinical history, physical examination findings, chest radiography results, and pulmonary function tests in accordance with the diagnostic and severity criteria for COPD outlined by the Global Initiative for Chronic Obstructive Lung Disease (GOLD);21
- Inpatients or outpatients diagnosed with stable COPD and exhibiting peripheral oxygen saturation (SpO2) ≥ 92% during calm breathing;
- Absence of acute exacerbation for a minimum duration of 4 weeks and self-reported the history of OSA.
- No clinically significant respiratory, neuromuscular, or other disorders causing hypercapnia;
- Ability to undergo all-night polysomnographic (PSG) testing. The severity of OSA was categorized as mild if the AHI ranged from ≥5/h to <15/h, moderate if it ranged from ≥15/h to <30/h, and severe if it was ≥30/h.
The exclusion criteria in this study were as follows:
- Patients presenting with gas exchange abnormalities resulting from alternative etiologies and restrictive pulmonary conditions. (eg, bronchiectasis, interstitial fibrosis, diaphragmatic paralysis, and kyphoscoliosis) were excluded;
- Concurrent administration of anxiolytics, analeptic, or treatment for other comorbid respiratory conditions;
- The diseases exerted negative effects on the diaphragm by affecting small vessels and inducing neuropathy were excluded. Furthermore, patients with cognitive or psychiatric disorders, speech disorders, wound healing disorders, as well as other orthopedic and neurological disorders that restrict movement from the scope of patient recruitment were also excluded.
Patients provided informed consent prior to participation, and the protocols adhered to international ethical standards.
Measurements
Demographic and clinical data, including age, gender, GOLD stage, and Body Mass Index (BMI) at the initiation of PR, as well as results of pulmonary function tests and frequency of COPD exacerbations were extracted from the medical records. Two time points for evaluations were conducted at baseline and after 20 weeks of PR.
Ultrasonography Study
Ultrasonography (SONIMAGE HS1, Konica Minolta, Tokyo, Japan) was conducted to assess diaphragm excursion (DE) and diaphragm thickness in all participants. A convex array probe with a frequency range of 1 to 5 MHz and a linear array probe with a frequency range of 8 to 10 MHz were employed. Diaphragm excursion was the vertical distance between the position of the diaphragm raised at the end of expiration and the position of the diaphragm lowered at the end of inspiration (Figure 1B2 and C2). Under the B-mode, the diaphragm was seen as a single echogenic line (Figure 1B1 and C1), moving towards the probe during inhalation and away from the probe during exhalation. The convex array probe was positioned between the mid-clavicular and mid-axillary lines below the right costal margin, and the right hemidiaphragm was measured with the liver as the acoustic window at a frequency of 3.5-MHz.22,23 The probe was placed medially, cranially, and dorsally, so that the ultrasound beam could be perpendicular to the right hemi-diaphragmatic dome. The convex array probe visualized the right hemi-diaphragm in B-mode, and the diaphragm excursion was quantified using images acquired during calm breathing and deep breathing in M mode. The highest value obtained from three measurements was utilized.
 |
Figure 1 Using the liver as an acoustic window. (A) Represents the diaphragm thickness. (B) Represents the diaphragm excursion during deep breathing. (C) Represents the diaphragm excursion during calm breathing. |
For diaphragm thickness assessment, the patient was positioned in a supine posture, and the high-frequency linear array probe was placed along the mid-clavicle line, extending towards the midpoint of the front axillary line until reaching the junction between the seventh and eighth costal cartilage. The thickness of the diaphragm, which exhibited hyperechoic characteristics on both sides and hypoechoic characteristics internally, was measured and recorded at the termination of inspiratory and expiratory phases (Figure 1A). The average value was determined through three measurements. The diaphragm thickness fraction (DTF) was computed as (diaphragmatic thickness at the end of inspiration, DTei) - (diaphragmatic thickness at the end of expiration, DTee)/DTee × 100%.
Pulmonary Function Tests
The spirometry and plethysmography were performed using a Master Screen device (Care Fusion Germany 234 GmbH, Germany) by proficient personnel in a quiet environment. Three trials were conducted for each test, and the optimal outcomes were recorded to determine forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1), and the FEV1/FVC ratio.
PSG Study
All participants underwent a single night of PSG study, lasting at least 8 hr, at the sleep laboratory within our department. Overnight sleep polysomnography (SOMNO check 2; Weinmann; Germany) included electroencephalography, electrooculography, submental electromyography, electrocardiography, bilateral anterior tibialis electromyography, nasal airflow measurement, oxygen saturation assessment, thoracoabdominal movement monitoring, body position tracking, and snoring. The sleep parameters were manually scored in accordance with the American Academy of Sleep Medicine (AASM) Manual v2.3 2016.24 Respiratory sleep patterns were examined following the recommendations provided by AASM.25 Apnea was defined as the cessation of airflow for a minimum duration of 10 s, accompanied by respiratory effort, while hypopnea was characterized by a reduction in airflow of at least 30% lasting for at least 10 s and associated with either a decrease in oxygen saturation of ≥3% or arousal. TS90 referred to the percentage of time spent during sleep with oxygen saturation levels <90%. The AHI was calculated to assess severity, referred to as the average number of apnea and hypopnea events per hour. Individuals with an AHI ≥ 5 were classified as having OSA, whereas those with an AHI of <5 were categorized as primary snorers.
Assessment of Other Parameters
Arterial blood gases, including pH, PaO2, and PaCO2, were evaluated through supine resting arterial blood gas analysis upon waking in the morning.
A modified British Medical Research Council (mMRC) questionnaire was applied to assess the severity of dyspnea during daily activities.26
The six-minute walk distance (6MWD) was conducted in accordance with a statement from the American Thoracic Society (ATS)/European Respiratory Society (ERS) to assess walking capacity.27–29 The 6MWD test was conducted on both pro- and post-PR programs for all participants. Responders to PR in terms of exercise capacity were defined as individuals who exhibited a post-PR increase of more than 30 m in the 6MWD, which was considered the minimal clinically important difference (MCID) for this measure.30
Cardiopulmonary Exercise Testing
In the current study, an incremental exercise test was conducted on a MasterScreen CPX electrically braked cycle ergometer (CareFusion Germany 234 GmbH) with a pedaling cadence of approximately 60 revolutions per minute and terminated upon symptom limitation or in the presence of electrocardiographic changes. After a 3-min rest period followed by 3 min of unloaded pedaling, the work rate was progressively increased (ramp) at a rate of 5–10 Watts per minute, based on the spirometry results of each subject. Upon cessation of exercise, participants were requested to articulate their primary reason for discontinuing physical activity, such as experiencing breathing difficulties or discomfort in the legs, or any other documented rationale. The intensity of PR was determined through cardiopulmonary exercise testing, specifically targeting a range of 50–70% of peak oxygen uptake, which is defined as moderate-intensity PR exercise. Similar to previous studies, these cutoff values were determined based on the prognostic significance of patients’ maximal oxygen uptake.31
PR Intervention
Patients diagnosed with COPD-OSA overlap syndrome participated in a standardized multidisciplinary inpatient PR program, encompassing comprehensive health education, psychological support, and tailored aerobic exercise. The provision of psychological support offers patients assistance, guidance, solace, and encouragement while also directing them towards active participation in rehabilitation training. Exercise duration and intensity were adjusted based on individual clinical complaints and cardiopulmonary exercise testing results. All enrolled patients underwent a 20-week course of PR treatment, consistently attending sessions 5 days per week.
The aerobic exercise lasted for 40 min daily, comprising a 10-min pre-exercise warm-up, a 10-min post-exercise relaxation, and a 20-min stationary cycling exercise utilizing the Upper-Lower Limb Coordination Exercise Machine (Jiangsu Tianrui Medical Equipment Co., Ltd., Nanjing, China). The exercise started at 50% of the maximum load achieved during the cardiopulmonary exercise test. If the patient maintained stable heart rate and blood oxygen saturation demonstrating good exercise tolerance, the workload was gradually incremented by 10 W. The electrocardiogram signals and the SpO2 level were continuously monitored throughout the exercise session and post-exercise period.
Exercise was terminated if the SpO2 dropped below 85%, blood pressure exceeded 200/100 mmHg, or the heart rate reached 90% of the maximum value during cardiopulmonary exercise testing to ensure patient safety. If a patient experienced severe dyspnea and exhibited subjective intolerance to exercise, the physiotherapist would document the case and provide the patient with a 5-min rest period prior to resuming their training. Patients who exhibited repeated refusal to do aerobic training more than three times or demonstrated poorly cooperative behavior were excluded from this study.
Statistical Analysis
The statistical analyses were conducted using SPSS 22.0 software (IBM, Armonk, NY, USA). Prior to analysis, the normality of continuous data was assessed through the application of both the Kolmogorov–Smirnov test and the Shapiro–Wilk test. The paired t-test or the Wilcoxon signed-rank test was employed to assess alterations in parameters pre- and post-implementation of the PR program. Responders and non-responders were compared using appropriate statistical tests, including the t-test, the Wilcoxon rank-sum test, or χ2 test. The Pearson correlation coefficient was employed to examine the association between changes in 6MWD and independent variables. The receiver operating characteristic curve analysis was employed to evaluate the predictive capacity of diaphragm excursion in determining the response. The statistical significance was determined at a significance level of P<0.05 (two-tailed).
Result
Among the 63 patients diagnosed with COPD-OSA overlap syndrome and included in this study, a total of 58 individuals successfully completed the PR program (Figure 2). Three patients terminated their involvement in the PR program owing to poor cooperation, while two patients discontinued their participation due to severe exacerbation of COPD.
 |
Figure 2 Study flow diagram. Abbreviation: 6MWD, 6-min walk distance. |
Baseline Characteristics of the Participants
Among the patients who underwent PR, 33 individuals demonstrated a significant increase of >30 meters in their 6MWD post-intervention, indicating a positive response rate of 57%. Conversely, 25 patients (43%) were categorized as non-responders. Responders had significantly higher baseline values of FEV1, FEV1/FVC, FEV1%predicted, 6MWD, diaphragm excursion during deep breathing, DTF, and PaO2, and significantly lower mMRC scores compared to non-responders (all P<0.05) (Table 1). However, no significant differences were observed in gender, age, BMI, GOLD stage, underlying disease, number of positive airway pressure (PAP), and long-term oxygen therapy (LTOT) users, PaCO2, and diaphragm excursion during calm breathing between responders and non-responders (all P > 0.05) (Table 1).
 |
Table 1 Baseline Characteristics of Study Participants |
Effects of Pulmonary Rehabilitation
After the implementation of PR program, there was a significant improvement observed in all patients regarding 6MWD result, mMRC scores, AHI, diaphragm excursion during deep breathing, and DTF values (all P<0.05) (Table 2).
 |
Table 2 Effects of Pulmonary Rehabilitation (n = 58) |
Associations Between Changes in 6MWD and Baseline Characteristics
The changes in 6MWD were significantly and positively associated with baseline values of DTF, diaphragm excursion during deep breathing, FEV1, FEV1/FVC, FEV1%predicted, and PaO2,(all P<0.001). Additionally, they exhibited a negative correlation with baseline values of AHI and mMRC (all P<0.05) (Table 3, Figure 3).
 |
Table 3 Associations Between Changes in 6MWD and Baseline Characteristics |
 |
Figure 3 The relationship between DTF (%) and changes in 6MWD after pulmonary rehabilitation was examined. The results showed a significant positive correlation between changes in 6MWD and DTF% (r = 0.758; P< 0.001). Abbreviations: DTF, diaphragm thickness fraction; 6MWD, 6-min walk distance. |
ROC Curve Assesses the Predictive Ability of Independent Variables for 6MWD (> 30 m) Following PR
The ROC curve analysis demonstrated that the area under the curve (AUC) values for DE during deep breathing and DTF in predicting positive response individuals were 0.753 and 0.769, respectively, with a sensitivity of 91% and 85%, specificity of 56% and 68%, at the cut-off values of 3.61 cm and 17.26%. Similarly, the AUCs of FEV1%predicted and PaO2 for predicting responders were found to be 0.754 and 0.719, respectively, with a sensitivity of 79% for both variables, specificity of 64% and 60%, at the cutoff values of 47.5% and 60.5 mmHg (Figure 4) (Table 4).
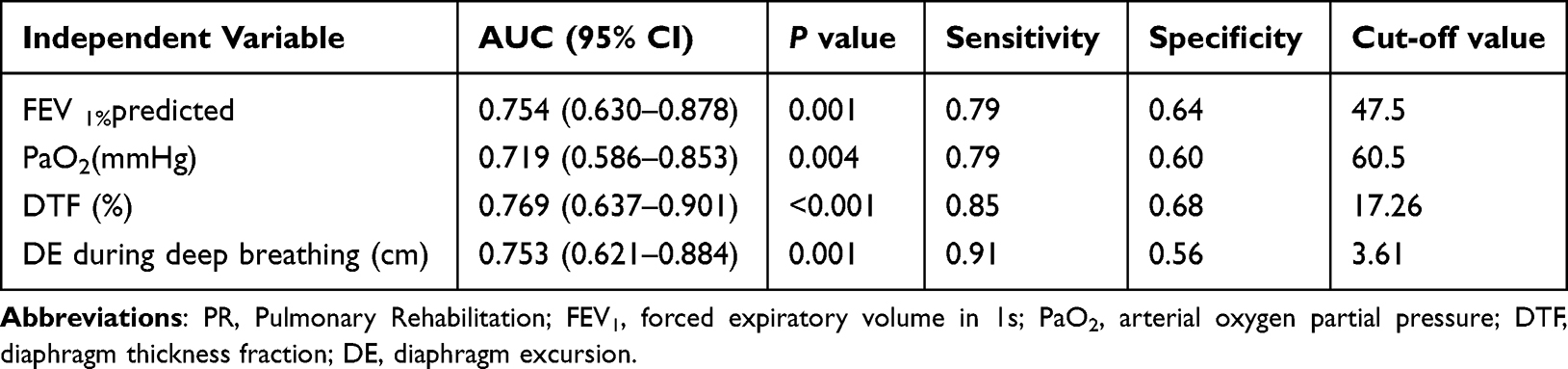 |
Table 4 ROC Curve Assesses the Predictive Ability of Independent Variables for 6MWD (>30 m) Following PR |
 |
Figure 4 Receiver operating characteristic (ROC) curves were generated to assess the predictive ability of baseline DE during deep breathing, DTF (%), FEV1%predicted, and PaO2 for the response to pulmonary rehabilitation. Abbreviation: DE, diaphragm excursion. |
Discussion
This study represents the initial demonstration of diaphragm excursion’s utility in predicting the effectiveness of a 20-week pulmonary rehabilitation program for patients with COPD-OSA overlap syndrome. Among the participants, 33 patients (57%) were categorized as responders, while 25 patients (43%) were classified as non-responders. The changes in 6MWD exhibited a significant positive correlation with the baseline values of diaphragm excursion during deep breathing and DTF, while displaying a negative correlation with mMRC. Interestingly, no difference was observed in diaphragm excursion during calm breathing between responders and non-responders; however, it increased significantly during exercise. The ROC curve analysis revealed that the AUC of diaphragm excursion during deep breathing in predicting the responders was 0.753, with a sensitivity of 91% and a specificity of 56% at a cutoff value of 3.61cm. Additionally, the AUC of DTF in predicting the responders was 0.769, with a sensitivity of 85% and a specificity of 68% at a cutoff value of 17.26%.
The efficacy of PR has been demonstrated in patients with chronic respiratory diseases, as supported by our previous research32 and confirmed in this study. However, the extent of benefit from PR varies among patients. While ideally PR would be effective for all patients,33 it has been observed that the response to PR differs significantly between individuals34–37. In this study, responders exhibited significantly higher baseline values of pulmonary ventilation function, 6MWD, diaphragm excursion during deep breathing, DTF, and PaO2, while significantly lower mMRC scores compared to non-responders. However, there was no statistical difference in AHI and other indicators of OSA. Likewise, no significant differences were observed in BMI, GOLD classification, PAP, LTOT, and diaphragm excursion during calm breathing between the two groups, despite overall improvements noted in AHI, mMRC, 6MWD, diaphragm excursion during deep breathing, and DTF following PR.
Our study revealed an overall FEV1%predicted value of 48.95±5.99 for the patient cohort, with responders demonstrating a significantly higher value (51.09±6.13) compared to non-responders (46.12±4.52). These results are in line with prior studies, indicating that individuals with elevated initial values of FEV1 or FEV1/FVC tend to have substantial enhancements in 6MWD following PR.14,38,39 Similarly, patients with milder mMRC scores also showed a better response to PR.34 However, some studies have reported contradictory findings12,13,40–42 or failed to identify any significant baseline characteristics for predicting PR response.43 The identification of predictors of response is therefore essential for ensuring the effectiveness and individualization of PR programs for patients diagnosed with COPD-OSA overlap syndrome.
The diaphragm, as the primary skeletal muscle involved in respiration, plays a crucial role by contributing to approximately 75% of the maximal tidal volume.44 The diaphragm may experience fatigue in patients with COPD-OSA overlap syndrome when they exert effort against upper airway obstruction, potentially impacting the occurrence of OSA. However, the effects of diaphragm function vary in different stages of the disorder.45 Dyspnea and limited exercise capacity are observed due to the impact of chronic obstructive pulmonary disease (COPD) on ventilator workload and inspiratory muscle strength, resulting from dynamic lung hyperinflation caused by diaphragm dysfunction.46 Although the pathophysiological mechanisms are complex, the exact contribution of the diaphragm to the pathophysiology of COPD-OSA overlap syndrome remains elusive, and its impact on rehabilitation is also unclear. Therefore, in this study, we employed ultrasound imaging, a relatively inexpensive and readily available technology, as a diagnostic tool to assess diaphragmatic dysfunction associated with COPD-OSA overlap syndrome, which is particularly important for evaluating the efficacy of PR.
A significant finding of this research is that DE during deep breathing and DTF at baseline were crucial predictors for identifying patients who responded positively to PR, specifically in terms of their 6MWD. The strong predictability of diaphragm movement may be attributed to its correlation with dynamic lung hyperinflation and exercise-induced breathlessness, as previously observed in patients with COPD.47 In a study by Shiraishi et al,20 DE max, reflecting the degree of dynamic lung hyperinflation and exercise-induced dyspnoea, was shown to be superior to other physiological indices. However, there have been limited studies on diaphragm function and morphology in patients with OSA. Pazarlı et al observed a positive correlation between the severity of OSAS and an augmented diaphragm thickness in patients with OSAS, while finding no significant difference in the thickness ratio compared to individuals without OSAS.48 Diaphragmatic exhaustion resulting from the exertion of inhaling against a blocked airway has also been suggested,49 in addition to diaphragm contractility and heightened pressure across the diaphragm.50,51 The development of dyspnea is predominantly influenced by dynamic lung hyperinflation, resulting in shortness of breath after activity, which is closely associated with the pathophysiology of COPD. Both dynamic pulmonary hyperinflation and dyspnea play role in determining the improvement of 6MWD in patients.
Moreover, the positive cycle observed in our PR program, which included moderate-intensity aerobic training, could potentially be attributed to enhanced respiratory patterns, even though certain patients utilized LTOT and PAP while exercising. The findings from studies on mechanically ventilated patients suggest that52 enhanced diaphragm function and morphology may facilitate the improvement of ventilation patterns. This could potentially result in decreased dyspnoea after a period of 12 weeks participating in PR, as well as an improvement in exercise capacity. Exercise therapy is a pivotal element of PR, exerting significant effects on the reduction of blood lactate levels, decrease in minute ventilation, and enhancement of exercise tolerance.53 The moderate-intensity aerobic exercise, which is performed at 50–70% of the peak oxygen uptake, elicits a greater physiological response compared to low-load exercise. Individuals with enhanced diaphragm excursion may demonstrate improved tolerance towards high-load exercise, thereby leading to more efficient PR.
The strength of our study lies in the finding that baseline lung function and diaphragm characteristics are key determinants of rehabilitation responders among patients with COPD-OSA overlap syndrome. Specifically, DE during deep breathing >3.61cm and DTF>17.26% predicted a significant improvement in exercise ability after PR. However, the present study is subject to certain limitations. The study was conducted at a single research center and had a relatively limited sample size, potentially leading to the preservation of participants’ baseline condition. Nevertheless, 50% of the patients had FEV1 < 50%, 43% were on LTOT, and 36% used PAP. Additionally, there is a lack of standardization in procedures pertaining to the selection of hemi-diaphragm, patient positioning, and breathing patterns, which poses challenges for the routine implementation of DE assessment. Standardizing these parameters would enhance the clinical and research utility of DE. Furthermore, we did not assess the impact of malnutrition factors or resistance training prescription, both of which are potentially significant determinants influencing diaphragmatic mobility. In future studies, attention should be given to strengthening nutrition, combining aerobic and resistance training, and establishing standardized evaluation criteria for PR.
Conclusion
We conclude that diaphragm excursion is a reliable and easily measurable parameter that can demonstrate its effectiveness in predicting the enhancement of exercise tolerance following PR in individuals with COPD-OSA overlap syndrome. Assessing diaphragm excursion may be valuable in guiding medical decisions pertaining to therapeutic approaches.
Data Sharing Statement
The datasets generated and/or analysed during the current study are available from the corresponding author upon reasonable request.
Ethical Statement
It has therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki (Revised in 2013). The study received approval from the Ethics Committee of The Fourth Rehabilitation Hospital of Shanghai (SP202002), and written informed consent was obtained from all participants. All methods were carried out in accordance with relevant guidelines and regulations.
Author Contributions
All authors have made significant contributions to the reported work, encompassing conception, study design, execution, data acquisition, analysis and interpretation. They have also participated in drafting, revising, or critically reviewing the article. Furthermore, they have provided final approval for the publication of this version and agreed upon its submission to the journal. Additionally, they acknowledge their accountability for all aspects of the work.
Funding
The National Natural Science Foundation of China (NSFC81770085, NSFC82070095). 2020 Jing’ an District Medical Research Project (face project 2020MS20).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Flenley DC. Sleep in chronic obstructive lung disease. Clinics Chest Med. 1985;6(4):651–661.
2. Toraldo DM, De Nuccio F, Nicolardi G. Fixed-pressure nCPAP in patients with obstructive sleep apnea (OSA) syndrome and chronic obstructive pulmonary disease (COPD): a 24-month follow-up study. Sleep Breath. 2010;14(2):115–123. doi:10.1007/s11325-009-0291-1
3. Zhang P, Chen B, Lou H, et al. Predictors and outcomes of obstructive sleep apnea in patients with chronic obstructive pulmonary disease in China. BMC Pulm Med. 2022;22(1):16. doi:10.1186/s12890-021-01780-4
4. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–582. doi:10.1164/rccm.201701-0218PP
5. Shawon MS, Perret JL, Senaratna CV, Lodge C, Hamilton GS, Dharmage SC. Current evidence on prevalence and clinical outcomes of co-morbid obstructive sleep apnea and chronic obstructive pulmonary disease: a systematic review. Sleep Med Rev. 2017;32:58–68. doi:10.1016/j.smrv.2016.02.007
6. Donovan LM, Feemster LC, Udris EM, et al. Poor outcomes among patients with chronic obstructive pulmonary disease with higher risk for undiagnosed obstructive sleep apnea in the LOTT cohort. J Clin Sleep Med. 2019;15(1):71–77. doi:10.5664/jcsm.7574
7. McNicholas WT. Chronic obstructive pulmonary disease and obstructive sleep apnea: overlaps in pathophysiology, systemic inflammation, and cardiovascular disease. Am J Respir Crit Care Med. 2009;180(8):692–700. doi:10.1164/rccm.200903-0347PP
8. Du W, Liu J, Zhou J, Ye D, OuYang Y, Deng Q. Obstructive sleep apnea, COPD, the overlap syndrome, and mortality: results from the 2005–2008 national health and nutrition examination survey. Int J Chronic Obstr. 2018;13:665–674. doi:10.2147/copd.S148735
9. Marin JM, Soriano JB, Carrizo SJ, Boldova A, Celli BR. Outcomes in patients with chronic obstructive pulmonary disease and obstructive sleep apnea: the overlap syndrome. Am J Respir Crit Care Med. 2010;182(3):325–331. doi:10.1164/rccm.200912-1869OC
10. Dong J, Li Z, Luo L, Xie H. Efficacy of pulmonary rehabilitation in improving the quality of life for patients with chronic obstructive pulmonary disease: evidence based on nineteen randomized controlled trials. Int j Surg. 2020;73:78–86. doi:10.1016/j.ijsu.2019.11.033
11. Spruit MA, Singh SJ, Garvey C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13–e64. doi:10.1164/rccm.201309-1634ST
12. Boutou AK, Tanner RJ, Lord VM, et al. An evaluation of factors associated with completion and benefit from pulmonary rehabilitation in COPD. BMJ Open Respir Res. 2014;1(1):e000051. doi:10.1136/bmjresp-2014-000051
13. Costi S, Crisafulli E, Trianni L, et al. Baseline exercise tolerance and perceived dyspnea to identify the ideal candidate to pulmonary rehabilitation: a risk chart in COPD patients. Int J Chronic Obstr. 2019;14:3017–3023. doi:10.2147/copd.S223038
14. van Ranst D, Otten H, Meijer JW, van ‘t Hul AJ. Outcome of pulmonary rehabilitation in COPD patients with severely impaired health status. Int J Chronic Obstr. 2011;6:647–657. doi:10.2147/copd.S24579
15. Pettiaux N, Cassart M, Paiva M, Estenne M. Three-dimensional reconstruction of human diaphragm with the use of spiral computed tomography. J Appl Physiol. 1997;82(3):998–1002. doi:10.1152/jappl.1997.82.3.998
16. Tian Y, Ma SL, Zhang YN, Shi L, Zhang WQ, Zhu XP. 慢性阻塞性肺疾病患者膈肌形态学的CT三维重建技术研究 [The morphological alteration of the diaphragm in patients with chronic obstructive pulmonary disease with three-dimensional reconstruction of 64-slice spiral CT]. Zhonghua Jie He He Hu Xi Za Zhi. 2013;36(2):94–99. Chinese.
17. McKenzie DK, Gorman RB, Tolman J, Pride NB, Gandevia SC. Estimation of diaphragm length in patients with severe chronic obstructive pulmonary disease. Respiration Physiol. 2000;123(3):225–234. doi:10.1016/s0034-5687(00)00172-9
18. Crimi C, Heffler E, Augelletti T, et al. Utility of ultrasound assessment of diaphragmatic function before and after pulmonary rehabilitation in COPD patients. Int J Chronic Obstr. 2018;13:3131–3139. doi:10.2147/copd.S171134
19. Xu Y, Yang D, Lu B, Zhang Y, Ren L, Shen H. Efficacy of aerobic training and resistance training combined with external diaphragm pacing in patients with chronic obstructive pulmonary disease: a randomized controlled study. Clin rehabilitat. 2023;2692155231172005. doi:10.1177/02692155231172005
20. Shiraishi M, Higashimoto Y, Sugiya R, et al. Diaphragmatic excursion is correlated with the improvement in exercise tolerance after pulmonary rehabilitation in patients with chronic obstructive pulmonary disease. Respir Res. 2021;22(1):271. doi:10.1186/s12931-021-01870-1
21. Global Initiative for Chronic Obstructive Lung Disease (GOLD) [EB/OL]. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease; 2021. Availbale from: http://www.goldcopd.org/.
22. Boussuges A, Gole Y, Blanc P. Diaphragmatic motion studied by m-mode ultrasonography: methods, reproducibility, and normal values. Chest. 2009;135(2):391–400. doi:10.1378/chest.08-1541
23. Testa A, Soldati G, Giannuzzi R, Berardi S, Portale G, Gentiloni Silveri N. Ultrasound M-mode assessment of diaphragmatic kinetics by anterior transverse scanning in healthy subjects. Ultrasound Med Biol. 2011;37(1):44–52. doi:10.1016/j.ultrasmedbio.2010.10.004
24. Berry RB, Brooks R, Gamaldo CE. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology, and Technical Specifications, Version 2.3. Darien, IL, USA: American Academy of Sleep Medicine; 2016.
25. Berry RB, Budhiraja R, Gottlieb DJ, et al. Rules for scoring respiratory events in sleep: update of the 2007 AASM manual for the scoring of sleep and associated events. Deliberations of the sleep apnea definitions task force of the American Academy of Sleep Medicine. J Clin Sleep Med. 2012;8(5):597–619. doi:10.5664/jcsm.2172
26. Mahler DA, Wells CK. Evaluation of clinical methods for rating dyspnea. Chest. 1988;93(3):580–586. doi:10.1378/chest.93.3.580
27. ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111–117. doi:10.1164/ajrccm.166.1.at1102
28. Holland AE, Spruit MA, Troosters T, et al. An official European Respiratory Society/American Thoracic Society technical standard: field walking tests in chronic respiratory disease. Europ resp J. 2014;44(6):1428–1446. doi:10.1183/09031936.00150314
29. Singh SJ, Puhan MA, Andrianopoulos V, et al. An official systematic review of the European Respiratory Society/American Thoracic Society: measurement properties of field walking tests in chronic respiratory disease. Europ resp J. 2014;44(6):1447–1478. doi:10.1183/09031936.00150414
30. Polkey MI, Spruit MA, Edwards LD, et al. Six-minute-walk test in chronic obstructive pulmonary disease: minimal clinically important difference for death or hospitalization. Am J Respir Crit Care Med. 2013;187(4):382–386. doi:10.1164/rccm.201209-1596OC
31. Morris NR, Walsh J, Adams L, Alision J. Exercise training in COPD: what is it about intensity? Respirology. 2016;21(7):1185–1192. doi:10.1111/resp.12864
32. He GX, Li N, Ren L, et al. Benefits of different intensities of pulmonary rehabilitation for patients with moderate-to-severe COPD according to the GOLD stage: a prospective, multicenter, single-blinded, randomized, controlled trial. Int J Chronic Obstr. 2019;14:2291–2304. doi:10.2147/copd.S214836
33. Lacasse Y, Goldstein R, Lasserson TJ, Martin S. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2006;4:Cd003793. doi:10.1002/14651858.CD003793.pub2
34. Garrod R, Marshall J, Barley E, Jones PW. Predictors of success and failure in pulmonary rehabilitation. Europ resp J. 2006;27(4):788–794. doi:10.1183/09031936.06.00130605
35. Spruit MA, Gosselink R, Troosters T, Kasran A, Van Vliet M, Decramer M. Low-grade systemic inflammation and the response to exercise training in patients with advanced COPD. Chest. 2005;128(5):3183–3190. doi:10.1378/chest.128.5.3183
36. de Torres JP, Pinto-Plata V, Ingenito E, et al. Power of outcome measurements to detect clinically significant changes in pulmonary rehabilitation of patients with COPD. Chest. 2002;121(4):1092–1098. doi:10.1378/chest.121.4.1092
37. Troosters T, Gosselink R, Decramer M. Exercise training in COPD: how to distinguish responders from nonresponders. J Cardiopulmonary Rehabil. 2001;21(1):10–17. doi:10.1097/00008483-200101000-00004
38. Vagaggini B, Costa F, Antonelli S, et al. Clinical predictors of the efficacy of a pulmonary rehabilitation programme in patients with COPD. Respir Med. 2009;103(8):1224–1230. doi:10.1016/j.rmed.2009.01.023
39. Scott AS, Baltzan MA, Fox J, Wolkove N. Success in pulmonary rehabilitation in patients with chronic obstructive pulmonary disease. Can Respir J. 2010;17(5):219–223. doi:10.1155/2010/203236
40. Crisafulli E, Gorgone P, Vagaggini B, et al. Efficacy of standard rehabilitation in COPD outpatients with comorbidities. Europ resp J. 2010;36(5):1042–1048. doi:10.1183/09031936.00203809
41. Zanini A, Chetta A, Gumiero F, et al. Six-minute walking distance improvement after pulmonary rehabilitation is associated with baseline lung function in complex COPD patients: a retrospective study. Biomed Res Int. 2013;2013:483162. doi:10.1155/2013/483162
42. Ragaselvi S, Janmeja AK, Aggarwal D, Sidana A, Sood P. Predictors of response to pulmonary rehabilitation in stable chronic obstructive pulmonary disease patients: a prospective cohort study. J Postgraduate Med. 2019;65(2):101–106. doi:10.4103/jpgm.JPGM_433_18
43. Selzler AM, Simmonds L, Rodgers WM, Wong EY, Stickland MK. Pulmonary rehabilitation in chronic obstructive pulmonary disease: predictors of program completion and success. COPD. 2012;9(5):538–545. doi:10.3109/15412555.2012.705365
44. Gerscovich EO, Cronan M, McGahan JP, Jain K, Jones CD, McDonald C. Ultrasonographic evaluation of diaphragmatic motion. J Ultrasound Med. 2001;20(6):597–604. doi:10.7863/jum.2001.20.6.597
45. Kerl J, Noeke P, Heyse D, Dellweg D. Normal and obstructive breathing physiology during sleep. Sleep Breath. 2021;25(3):1335–1341. doi:10.1007/s11325-020-02217-8
46. Gagnon P, Guenette JA, Langer D, et al. Pathogenesis of hyperinflation in chronic obstructive pulmonary disease. Int J Chronic Obstr. 2014;9:187–201. doi:10.2147/copd.S38934
47. Shiraishi M, Higashimoto Y, Sugiya R, et al. Diaphragmatic excursion correlates with exercise capacity and dynamic hyperinflation in COPD patients. ERJ Open Res. 2020;6(4):00589–2020. doi:10.1183/23120541.00589-2020
48. Pazarlı AC, Özmen Z, Inönü Köseoğlu H, Ekiz T. Ultrasonographic measurement of the diaphragm thickness in patients with obstructive sleep apnea syndrome. Sleep Breath. 2020;24(1):89–94. doi:10.1007/s11325-019-01931-2
49. Matziaras G, Vlami K, Antaraki A, et al. Ultrasound evaluation of diaphragmatic function in obstructive sleep apnea. Europ Resp J. 2011;38(55):2219.
50. El-Kabir DR, Polkey MI, Lyall RA, Williams AJ, Moxham J. The effect of treatment on diaphragm contractility in obstructive sleep apnea syndrome. Respir Med. 2003;97(9):1021–1026. doi:10.1016/s0954-6111(03)00132-x
51. Wilcox PG, Paré PD, Road JD, Fleetham JA. Respiratory muscle function during obstructive sleep apnea. Am Rev Respir Dis. 1990;142(3):533–539. doi:10.1164/ajrccm/142.3.533
52. Li C, Li X, Han H, Cui H, Wang G, Wang Z. Diaphragmatic ultrasonography for predicting ventilator weaning: a meta-analysis. Medicine. 2018;97(22):e10968. doi:10.1097/md.0000000000010968
53. Rabinovich RA, Ardite E, Troosters T, et al. Reduced muscle redox capacity after endurance training in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;164(7):1114–1118. doi:10.1164/ajrccm.164.7.2103065
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.