")
Back to Journals » Clinical Interventions in Aging » Volume 19
Correlation Between Anesthesia Methods and Adverse Short-Term Postoperative Outcomes Depending on Frailty: A Prospective Cohort Study
Authors Feng Y, Sun JF, Wei HC, Cao Y, Yao L, Du BX
Received 4 December 2023
Accepted for publication 28 March 2024
Published 16 April 2024 Volume 2024:19 Pages 613—626
DOI https://doi.org/10.2147/CIA.S448898
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Yan Feng,* Jia-Feng Sun,* Hai-Chao Wei,* Ying Cao, Lei Yao, Bo-Xiang Du
The Affiliated Hospital 2 of Nantong University, Nantong City, Jiangsu Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bo-Xiang Du; Lei Yao, Email [email protected]; [email protected]
Purpose: This study aims to investigate how the type of anesthesia used during major orthopedic surgery may impact adverse short-term postoperative outcomes depending on frailty.
Methods: To conduct this investigation, we recruited individuals aged 65 years and older who underwent major orthopedic surgery between March 2022 and April 2023 at a single institution. We utilized the FRAIL scale to evaluate frailty. The primary focus was on occurrences of death or the inability to walk 60 days after the surgery. Secondary measures included death within 60 days; inability to walk without human assistance at 60 days; death or the inability to walk without human assistance at 30 days after surgery, the first time out of bed after surgery, postoperative blood transfusion, length of hospital stay, hospital costs, and the occurrence of surgical complications such as dislocation, periprosthetic fracture, infection, reoperation, wound complications/hematoma.
Results: In a study of 387 old adult patients who had undergone major orthopedic surgery, 41.3% were found to be in a frail state. Among these patients, 262 had general anesthesia and 125 had neuraxial anesthesia. Multifactorial logistic regression analyses showed that anesthesia type was not linked to complications. Instead, frailty (OR 4.04, 95% CI 1.04 to 8.57, P< 0.001), age (OR 1.05, 95% CI 1.00– 1.10, P= 0.017), and aCCI scores, age-adjusted Charlson Comorbidity Index, (OR 1.36, 95% CI 1.12 to 1.66, P= 0.002) were identified as independent risk factors for death or new walking disorders in these patients 60 days after surgery. After adjusting for frailty, anesthesia methods was not associated with the development of death or new walking disorders in these patients (P > 0.05).
Conclusion: In different frail populations, neuraxial anesthesia is likely to be comparable to general anesthesia in terms of the incidence of short-term postoperative adverse outcomes.
Keywords: anesthesia, frailty, major orthopedic surgery, death, impaired walking ability
Introduction
Major orthopedic surgery is defined as total hip replacement (THR), total knee replacement (TKR), and hip fractures surgery (HFS).1 With the advancement of medical technology and aging population, the number of old adult patients undergoing major orthopedic surgeries is increasing, and the risk of postoperative adverse outcomes and mortality rate is increased in older patients compared to younger patients.2,3 Therefore, accurate preoperative risk assessment is essential.
Patients undergoing major orthopedic surgery may be advised to receive either general anesthesia or neuraxial anesthesia (such as spinal or epidural anesthesia) during their surgical procedure. Cement placement syndrome4 is a frequent complication in patients undergoing total hip replacement surgery. Anesthesia-related complications include tourniquet reaction,5 spinal cord injury,6 and commonly, postoperative nausea, vomiting,7 and urinary retention.8 There remains debate on the most suitable anesthesia type for major orthopedic surgery patients.
In many past studies9–12 it was concluded that neuraxial anesthesia is superior to general anesthesia for major orthopedic surgery, neuraxial anesthesia is associated with lower mortality and shorter hospital stays. A comprehensive study13 has determined that frailty is a crucial indicator for negative consequences subsequent to THA and TKA, and the utilization of neuraxial anesthesia in the case of vulnerable patients is linked with increased survival rates and reduced instances of wound complications. The assessment of recovery from surgery for orthopedic patients should not be solely based on mortality rates. Patients and their families are primarily concerned with the recovery of ambulation after surgery. Therefore, it is imperative to delve deeper into the risk factors associated with postoperative ambulation disorders. A randomized controlled study14 has advocated for there was no significant difference in the survival and ambulation recovery at 60 days between older adults undergoing hip-fracture surgery under neuraxial anesthesia and general anesthesia. Recent studies15 have also found that neuraxial anesthesia neither reduces mortality nor decreases delirium or increases the percentage of people who can walk at 60 days.
Old adult patients frequently experience the coexistence of multiple systemic diseases in their daily lives, including cardiovascular, respiratory, and digestive conditions. Consequently, this subgroup of old adult patients often finds themselves in a frail state. Frailty is a state marked by the depletion of biological reserves in various organ systems, breakdown of homoeostatic mechanisms, and susceptibility to physiological decompensation following minor stressor occurrences.16 The prevalence of frailty among older adults living in the community varies from 3.6% to 42.7%.17,18 Several systematic reviews and meta-analyses19–21 have advocated for frailty in the older population predicts may be associated with adverse outcomes such as higher risk of mortality, complications, prolonged length of stay and the loss of independence after surgery. In patients undergoing elective surgical procedures, frailty might provide a more precise portrayal of genuine biological age and perioperative vulnerability. The relationship between frailty and the recovery of the ability to walk after surgery is not clearly understood. It is also unclear whether the use of different anesthesia modalities for different frail individuals has any impact on their ability to walk after surgery.
The objective of this study was to investigate if the correlation between the level of preoperative frailty and the primary outcome of death or inability to walk without human assistance at 60 days after major orthopedic surgery differs based on the type of anesthesia used.
Accordingly, we predicted that the utilization of neuraxial anesthesia would lead to a lower occurrence of death or inability to walk without human assistance at 60 days after the surgery and that the impact of the anesthesia type on the outcome would differ depending on the level of frailty.
Methods
Study Design, Setting and Participants
This study followed the Declaration of Helsinki during the research process. Ethical approval for this study (2021KT082) was provided by the Ethical Committee of Nantong First Hospital on 30 June 2021.
It was registered with the Chinese Clinical Trials Registry (ChiCTR2100052088, https://www.chictr.org.cn/showproj.html?proj=134678)before any patient enrollment. All participants provided written informed consent before enrollment. This prospective cohort study encompassed individuals who underwent surgical procedures including total hip arthroplasty (THA), total knee arthroplasty (TKA) (primary or revision), or hip fracture (HF) repair. The study population consisted of patients who underwent initial surgery for total hip and total knee replacements. Specific types of hip fractures included internal fixation of femoral neck, intertrochanteric, and subtrochanteric fractures.
The study enlisted patients aged 65 years or above who could stroll independently for about 10 ft (3m) or throughout a room without reliance on external assistance before the surgery. Patients were excluded from the study if they had contraindications to neuraxial anesthesia, such as coagulation disorders, use of anticoagulant or antiplatelet agents, critical or severe aortic stenosis, high risk of infection at the site of insertion of the spinal needle, or increased intracranial pressure. Additionally, patients with a combination of spinal, craniofacial, and multiple rib fractures, multiple injuries of the internal organs, or sepsis and surgical site infection were also excluded. Those who had previously participated in the trial or refused to participate were not eligible.
Variables, Data Sources and Measurements
Characteristics of patients such as included age, sex, body mass index (BMI), hypertension, diabetes, current smoker, days of hospitalization before surgery and hospital length of stay were obtained from the e-case on the day of admission. Blood indices were routinely collected from venous blood samples taken by orthopedic nurses on the day of admission and analyzed in the laboratory. Surgery-related variables were consistently recorded by anesthesia specialists. To document the postoperative period, two physicians, who were unaware of the anesthesia and frailty subgroups, primarily followed up with patients by telephone to record their recovery.
All included patients were required to complete preoperative frailty assessment based on the FRAIL scale was conducted by a specially trained anesthesiologist on the admission day. Based on a comprehensive review of numerous literature sources and clinical practice experiences,22–25 additional common confounders were identified and gathered for analysis. These include: (1) patients’ underlying disease conditions, as measured by the age-adjusted Charlson comorbidity index (aCCI) score;26 (2) blood indices such as hemoglobin and albumin; and (3) surgery-related variables including ASA classification, duration of surgery, type of surgery, mode of anesthesia, and intraoperative blood transfusion. The aCCI score was assessed on the day of admission by an anesthesiologist specializing in evaluating debility.
The FRAIL Scale,27 a widely used assessment tool for clinical frailty, was proposed by the International Society for Geriatric Nutrition. It comprises 5 components: (1) Fatigue: experiencing fatigue and weakness persistently over the past 4 weeks; (2) Reduced endurance/increased resistance: facing difficulty in ascending a single flight of stairs without any breaks or external support; (3) Restricted mobility: encountering challenges while walking a distance of 1 block (equivalent to 100m) unaccompanied and without any aid; (4) Disease burden: affected by 5 or more of the following diseases – malignant tumors, hypertension, heart failure, kidney disease, diabetes mellitus, angina pectoris, stroke, arthritis, asthma, and chronic lung disease, among others; (5) Weight loss: experiencing a weight reduction of beyond 5% of the previous year’s body weight within a span of 1 year. A diagnosis of “Frail” is given when 3 or more of these 5 items are present, while “Vulnerable” applies to individuals with 1 to 2 items, and “Non-frail” for those scoring 0 on the scale.
Anesthesia Procedures
In the decision-making process for anesthesia, multiple parties, including the anesthesiologist, treating clinicians, and the patient, play significant roles. When it comes to neuraxial anesthesia, the anesthesiologist conducts a standard puncture in the intrathecal area, adjusts sedation levels appropriately, and administers a specific dosage of sedative to alleviate the patient’s nervousness and anxiety. This approach guarantees that the patient maintains an intraoperative sedation score within the range of 5 to 2, as evaluated by the RASS scale.28 In circumstances where patients undergo general anesthesia, adherence to the established protocol is essential for choosing the appropriate anesthetic drugs and managing the airway effectively.
Outcomes
The primary measure was the occurrence of death or inability to walk 60 days after surgery. Gait impairment was defined as the inability to walk 10 feet without the assistance of a walker or cane, or to walk across a room without assistance. Secondary measures included death within 60 days; inability to walk without human assistance at 60 days; death or inability to walk without human assistance at 30 days after surgery, first time out of bed after surgery, postoperative blood transfusion, days of hospitalization, hospital fees, and the occurrence of surgical complications within 60 days after surgery. Surgical complications13 such as dislocation, periprosthetic fracture, infection, reoperation, wound complications/hematoma, and mortality were also documented. Surgical complications were diagnosed and documented by the orthopedic surgeon. Other relevant indicators were determined by analyzing medical records and prescription systems.
Sample Size Calculation
Based on previous studies,29 the occurrence of impaired ambulation and mortality combined was found to be around 34.2% after 60 days of surgery in hip fracture patients who received general anesthesia. A significant reduction of 50% in the occurrence of this combined outcome was considered statistically meaningful. With a significance level of 0.05, a confidence level of 80%, and a dropout rate of 10%, the initial calculations determined that a sample size of 152 patients in the general anesthesia group and 76 patients in the neuraxial anesthesia group would be required.
Statistical Analysis
SPSS version 26.0 (IBM Corporation, Armonk, NY, USA) was used for statistical analysis. Normality of data was assessed. Means (SD) or medians (25th percentile, 75th percentile) and proportions (n/%) were calculated for baseline characteristics according to the frailty groups and the anesthesia groups. Kolmogorov–Smirnov test was used for determining whether variables were normally distributed. A comparison of the variables between groups was performed by using the independent samples t-test, group f-test or Mann–Whitney U-test with regard to the normality of distribution. The chi-square test (Fisher’s exact test) for categorical variables were applied to compare the characteristics of the study subjects among the frailty groups and the anesthesia groups. Indicators with statistically significant differences in the univariate analysis were included in a multifactor logistic regression model to screen for independent risk factors for the occurrence of adverse outcomes. The predictive value was analyzed by receiver operating characteristic (ROC) curve, and the area under the curve (AUC) was calculated. P<0.05was considered as statistically significant difference. To analyze the interaction between FRAIL and anesthesia type on outcomes, one multivariable model was fit for each outcome. Each model included FRAIL and anesthesia type. A two- sided overall P < 0.10 was determined to be significant for the interactions. To better illustrate the effects of the interaction, we presented ORs for neuraxial block relative to general anesthesia in subsets for the non-frail, vulnerable, and frail patients.
Flow Chart
Between March 1, 2022, and April 30, 2023, a total of 502 patients were treated for major orthopedic surgery. Of these, 74 were excluded because they did not meet the age limit of 65 years, 8 were unable to walk independently for 3 meters or across a room before hospitalization, 8 had a combination of other traumatic injuries, and 2 refused to participate. Thus, there were a total of 410 participants. When telephone follow-up was performed 60 days after surgery, 23 patients were excluded because they were out of contact or refused follow-up, and 387 were ultimately included in the initial analysis (Figure 1).
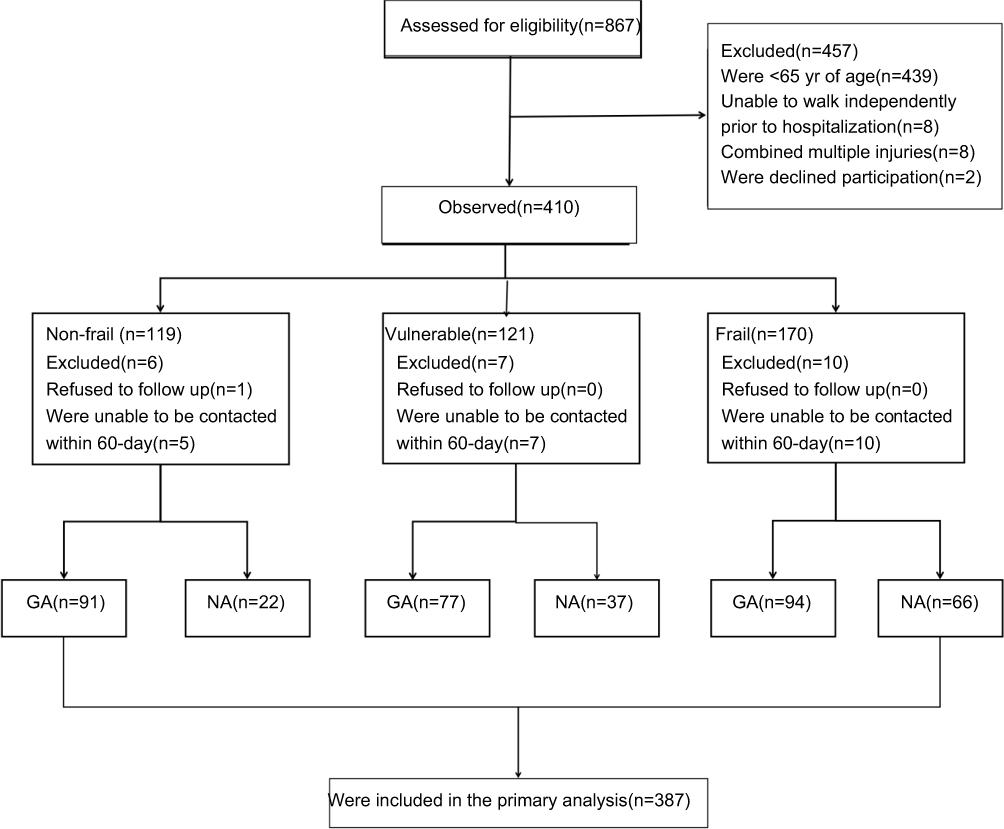 |
Figure 1 Flow chart of the selection process. Abbreviations: GA, general anesthesia; NA, Neuraxial anesthesia. |
Results
Analysis of General Information
When comparing different types of anesthesia (Table 1,P < 0.05), it was observed that patients undergoing neural anesthesia were generally older, had lower BMI, lower levels of albumin and hemoglobin, and had ASA physical fitness status III or IV. These patients also underwent shorter procedures. Frail and vulnerable patients, who are typically older with an ASA physical status of III or IV, required longer surgical procedures compared to non-frail patients. Furthermore, patients classified as frail and vulnerable showed an increased use of neuraxial anesthesia with increasing frailty, as shown in Table 2 (P<0.05).
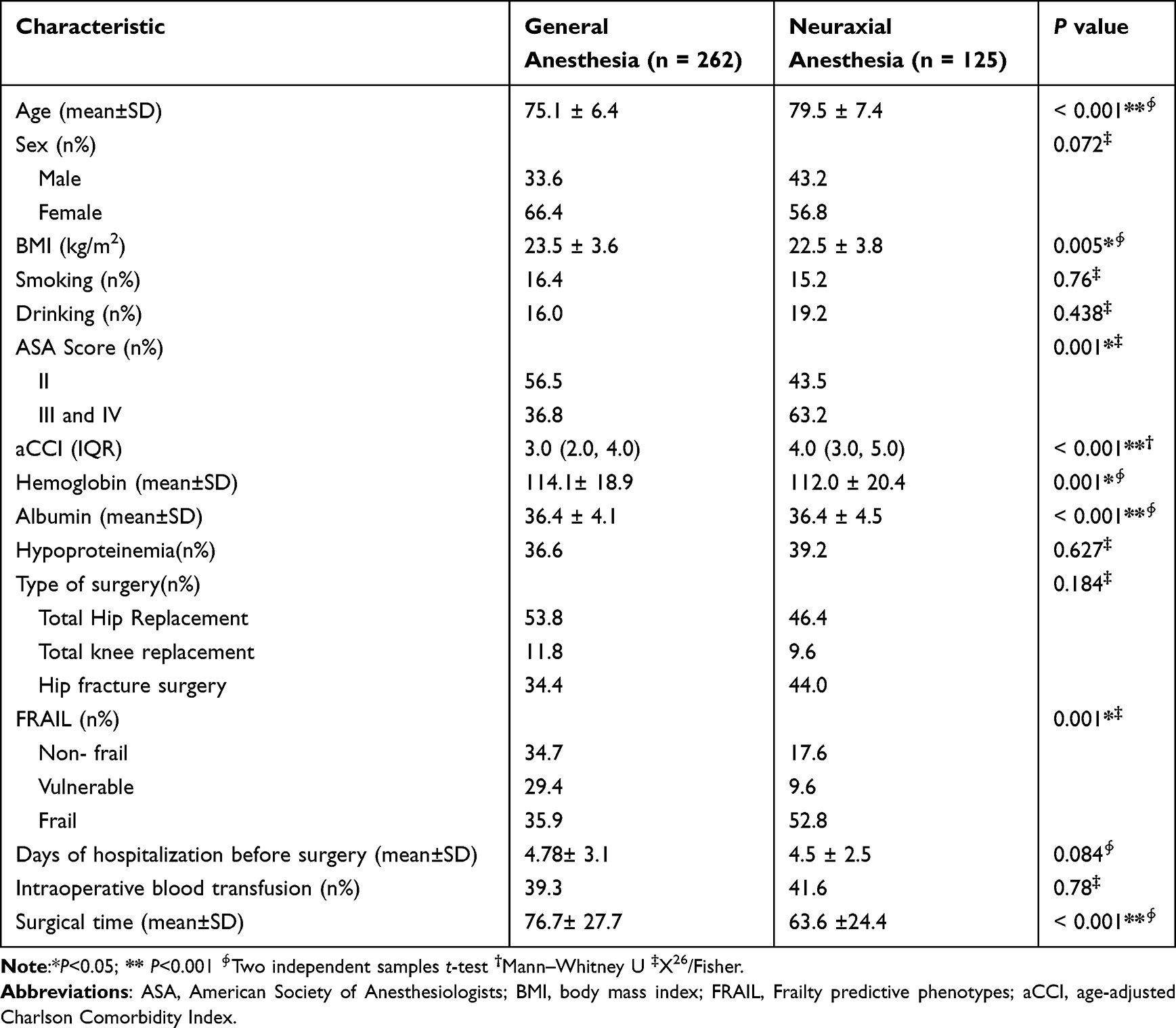 |
Table 1 Patient Demographics and Clinical Characteristics by Anesthesia Type |
 |
Table 2 Patient Demographics and Clinical Characteristics by Categorized Frailty |
Analysis of the Correlation Between Frailty/Anesthesia Modalities and Adverse Outcomes
- Impact of choice of anesthesia methods on outcomes within the overall population
Among old adult patients undergoing major orthopedic surgery, those receiving neuraxial anesthesia had a higher incidence of death or new inability to ambulate within 60 days after surgery compared with those receiving general anesthesia (Table 3,P=0.011).
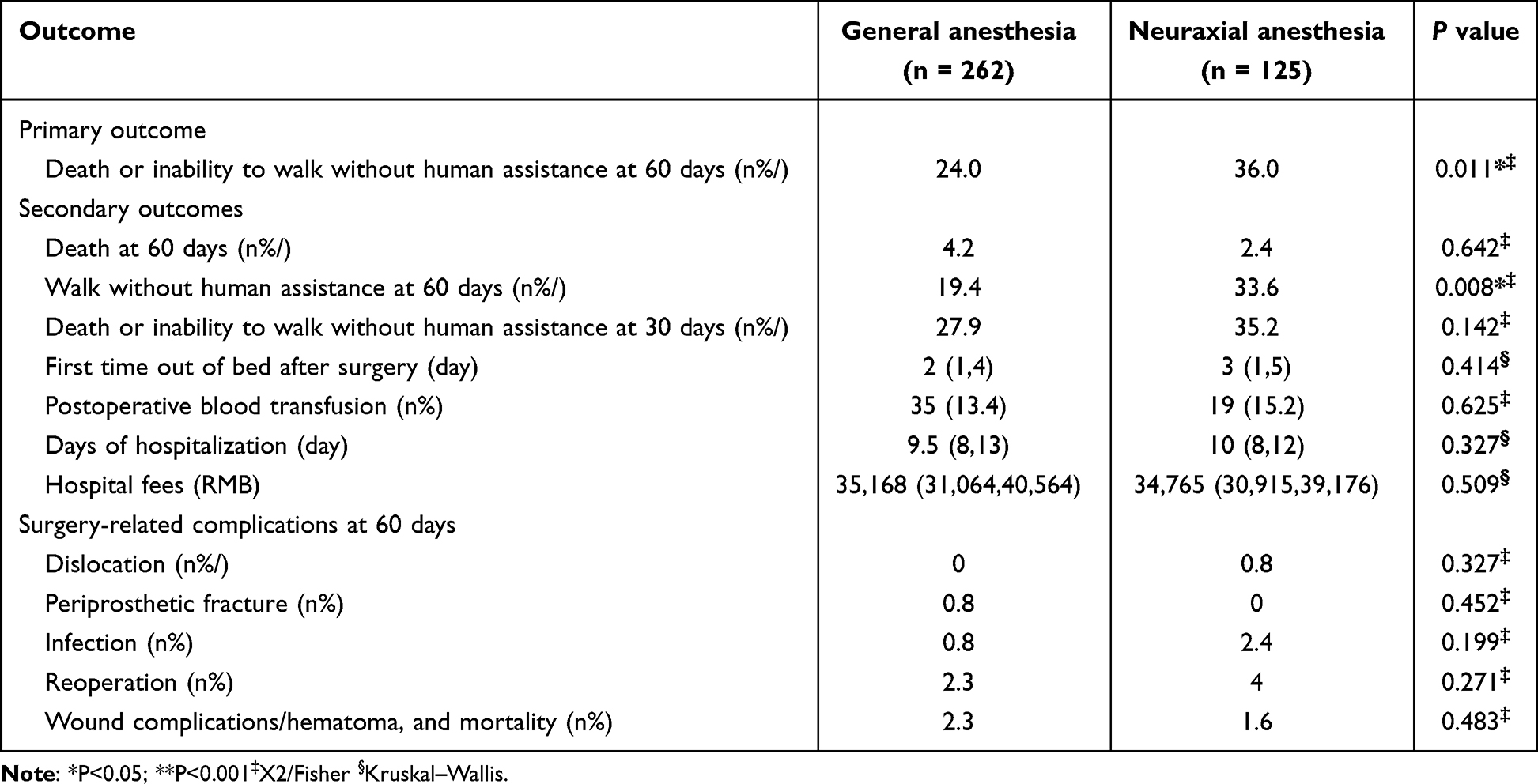 |
Table 3 Primary Outcome and Prespecified Secondary Outcomes by Categorized Anesthesia Type |
The incidence of new inability to ambulate within 60 days after surgery was higher in patients who received neuraxial anesthesia, while death at 60 days postoperatively was higher in patients who received general anesthesia (Table 3,P<0.05). There were no significant differences in other secondary outcomes between the two groups (Table 3,P>0.05).
(2) Impact of frailty on outcomes within the overall population
Seventy patients in the frail group experienced death or ambulation disorders 60d postoperatively, which was significantly higher than the remaining two groups. Additionally, death rates were found to be higher in vulnerable patients compared to non-frail and frail patients, with frail patients showing poorer recovery of postoperative ambulation (Table 4, P<0.05). The rates of death or ambulation disorder at 30d postoperatively, postoperative blood transfusion rate, number of days in hospital, hospitalization cost, rate of surgical site infection, reoperation, and wound oozing and hematoma in the debilitated group were all higher than those in the remaining two groups (Table 4,P<0.05).
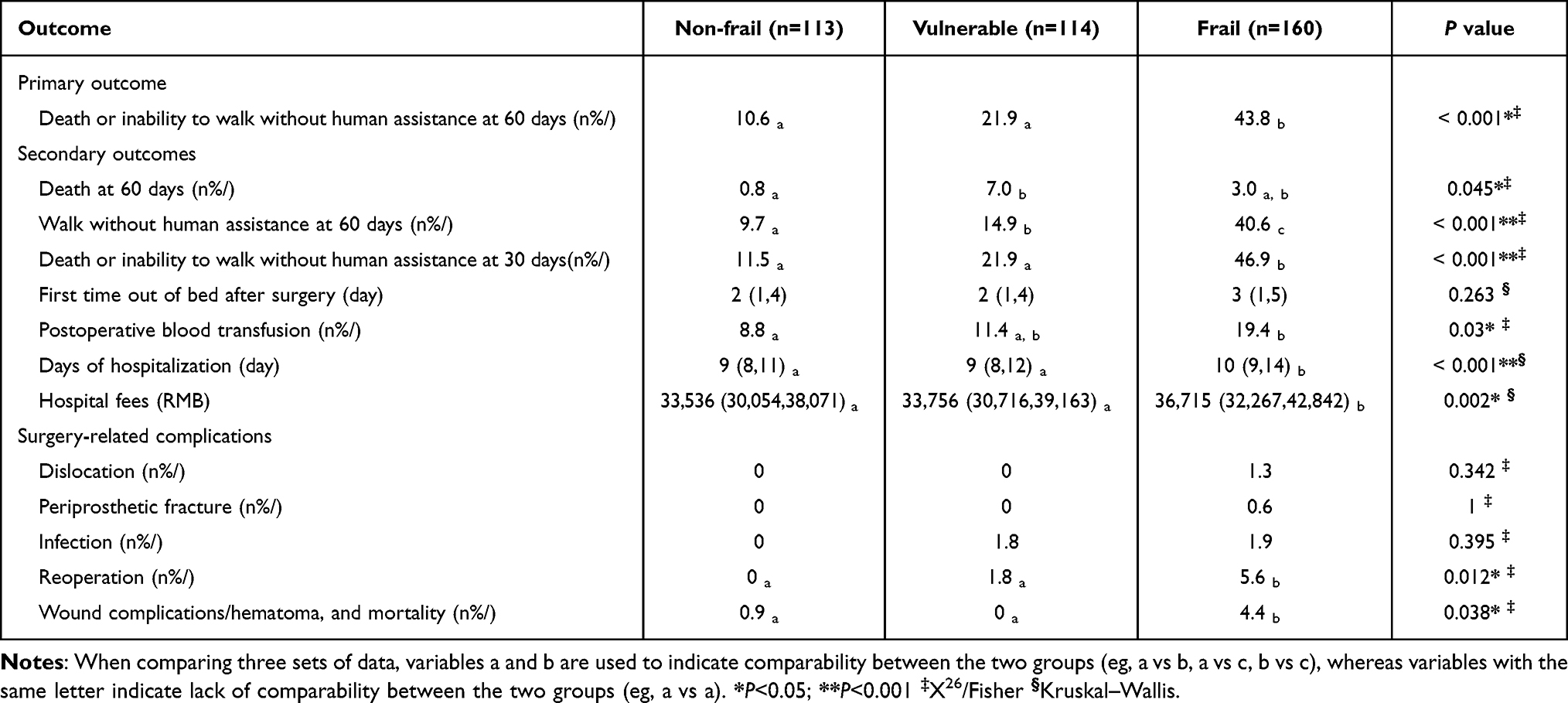 |
Table 4 Primary Outcome and Prespecified Secondary Outcomes by Categorized Frailty |
Screening for Risk Factors for Primary Outcomes
- Single-factor and multifactor logistic regression models
Indicators with correlation with the occurrence of death or ambulation disorder at 60d postoperatively were screened by univariate logistic regression analysis, and after incorporating multivariate logistic regression analysis, the results showed that preoperative debilitating state was associated with the occurrence of death or ambulation disorder at 60d postoperatively (OR 4.04, 95% CI 1.04~8.57,P<0.001). It was also found that increasing age (OR 1.05, 95% CI 1.00–1.10, P=0.017) and increasing preoperative aCCI score (OR 1.36, 95% CI 1.12~1.66, P=0.002) were risk factors for the occurrence of death or impaired walking at 60d postoperatively (Table 5).
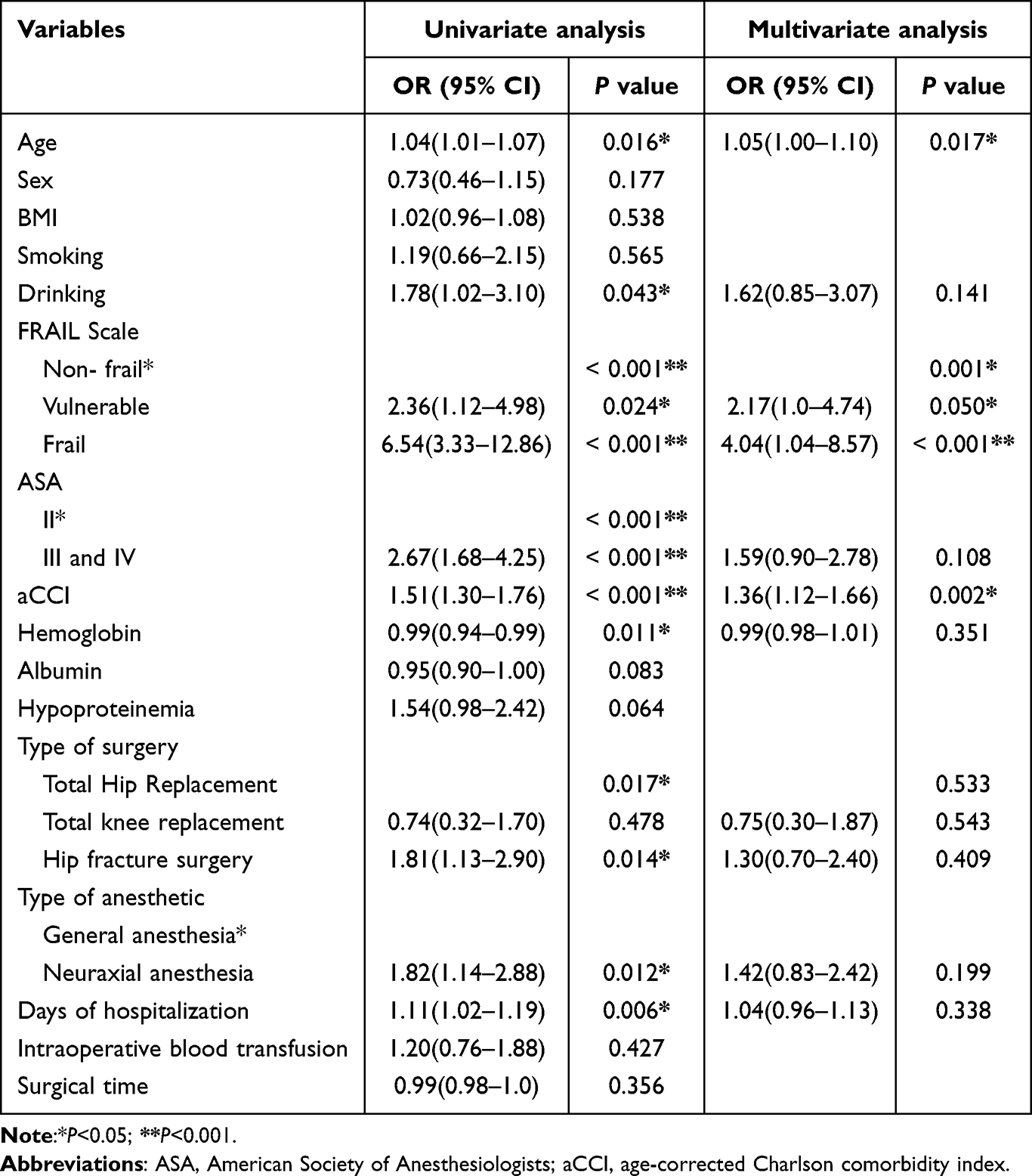 |
Table 5 Binary Logistic Regression Analysis of Outcome Risk Factors for Death or a New Inability to Walk 60 Days Postoperatively |
(2) ROC curve
The area under the ROC curve for preoperative debilitation status predicting the occurrence of death or ambulation impairment at 60 d postoperatively was 0.691, with a sensitivity of 65.4% and a specificity of 67.9% (Table 6, Figure 2).
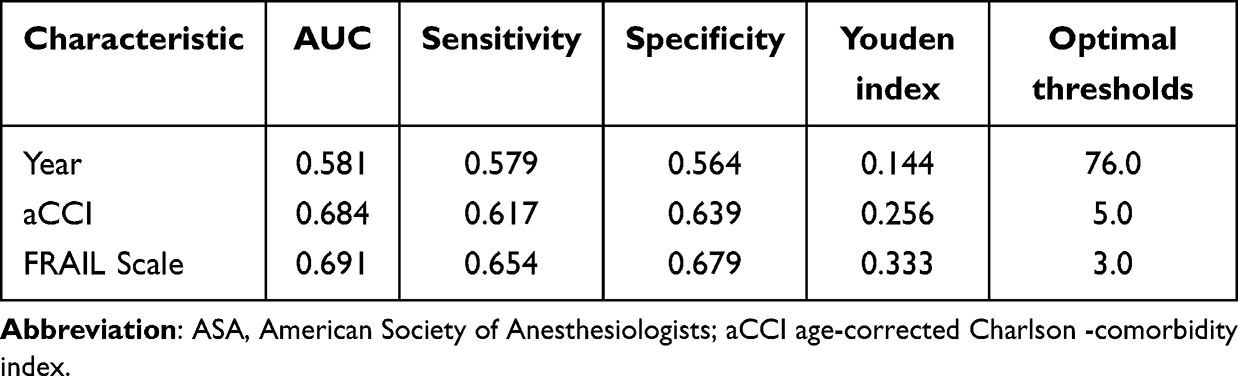 |
Table 6 Preoperative Debilitating Status, Age, and aCCI Score Predicted Death or Impaired Ambulation at 60d Postoperatively |
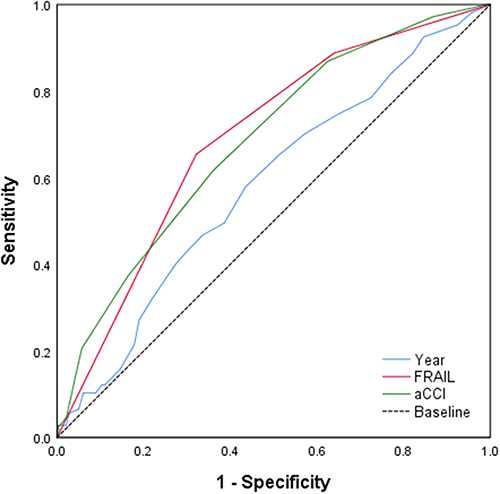 |
Figure 2 ROC curves for age, preoperative frailty and aCCI predicting death or a new inability to walk 60 days. |
(3) Multivariate stratified regression models predicting death or impaired ambulation within 60 days after surgery
Results indicated that patients with hip fractures exhibited higher frailty levels and increased risk of death or impaired ambulation 60 days post-surgery compared to those undergoing hip replacement surgery (Table 7, P=0.02). However, upon integrating frailty into the model, no significant correlation was found between surgery type and the occurrence of death or impaired mobility at the 60 days mark postoperatively (Table 8, P>0.05).
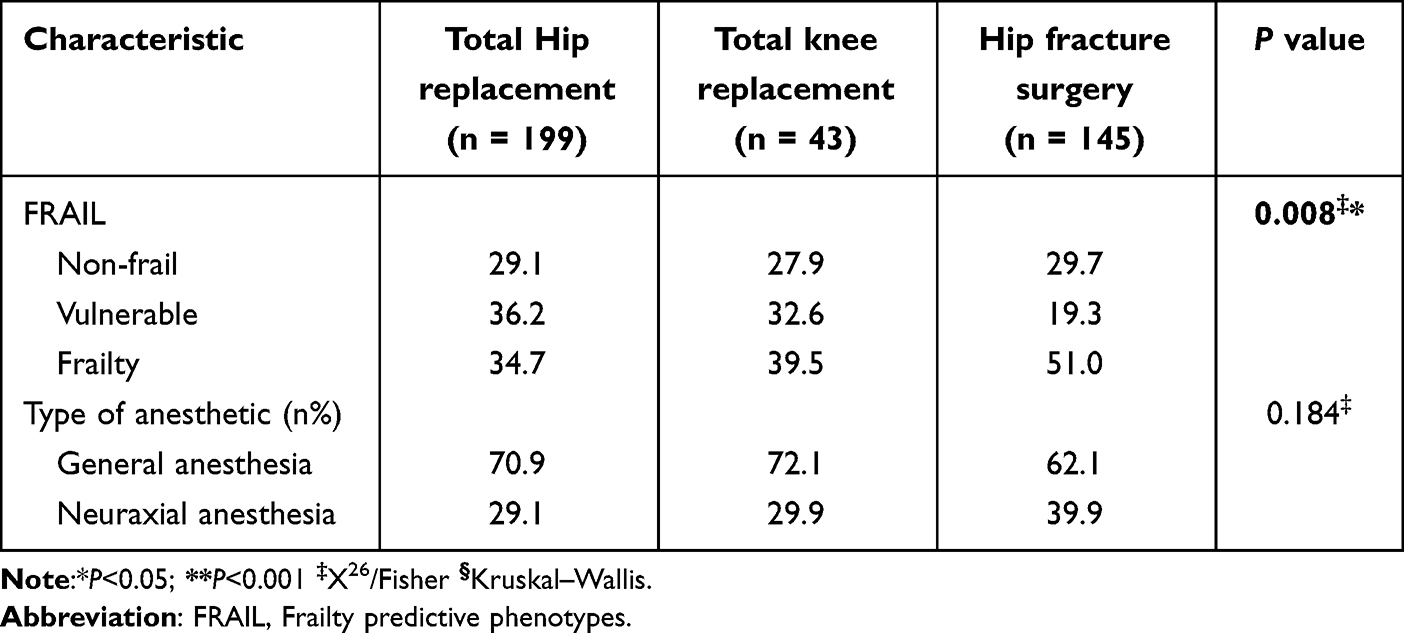 |
Table 7 Patient Stratification of Debilitation and Anesthesia Methods by Type of Surgery |
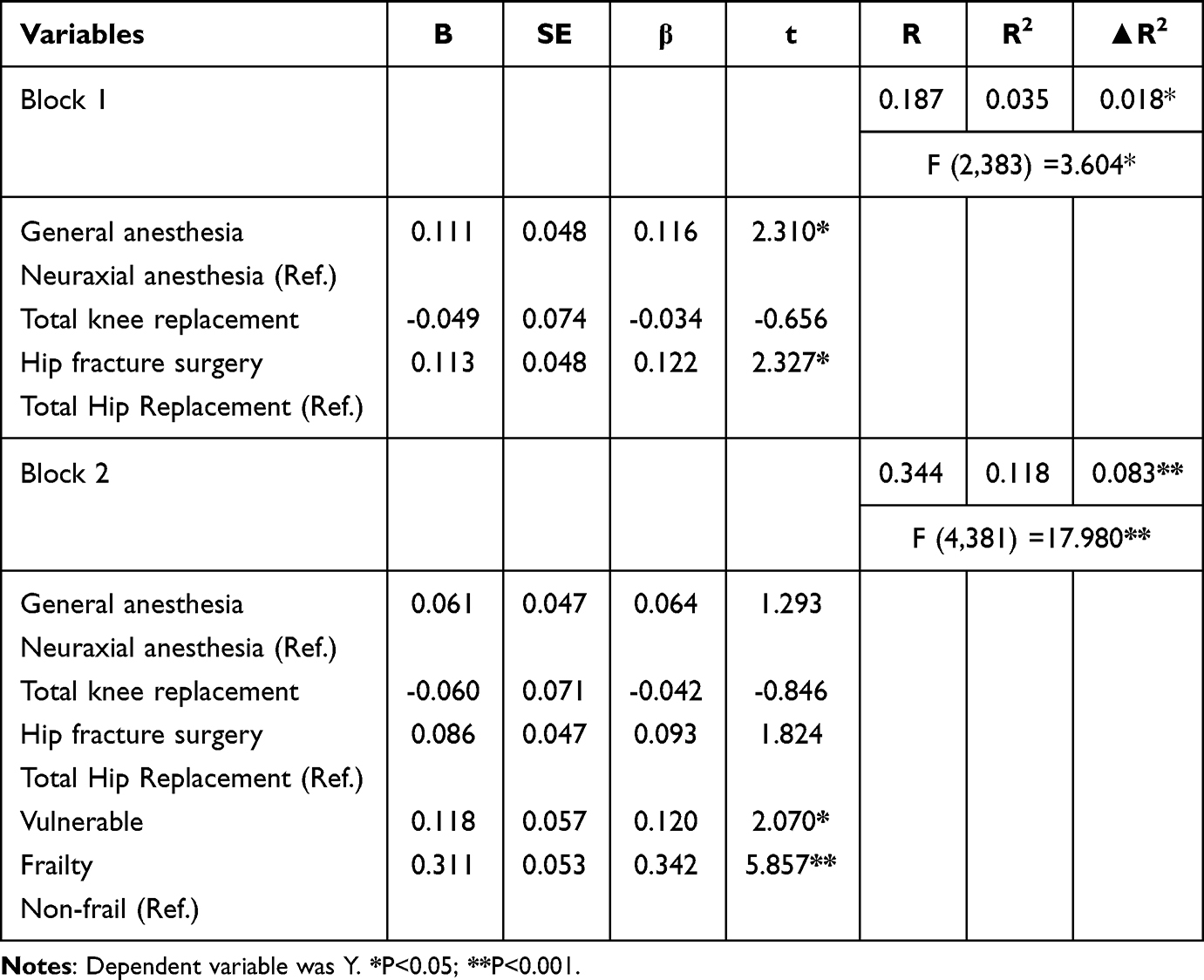 |
Table 8 Multivariate stratified regression models predicting death or impaired ambulation within 60 days after surgery |
(4) Impact of choice of anesthesia methods on adverse outcomes depending on frailty
The choice of anesthesia method does not seem to independently increase the risk of death or impaired ambulation 60 days after surgery, as shown in Table 5. Upon analyzing the baseline data, it was observed that the type of anesthesia used was associated with the frailty. An interaction analysis was conducted between the anesthesia method and frailty (Figure 3).
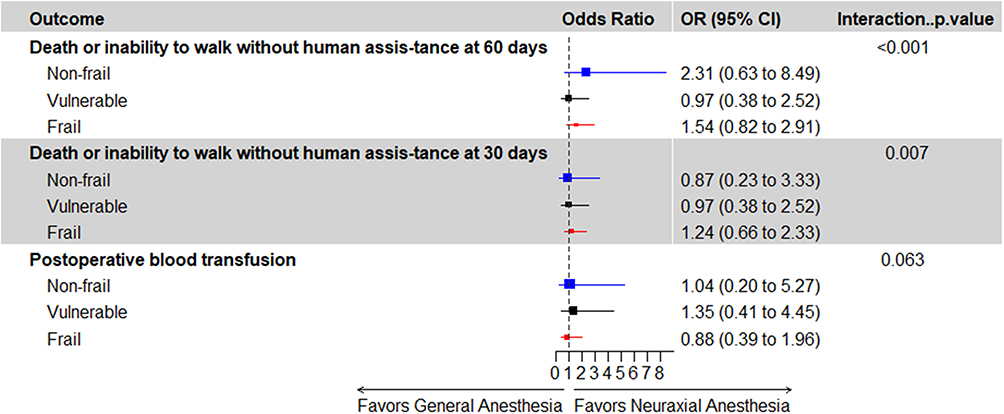 |
Figure 3 OR regression model for neuraxial anesthesia versus general anesthesia based on categorical frailty index using multivariate proportional hazards regression model. |
Approximately 28.4% of patients experienced death or impaired ambulation within 60 days after major orthopedic surgery. The interaction between the FRAIL and anesthesia was significant (Table 3, P<0.001). When categorized according to FRAIL group, it was observed that both intralesional anesthesia and general anesthesia were not correlated with the occurrence of death or impaired ambulation within 60 days post-surgery among non-frail, vulnerable, and frail patients (Figure 3).
The incidence of the composite outcome of death or impaired ambulation at 30 days postoperatively for major orthopedic surgery was 30.2% (Table 3), which was high compared with the incidence of death or impaired ambulation at 60 days postoperatively. There was significant evidence of an interaction between FRAIL and anesthesia methods for the outcome of death or impaired ambulation at 30 days postoperatively (P=0.007), whereas further stratification according to FRAIL revealed a broadly similar incidence in the intrathecal anesthesia versus general anesthesia groups (Figure 3).
The incidence of postoperative blood transfusion in major orthopedic surgery was approximately 14.0% (Table 3). It was noted that there was a potential interaction between FRAIL and anesthesia methods on postoperative blood transfusion (P=0.063). However, the incidence of transfusion was similar between the neuraxial and general anesthesia groups in patients who were non-frail, vulnerable, and frail patients (Figure 3).
Discussion
In this study, we investigated the impact of the choice of anesthesia (neuraxial anesthesia vs general anesthesia) on patients undergoing major orthopedic surgery. Our findings suggest that patients classified as debilitated prior to surgery were more likely to receive neuraxial anesthesia. However, we did not observe a significant reduction in the occurrence of death or impaired ambulation 60 days after surgery among patients in different frail states who received neuraxial anesthesia compared to those who received general anesthesia.
In recent years, there has been a shift in focus within orthopedic patient prognosis studies. While previous studies primarily focused on mortality rates, there is now increased attention on the recovery of postoperative ambulation. This shift is driven by the recognition that postoperative ambulation is of significant concern to patients and their families. However, when using walking impairment as the sole observation index, the outcomes of patients who died during the observation period may be overlooked, leading to potential bias in the results. Therefore, considering death or walking impairment as a composite outcome indicator provides a novel approach to address this limitation.30
Frailty is a nonspecific clinical syndrome of decreased physiologic reserve in the old adult that results in increased vulnerability and decreased stress resistance in the body.31 Performing a preoperative frailty assessment is critical for old adult patients at risk for poor prognosis.FRAIL scale,27 a commonly used clinical frailty assessment scale proposed by the International Society for Geriatric Nutrition, is one of several validated measures of frailty. Several previous clinical studies and meta-analyses32,33
have found that frailty predicts one-year postoperative mortality in old adult orthopedic patients, but there are limitations in determining surgical regression based on mortality alone in old adult patients due to their limited life expectancy and the patients may place more importance on the recovery of independent ambulation after surgery. Therefore, in this study, the composite outcome of death or a new inability to walk 60 days was used as the primary outcome indicator, and debility was found to be an independent risk factor for death or a new inability to walk 60 days postoperatively (OR 4.04, 95% CI 1.04 to 8.57, P<0.001). ASA grading is a common method of preoperative assessment in the preoperative clinic, but it does not accurately assess the preoperative status of older adults. However, after the inclusion of multiple confounders in this study, the correlation between ASA grading and the incidence of death or ambulation impairment occurring at 60d of surgery was not significant. This suggests that frailty assessment is more suitable than ASA grading for preoperative assessment of old adult patients undergoing major orthopedic surgery, and is an effective complement to ASA grading. aCCI scores are often used to reflect the complexity and severity of a patient’s preoperative co-morbidities, with higher scores representing more preoperative comorbidities and a poorer overall state of the patient’s organism. The multifactorial logistic regression analysis showed that higher aCCI score (OR1.36, 95% CI 1.12to1.66, P=0.002) was also a risk factor for death or ambulation disorders at 60d after surgery, suggesting that debility and multimorbidity are closely related and interact with each other, and that active treatment and effective control of co-morbidities in old adult patients before surgery may be able to slow down or even reverse the process of debility, which may help the patients’ regression.
Our study conducted a univariate analysis of the primary outcome and found that the choice of anesthesia modality had an effect on death or walking impairment at 60 days postoperatively (OR 1.82 95% CI 1.14 to 2.88, P=0.012). whereas in, after including multifactorial analysis, the effect of anesthesia modality was not significant (OR 1.42 95% CI 0.83 to 2.42, P=0.199). The further found that in frail patients, the choice of anesthesia was not associated with the incidence of adverse outcomes at 60d postoperatively, which is consistent with what Feng et al14 concluded in a randomized controlled trial of 1600 patients with hip fractures. In a study conducted by Ting Li et al34 it was observed that regional block anesthesia did not show superiority over general anesthesia in terms of all-cause mortality at 30 days postoperatively and postoperative complications. This study specifically focused on 950 patients aged 65 years and older with fragility hip fractures who required surgical repair. These findings are consistent with the results of the current study.
The difference between our study and other similar studies35–37 is that most of the populations they studied were part of major orthopedic surgeries and the surgeries occurred several years ago. These studies did not analyze the impact of frailty on the patient’s postoperative period. Considering that the choice of anesthesia is influenced by multiple factors, it is important to recognize frailty as a confounding factor when investigating the incidence of poor prognosis in old adult patients. This suggests that the mode of anesthesia is affected by confounding factors that can contribute to death or ambulation impairment at 60 days postoperatively. The patient’s frailty status can also significantly influence the choice of anesthesia. It is worth noting that in this study, the number of patients opting for neuraxial anesthesia increased with the degree of frailty, which may indicate selection bias.
Ziyad et al38 designed a paired cohort analysis with a sample of 48,440 total hip arthroplasty patients, it was concluded that patients who received neuraxial anesthesia had a lower incidence of 30-day postoperative death or impaired walking, a result that differs from the present study. However,Gao et ai39 concluded that the choice of anesthesia does not appear to affect 30-day postoperative mortality. Consistent conclusions after we adjusted for debilitation. Interestingly, the choice of anesthesia method also appeared to have no impact on surgical complications, consistent with previous studies.13,35 However, since 50% of postoperative hip arthroplasty dislocations40,41 occurred 90 days after the operation, it would be advisable to further explore this relationship by extending the duration of our follow-up assessments.
We also found that neuraxial anesthesia did not offer any advantages over general anesthesia in frail patients in terms of first postoperative discharges, length of hospital-stay, and hospitalization costs. This lack of difference could be attributed to advancements in general anesthesia medication development, improvements in intraoperative monitoring tools, and the widespread availability of national health insurance policies. Additionally, the use of laryngeal masks has made airway management safer and more comfortable compared to previous methods. Overall, it appears that general anesthesia is a safer option compared to intrathecal anesthesia, which has seen minimal changes in intraoperative management over the past decade. In many surgeries, sedative drugs are commonly used alongside neuraxial anesthesia to alleviate fear and anxiety in patients.42 These drugs are administered after the patient is positioned, and as the sedation score reaches a certain level, the distinction between intrathecal anesthesia and general anesthesia becomes less clear.
Several limitations of this study should be acknowledged. Firstly, it is important to note that this study was conducted at a single center and involved a small sample size of old adult patients undergoing major orthopedic surgery. Therefore, the generalizability of the findings may be limited. Secondly, it is possible that the results of the study were somewhat influenced by the anesthesiologist’s selection preference and the exclusion of debilitated patients who were unable to walk before the surgery. Thirdly, the follow-up period of this study was relatively short, lasting only 60 days, due to energy and time constraints. Lastly, it is worth mentioning that we solely assessed the debilitated state of old adult patients prior to hospitalization. However, it is important to recognize that the debilitated state of patients can significantly change after sustaining injuries, particularly fractures. Therefore, close monitoring of such patients is essential. In future research, it would be beneficial to conduct multicenter, large-sample randomized controlled studies with extended follow-up periods in order to gather more comprehensive data on the long-term prognosis of patients undergoing major orthopedic surgery and experiencing debilitation.
Conclusion
The choice of anesthesia method is influenced by the state of frailty. The selection of neuraxial anesthesia or general anesthesia did not show a significant correlation with death or inability to walk without human assistance at 60 days after surgery in patients depending on frailty.
Preoperative frailty was identified as an independent risk factor for death or impaired ambulation 60 days after surgery in elderly adult patients undergoing major orthopedic procedures. Frail patients exhibited poorer surgical recovery compared to non-frail patients. The integration of frailty assessment into preoperative evaluations enables the timely implementation of perioperative interventions for frail patients, leading to improved patient outcomes.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mitchell MD, Betesh JS, Ahn J, Hume EL, Mehta S, Umscheid CA. Transfusion Thresholds for Major Orthopedic Surgery: a Systematic Review and Meta-analysis. J Arthroplasty. 2017;32(12):3815–3821. doi:10.1016/j.arth.2017.06.054
2. Salminen M, Viljanen A, Eloranta S, et al. Frailty and mortality: an 18-year follow-up study among Finnish community-dwelling older people. Aging Clin Exp Res. 2020;32(10):2013–2019. doi:10.1007/s40520-019-01383-4
3. Susano MJ, Grasfield RH, Friese M, et al. Brief preoperative screening for frailty and cognitive impairment predicts delirium after spine surgery. Anesthesiology. 2020;133(6):1184–1191. doi:10.1097/ALN.0000000000003523
4. Al-Husinat L, Jouryyeh B, Al Sharie S, et al. Bone cement and its anesthetic complications: a narrative review. J Clin Med. 2023;12(6):2105. doi:10.3390/jcm12062105
5. Ran W, Li S, Yuan R, Luo H, Li P, Gao J. Effect of tourniquet technique on postoperative delirium in elderly patients with total knee arthroplasty: a randomized single-blind controlled trial. BMC Anesthesiol. 2022;22(1):396. doi:10.1186/s12871-022-01938-5
6. Rao S, Treggiari MM. Anesthesia for Acute Spinal Cord Injury. Anesthesiol Clin. 2021;39(1):127–138. doi:10.1016/j.anclin.2020.11.011
7. Veiga-Gil L, Pueyo J, Lopez-Olaondo L, Jiang L. Postoperative nausea and vomiting: physiopathology, risk factors, prophylaxis and treatment. Rev Esp Anestesiol Reanim. 2017;64(4):223–232. doi:10.1016/j.redar.2016.10.001
8. Jackson J, Davies P, Leggett N, et al. Systematic review of interventions for the prevention and treatment of postoperative urinary retention. BJS Open. 2019;3(1):11–23. doi:10.1002/bjs5.50114
9. Memtsoudis SG, Rasul R, Suzuki S, et al. Does the impact of the type of anesthesia on outcomes differ by patient age and comorbidity burden? Reg Anesth Pain Med. 2014;39(2):112–119. doi:10.1097/AAP.0000000000000055
10. Johnson RL, Kopp SL, Burkle CM, et al. Neuraxial vs general anaesthesia for total hip and total knee arthroplasty: a systematic review of comparative-effectiveness research. Br J Anaesth. 2016;116(2):163–176. doi:10.1093/bja/aev455
11. Ahn EJ, Kim HJ, Kim KW, Choi HR, Kang H, Bang SR. Comparison of general anaesthesia and regional anaesthesia in terms of mortality and complications in elderly patients with Hip fracture: a nationwide population-based study. BMJ Open. 2019;9(9):e029245. doi:10.1136/bmjopen-2019-029245
12. Ravi B, Pincus D, Choi S, Jenkinson R, Wasserstein DN, Redelmeier DA. Association of duration of surgery with postoperative delirium among patients receiving hip fracture repair. JAMA Network Open. 2019;2(2):e190111. doi:10.1001/jamanetworkopen.2019.0111
13. Johnson RL, Frank RD, Habermann EB, et al. Neuraxial anesthesia is associated with improved survival after total joint arthroplasty depending on frailty: a cohort study. Reg Anesth Pain Med. 2020;45(6):405–411. doi:10.1136/rapm-2019-101250
14. Neuman M, Feng R, Carson J, et al. Spinal anesthesia or general anesthesia for hip surgery in older adults. The New England Journal of Medicine. 2021;385(22):2025–2035. doi:10.1056/NEJMoa2113514
15. Schwenk ES, McCartney CJ. General anesthesia is an acceptable choice for hip fracture surgery. Reg Anesth Pain Med. 2023;48(8):428–429. doi:10.1136/rapm-2023-104454
16. Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet. 2013;381(9868):752–762. doi:10.1016/S0140-6736(12)62167-9
17. Ma L, Sun F, Tang Z. Social frailty is associated with physical functioning, cognition, and depression, and predicts mortality. J Nutr Health Aging. 2018;22(8):989–995. doi:10.1007/s12603-018-1054-0
18. Yamada M, Arai H. Social frailty predicts incident disability and mortality among community-dwelling Japanese older adults. J Am Med Dir Assoc. 2018;19(12):1099–1103. doi:10.1016/j.jamda.2018.09.013
19. Kennedy CA, Shipway D, Barry K. Frailty and emergency abdominal surgery: a systematic review and meta-analysis. Surgeon. 2022;20(6):e307–e314. doi:10.1016/j.surge.2021.11.009
20. Lemos JL, Welch JM, Xiao M, Shapiro LM, Adeli E, Kamal RN. Is frailty associated with adverse outcomes after orthopaedic surgery?: a systematic review and assessment of definitions. JBJS Rev. 2021;9(12). doi:10.2106/JBJS.RVW.21.00065
21. Yan B, Sun W, Wang W, Wu J, Wang G, Dou Q. Prognostic significance of frailty in older patients with hip fracture: a systematic review and meta-analysis. Int Orthop. 2022;46(12):2939–2952. doi:10.1007/s00264-022-05605-9
22. Meyer M, Leiss F, Greimel F, et al. Impact of malnutrition and vitamin deficiency in geriatric patients undergoing orthopedic surgery. Acta Orthop. 2021;92(3):358–363. doi:10.1080/17453674.2021.1882092
23. Zazzara MB, Vetrano DL, Carfi A, Onder G. Frailty and chronic disease. Panminerva Med. 2019;61(4):486–492. doi:10.23736/S0031-0808.19.03731-5
24. Wang D, Yin P, Li Y, et al. Frailty factors and outcomes in patients undergoing orthopedic surgery: protocol for a systematic review and meta-analysis. JMIR Res Protoc. 2022;11(4):e28338. doi:10.2196/28338
25. Zhang DL, Cong YX, Zhuang Y, Xu X, Zhang BF. Age-adjusted Charlson comorbidity index predicts postoperative mortality in elderly patients with hip fracture: a prospective cohort. Front Med. 2023;10:1066145. doi:10.3389/fmed.2023.1066145
26. Jiang L, Chou ACC, Nadkarni N, et al. Charlson comorbidity index predicts 5-year survivorship of surgically treated hip fracture patients. Geriatr Orthop Surg Rehabil. 2018;9:2151459318806442. doi:10.1177/2151459318806442
27. Morley JE, Malmstrom TK, Miller DK. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged African Americans. J Nutr Health Aging. 2012;16(7):601–608. doi:10.1007/s12603-012-0084-2
28. Medlej K. Calculated decisions: Richmond Agitation-Sedation Scale (RASS). Emerg Med Pract. 2021;23(Suppl 3):CD3–CD4.
29. Carson JL, Terrin ML, Noveck H, et al. Liberal or restrictive transfusion in high-risk patients after hip surgery. N Engl J Med. 2011;365(26):2453–2462. doi:10.1056/NEJMoa1012452
30. Diehr P, Johnson LL, Patrick DL, Psaty B. Methods for incorporating death into health-related variables in longitudinal studies. J Clin Epidemiol. 2005;58(11):1115–1124. doi:10.1016/j.jclinepi.2005.05.002
31. Hoogendijk EO, Afilalo J, Ensrud KE, Kowal P, Onder G, Fried LP. Frailty: implications for clinical practice and public health. Lancet. 2019;394(10206):1365–1375. doi:10.1016/S0140-6736(19)31786-6
32. Ma Y, Wang A, Lou Y, Peng D, Jiang Z, Xia T. Effects of frailty on outcomes following surgery among patients with hip fractures: a systematic review and meta-analysis. Front Med. 2022;9:829762. doi:10.3389/fmed.2022.829762
33. Song Y, Wu Z, Huo H, Zhao P. The impact of frailty on adverse outcomes in geriatric hip fracture patients: a systematic review and meta-analysis. Frontiers in Public Health. 2022;10:890652. doi:10.3389/fpubh.2022.890652
34. Li T, Li J, Yuan L, et al. Effect of regional vs general anesthesia on incidence of postoperative delirium in older patients undergoing hip fracture surgery: the raga randomized trial. JAMA. 2022;327(1):50–58. doi:10.1001/jama.2021.22647
35. Owen AR, Amundson AW, Larson DR, et al. Spinal versus general anaesthesia in contemporary primary total knee arthroplasties. Bone Joint J. 2022;104-B(11):1209–1214. doi:10.1302/0301-620X.104B11.BJJ-2022-0469.R2
36. Chen DX, Yang L, Ding L, Li SY, Qi YN, Li Q. Perioperative outcomes in geriatric patients undergoing Hip fracture surgery with different anesthesia techniques: a systematic review and meta-analysis. Medicine. 2019;98(49):e18220. doi:10.1097/MD.0000000000018220
37. Memtsoudis SG, Cozowicz C, Bekeris J, et al. Anaesthetic care of patients undergoing primary hip and knee arthroplasty: consensus recommendations from the International Consensus on Anaesthesia-Related Outcomes after Surgery group (ICAROS) based on a systematic review and meta-analysis. Br J Anaesth. 2019;123(3):269–287. doi:10.1016/j.bja.2019.05.042
38. Knio ZO, Clancy PW, Zuo Z. Effect of spinal versus general anesthesia on thirty-day outcomes following total Hip arthroplasty: a matched-pair cohort analysis. J Clin Anesth. 2023;87:111083. doi:10.1016/j.jclinane.2023.111083
39. Cao MM, Zhang YW, Sheng RW, et al. General anesthesia versus regional anesthesia in the elderly patients undergoing hip fracture surgeries: a systematic review and meta-analysis of randomized clinical trials. World J Surg. 2023;47(6):1444–1456. doi:10.1007/s00268-023-06949-y
40. Abdel MP, Ledford CK, Kobic A, Taunton MJ, Hanssen AD. Contemporary failure aetiologies of the primary, posterior-stabilised total knee arthroplasty. Bone Joint J. 2017;99;1.
41. Abdel MP, von Roth P, Jennings MT, Hanssen AD, Pagnano MW. What safe zone? the vast majority of dislocated THAs are within the Lewinnek safe zone for acetabular component position. Clin Orthop Relat Res. 2016;474(2):386–391. doi:10.1007/s11999-015-4432-5
42. Li JQ, Yuan H, Wang XQ, Yang M. Dexmedetomidine-induced anesthesia in elderly patients undergoing hip replacement surgery. World J Clin Cases. 2023;11(16):3756–3764. doi:10.12998/wjcc.v11.i16.3756
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.