")
Back to Journals » Clinical Audit » Volume 14
Compliance to Post-Anesthesia Care Unit Discharge Score Practice Among Nurses at Post-Anesthesia Care Unit in the Jimma Medical Center in Ethiopia: A Best Practice Implementation Project, 2021
Authors Tageza Ilala T , Yinges Kebede M, Teku Ayano G, Kelbesa Olika M
Received 21 February 2022
Accepted for publication 27 June 2022
Published 8 July 2022 Volume 2022:14 Pages 55—64
DOI https://doi.org/10.2147/CA.S361924
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zoka Milan
Tajera Tageza Ilala,1 Mengistu Yinges Kebede,1 Gudeta Teku Ayano,1 Megersa Kelbesa Olika2
1Department of Anesthesia, Faculty of Medicine, Hawassa University, Hawassa, Ethiopia; 2Department of Anesthesia, Institute of Health, Jimma University, Jimma, Ethiopia
Correspondence: Tajera Tageza Ilala, Department of Anesthesia, Faculty of medicine, Hawassa University, Hawassa, Ethiopia, Email [email protected]
Background: PACU discharge score criteria facilitate a risk safe and timely discharge of surgical patients under satisfactory safety conditions, thereby improving post-operative patient outcomes and requiring minimum resources. The aim of this best practice study was to provide best evidence-based practice on post-anesthesia discharge score criteria among nurses at the post-anesthesia care unit in the Jimma Medical Center.
Methods: An audit and re-audit inter-professional study was employed. Twenty-four post-anesthesia care unit nurses were interviewed for baseline audit and 118 post-anesthesia care unit discharge scoring opportunities were observed for follow-up audit using three audit criteria.
Results: First stage of the audit showed a performance of 37.5% for successful pain assessment, level of consciousness, nausea, vomiting, and blood pressure prior to patient discharge from the post-anesthesia care unit, and 62.5% for routine use of discharge criteria score to determine discharge readiness of patients from the post-anesthesia care unit. Re-audit results revealed an average of 40% improvement of the audit criteria practice toward post-anesthesia care unit discharge score.
Conclusion: This study revealed that the use of various strategies such as role modeling, posting reminders about PACU discharge criteria, and presenting guidelines to the recovery teams resulted in improved practice toward best available evidence for post-anesthesia care unit discharge score practice. Including the stakeholders in determining the strategies to upgrade practice is crucial in the accomplishment of promoting successful PACU discharge score. To ensure sustainable compliance to successful PACU discharge score criteria, a planned schedule of random report was employed by the clinical team.
Keywords: audit, best practice, nurses, PACU discharge score, PACU, implementation project
Background
The post-anesthesia care unit (PACU) is seen as the suitable place for the immediate recovery of the surgical patient after an operation. Hence, nurses play a major role in the caring for patients in the recovery room, and the anesthesia provider usually authorizes the fitness for transfer to the post-anesthesia care nursing team.1 However, the occurrence of communication gaps or errors is suggested to affect the safety of patients, and might lead to care-giver frustration as a result of inadequate care given, delays, and the increased burden in workload.1,2
The main issue to be addressed in the pace of quality of clinical care is safe and early patient discharge following emergence from general anesthesia and/or sedation.3
The immediate time after anesthesia is a critical time for patient emergence, and/or awakening from general anesthesia, which obliges careful monitoring to ensure early recognition and management of post-operative complications. It has been reported that the length of post-anesthesia care unit stay was affected by a variety of factors, such as preoperative health status of the patient, the type and site of the procedure, techniques of anesthesia, and the perioperative status of patient vital signs. This culminates in a routine practice of post-anesthesia care unit patient transfer protocol or guidelines in facilitating an acceptably short duration of PACU stay time, in relation to patient fitness for transfer to the respective ward, which is conventionally practiced as a subjective evaluation of discharge fitness and safe hemodynamic measurements by nurses.2,4,5
The post-anesthesia care standards usually stress the role of anesthetists, or anesthesiologists; but the role of nurses in patient care at post-anesthesia care unit needs to focus on the provision of post-anesthetic nursing care. Therefore, promoting nursing care on the scientific grounds of practice is a framework for proper and better care delivery. Even though a multitude of benchmarks were used to evaluate patient transfer from the post-anesthesia care unit, we aimed to apply best evidence practice that will help PACU teams to define the right discharge time avoiding dilemmas during discharge.1,3,6
Guidelines need to be there to ensure that the recovery room nurses or other professionals make proper and right decisions during patient transfer to their respective wards. Furthermore, it is pivotal to take into account the level of sedation (mental status), breathing, hemodynamic status, pain management, and care for the wound or surgical site.6–8
We believe that patients were often unnecessarily kept in the recovery room for a prolonged duration, due to lack of appropriate discharge score, and this may lead to increased PACU resource load, including human burden, hospital stay, and may create an operating room backlog. Thus, the presence of predetermined, criteria-based discharge standards facilitates the identification and early management of patients vulnerable to deterioration in the post-anesthesia care unit, upgrades record keeping habits for handover among the post-anesthesia care unit team or nurses to the ward nurse, and ameliorates patient safety, leading to better outcomes and minimizing healthcare charges.6,9,10
Concern about poor post-anesthesia care unit discharge score practice in our country and its consequences for the patient’s unnecessary cost with delayed discharge and hospital resource wastage was the motive behind conducting this study. To date, the Joanna Briggs Institute system of evidence-based best practice was not conducted in our country, particularly Jimma Medical Center. Hence, this points to a clear need of enhancing post-anesthesia care unit discharge criteria practice in Ethiopia, and promoting best PACU discharge practices.
Furthermore, the purpose of this study was to promote the best PACU discharge score criteria practice at the recovery room in the Jimma Medical Center. By implementing a successful post-anesthesia care unit discharge score criteria practice project within the institution, we were obliged to share a contribution in minimizing resource wastage, and increasing recognition of clinical deterioration, and thus upgrading the clarity of handover from PACU to wards.
Therefore, we aimed primarily to compare the standard best practice evidence of PACU discharge criteria with the current discharge criteria of PACU in Jimma Medical Center and implement the best practice.
Aim and Objectives
The objective of our study was to provide evidence informed best practice of PACU discharge scoring criteria among nurses at Post-Anesthesia Care Unit in the Jimma Medical Center.
Specific Objectives of the Study
- To recognize and include a multidisciplinary professional team important for facilitating evidence informed practice in the recovery room and evaluate the best practice compliance in the recovery room utilizing the baseline audit.
- To present results of a baseline audit, and design and undertake action to ear-mark areas of poor performance with best practice in the recovery room.
- To conduct a follow-up audit, evaluate the extent and nature of improved compliance toward evidence informed best practice, identify areas of poor practice, and design policy to sustain and promote provision of recovery room care to post-operative surgical patients in the Jimma Medical Center.
The goal of our project is to evaluate compliance toward evidence informed practice regarding post-anesthesia care unit discharge score criteria among the PACU nurses in the Jimma Medical Center (JMC).
The specific aims are:
- To assess the baseline or current compliance with evidence informed criteria toward PACU discharge score
- To assess ongoing compliance with evidence informed criteria toward post-anesthesia care unit discharge score
- To upgrade the practice toward PACU discharge score criteria among PACU teams
- To upgrade compliance with evidence informed criteria toward post-anesthesia care unit discharge score
- To upgrade outcomes toward PACU discharge score criteria practice
Methods
The project was carried out at the PACU in the Jimma Medical Center. Jimma Medical Center (JMC) is one of the oldest public hospitals in Ethiopia. It was established in 1938. Geographically, it is located in Jimma city, 352 km southwest of Addis Ababa. After the transfer of its ownership to Jimma University, the university has undertaken renovation and expansion work to make the hospital conducive for service, teaching, and research. It is the only referral and specialized hospital in the southwest part of Ethiopia, serving as teaching and research center. It serves a population of around 15 million from the Oromia zones, Gambella, South nation, as well as nationalities and peoples from other nearby regions or parts of Ethiopia. Annually, greater than six thousand patients were operated on, including cesarean section, and were given PACU service. It has a bed capacity of 800, and 1600 staff, among which 610 were nurses, 105 were senior physicians with different specialty and sub-specialty, and 61 were general practitioners. The services provided by the hospital were clinical (internal medicine, general surgery, pediatrics, gynecology/obstetrics, ophthalmology, ENT/plastic), radiology, laboratory, and pharmacy services.
Jimma Medical Center has 11 major operation theaters, two intensive care units (ICU), and one post-anesthesia care unit with 8 beds equipped with one monitor and one oxygen cylinder for two beds, and one mobile suction machine (Supplementary Figure 1). Jimma Medical Center post-anesthesia care unit has 24 nurses; 15 of them were males, and 9 of them were females. The PACU gives 24-hour service, with three shifts of 8 hours as eight nurses were assigned per one shift for 8 hours and two nurses were considered for one bed.
A baseline clinical audit was done on all adult patients admitted to the post-anesthesia care unit, and the discharge score criteria evaluation policy was utilized at the post-anesthesia care unit of JMC after the operation. An exhaustive exploration of the literature was conducted to obtain any important information on the best practice of PACU discharge score criteria.
This study applies the introducing research into clinical practice report and the strength and weakness tool. The introduction of research into clinical practice principles for providing evidence informed clinical care includes three stages of action:
- Project team establishment and conducting baseline audit depending on evidence based standard
- Reflect on the baseline audit results, plan and employment of plan of action to improve areas of reduced or non-compliance identified by the introducing research into clinical practice principles
- Employ continuous follow-up to determine the response to undertaken action in improving clinical care, and assess ongoing concern of practice to be raised in the subsequent audits.
The clinical audit was done in all adult populations (≥18 years) who were admitted to the post-anesthesia care unit after their operation and given PACU care, both emergency and elective surgery. Hence, we implemented the best evidence-based practice by considering patient preference, PACU experts’ opinion, and Jimma Medical Center rules and regulations.
The project team leader instructed the team on the practice of successful post-anesthesia care unit discharge score standards.
Three audit criteria listed below were utilized for successful post-anesthesia care unit discharge score practice and was employed in the first audit stage (baseline) and the follow-up report dependent on evidence summary.
This evidence informed implementation project uses the guidelines of PACU discharge criteria that have been prepared by the Danish Society of Anesthesiology and Intensive Care Unit.
This guideline scheme for facilitating evidence informed healthcare tasks involve three steps:
Step 1: Team Establishment and First Stage Report
First, permission was sought from Jimma Medical Center and the respective administrators to employ this best implementation study. Even though a formal written letter of ethics was not required, consent was obtained to retain the confidentiality of data delivered by each study subject.
The principal investigator established who were the stakeholders in the institution to become engaged in the project.
- The implementation of the project was to involve management bodies, PACU Nurses, anesthesiologists, anesthetists, anesthesia students, and patients:
- Administrative bodies
- o Showing readiness and interest for project implementation
- o They were helping us in allowing implementation of the intervention and facilitation process.
- Anesthesiologist’s role:
- o Making sure that every member of staff has a clear understanding of their role and application to the healthcare environment
- o Convincing and influencing management bodies regarding the implementation of the project
- o Promoting use of best PACU discharge criteria by nurses.
- Anesthetist’s role:
- o Supervising nurses while they were implementing the project
- Students’ role:
- o Showing commitment to implementation guideline and willingness to apply it during their practice
- PACU Coordinator: coordinator provides relevant information about their current discharge criteria and facilitates implementation of best practice of patient discharge criteria by coordinating PACU nurses.
In stage 1, we conducted a baseline audit to evaluate areas of deficiency between current post-anesthesia care unit discharge score practice and evidence-based post-anesthesia care unit discharge score criteria. The post-anesthesia care unit discharge score practices of post-anesthesia care unit nurse professionals were evaluated by utilizing three criteria of successful post-anesthesia care unit discharge score practice. A consecutive sampling technique was employed, and we had 118 post-anesthesia care unit discharge score observations. Observational study was conducted to collect data, and then the practices of these three audit criteria of successful post-anesthesia care unit discharge score were assessed. We believe that the staff had never received education about the post-anesthesia care unit discharge score.
We received verbal informed consent from each PACU healthcare provider; they were notified of the particular parameters that were being evaluated. Data were collected through observation of the PACU nurse practice by two master’s students. The data collectors were trained in the fundamentals of evidence informed post-anesthesia care unit discharge score criteria. During the data collection period 118 post-anesthesia care unit discharge score opportunities were obtained (from April 17 to June 17, 2021) in the PACU.
Furthermore, implementation of this evidence informed study needs a favorable working area. As a result, on top of aforementioned assessment, facility assessment with regard to the application of best practice was made, for the implementation of best post-anesthesia care unit discharge scoring. The resource availability assessment parameters were constructed dependent on the needed appropriate PACU instruments.
This evidence informed study of best practice was employed from April 17 to August 17, 2021, for a duration of 20 weeks.
Audit Standards
An evidence-based audit criteria set was used in combination with the explanation of the study unit and techniques of assessing compliance toward best evidence informed practice for every particular audit criterion as shown (Table 1).
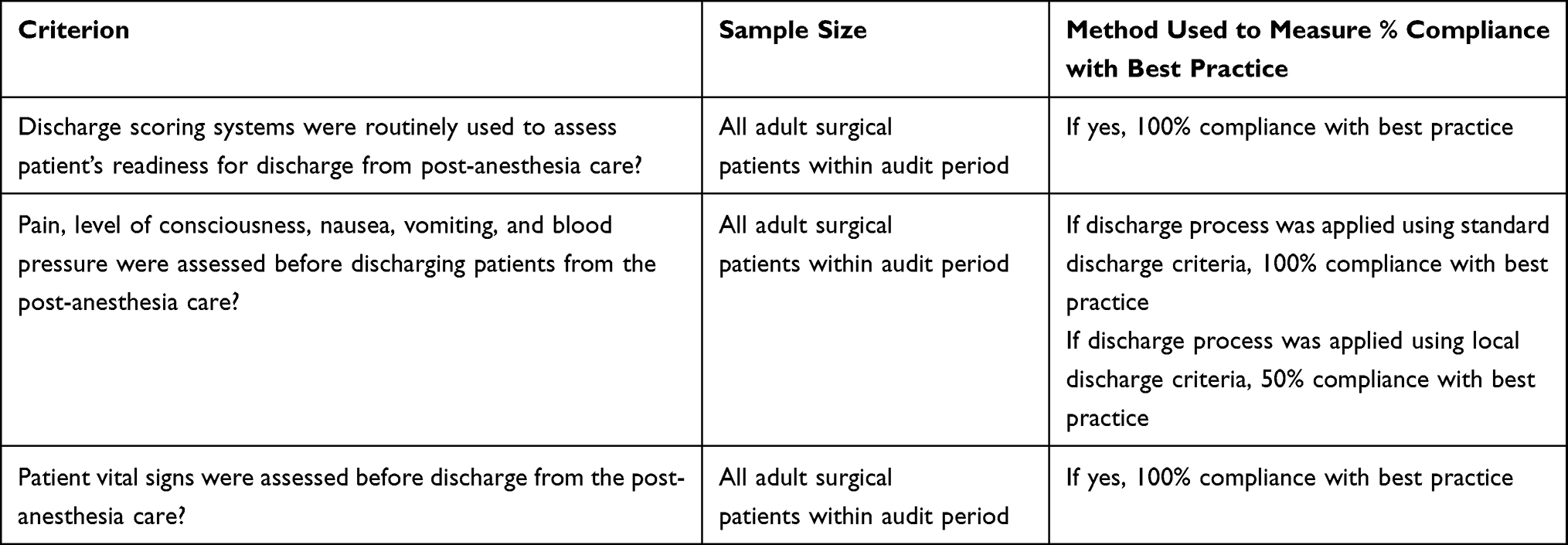 |
Table 1 The Evidence-Based Audit Criteria Used in Combination with an Explanation of the Study Unit and Techniques of Assessing Compliance Toward Best Evidence Informed Practice for Every Particular Audit Criterion |
Stage 2: Design and Implementation of Policies and Identification of Problems to Promote Clinical Practice
- General implementation strategies were:
Stage 3: Re-Audit After Implementing Action Plan
A re-audit time period for the study was four weeks. Before and during this time, each instance of PACU discharge score criteria manipulation and usage was followed and assessed against the implementation of standard practice.
This re-audit project includes all adult surgical patients for which PACU discharge score criteria was applied.
Data were collected for 118 PACU discharge score opportunities during patient discharge from PACU by nurses using three audit criteria.
Results
Stage 1: First Audit
The first stage audit evaluation described that the problems of conducting successful post-anesthesia care unit discharge score performance may be lack of PACU staff awareness toward PACU discharge score criteria, and also inadequate equipment supply (monitors) as shown (Table 2).
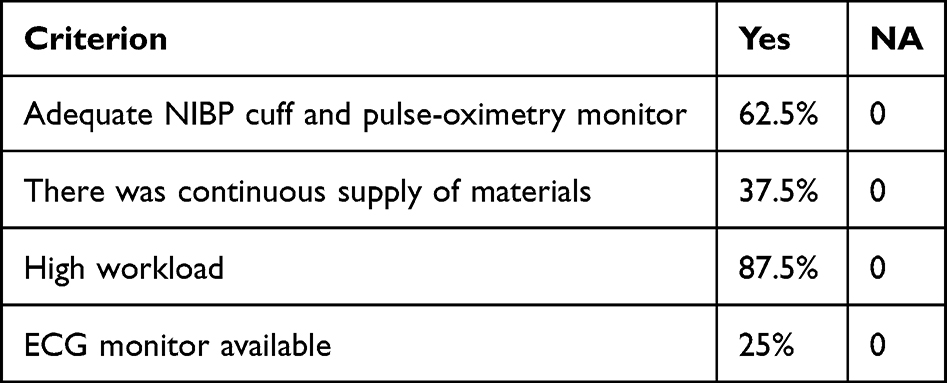 |
Table 2 Results of Baseline Audit on Facility Assessment at Post-Anesthesia Care Unit in the Jimma Medical Center, 2021 |
Compliance to successful post-anesthesia care unit discharge score was lowest for criterion 2 with 37.5%. Compliance was highest for criterion 3. The description of frequencies of the three audit criteria of successful post-anesthesia discharge scoring for baseline audit are shown in Table 3. The compliance rate of each audit criterion is described in Figure 1.
 |
Table 3 Results of Baseline Audit on the Practice of Post-Anesthesia Care Unit Discharge Score Criteria Among PACU Nurses at PACU in the JMC, Ethiopia, 2021 |
 |
Figure 1 The compliance rate of effective post-anesthesia care unit discharge score criteria practice among PACU nurses at PACU in the JMC, South West Ethiopia, 2021. |
Stage 2: Implementation of Best Practice
The problems, action, and materials were established with the stakeholders as explained in the methods portion. As a whole, the strategies were applied for 8 weeks' duration to reduce or remove the areas of inadequate practice identified in the first phase of audit. It includes:
- Reporting and reflecting on the low results from the first stage of audit.
- Discussion with PACU nurses to identify problems.
- Posting reminders and PACU transfer score criteria on the PACU walls (inside). We posted reminders and PACU discharge score criteria on walls of PACU as shown in the Appendix 2A and B.
- Education through distribution of the post-anesthesia care unit discharge score criteria.
- Attaching the PACU discharge score criteria with each patient card after filling during discharge to ward.
The introducing research into clinical practice systems and responses are explained in Appendix 1.
Stage 3: Re-Audit
The re-audit result described that the rate of compliance for audit criteria one and three was 100%, and found a slightly lower compliance rate with criterion two, which is 93.2% as shown in Table 4.
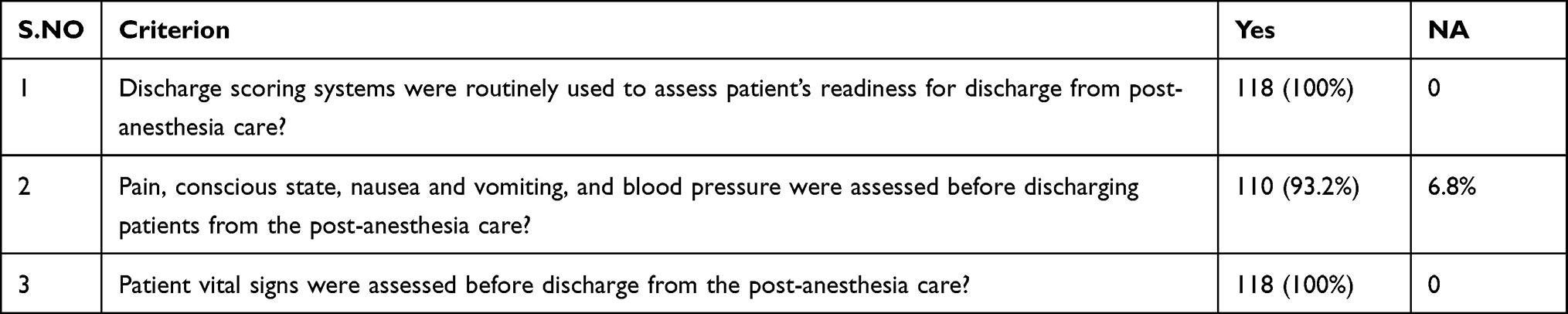 |
Table 4 The Result of Post-Implementation Audit on the Practice of Successful Post-Anesthesia Care Unit Discharge Score Criteria Among PACU Nurses at PACU in the JMC, Ethiopia, 2021 |
We appreciated that there was a considerable improvement in the compliance rate toward PACU discharge score criteria after the implementation of the action planned to manage the identified problems.
Results of baseline audit were compared with the re-audit or post-implementation report, and the comparison of rate of compliance to successful post-anesthesia care unit discharge score criteria practice is described in Figure 2.
 |
Figure 2 Results of baseline audit as compared with the post-implementation audit; comparison of rate of compliance to successful post-anesthesia care unit discharge score criteria practice among PACU nurses in the JMC, South West Ethiopia, 2021. |
There was a marked change in compliance when we compare the compliance of baseline audit with the compliance to post-implementation audit of post-anesthesia care unit discharge score among nurses in PACU in the Jimma Medical Center after implementation of the action planned to manage the identified problems (Figure 2).
Discussion
A first stage of audit revealed that there exists a lack of or reduced adherence toward the basic principles of post-anesthesia care unit discharge score among PACU nurses, as they were obliged to assess patient vital signs before discharge from the PACU.
The evidence implementation study was effective in the sense that dramatic changes were reported on all of the evidence informed auditing score criteria ranging from 25% to 56%. The re-audit and post-implementation report revealed a 100% rate of compliance toward criteria one and three. However, the rate of compliance with criterion two was reported to be 93.2%.
The main problems detected upon evaluation of appropriate resources were the increased staff workload and inadequate access to monitoring instruments. We facilitate sustainable provision of monitoring devices by using the data acquired from resource assessment. Consequently, this has in advance created a “favorable” work area for the evidence based best PACU practice.
In addition to aforementioned problems, there were a variety of hindering factors identified including the low level of performance and lack of awareness, as well as misunderstanding and ignorance. With respect to this, the change directed policies designed to address those challenges were successful in improving the compliance rate. Additionally, we observed a remarkable improvement in compliance to successful post-anesthesia care unit discharge score in the expense of PACU staff education, and awareness creation toward areas of inconvenience. For instance, we worked towards convincing the PACU nurses about the use and practice of discharge score appropriately before transferring patients to ward and attaching the filled criteria to each patient card during discharge.
To support and promote the compliance of PACU nurses with effective post-anesthesia care unit discharge score criteria, learning materials were provided to them via sharing updated evidence such as guidelines and standard protocols, role modeling, putting up reminder posters, demonstrations, and discussion at the morning session in daily practice. Setting protocol and identification of an individual’s ignorant practice followed by active feedback had also resulted in substantial changes toward the compliance with successful post-anesthesia care unit discharge score.
The re-audit revealed remarkable improvements in all of the 118 observations. Accordingly, subsequent evidence implementation studies should stress the importance of adherence to the criteria of the post-anesthesia care unit discharge score.
We shared the result of this best evidence informed practice implementation study with team members and respective stakeholders to facilitate possible decision making.
Sustainability
It was noteworthy that the study was an effective study, and it plays a crucial role in promoting the patient outcomes in the institution where it was done, even if it was on a limited scale.
Also worth noting is that, although of limited scope, the present study might delineate why a comparably simple-to-implement study can foster effective change in PACU discharge score criteria practice. The current experience stipulated that the engagement of stakeholders and clinical practitioners or care providers is a key approach for putting the best available evidence into clinical practice. Because of the high workload, efforts were required to carefully incorporate the specified strategies in the present study into routine clinical care. After regular build-up policies were settled, it is challenging to establish continuous progression. In relation to this, appreciation of good practice among PACU nurses, by initiating them for successful post-anesthesia care unit discharge score practice, is very important.
Furthermore, so as to establish a continuous progress of the best evidence informed practice, the participation of students (interns, residents, and post-graduate students) into the clinical practice, and other health providers could be considered. Hence, regular random orientation and training will be necessitated for the effective step-up of the study. Constant programmed reports will be essential.
Conclusion
In general, the goal of the present study was to apply current best evidence of PACU transfer score practice. In the baseline audit, we were unable to include the use of appropriate equipment as it needs time and arrangement of working habit to change PACU material handling. But we have managed to implement post-anesthesia care unit discharge score criteria. This project has demonstrated and confirmed that the implemention of these guidelines has significant effect on promotion of PACU nurse and other professional practice toward standard level.
Abbreviations
ECG, electrocardiograph; JMC, Jimma Medical Center; BP, blood pressure; PACU, post-anesthesia care unit.
Data Sharing Statement
Data are available from corresponding author email upon reasonable request.
Consent for Publication
Informed written consent for the publication of their images was obtained from the respective PACU nurses.
Acknowledgments
The authors would like to extend our deep gratitude to JMC staff, team members, and PACU nurses for technical support, devoting their time, and genuine participation.
Author Contributions
All authors made a significant contribution in the conception, study design, execution, and acquisition of data, analysis, and interpretation. All authors took part in drafting, revising, or critically reviewing the article, gave final approval of the version to be published, have agreed to submit the article to this journal, and also agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Do IB, Jellish WS, Kleinman B, et al. Use of postanesthesia discharge criteria to reduce discharge delays for inpatients in the postanesthesia care unit. J Clin Anesth. 2008;20(3):175–179. doi:10.1016/j.jclinane.2007.09.014
2. Prates A, Colognese B, Cadore L, Caumo W. Development of a recovery-room discharge checklist (SAMPE checklist) for safe handover and its comparison with Aldrete and White scoring systems. Braz J Anesthesiol. 2021;(xx). doi:10.1016/j.bjane.2021.07.004
3. Phillips N. discharge scoring criteria: a systematic review School of Nursing & Midwifery. J Evid Based Healthcare. 2013;11(4):275–284.
4. Phillips NM, Street M, Kent B, Haesler E, Cadeddu M. Post-anaesthetic discharge scoring criteria: key findings from a systematic review. Int J Evid Based Healthc. 2013;11(4):275–284. doi:10.1111/1744-1609.12044
5. Lee JH, Ki M, Choi S, et al. Validity and reliability of the Korean version of the Quality of Recovery-15 questionnaire. Korean J Anesthesiol. 2021;74(2):142–149. doi:10.4097/kja.20435
6. Street M, Phillips NM, Kent B, Colgan S, Mohebbi M. Minimising post-operative risk using a Post-Anaesthetic Care Tool (PACT): protocol for a prospective observational study and cost-successfulness analysis. BMJ Open. 2015;5:e007200.
7. Reed AH. Criteria for the safe discharge of patients from the recovery room. Nurs Times. 2003;99(38):22–24.
8. Armstrong J, Forrest BH, Crawford BMW. A prospective observational study comparing a physiological scoring system with time-based discharge criteria in pediatric ambulatory surgical patients ´ tude d ’ observation prospective, comparant un syste ` me de Une e ` des crite ` res de conge ´ fond. Can J Anaesth. 2015;62(10):1082–1088. doi:10.1007/s12630-015-0428-6
9. Jenkins K, Grady D, Wong J, Correa R, Armanious S, Chung F. Post-operative recovery: day surgery patients ’ preferences. Br J Anaesth. 2001;86(2):272–274. doi:10.1093/bja/86.2.272
10. Chungl FF, Ghan VWS, Ong D. A postanaesthetic discharge scoring system for home readiness after ambulatory surgery. Ambul Surg. 1993;1:189–193.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.