")
Back to Journals » Nature and Science of Sleep » Volume 15
Bidirectional Relationship Between Circadian Rhythm and Frailty
Authors Pan Y, Feng ZQ, Yuan Y, Hu GM, Jiang Y, Dong JC
Received 22 August 2023
Accepted for publication 7 November 2023
Published 21 November 2023 Volume 2023:15 Pages 949—953
DOI https://doi.org/10.2147/NSS.S436488
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Yu Pan,* Zhu Qing Feng,* Yan Yuan,* Gui Ming Hu, Yi Jiang, Jiang Chuan Dong
Department of Geriatrics, The Second Affiliated Hospital of Chongqing Medical University, Chongqing, 400010, People’s Republic of China
*This authors Contributed equally to this work
Correspondence: Jiang Chuan Dong, Department of Geriatrics, The Second Affiliated Hospital of Chongqing Medical University, No. 74 Linjiang Road, Yuzhong District, Chongqing, 400010, People’s Republic of China, Email [email protected]
Abstract: Coupled with the ageing population, frailty, characterized by high prevalence and difficult treatment, has progressively evolved into a significant public health concern. Frail individuals can often observe serious metabolic disorders and sleep-wake cycle disruption, which may be caused by the decline in physiological reserve and increased vulnerability. Moreover, sleep-wake cycle disruptions and metabolic dysfunctions associated with circadian rhythm disorders are considered to be a central part of the disorder. Previous studies have documented a correlation between frailty and sleep-wake disruptions; nevertheless, the association between circadian rhythm disorders and frailty has not yet been definitively established. Hence, we hypothesize a bidirectional link between circadian rhythm disorders and frailty, with each condition exerting a significant influence on the progression of the other’s disease trajectory.
Keywords: circadian rhythm, frailty, metabolism, neuropathy, insulin resistance
Introduction
Circadian rhythm abnormalities and frailty are significant factors that relate to various biological processes and exert an impact on a range of human diseases. Research has indicated that the primary regulator of the body’s circadian rhythm, responsible for the regulation of circadian rhythm, is the suprachiasmatic nucleus (SCN), located in the anterior hypothalamus (Figure 1).1,2 The human body possesses the capacity to perceive alterations in both the external and biological environment, and subsequently, it can effectively regulate human biorhythms. This regulatory process mostly occurs through a feedback loop involving six fundamental genes, namely CLOCK, BMAL1, PER1, PER2, CRY1, and CRY2.3 In addition, frailty, which refers to an elevated susceptibility to stressors affecting various physiological systems among older adults,4 exhibits a strong association with factors within the biological internal environment, including diminished levels of physical activity and alterations in body weight.5 Interestingly, circadian rhythm disorders and frailty are common in numerous diseases. On the one hand, the effectors involved in the regulation of the human circadian rhythm are closely linked to the physiological reserve function of the body. These effectors have been found to play an important role in numerous pathological pathways, including metabolic diseases,6 inflammation,7 and sleep disorders.8 On the other hand, frailty can exacerbate circadian rhythm disorders, such as insulin resistance and insomnia, by impacting metabolic levels and cognitive function.9,10
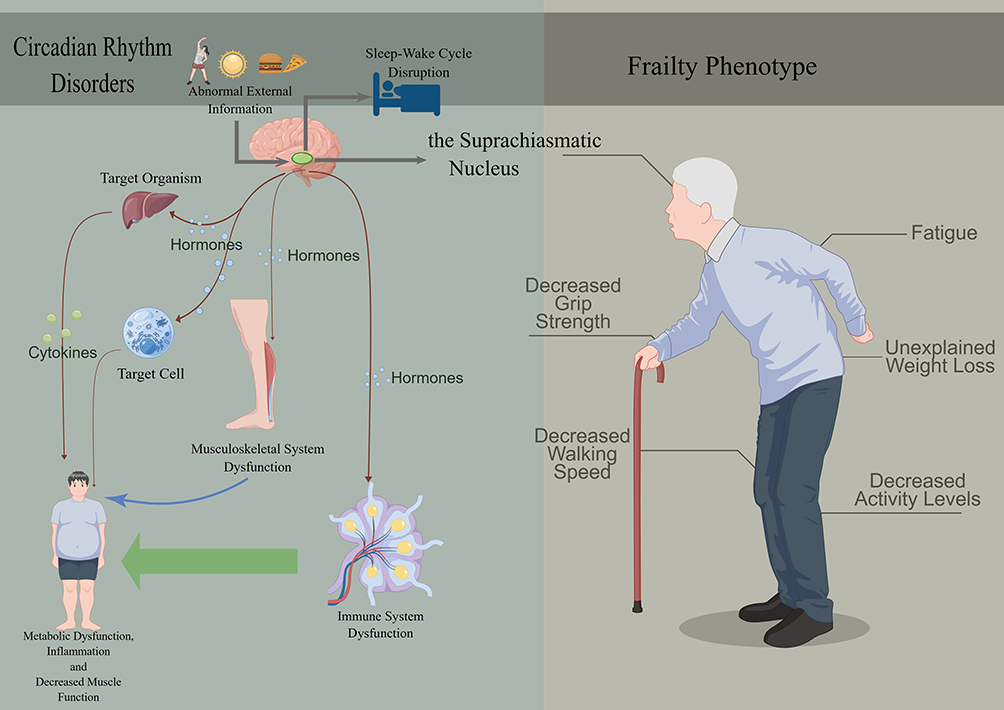 |
Figure 1 A brief introduction about how circadian rhythm disorders effect our body and potentially induce frailty among older adults. The SCN controls melatonin secretion and the appropriate sleep-wake cycle. The right figure is a schematic diagram of the frailty phenotype. This figure was drawn by Figdraw. |
At present, the investigation of circadian rhythm disruptions and frailty has emerged as a prominent area of interest within the realm of health research. However, the existing studies cannot establish a direct association between circadian rhythm disorders and frailty. A prior study conducted on a sample of 105 older individuals residing in the community revealed a correlation between rest-activity patterns and frailty.11 Another research group conducted an analysis of cohort data encompassing a sample size of over 1000 individuals of advanced age. Their findings indicate that perturbed circadian rest-activity rhythms is an early sign or risk factor for frailty in older adults.12 Conversely, in a separate cross-sectional investigation conducted on a sample of 69 older persons residing in institutional settings, the observed correlations between rest-activity rhythms and frailty did not reach statistical significance.13 The observed variations among these studies can potentially be ascribed to disparities in the study population, methods of frailty assessment, and characteristics of the individuals. Unfortunately, none of the aforementioned research has provided a precise elucidation of the connection between disruption of circadian rhythm and the manifestation of frailty. The significance of circadian rhythm function in the pathogenesis of several age-related illnesses, including metabolic disorders,6 cognitive impairment,14,15 and neurodegenerative conditions such as Parkinson’s disease and Alzheimer’s disease,16,17 is well acknowledged. The prevalence of these illnesses, compared to non-frail individuals, is higher in frail individuals. From a logical point of view, it is reasonable to hypothesize that circadian rhythm disorders are likely to contribute to or potentially induce frailty. Hence, the modulation of circadian rhythms could be regarded as a novel therapeutic approach for frailty. Moreover, elderly individuals with vulnerable physical conditions frequently exhibit psychological disorders such as anxiety and depression as a consequence of diminished quality of life.18 These conditions subsequently exacerbate sleep-wake disturbances, disrupt regular eating patterns, diminish nutritional intake, and ultimately contribute to the development of circadian rhythm disorders. The progressive emergence of these findings prompts an enquiry into the potential relationship between circadian rhythm disruption and the manifestation of frailty.
Hypothesis
We hypothesize that a bidirectional relationship exists between frailty and circadian rhythm disorders. The intersection of both pathological mechanisms, such as inflammation, metabolic disorders, and nervous system diseases, may be the cause of this relationship.
Discussion
Human trials found that circadian rhythm disorders, such as advanced sleep-wake phase disorder, delayed sleep-wake phase disorder, non-24-hour sleep-wake rhythm disorder, and irregular sleep-wake rhythm disorder, can increase glucose, insulin, and triglyceride levels, accelerate lipid accumulation, cause obesity, and reduce muscle content.19,20 Another study indicates that the frail state negatively affects the secretion of many hormones and has an adverse impact on the brain, immune system, endocrine system, and skeletal muscle, resulting in cognitive impairment, inflammation, metabolic disorder, muscle loss, and other pathological conditions.21,22 The risk factors, including metabolic syndrome, lack of exercise, and fat accumulation, will eventually cause diabetes and muscle function decline,23,24 which significantly decrease the daily activity ability and disrupt the normal sleep-wake cycle of older patients, making contributions to frailty and circadian rhythm disorders. Moreover, chronic inflammation has also been confirmed to be highly correlated with frailty and circadian rhythm.7,18 The correlation between the inflammatory state, circadian rhythm, and frailty can be confirmed by the detection of elevated pro-inflammatory cytokines (such as the inflammatory markers interleukin-6 (IL-6) and C-reactive protein (CRP)) in frail older adults.25
In addition, research has indicated that individuals suffering from neurodegenerative disorders, including sleep disorders, Alzheimer’s disease, and Parkinson’s disease, exhibit alterations in circadian rhythms, such as disrupted sleep patterns, decreased metabolic levels, and fluctuations in melatonin secretion.6,17,26 Furthermore, in a subsequent study spanning a duration of 11 years, researchers observed that a reduction in the amplitude of the circadian rhythm, the average value of rhythm adjustment, or its stability in the first stage was strongly associated with an increased risk of Parkinson’s disease.17 Previous research has shown that individuals with Parkinson’s disease have alterations in the expression of circadian core clock genes, with the most pronounced impact seen in the oscillation of BMAL1.27 The aforementioned evidence provides compelling indications of a significant association between neurodegenerative illnesses and the circadian rhythm. Besides, the correlation between neurodegeneration and frailty has been confirmed. Yuki and his colleagues28 have proved that physical activity and total energy consumption are significant predictors of the progression of frontal lobe atrophy in 8 years, which indicates the role of physical activity in maintaining brain function. Moreover, the study found that the coexistence of slow gait and cognitive impairment has the highest risk of developing dementia. Feng and his colleagues29 conducted a three-year population-based longitudinal study in Singapore involving 2375 subjects older than 55 (mean age 66). The result is that cognitive impairment will promote the occurrence of frailty, increase functional disability and mortality, and reduce patients’ quality of life.
Furthermore, the sleep-wake cycle plays a significant role both in circadian rhythm and frailty. Circadian rhythm impairments have been shown to be linked with various sleep-related issues and disruptions 8, including insomnia, diminished sleep quality, and reduced sleep duration, all of which have been regarded as predictors of frailty.30 The observed phenomenon may be attributed to the occurrence of oxidative damage in the brain and subsequent neuronal death resulting from the disruption of daily rhythmic patterns.31 Additionally, studies have shown a correlation between age-related alterations in brain function and diminished physical strength.32 Hence, the presence of circadian rhythm impairment may potentially contribute to the onset of frailty by exerting detrimental effects on the brain. Meanwhile, other research has indicated the presence of a reciprocal association between cognitive impairment and frailty.33 It implies that disturbances in the circadian rhythm may serve as one of the risk factors for cognitive impairments. Furthermore, these disruptions in circadian rhythm have the potential to impact frailty through their influence on cognitive functioning.
The outcomes of animal trials further supported the theory. Research was conducted on the BAML1 gene using mice as experimental subjects. The outcomes revealed that mice without the BAML1 gene significantly accelerated ageing processes, and notably reduced muscle function.34–36 In the assessment of frail individuals, the decrease in activity capacity and activity levels represents an increase in the risk of frailty.37 Unfortunately, there are no animal experiments or genetic studies on the circadian rhythm of frail animal.
In conclusion, here we provide evidence to verify the hypothesis that a bidirectional relationship exists between frailty and circadian rhythm disorders. Data from various animal and human experiments persuasively support the hypothesis. Our hypothesis would add a new perspective to the intervention of frailty. Additional large-scale, randomized, multicenter studies are imperative to thoroughly verify this hypothesis. To keep the balance of baseline data as much as possible when conducting the study, we advise that subsequent research endeavors should rigorously identify frail individuals through comprehensive geriatric assessment, and evaluate their circadian rhythm using scales specifically designed for circadian rhythm assessment such as the Munich Chronotype Questionnaire, and consider the influence on the circadian rhythm disorders of related conditions such as cognitive impairment. Researchers should employ interventions such as light therapy, medications, sleep pattern optimization, and regulating melatonin levels through exogenous supplementation to rectify patients’ circadian rhythm disorders. Additionally, comprehensive interventions for frail individuals encompassing exercise, improved nutrition, treatment of underlying ailments, and enhanced frailty care should be implemented, while simultaneously monitoring the improvement of circadian rhythm disorder or frailty in the patients across various aspects, including observing the changes of inflammatory cytokines (such as IL-6, TNF-a and CRP), related cytokines and hormones (such as growth hormone, insulin-like growth factor-1, epiandrosterone, testosterone and cortisol), insulin resistance, lipid metabolism disorders, muscle mass, daytime activity level, and body mass index (BMI) pre- and post-interventions. Moreover, investigating the effects of the interventions on patients’ cognitive impairment, senile anxiety, and other mental aspects before and after the interventions is also important. In addition, researchers should pay attention to the effects of the interventions on the types of circadian rhythm disturbances such as sleep-wake phase disorder, delayed sleep-wake phase disorder and the degree of circadian rhythm disturbance pre- and post-interventions as well. Another approach involves examining the impact of suprachiasmatic nucleus oscillation levels, limb motor neuron excitability, and cortical electrical activity levels pre- and post-interventions to verify the hypothesis. These studies have the potential to elucidate the underlying rules and pathological mechanisms governing the bidirectional relationship between circadian rhythm and frailty. Consequently, the results of this kind of research can contribute to enhancing the management of frailty, slowing down its progression, and ultimately enhancing the quality of life and clinical outcomes for patients.
Acknowledgments
This work was supported by the 2021 Future Medical Innovation Team Support Program of Chongqing Medical University (Project No.W0070) and Chongqing Natural Science Foundation (Project No.CSTB2022NSCQ-MSX0125). Yu Pan, Zhu Qing Feng and Yan Yuan, are co-first authors of this paper.
Disclosure
None of the authors has any potential financial conflict of interest related to this article.
References
1. Patke A, Young MW, Axelrod S. Molecular mechanisms and physiological importance of circadian rhythms. Nat Rev Mol Cell Biol. 2020;21(2):67–84. doi:10.1038/s41580-019-0179-2
2. Van Someren EJ, Kessler A, Mirmiran M, Swaab DF. Indirect bright light improves circadian rest-activity rhythm disturbances in demented patients. Biol Psychiatry. 1997;41(9):955–963. doi:10.1016/S0006-3223(97)89928-3
3. Aryal RP, Kwak PB, Tamayo AG, et al. Macromolecular Assemblies of the Mammalian Circadian Clock. Mol Cell. 2017;67(5):770–82.e6. doi:10.1016/j.molcel.2017.07.017
4. Ni Lochlainn M, Cox NJ, Wilson T, et al. Nutrition and Frailty: opportunities for Prevention and Treatment. Nutrients. 2021;13(7):2349. doi:10.3390/nu13072349
5. Navarrete-Villanueva D, Gómez-Cabello A, Marín-Puyalto J, Moreno LA, Vicente-Rodríguez G, Casajús JA. Frailty and Physical Fitness in Elderly People: a Systematic Review and Meta-analysis. Sports Med. 2021;51(1):143–160. doi:10.1007/s40279-020-01361-1
6. Qian J, Dalla Man C, Morris CJ, Cobelli C, Scheer F. Differential effects of the circadian system and circadian misalignment on insulin sensitivity and insulin secretion in humans. Diabetes Obes Metab. 2018;20(10):2481–2485. doi:10.1111/dom.13391
7. Morris CJ, Purvis TE, Hu K, Scheer FA. Circadian misalignment increases cardiovascular disease risk factors in humans. Proc Natl Acad Sci U S A. 2016;113(10):E1402–11. doi:10.1073/pnas.1516953113
8. Duffy JF, Wang W, Ronda JM, Czeisler CA. High dose melatonin increases sleep duration during nighttime and daytime sleep episodes in older adults. J Pineal Res. 2022;73(1):e12801. doi:10.1111/jpi.12801
9. Jiang X, Xu X, Ding L, et al. The association between metabolic syndrome and presence of frailty: a systematic review and meta-analysis. Eur Geriatr Med. 2022;13(5):1047–1056. doi:10.1007/s41999-022-00688-4
10. Wen Q, Yan X, Ren Z, Wang B, Liu Y, Jin X. Association between insomnia and frailty in older population: a meta-analytic evaluation of the observational studies. Brain Behav. 2023;13(1):e2793. doi:10.1002/brb3.2793
11. Maekawa H, Kume Y. Imbalance of nonparametric rest-activity rhythm and the evening-type of chronotype according to frailty indicators in elderly community dwellers. Chronobiol Int. 2019;36(9):1208–1216. doi:10.1080/07420528.2019.1626416
12. Cai R, Gao L, Gao C, et al. Circadian disturbances and frailty risk in older adults: a prospective cohort study. Res Square. 2023. doi:10.21203/rs.3.rs-2648399/v1
13. Nóbrega PV, Maciel AC, de Almeida Holanda CM, Oliveira Guerra R, Araújo JF. Sleep and frailty syndrome in elderly residents of long-stay institutions: a cross-sectional study. Geriatr Gerontol Int. 2014;14(3):605–612. doi:10.1111/ggi.12144
14. Schmidt C, Peigneux P, Cajochen C. Age-related changes in sleep and circadian rhythms: impact on cognitive performance and underlying neuroanatomical networks. Front Neurol. 2012;3:118. doi:10.3389/fneur.2012.00118
15. Souza KA, Powell A, Allen GC, Earnest DJ. Development of an age-dependent cognitive index: relationship between impaired learning and disturbances in circadian timekeeping. Front Aging Neurosci. 2022;14:991833. doi:10.3389/fnagi.2022.991833
16. Wang C, Holtzman DM. Bidirectional relationship between sleep and Alzheimer’s disease: role of amyloid, tau, and other factors. Neuropsychopharmacology. 2020;45(1):104–120.
17. Leng Y, Blackwell T, Cawthon PM, Ancoli-Israel S, Stone KL, Yaffe K. Association of Circadian Abnormalities in Older Adults With an Increased Risk of Developing Parkinson Disease. JAMA Neurol. 2020;77(10):1270–1278. doi:10.1001/jamaneurol.2020.1623
18. Soysal P, Veronese N, Thompson T, et al. Relationship between depression and frailty in older adults: a systematic review and meta-analysis. Ageing Res Rev. 2017;36:78–87. doi:10.1016/j.arr.2017.03.005
19. Scheer FA, Hilton MF, Mantzoros CS, Shea SA. Adverse metabolic and cardiovascular consequences of circadian misalignment. Proc Natl Acad Sci U S A. 2009;106(11):4453–4458. doi:10.1073/pnas.0808180106
20. Gentry NW, Ashbrook LH, Fu YH, Ptáček LJ. Human circadian variations. J Clin Invest. 2021;131(16). doi:10.1172/JCI148282
21. Bu Z, Huang A, Xue M, Li Q, Bai Y, Xu G. Cognitive frailty as a predictor of adverse outcomes among older adults: a systematic review and meta-analysis. Brain Behav. 2021;11(1):e01926. doi:10.1002/brb3.1926
22. Clegg A, Hassan-Smith Z. Frailty and the endocrine system. Lancet Diabetes Endocrinol. 2018;6(9):743–752. doi:10.1016/S2213-8587(18)30110-4
23. Leenders M, Verdijk LB, van der Hoeven L, et al. Patients with type 2 diabetes show a greater decline in muscle mass, muscle strength, and functional capacity with aging. J Am Med Dir Assoc. 2013;14(8):585–592. doi:10.1016/j.jamda.2013.02.006
24. Anbalagan VP, Venkataraman V, Pradeepa R, Deepa M, Anjana RM, Mohan V. The prevalence of presarcopenia in Asian Indian individuals with and without type 2 diabetes. Diabetes Technol Ther. 2013;15(9):768–775. doi:10.1089/dia.2013.0068
25. Picca A, Coelho-Junior HJ, Calvani R, Marzetti E, Vetrano DL. Biomarkers shared by frailty and sarcopenia in older adults: a systematic review and meta-analysis. Ageing Res Rev. 2022;73:101530. doi:10.1016/j.arr.2021.101530
26. Zhang W, Chen XY, Su SW, et al. Exogenous melatonin for sleep disorders in neurodegenerative diseases: a meta-analysis of randomized clinical trials. Neurol Sci. 2016;37(1):57–65. doi:10.1007/s10072-015-2357-0
27. Breen DP, Vuono R, Nawarathna U, et al. Sleep and circadian rhythm regulation in early Parkinson disease. JAMA Neurol. 2014;71(5):589–595. doi:10.1001/jamaneurol.2014.65
28. Yuki A, Lee S, Kim H, Kozakai R, Ando F, Shimokata H. Relationship between physical activity and brain atrophy progression. Med Sci Sports Exerc. 2012;44(12):2362–2368. doi:10.1249/MSS.0b013e3182667d1d
29. Feng L, Zin Nyunt MS, Gao Q, Feng L, Yap KB, Ng TP. Cognitive Frailty and Adverse Health Outcomes: findings From the Singapore Longitudinal Ageing Studies (SLAS). J Am Med Dir Assoc. 2017;18(3):252–258. doi:10.1016/j.jamda.2016.09.015
30. Pourmotabbed A, Boozari B, Babaei A, et al. Sleep and frailty risk: a systematic review and meta-analysis. Sleep Breathing. 2020;24(3):1187–1197. doi:10.1007/s11325-020-02061-w
31. Musiek ES, Lim MM, Yang G, et al. Circadian clock proteins regulate neuronal redox homeostasis and neurodegeneration. J Clin Invest. 2013;123(12):5389–5400. doi:10.1172/JCI70317
32. Chen WT, Chou KH, Liu LK, et al. Reduced cerebellar gray matter is a neural signature of physical frailty. Hum Brain Mapp. 2015;36(9):3666–3676. doi:10.1002/hbm.22870
33. Buchman AS, Yu L, Wilson RS, Boyle PA, Schneider JA, Bennett DA. Brain pathology contributes to simultaneous change in physical frailty and cognition in old age. J Gerontol a Biol Sci Med Sci. 2014;69(12):1536–1544. doi:10.1093/gerona/glu117
34. Bunger MK, Wilsbacher LD, Moran SM, et al. Mop3 is an essential component of the master circadian pacemaker in mammals. Cell. 2000;103(7):1009–1017. doi:10.1016/S0092-8674(00)00205-1
35. Andrews JL, Zhang X, McCarthy JJ, et al. CLOCK and BMAL1 regulate MyoD and are necessary for maintenance of skeletal muscle phenotype and function. Proc Natl Acad Sci U S A. 2010;107(44):19090–19095. doi:10.1073/pnas.1014523107
36. Kondratov RV, Kondratova AA, Gorbacheva VY, Vykhovanets OV, Antoch MP. Early aging and age-related pathologies in mice deficient in BMAL1, the core component of the circadian clock. Genes Dev. 2006;20(14):1868–1873. doi:10.1101/gad.1432206
37. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol a Biol Sci Med Sci. 2001;56(3):M146–56. doi:10.1093/gerona/56.3.M146
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.